

Adolescence is a period of nutritional vulnerability as a result of increased nutritional needs as well as unhealthy dietary patterns(Reference Enes and Slater1–4). At this stage of life, sedentary lifestyle, inadequate eating habits and susceptibility to social influence are major risk factors for chronic diseases in developing countries(3,4) .
Despite advances in global health indicators, there has been an exponential growth in the prevalence of overweight, especially among adolescents(5–Reference Bloch, Cardoso and Sichieri7). Thus, actions for the promotion of healthy dietary practices among adolescents represent a large investment in their present and future health and quality of life(3,4) .
Brazilian research on health, diet and nutrition of school-aged adolescents has revealed a critical situation. The prevalence of overweight and obesity has exceeded 25 % in adolescence(Reference Bloch, Cardoso and Sichieri7). Regarding dietary behaviours, regular consumption of ultraprocessed foods (e.g. sweets, cookies and soft drinks) has been observed as well as low consumption of in natura and minimally processed foods (e.g. fresh fruits and vegetables), leading to insufficient intake of micronutrients such as Ca and vitamins A and E(8,Reference Souza, Barufaldi and Abreu9) . Other problematic habits include skipping meals during the day and adopting sedentary behaviours(8,Reference Cureau, Silva and Bloch10) .
In this life stage, choosing what to eat is considered a way of expressing autonomy and transforming the social circle(Reference McLean and Mansfield11,Reference Hare, Szwedo and Schad12) . These characteristics make adolescents a potential target of educational actions that could promote healthy eating habits for the lifetime(13). Nonetheless, Ramos et al.(Reference Ramos, Santos and Reis14) indicated that innovative methods should be adopted to promote health education at school. In this context, digital technologies emerge as a promising strategy to be incorporated into food and nutrition education programmes, aimed at this specific age group(Reference Lindqvist, Kostenius and Gard15–Reference Salam, Das and Lassi17).
A systematic review on the use of technology in nutritional interventions for this age group showed that the ones involving games were effective in improving determining factors for the choice and consumption of healthy food, such as decreased sugar consumption and increased home availability of healthy food; intake of fibre, Ca, and vitamins C and B2; and nutritional knowledge(Reference Melo, Vargas and Chagas18). As media capable of influencing people’s behaviour, games can be used for educational purposes. In the context of development and expansion of cognitive and intellectual abilities, they are called educational games, learning games or serious games(Reference Thompson19). The literature also demonstrates that the use of games aimed at fighting obesity in children and adolescents may support an engaging and active process of change, as a systematic review showed improvements in nutritional knowledge, increased availability and consumption of healthy foods and water, and greater self-efficacy in vegetable intake(Reference Guy, Ratzki-Leewing and Gwadry-Sridhar20).
This study aimed to assess the individual-level impact of a nutritional intervention for high school students on food consumption, nutritional knowledge and self-efficacy in the adoption of healthy eating practices, based on the use of a digital game that was developed to promote healthy eating.
Methods
Study design
This cluster randomised controlled trial recruited both male and female adolescents from private schools in the Federal District, Brazil. Private schools were considered more appropriate because the intervention required students to play the game on their own mobile devices (smartphones and tablets), which tend to be expensive and thus more accessible to private than public school students. The study was conducted and reported according to the Consolidated Standards of Reporting Trials guidelines(Reference Campbell, Piaggio and Elbourne21).
Participants
Randomisation and recruitment
After a simple randomisation procedure, eight schools were drawn, four for each group, from a universe of 121 private schools(22). However, fifty-three schools had to be invited (by email, phone and personal visit) until eight agreed to participate. Sixteen schools refused to participate and twenty-nine did not respond to or denied the invitation because of excessive school activities; lack of time for research involvement; development of other activities related to healthy eating and non-authorisation of underage participants. This explains the exclusion of forty-five schools that were previously drawn (Fig. 1). Each school unit was invited to participate in the study without any previous knowledge of the allocation group. After the schools agreed to participate in the study, the students’ parents signed an informed consent form and then the students were asked to express their interest. This study had no exclusion criteria. Additional sampling information has been published elsewhere(Reference Chagas, Silva and Reffatti23).

