



Quilombolas communities were formed during the colonial period in resistance to the slave system to which black slaves from Africa were subjected in Brazil(Reference Filho and Prioste1). Despite the abolition of slavery in 1888, only after a century, through the Federal Constitution of 1988, did quilombolas acquire official recognition of their identity and the right to own their own land(2). This population lives in communities called quilombos, which mostly comprise black-skinned and brown-skinned descendants of the enslaved, maintain the form of social organisation of their ancestors and have unique relations with the land and specific cultural practices(3).
Brazil owes a historic debt to quilombolas. They exist in a context of ethnic–racial discrimination and social exclusion, have the worst socio-economic indicators and, as one of the most evident problems, experience food insecurity (FI)(Reference Cordeiro, Monego and Martins4–Reference Carvalho, Alberto and Pereira8). With a goal of combatting hunger, poverty and FI, the Brazilian government has invested in public policies aimed at guaranteeing food and nutrition security (FNS) as an intervention strategy(9–Reference Kepple and Segall-Corrêa11). Evaluation of FI at the household level through hunger perception scales, such as the Brazilian Household Food Insecurity Measurement Scale (Escala Brasileira de Insegurança Alimentar, EBIA), has been established as an adequate approach for evaluating this outcome among population surveys(Reference Marques, Reichenheim and Moraes12–Reference Sperandio, Morais and Priore15).
The Brazilian national FI survey(16) revealed a picture of inequality. Populations of people with black or brown skin had a much higher prevalence of FI than populations of other colour/race. These data reinforce the historical social and racial inequities in the country(Reference Chor17). The relationship between colour/race and FI is complex and interconnected with other determining factors, including poverty and public policies that guarantee access to health and food(Reference Odoms-Young and Bruce18).
There is little information about this population. To date, the existing studies suggest that the population is socioeconomically vulnerable, in addition to experiencing difficulties accessing their territories and having adequate food access and health(Reference Cordeiro, Monego and Martins4–Reference Carvalho, Alberto and Pereira8). However, there are still knowledge gaps regarding access to FNS related to governmental programmes (GP) as a way of reducing hunger and poverty in this group. The objective of the current study was to assess access to GP and their association with FI among quilombolas. The analyses of the GP presented in this research investigated whether quilombolas families were able to access GP and, among those that did, how this related to the FI in their homes.
Methods
Microdata from a national survey, the Quilombolas Census(19), that was carried out from April to November 2011 were used. The target population was represented by 169 quilombolas communities, which corresponded to 9193 families that had received judicial titles for their territories between 1995 and 2009(20). More methodological details were published in the technical report of the Quilombolas Census(20). The current study did not consider families without a member who declared themselves quilombolas (n 2510; 2·7 %), living outside the quilombo territory (n 75; 0·9 %), whose head of household was a teenager (age < 15 years; n 3; 0·03 %) or with missing data (n 121; 1·3 %). Thus, a final sample of 8743 families (95·1 %) was considered.
The EBIA was established as a tool for measuring household FI in population studies(19). It is an experience-based scale adapted from the US Household Food Security Survey Module that has been validated for use in the Brazilian population since 2003(Reference Segall-Corrêa, Marin-León and Melgar-Quiñonez21–Reference Reichenheim, Interlenghi and Moraes23). The theoretical underpinning of this instrument is that it considers FI to be a progressive phenomenon experienced at the household level with different levels of severity(Reference Palmeira, Bem-Lignani and Maresi24). As FNS is a multidimensional issue, it is challenging to define instruments that can measure it at the population level. The EBIA measures the prevalence of FI, but it does not cover the ‘nutrition’ dimension of the FNS so that households can be classified according to food security or FI level(Reference Segall-Corrêa, Marin-León and Melgar-Quiñonez21). The FNS is considered in its broad concept to dialogue with FI and to guide public policies to promote health, nutrition and healthy eating. The FI measure, performed by the EBIA, is used to monitor food security in population studies.