Fig. 1 Flow diagram of adolescents’ participation in the study
Intervention
The digital game used in the intervention was developed specifically for this study. The name Rango Cards combines a Brazilian cultural expression related to food (‘rango’) and an English reference to card games (‘cards’). Its purpose is to present the concept of healthy and adequate diet based on the Dietary Guidelines for the Brazilian Population (24). The mechanics of the game is similar to that of Hearthstone® (Blizzard Entertainment), named the best multiplayer game by Google Play in 2017(Reference Kochikar25). In Rango Cards, however, the matches take place on a dining table and the characters have common features of Japanese animation (anime) and American comic books, in order to create similarity with other popular games. Figure 2 shows the general components of the game.

Fig. 2 Screenshot of Rango Cards’ interface
The game is based on social cognitive theory, especially the idea of determinants of eating behaviour, that is, knowledge and self-efficacy(Reference Bandura26,Reference Bandura27) . The virtual environment where the narrative of Rango Cards unfolds is a school (consisting of courtyard, library and auditorium), except for the third phase, in which the player visits a restaurant that serves healthy meals. The game is divided into seven phases, addressing the following themes: food classification; healthy eating practices; importance of the act of cooking; food marketing focused on misleading advertisement and importance of reading food labels to understand the nutritional content of food items(24).
Game design, theme selection and phase order were conceived to provide the player with a learning experience. Rango Cards is free, in Portuguese, compatible with Android and iOS devices and available from Google Play and App Store since April 2017. More information about the game can be found in Chagas et al.(Reference Chagas, Silva and Reffatti23).
Intervention group
Adolescents from the intervention group were instructed to download the game. They first played it at school accompanied by a researcher responsible for answering questions. Then, they could play it at the time and space that best suited their routine, individually or collectively, from 7 (minimum) to 17 (maximum) days.
Control group
Adolescents from the control group were not instructed to play the game nor received any healthy dietary recommendations, that is, the researchers did not provide them with any additional material during the study.
Data collection
School recruitment and data collection were conducted from June to September 2017. Previously trained unblinded researchers were responsible for, after completion of the pre-intervention questionnaire, guiding adolescents in the intervention group on how to download and play the game. Both groups completed previously tested questionnaires, which were applied at schools before and after the nutritional intervention. The following variables were investigated: age, sex, monthly family income, maternal education level, dietary perceptions and practices, nutritional knowledge and self-efficacy in the adoption of healthy eating practices. The pre- and post-intervention questionnaires included the same questions, except for the socio-demographic variables, which were collected only at the first moment of the study.
Measures
Socio-demographic data, dietary perceptions and practices
The assessment of monthly family income and maternal education level was based on questions included in periodic population surveys conducted in Brazil(28). Regarding dietary perceptions, participants were asked to provide scores for how healthy they considered their diet to be and how much they knew about the topic, ranging from 0 to 10.
Dietary practices were assessed according to National School-Aged Adolescent Health Survey criteria(8). Participants were asked about frequency of consumption of healthy (beans, vegetables and fruits) and unhealthy foods (ultraprocessed foods, fried snacks, soft drinks, sweets and fast foods) and frequency of having breakfast, lunch or dinner with parents or guardians and of eating while watching television or studying.
Knowledge and self-efficacy
Nutritional knowledge and self-efficacy in the adoption of healthy eating practices were assessed based on the content of the game and on items from previous studies with adolescents and young adults(Reference Toral and Slater29–Reference Tassitano, Cabral and Silva31).
Regarding nutritional knowledge, the participants should consider fifteen statements and express their level of agreement using a five-point Likert-type scale, ranging from 1 (‘I strongly disagree’) to 5 (‘I strongly agree’) (see Supplementary material, Appendix I). Similarly, self-efficacy was evaluated using nineteen statements, for which the participants should express whether they planned to, would be able to or would feel confident to perform a list of actions, with scores ranging from 1 (‘No, not at all’) to 5 (‘Yes, certainly’) (see Supplementary material, Appendix II).
The assessment of the validity of the questionnaire included 539 first-grade high school students from eight private schools in the Federal District, Brazil. Analyses were performed using exploratory factor analysis. Kaiser-Meyer-Olkin and Bartlett’s sphericity tests were performed to determine whether data fitted the exploratory factor analysis. Cronbach’s alpha (α) was used to determine the internal consistency of nutritional knowledge and self-efficacy to adopt healthy eating behaviours, and values of 0·808 and 0·875, respectively, were obtained. The analyses confirmed the validity of the tool for nutritional knowledge and self-efficacy to adopt healthy eating behaviours among adolescents.
Data management and analysis
After data collection, the answers to the questionnaires were double-entered into electronic spreadsheets. Socio-demographic variables were analysed descriptively using means, standard deviations and frequencies. Then, for nonparametric data, Pearson’s χ 2 test (sex and age) and Mann–Whitney U test (monthly family income and maternal education level) were performed according to clusters.
To assess the impact of the intervention, unpaired analyses were performed using the Student’s t test for numerical variables (dietary perceptions) and Likert-type scales (knowledge and self-efficacy) considered continuous. The Mann–Whitney U test was used for dietary practices and consumption. The level of significance was set at 5 %. For inferential analyses, pre- and post-intervention differences were considered when assessing numerical or ordinal responses. The statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 21.0.
Results
Initially, this study included 570 adolescents, being 348 in the control group and 222 in the intervention group. There were no significant differences between control and intervention groups regarding age (P = 0·381), sex (P = 0·902), monthly family income (P = 0·700) and maternal education level (P = 0·765) (data not shown). Of those, 319 participants completed the study, being 202 in the control group and 117 in the intervention group (Fig. 1).
The participants were homogeneously distributed in terms of sex (57·4 % were girls), and almost all of them were between 13 and 16 years old (94·6 %), with a mean age of 15·8 (sd 0·7) years. Of those who provided information about monthly family income (n 175), 48 % reported income of up to BRL (Brazilian Real or R$) 4685·00. Regarding level of education, the mothers of only 19·7 % (n 173) of adolescents did not complete high school. At baseline, there were no significant differences between control and intervention groups with regard to socio-demographic data (Table 1), dietary perceptions (Table 2) and practices, and the set of statements on nutritional knowledge and self-efficacy in the adoption of healthy practices.
Table 1 Baseline study data, Federal District, Brazil, 2017*

BRL, Brazilian Real or R$.
* Only valid responses were considered for each variable. Income assessment based on the Brazilian National Household Survey (PNAD); minimum wage of R$937 (approximately US$226) considered.
† Pearson’s χ 2 test.
‡ Mann–Whitney U test.
Table 2 Dietary perceptions of the intervention and control groups before and after the intervention, Federal District, Brazil, 2017
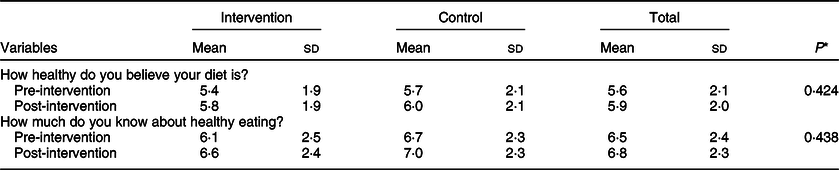
* Student’s t test.
The analysis of regular dietary practices revealed that eating while watching TV or studying and having meals at fast food restaurants reduced significantly in the intervention group compared with the control group (Figs 3 and 4).

Fig. 3 Comparison between the habit of eating while performing other activities before and after the intervention, Federal District, Brazil, 2017. ![]() , No;
, No; ![]() , rarely;
, rarely; ![]() , yes, 1–2 d/week;
, yes, 1–2 d/week; ![]() , yes, 3–4 d/week;
, yes, 3–4 d/week; ![]() , yes, 5–6 d/week;
, yes, 5–6 d/week; ![]() , yes, everyday
, yes, everyday

Fig. 4 Comparison between having meals at fast food restaurants before and after the intervention, Federal District, Brazil, 2017. ![]() , 5 d or more;
, 5 d or more; ![]() , 4 d;
, 4 d; ![]() , 3 d;
, 3 d; ![]() , 2 d;
, 2 d; ![]() , 1 d;
, 1 d; ![]() , none
, none
For the set of statements regarding nutritional knowledge and self-efficacy in the adoption of healthy eating practices, very similar mean scores were found between the groups before and after the intervention, with no significant differences. The items regarding knowledge of fruit and vegetable consumption, intention to reduce Na consumption and intention to prepare healthy meals are worth mentioning. They achieved higher mean scores in the intervention group at the second moment of the study, with significant differences compared with the control group. These results are shown in Table 3.