Nevertheless, the EBIA has consistently been shown to be psychometrically valid(Reference Segall-Corrêa, Marin-León and Melgar-Quiñonez21,Reference Reichenheim, Interlenghi and Moraes23) , which reinforces its suitability for monitoring FI through prevalence studies, identifying risk groups, such as quilombolas communities(Reference Gubert, Segall-Corrêa and Spaniol6) and studying the causes (e.g. poverty) and consequences (e.g. dietary and health outcomes) of FI(Reference Morales and Berkowitz25–Reference Moradi, Mirzababaei and Mohammadi27). It is a scale composed of fourteen dichotomous items (yes/no) for households with children and/or adolescents under 18 years of age and eight items for households with only adults. Based on the sum of affirmative responses to the EBIA, households were classified into four categories: food security, mild FI, moderate FI and severe FI. In the current study, the categories of moderate and severe FI were considered together due to interest in discussing the most severe levels of FI.
The GP related to FNS promotion were identified and categorised into four groups. The GP constituting a set of actions planned to guarantee the offer of and access to food for the entire population and promote nutrition and health were selected. These GP were categorised according to their area of activity and are in the guidelines of the FNS policy proposed by the working group of the Brazilian National Council for Food and Nutrition Security(28,29) . The GP were evaluated through questions considering the participation of quilombolas in ‘rural development’ programmes, including the National Program of Family Agriculture Strengthening (Programa Nacional de Fortalecimento da Agricultura Familiar), the Food Acquisition Program (Programa de Aquisição de Alimentos), Family Farm Insurance (Seguro da Agricultura Familiar), Rural Technical Assistance and Extension (Assistência Técnica e Extensão Rural) and crop guarantee (Garantia-safra); in ‘health’ programmes, including home visits by a community health agent (agentes comunitários de saúde) and the Center for Family Health Support (Estratégia Saúde da Família); in ‘food or water supply’ programs, including food baskets (cestas de alimentos) and the Cisterns Program (Programa Cisternas); and in ‘income increase’ programs, including Brazilian conditional cash transfer (Bolsa Família) and Continued Benefit Transfer (Benefício de Prestação Continuada).
Considering that GP have different eligibility criteria, that is, that some are specific to families with different types of vulnerability (e.g. poverty or extreme poverty, participation in family farming, presence of individuals with low education, presence of elderly people or families living in specific regions), the current study assessed eleven GP independently. Participation in the programmes was considered according to an affirmative response for one or more policies within each of the above categories.
The groups, GP, characteristics, goals and target audience are described in Fig. 1. The rural development categories cover five policies related to family farming, as they operate with rural credit lines and infrastructure and technical assistance(30–Reference Ribeiro, Moreira and Rodrigues33). The health category was composed of two GP considering policies for the promotion, prevention and surveillance of health and quality of life(32,34) . Another two GP comprised the food or water supply group, which included donations of basic food baskets for emergency situations and the production of cisterns with rainwater harvesting for low-income and socially vulnerable families(31,32) . The income increase group was organised considering the programmes that adopt initiatives to supplement the beneficiaries’ income in the short and long terms(32,35) .

Fig. 1 Group, governmental programs, characteristics and goals and target audience. *Free translation of governmental programmes. Sources: Brazil, Lei 10·420, de 10 de abril de 2002; Ministério do Desenvolvimento Agrário, 2010; Secretaria de Políticas de Promoção da Igualdade Racial, 2013; Ribeiro et al., 2017; Brazil, Portaria 2·488, de 21 de outubro de 2011; Brazil, Decreto 6·214, de 26 de setembro de 2007
A structured questionnaire on household socio-demographic characteristics was applied to assess data on the head of household (gender, age, marital status and educational level) and household characteristics (number of residents, number of children under 5 years of age, electricity, adequate sanitation and adequate water supply). Adequate sanitation considered the collection of garbage and sewage in the home. The locations of the households were grouped according to the regions of Brazil (North, Northeast, South/Southeast and Central-West). The South and Southeast regions were considered together due to the small number of quilombos in each region and socio-demographic similarity.
Total monthly household income was estimated considering the sum of the income from all household residents (Bolsa Família benefit, paid work, pensions, the sale or cultivation of animals and the sale of handicrafts). Monthly household income was categorised as minimum wage multiples, considering the sum of all monthly income for the whole family. The Brazilian minimum wage was $US349·3 (R$545, where R$ is Brazilian real) in 2011, and the corresponding average US dollar-real exchange rates was R$1·56 per US dollar.
The first step of the analysis consisted of estimating the distribution (%) of FI among the quilombolas families in the country and by region. A χ 2 test was performed to investigate the relations between the socio-demographic variables, the region of the country and FI. Descriptive analyses of the quilombolas’ socio-demographic characteristics and GP were carried out. Subsequently, the prevalence and the respective CI (95 % CI) of the socio-demographic characteristics and access to GP were estimated according to the levels of FI. The three-level household FI-dependent variable considering three categories of FI (food security [reference level], mild and moderate/severe) was used in the bivariate analyses. Considering that the purpose of this article was to investigate whether quilombolas families had access to GP and to discuss this access, an analysis of each social programme and its relationship with the reduction of FI was conducted separately.
Multinomial logistic regression analysis was performed to estimate the OR and the 95 % CI. Statistical models were used to estimate the OR of each socio-demographic variable and GP separately considering the different inclusion criteria of the respondents in each program. The adjusted model for the effect of the socio-demographic variables was considered, and the level of 20 % was adopted for inclusion in the final model. The decision to adopt a conservative significance level of 20 % was based on the related literature(Reference Hosmer and Lemeshow36,Reference Abreu, Siqueira and Caiaffa37) . Model adjustment tests were performed using the Akaike information criterion and variance inflation factor(Reference Fávero, Belfiore and Silva38). The analyses were performed using Stata 13.0 statistical software(39).
Results
The prevalence of FI was 86·1 %. The North (67·1 %) and Northeast (48·3 %) regions presented the highest proportions of moderate/severe FI, and the FI in the North region was higher than the national average (55·9 %) and 3·7 times greater than that in the South/Southeast region (14·4 %). Families in the South/Southeast region had 47·3 % food security; that is, they reported not having any concern about the lack of food in the future (Fig. 2).

Fig. 2 Distribution (%) of food insecurity (FI) measured by the Brazilian Household Food Insecurity Measurement Scale (Escala Brasileira de Insegurança Alimentar, EBIA) among Quilombolas families in the country and by regions. Communities of descendants of enslaved blacks in Brazil, 2011. *χ
2 test indicates presence of difference between distribution in Brazil and the regions of the country (P < 0·001). ![]() , Food security;
, Food security; ![]() , mild FI;
, mild FI; ![]() , moderate/severe FI
, moderate/severe FI
Low participation in rural development programmes was observed. The coverage of the health GP was greater regarding the actions of home visits by a community health agent (75·0 %); however, 34·9 % of households reported accessing the Center for Family Health Support. The food or water supply GP were not as significant, as 31·9 % received food baskets and only 4·2 % accessed the Cisterns Program. Bolsa Família is among the programmes with the largest national coverage, yet 61·3 % of households reported receiving the benefit and 11·2 % accessed Continued Benefit Transfer (Table 1).
Table 1 Descriptive analyses of the household food insecurity, socio-demographic characteristics and governmental programmes of Quilombolas families. Communities of descendants of enslaved blacks in Brazil, 2011

* Minimum wage in Brazil in 2011: $US 349.3 (R$ 545 (Brazilian real)).
Analysis of the socio-demographic variables and FI categories (Table 2) revealed that the heads of household aged 31–40 years, in a married/consensual union, with 1–7 years of schooling, living in homes with ≥ 6 residents, living in homes with the presence of a child under 5, living in homes without electricity, living in homes with adequate sanitation, with access to filtered water, living in homes located in the North region, or with a total monthly income between > ½ and ≤ 1 minimum wage were more likely to have moderate/severe FI (P-value < 0·05). Regarding participation in GP, 44·4 % of families that were included in the Food Acquisition Program were more likely to present mild FI, while those that received crop guarantee; received a home visit by a community health agent or who had received aid from the Center for Family Health Support, food baskets, the Cisterns Program, Bolsa Família or the Continued Benefit Transfer were more likely to have moderate/severe FI (P-value < 0·05).