Table 3 Comparison between the responses provided for nutritional knowledge and self-efficacy in the adoption of healthy eating practices in the intervention and control groups before and after the intervention, Federal District, Brazil, 2017

† Student’s t test.
* P < 0.05.
Discussion
This study innovates in the presentation of the concept of healthy and adequate diet for adolescents using the Dietary Guidelines for the Brazilian Population (24). Few game-based interventions have been created for such purpose. As innovative media, digital games are potentially capable of influencing health outcomes, providing engagement and pleasure(Reference Melo, Vargas and Chagas18,Reference Hieftje, Edelman and Camenga32,Reference Baranowski, Blumberg and Buday33) .
Several benefits have been attributed to game-based learning, and Rango Cards includes the following: opportunity for decision-making; attribution of meaning to concepts difficult to understand; stimulation of players’ active participation; creation of motivation and personal satisfaction; and use of different learning styles and skills(Reference Ebner and Holzinger34,Reference Van Lippevelde, Vangeel and De Cock35) . In addition, the mechanics of Rango Cards was inspired in a major worldwide success. According to Bakkes et al.(Reference Bakkes, Tan and Pisan36), a player-centred game design leads to a stronger connection between the player and the technology, ensuring increased playability and satisfaction, which could produce promising results, as those found in Rango Cards.
The Rango Cards intervention resulted in changes in some dietary behaviours displayed by the adolescents. Initially, a positive impact observed in the intervention group was a significant reduction of the habit of eating while watching TV or studying. This dietary behaviour is an important marker because of its association with the consumption of unhealthy foods(Reference Hare-Bruun, Nielsen and Kristensen37), whose explanatory mechanisms address food preferences and/or lack of attention(Reference Bickham, Blood and Walls38). Being attentive and aware while eating is a determining factor for adherence to healthy eating(Reference Jordan, Wang and Donatoni39,Reference Seguias and Tapper40) and is recommended in the Brazilian guidelines(24). This was considered in the elements of the game, including a specific card that ensures gameplay to the player and also explores the benefits of being calm during the match.
Regarding food consumption, the intervention had an impact on the frequency of having meals at fast food restaurants, which decreased in the intervention group. Reducing high-energy, low-nutrient and ultraprocessed food intake, which characterises fast food restaurants(Reference French, Story and Neumark-Sztainer41), is a target in the prevention of serious health damages, as there is convincing evidence that nutritionally unbalanced foods lead to overweight(Reference Louzada, Baraldi and Steele42–Reference Monteiro, Moubarac and Levy46). A possible explanation for this finding is that Rango Cards implements a system of measuring salt, sugar and fat, whose levels alter after the use of ultraprocessed foods (nutritionally unbalanced foods). The meters directly impact health levels, energy and time available to play the match.
Fruit and vegetable consumption is a health marker associated with diet quality and improved total energy density(Reference Thompson, Ferry and Cullen47). Thus, several educational strategies using games for health promotion seek to expand nutritional knowledge of the topic(Reference Baranowski, Blumberg and Buday33,Reference Haaranen, Rissanen and Laatikainen48,Reference DeSmet, Van Ryckeghem and Compernolle49) . In this study, the intervention group acquired more knowledge of the importance of fruit and vegetable consumption compared with the control group. This finding can be explained by the design and mechanics adopted for this food category in Rango Cards, in which in natura foods increase the maximum energy available for the player at the beginning of a match. The mechanics is in line with that suggested by Suttie et al.(Reference Suttie, Louchart and Lim50), so that the process of learning how to play the game provides the knowledge and skills intended in the strategy. Nonetheless, no significant changes were observed in the set of statements related to nutritional knowledge after the intervention, which is consistent with the lack of changes in the adolescents’ perception of their knowledge of the topic.