Table 2 Prevalence (%) and the respective confidence intervals (95 % CI) of the socio-demographic characteristics and access to governmental programmes according to the levels of household food insecurity (FI). Communities of descendants of enslaved blacks in Brazil, 2011
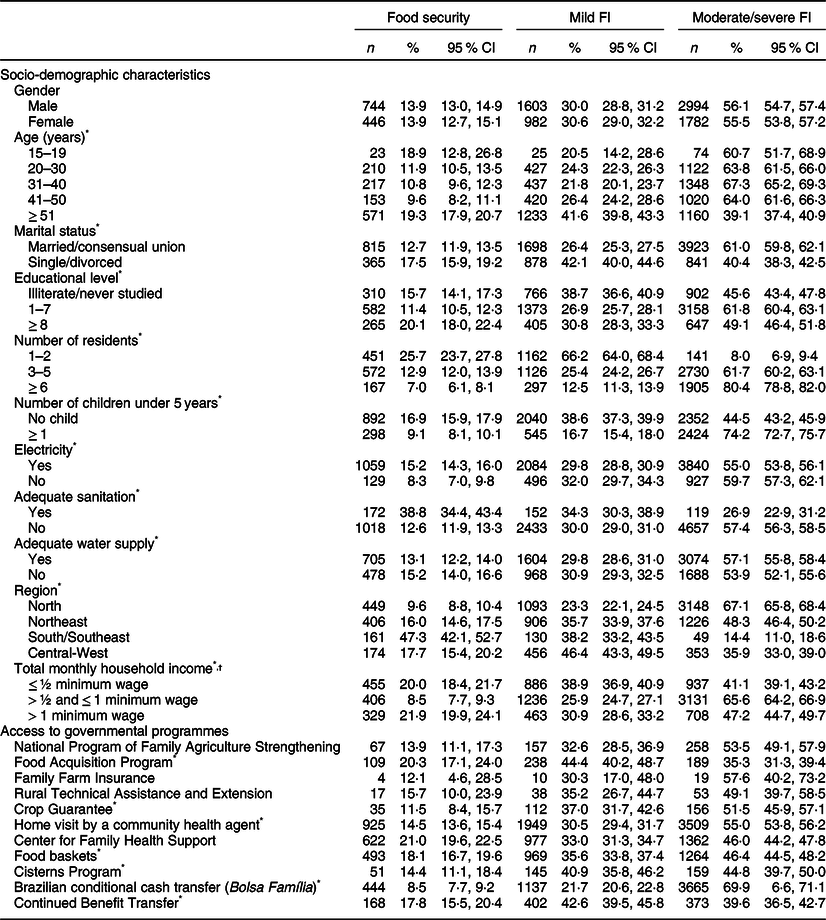
* Analysed variables that showed statistical significance in the bivariate analysis using the χ2 test and considering a significance level of P < 0·05.
† Minimum wage in Brazil in 2011: $US 349·3 (R$ 545 (Brazilian real)).
After adjusting for all variables (except gender), we highlight that households with ≥ 6 residents had 23·3 (95 % CI 16·7, 32·4) times higher odds of experiencing moderate/severe FI than those with 1–2 residents. Similarly, the households located in the North region had 11·0 (95 % CI 6·9, 17·7) times higher odds of experiencing moderate or severe FI than those located in the South/Southeast region. Quilombolas with access to the Food Acquisition Program and to the Center for Family Health Support presented a protective factor for moderate/severe FI (OR: 0·6, 95 % CI 0·7, 1·7; and OR: 0·5, 95 % CI 0·5, 0·7, respectively). Receiving Bolsa Família was significantly associated with the presence of moderate/severe FI (OR: 3·3, 95 % CI 2·8, 4·0) (Table 3). Variance inflation factor test indicated that there was no multicollinearity (variance inflation factor = 1·2)(Reference Fávero, Belfiore and Silva38).
Table 3 Unadjusted and adjusted OR and confidence intervals (95 % CI) of the relationship between socio-demographic characteristics and access to governmental programmes according to the levels of household food insecurity. Communities of descendants of enslaved blacks in Brazil, 2011
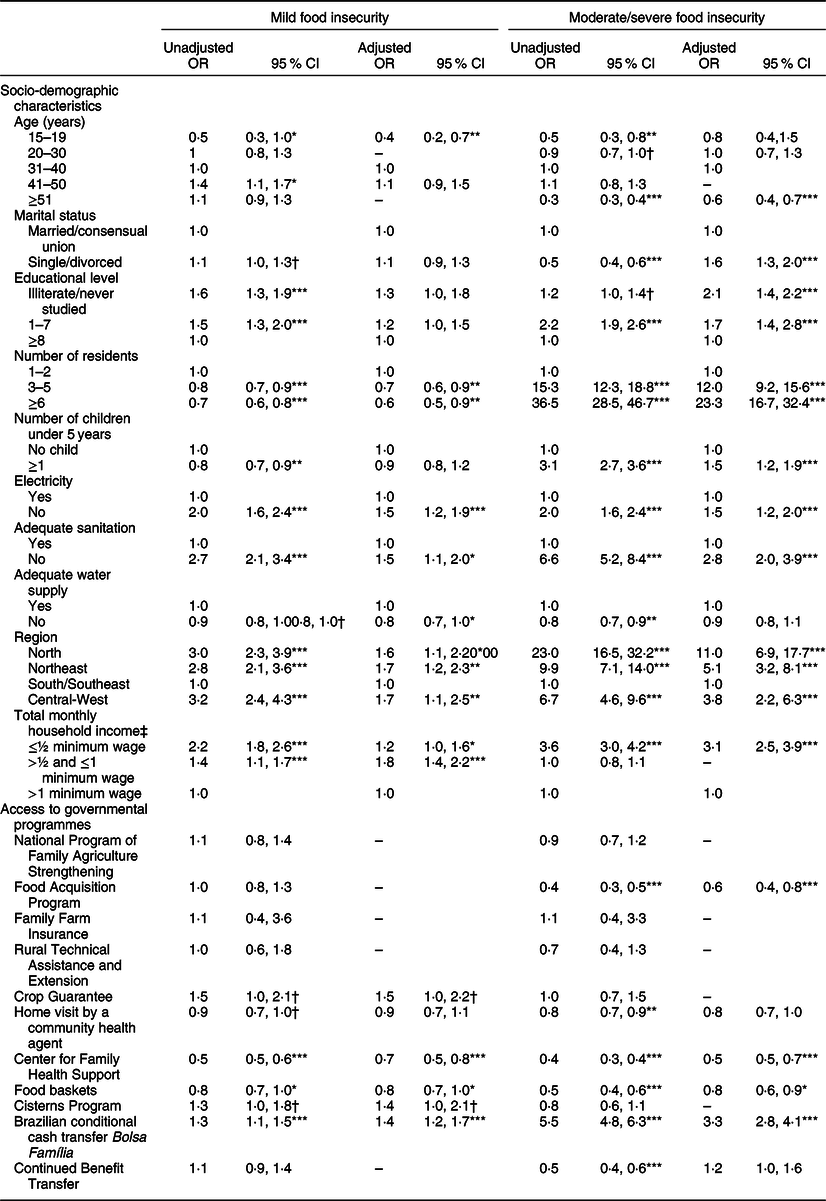
* P < 0·05.
** P < 0·01.
*** P < 0·001.
† P < 0·20.
‡ Minimum wage in Brazil in 2011: $US 349·3 (R$ 545 (Brazilian real)).
Discussion
Quilombolas can access any of the GP investigated in the current study. These GP were planned for the general population, which reinforces the importance of policies designed for and focused on the specificities of these communities. Each programme has different characteristics and is related to the promotion of FNS.
The latest national survey that investigated FI in Brazil(16) showed disparities between regions, where the North and Northeast regions had the highest proportions of FI. Considering the moderate/severe FI level, the panorama of regional inequality remained in the quilombolas population. It is worth mentioning that, in comparison to the other regions, these territories are less favoured socioeconomically, with high proportions of FI and poor access to health services(16,40) .
Brazil has been investigating FI through national surveys since 2003, and over the years, it has been possible to observe a significant reduction in FI(16). However, the most recent census(16) indicated that despite the reduction in moderate/severe FI over the years (2003–2013), in 2018, there was a significant increase in all levels of FI. In addition, there have been indications that Brazil has returned to the list of countries that make up the hunger map(41,42) , mainly after budget cuts to social programmes and a decrease in social protection networks. It should be noted that Brazilian population censuses do not include quilombolas.
The findings of previous studies that also used the EBIA to measure FI in quilombos (Reference Silva, Medeiros and Martins7,Reference Carvalho, Alberto and Pereira8,Reference Monego, Peixoto and Cordeiro43) corroborate the present data. The authors of those studies also found a high prevalence of FI and referred to the importance of public policies for reversing this situation and fighting hunger, racial inequalities, precarious living conditions and difficulties in accessing services and rights.