The adolescents from the intervention group also showed positive changes in two aspects evaluated for self-efficacy in the adoption of healthy eating practices. They reported planning to, being able to or feeling more confident to reduce Na consumption and to prepare healthy meals, which was a favourable outcome because self-efficacy is a predictor of health behaviour change(Reference Bandura26,Reference Bandura27) . This finding suggests that Rango Cards is associated with increased intention of making positive changes, which is reinforced by the actions, mechanics and design of the game. According to Lieberman(Reference Lieberman51), games allow players to rehearse skills repeatedly until they win, providing practice and showing cause and effect, which may lead to improved health outcomes. An increased level of motivation for small changes has also been found in other studies using different mobile strategies(Reference Rai, Chen and Pye52–Reference Rose, Barker and Maria Jacob55), showing the importance of such technologies.
Strengths and limitations
Determinants of eating behaviour, specifically in this study nutritional knowledge and self-efficacy in the adoption of healthy eating practices, influence individuals to make positive changes(Reference Thompson19,Reference Bandura26,Reference Bandura27) . Therefore, although limited to specific aspects of dietary consumption, practice, knowledge and self-efficacy, the impacts of the nutritional intervention with Rango Cards may be considered of great relevance, especially because such changes may improve adolescents’ health in the long term. Thus, the design of Rango Cards is potentially capable of having an impact on dietary outcomes and practices, as well as in determinants of eating behaviour.
Other variables showed no significant differences between the intervention and control groups. A possible explanation is the duration of the intervention (7–17 d), as the literature indicates that long-term strategies may achieve better results(Reference Melo, Vargas and Chagas18,Reference Baranowski, Blumberg and Buday33) . However, there is still no consensus on intervention time, and relatively short programmes have had effective impacts on health prevention(Reference Stice, Shaw and Marti56). We suggest the development of games focusing on food and nutrition with a longer duration of intervention or higher number of phases, thus enhancing the involvement and engagement of adolescents.
Because the game is free, available on major mobile app distribution platforms, and had satisfactory short-term results, it can be easily incorporated as an educational resource in Brazilian public policies. However, because Portuguese is the only language available in the game, international dissemination is compromised; nonetheless, this has never been an objective of this study, as the game is based on Brazilian nutritional material. We suggest then that each country should develop its own game consistent with local culture, food preferences and health priorities.
The absence of mechanisms to evaluate usability, including playing time, and to measure long-term effects is another limitation of the present study. There is a gap in the literature regarding maintenance of health behaviours, with few studies assessing the prolonged impact of digital games on health promotion(Reference Haaranen, Rissanen and Laatikainen48,Reference DeSmet, Van Ryckeghem and Compernolle49) .
The extrapolation of the results to different age groups and social contexts should be analysed with caution because the present study allowed direct contact between researchers, adolescents and the digital game. According to Newman et al.(Reference Newman, Szodny and Llera57), human contact may influence the results of interventions using technological tools. Thus, future studies using the present game should examine the mechanisms of influence on determinants of and changes in eating behaviour; assess the maintenance of healthy eating practices and determine the efficacy and usability of the tool in other contexts, age groups and social classes.
Conclusion
This study found an impact of the intervention on the habit of eating while watching TV or studying; on having meals at fast food restaurants; on knowledge related to the importance of fruit and vegetable consumption and on self-efficacy in the adoption of healthy eating practices such as reducing Na intake and preparing healthy meals. The results, although limited and not representative of Brazil, confirm the potential of Rango Cards among Brazilian adolescents who have access to mobile devices, providing opportunities for discussion of innovative tools that exceed the limits of space and time and promote autonomy and self-care in relation to adequate and healthy eating.
Acknowledgements
Acknowledgements: None. Financial support: This research was supported by the Research Support Foundation of the Federal District, Brazil (FAPDF), call notice no. 03/2015, spontaneous demand – grant no. 0193.000953/2015. The FAPDF had no role in the design, analysis or writing of this article. Conflicts of interest: None. Authorship: C.M.S.C. contributed to the conception and design, analysis and interpretation of data, and manuscript writing. R.B.A.B. and G.R.M. contributed to manuscript writing and review. N.T. collaborated in the concept and design, analysis and interpretation of data, manuscript writing and review. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Research Ethics Committee at the University of Brasília School of Health Sciences. Participants were thoroughly informed about the study. Only those whose parents or guardians provided written consent were included in the study.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020000531