An intersectional approach(Reference Blackell and Naber44,Reference Rios and Silva45) is important for the recognition of the historical and cultural complexity that most quilombolas communities in Brazil experience daily. This is because members of these communities are black, are mostly descendants of slaves, live marginally in society and live in rural areas and regions with the worst economic and social indicators in the country.
One of the great challenges of affirmative action for quilombolas is the development and implementation of policies that meet the specificities of these culturally different communities. Faced with mobilisation and demands for the rights of this segment of the population, since the 2000s, political coordination and regulatory bodies have been created to protect the rights of racial and ethnic groups and the black population(46). Actions include improving infrastructure, quality of life, local development and productive inclusion, which are coordinated mainly by the Brazil Quilombolas Program.
However, the current study revealed the low access of families to GP, especially rural development programmes. These government actions comprise some of the Brazil Quilombolas Program’s primary tools. They are related to the production and availability of food and are aimed at family farms. According to the law that established the guidelines of the National Family Agriculture Policy(47), quilombolas are recognised as beneficiaries of this programme, which indicates that they are an eligible population for GP whose target audience is family farmers. However, it has been questioned whether these programmes were designed to meet the specificities of quilombolas or for family farmers.
Food production and access to land are important factors for reducing the consequences of the high prevalence of moderate/severe FI among quilombolas since this group has previous knowledge and agricultural practices inherited from their families, which reinforces the importance of valuing these customs and agricultural practices(20). Thus, the current study emphasises the role of including more investments in social policies that integrate technology and rural development. It is expected that greater food production in the territories can increase family income and, thus, the circulation of money due to the sale and purchase of products from these areas, which will help reduce social vulnerabilities and FI and encourage autonomy and income generation.
There was good coverage of visits by community health agents, and this service was a protective factor against FI. These agents are fundamental in different cultural contexts, such as the investigated population(Reference Malta, Santos and Stopa48). In a study conducted with quilombolas from a community in the Northeast region, Amorim et al. (2013) observed that when someone fell ill, community agents were very much in demand and that most patients purchased medicines at health centres, reinforcing the importance of this system for this population(Reference Amorim, Tomazi and Silva49).
There was a low prevalence of access to the Family Health Strategy program; nevertheless, the families that accessed it had protection against moderate/severe FI. Thus, the study highlighted the importance of the actions of multiprofessional health teams in promoting quality of life and health. Therefore, it is possible that with increased access to these health programmes, FI could be reduced in households.
The food baskets programme distributes food to specific population groups that are in emergency situations (e.g. hunger and social vulnerability), and the Cisterns Program(Reference Monego, Peixoto and Cordeiro43) was developed to increase water access for families with low incomes in the semiarid Northeast region characterised by long periods of drought. The access of the entire population to a sufficient quality and quantity of food, including water, is a basic assumption of FNS(29). The low access to these programmes can be explained, first, by the lack of regular distribution of food baskets, the lack of clarity and periodicity in the distribution of baskets and the insufficient amount of food received by families(Reference Carvalho, Alberto and Pereira8,51) . Even so, access to food baskets was a protective factor for families with mild FI, which can be explained by the distribution of baskets affecting food security at home at a more immediate level.
Bolsa Família and the Continued Benefit Transfer program are not specific to quilombolas but are policies that guarantee FNS and must be associated with other policies for access to health, education, infrastructure and employment(Reference Silva, Medeiros and Martins7). To access Bolsa Família, it is necessary for the family to register in the cadastre for social programmes from the federal government and to comply with health and education conditions, such as monitoring the growth and development of children, keeping their vaccinations up to date and regularly attending school(52). However, the low infrastructure offered to the communities can make it difficult to comply with these conditionalities and, consequently, block the receipt of the benefits.
Families that accessed Bolsa Família were almost three times more likely to experience moderate/severe FI. In fact, the relationship between extreme poverty is strongly associated with severe levels of FI, as demonstrated by the literature(Reference Lignani, Palmeira and Antunes53). However, the household FI is not considered as an eligibility criterion for receiving the cash transfer in Brazil. The principal eligible criterion of Bolsa Família is the low monthly family income below the income cut-off point established by the programme(52), regardless of whether or not they are in severe forms of household FI. Therefore, considering the final adjusted model shown in Table 3, this article corroborated the focus of cash transfer between families with severe forms of FI, as observed in other studies(Reference Gubert, Segall-Corrêa and Spaniol6,Reference Palmeira, Bem-Lignani and Maresi54,Reference Raghunathan, Chakrabarti and Avula55) , such as observed among quilombolas. However, despite the current study being a cross-sectional study and the impossibility of assessing the longitudinal effect of Bolsa Família to reduce FI, it is worth considering that in a recent study carried out by Palmeira et al. (2020)(Reference Palmeira, Salles-Costa and Perez-Escamilla56), the authors observed the effect of the cash transfer in reducing FI among families with strong social vulnerability.
The government’s expectations and goals regarding policies were not met. In the data collection period, in 2011, the country was in a political, economic and social scenario marked by the encouragement of social policies aimed at FNS. However, since 2015, the Brazilian government has decreased investments in public policies to reduce FI in the country and to tackle extreme poverty(Reference Costa, Santos and Carvalho57), which may have mainly affected vulnerable populations such as quilombolas.
The current study has some limitations, the number of families varied for each social programme, which may have underestimated some associations. However, low access to GP should be considered, especially among those related to rural development. As for the population eligible for the Continued Benefit Transfer program, there is no information on which individuals had physical, mental or sensory disabilities, which can be considered a limitation of the study. Even so, only those who reported having access to the social programme were considered in the analysis. The lack of studies that investigate these communities makes it difficult to compare previous findings with our findings, and previous studies evaluated small samples or isolated quilombos (Reference Marques, Reichenheim and Moraes12–16). The Quilombolas Census investigated families that were owners of legalised territory and their rights; however, it did not analyse those without land titles that may have had the worst FI statuses and living conditions.
As this was a survey, it was not possible to assess the effectiveness of GP, since the best delineation for this type of investigation would consist of longitudinal data analysis, that is, the assessment of the level of household FI before and after the entry of families in GP whose goal is to reduce FI. Even so, considering that the Quilombolas Census has been the only national survey of FI in the quilombolas population with titled territories since its completion in 2011, it is worth considering the importance of the current study, even in light of its limit of not being able to assume the effectiveness of GP. We hope that our findings can contribute to the debate on racial inequality, FI and social exclusion and to mobilise new studies and more specific and effective GP for communities of descendants of enslaved blacks in Brazil.
Conclusions
Although Brazil is a pioneering country in its actions to confront FI, the scenario of social inequalities in relation to skin colour/race persists. The study’s findings reinforced the widespread racial inequalities in access to adequate food and the presence of hunger in addition to highlighting the low education, income and poor sanitation of the investigated families.
The inclusion of quilombolas families in GP was low, which indicated the need to evaluate and reformulate public policies to promote racial equality and social development and to fight hunger that meet the specificities of these people. Among the five programmes that involve the rural development area, only the Food Acquisition Program presented a significant association with protection against moderate/severe FI, as did the health GP that provided access to the Center for Family Health Support. The monitoring and evaluation of FNS indicators and continuing efforts to implement social programmes to fight hunger to reduce the chances of FI are necessary, especially in the current political and social context of the country.
Acknowledgements
Acknowledgements: The authors thank the organisations who have carried out the Quilombola Census, such as the Secretariat for Evaluation and Information Management of the Ministry of Social Development and Fight against Hunger, in partnership with the Secretariat for Policies for the Promotion of Racial Equality, Ministry of Health, Palmares Cultural Foundation and National Institute of Colonization and Agrarian Reform and the Center for Research, Information and Public Policies of Federal Fluminense University for fieldwork. Financial support: CCS Cherol was supported with scholarships by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). CAPES and CNPq had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: C.C.S.C. was responsible for the conception and development of the article, data analysis, interpretation of data and writing. A.A.F. was responsible for the conception and development of the article and writing. R.S.-C. was responsible for the conception and development of the article, data analysis, interpretation of data and writing. All authors approved the final version of the manuscript. Ethics human subject participation: According to resolution nº 510/2016 of the Brazilian Health Council, surveys that use information from a public domain database do not require registration or evaluation by the National Research Ethics Committee. Thus, ethical approval was not required for this paper. The study is based on secondary data analyses of unidentified public domain data collected through a national household sample survey.





