


Health promotion for couples includes the opportunity to use the partner’s support in encouraging healthy behaviours such as a balanced diet, weight control and physical activity(Reference Burke, Giangiulio, Gillam, Beilin and Houghton1, Reference Burke, Giangiulio, Gillam, Beilin, Houghton and Milligan2). Moreover, a dietary intervention programme may exert a beneficial effect on the participant’s spouse(Reference Burke, Mori, Giangiulio, Gillam, Beilin, Houghton, Cutt, Mansour and Wilson3–Reference Paisley, Beanlands, Goldman, Evers and Chappell7). Family environment also appears to significantly affect compliance(Reference Wens, Shepherd and Parchman8, Reference Schafer, Schafer, Dunbar and Keith9). As eating patterns are likely to be similar across family members(Reference Vauntheir, Lluch, Lecomte, Artur and Herbeth10, Reference Macario and Sorensen11), adherence and maintenance of certain eating patterns might be associated with the level of household support for healthy eating(Reference Wens, Shepherd and Parchman8, Reference Schafer, Schafer, Dunbar and Keith9). A combined worksite and family intervention is more successful in changing nutritional patterns than worksite intervention alone(Reference Sorensen, Stoddard and Peterson12–Reference Beresford, Thompson, Feng, Christianson, McLerran and Patrick14). This strategy might be a promising approach for long-term success in weight-loss programmes. However, few studies have explored the mutual effect of specific diet strategies on spouses.
In the 2-year Dietary Intervention Randomised Controlled Trial (DIRECT)(Reference Shai, Schwarzfuchs and Henkin15) among 322 participants, with dropout rates of 5 % after 1 year and 15 % after 2 years, we showed that the Low-carbohydrate and Mediterranean diets are effective alternatives to the Low-fat diet in terms of weight loss, achieving more favourable effects on lipids in the Low-carbohydrate diet and on glycaemic control in the Mediterranean diet. Here we describe a parallel study describing the 2-year effect of dietary intervention on weight and nutritional patterns of the spouses of the DIRECT participants across the three dietary arms. We further examined the association between a programme of spouse support, provided through periodic group meetings, and the success of the DIRECT participants in losing weight.
Methods
The DIRECT and DIRECT-Spouse study population
The DIRECT was conducted between July 2005 and June 2007 in a research centre workplace in the south of Israel. Participants (86 % of whom were men) were randomly assigned to one of three diets. The Low-fat diet(Reference Krauss, Eckel, Howard, Appel, Daniels and Deckelbaum16) aimed for 30 % of energy from fat, 10 % of energy from saturated fat and 300 mg cholesterol a day, with a total energy intake of 6276 kJ/d (1500 kcal/d) for women and 7531.2 kJ/d (1800 kcal/d) for men. The Mediterranean diet(Reference Willett and Skerrett17) aimed for 35 % of energy from fat, mainly from olive oil and nuts, and energy intake restricted to 6276 kJ/d (1500 kcal/d) for women and 7531.2 kJ/d (1800 kcal/d) for men. The Low-carbohydrate diet(Reference Atkins18) aimed for 20 g of carbohydrate daily for the induction phase (2 months), gradually reaching a specific target carbohydrate level that could maintain the weight loss. Total calories, protein and fat intake were not limited, although participants were counselled to prefer vegetarian sources and to avoid trans fat. The DIRECT-Spouse sub-study included wives of participants in the DIRECT, who share the same household but who were not part of the DIRECT themselves. The DIRECT-Spouse study was approved by the ethical committee of Soroka Medical Center.
Recruitment and follow-up of the study population
We invited the wives of participants in the DIRECT, and explained the theme and purpose of the sub-study. Those who agreed to participate filled out at baseline (August 2005) a baseline questionnaire that was sent to them personally, and included various demographic and lifestyle characteristics as well as questions regarding their predictions regarding the dieters’ success in the DIRECT. Wives were asked to also report their current weight.
Every 2 months during the first 6 months of the DIRECT, participating spouses were invited to a 90 min support group meeting led by a clinical dietitian specific to the DIRECT participant’s dietary arm. The curriculum of these meetings was similar in all groups and included various topics regarding the principles of the DIRECT intervention, learning about healthy nutrition and ways for leading a healthy lifestyle. The aim of the meetings was not to directly treat the spouses, but to update them about the principles of the diet strategy to which their husbands were randomised and to equip the spouses with materials that may enable the wives to support their husbands in their diet. The women were followed for changes of weight, diet and monthly expenses for food at 6 and 24 months.
Statistical analysis
One-way ANOVA and χ 2 tests were used to evaluate the demographic and lifestyle characteristics of the study population. We used non-parametric tests (Wilcoxon Signed test) to assess the weight changes within each dietary subgroup and non-parametric tests (Mann–Whitney test) to evaluate the differences between each group and the reference group (Low-fat diet). We evaluated weight changes of overweight spouses (n 40; BMI ≥ 25 kg/m2 at baseline) and compared weight loss across the diet groups using non-parametric tests (Mann–Whitney test). We further evaluated the correlation between weight changes of the DIRECT participants and their wives during the first 6 months, across the three dietary arms. In the DIRECT, we identified the first 6 months as the ‘maximal weight-loss phase’ and the 7–24 month period as the ‘maintenance’ phase(Reference Shai, Schwarzfuchs and Henkin15). To evaluate the impact of the spouse support group meetings, we compared the weight change of participants whose wives took part in the sub-study with that of DIRECT participants whose spouses did not take part in the study. The wives completed a food-changes questionnaire (FCQ)(Reference Shai, Henkin, Weitzman and Levi19) 6 months after baseline; we modified the 127-item Israeli FFQ, developed(Reference Shai, Vardi, Shahar, Azrad and Fraser20, Reference Shai, Shahar, Vardi and Fraser21) and validated(Reference Shai, Rosner, Shahar, Vardi, Azrad, Kanfi, Schwarzfuchs and Fraser22) in our Nutritional Center, to assess the changes of each food item among the wives, within the first 6 months of the DIRECT. In the FCQ, the spouses were asked whether their own consumption of each specific food item had changed (options: increased/did not change/decreased) since the beginning of the DIRECT. An increase in consumption of a specific food item was scored +1; a decrease in consumption of a specific food item was scored −1; no difference in consumption was scored 0. The scores were summed in each food group and divided by the number of items in the group; the results were used in the data analysis. All statistical analyses were performed with the use of SPSS statistical software, version 13 (SPSS Inc., Chicago, IL, USA). P value <0·05 was considered significant.
Results
Out of the 322 participants of the DIRECT, 90·5 % were married. Of the 113 wives who completed baseline questionnaires (38·8 % of spouses), seventy-four took part in support group meetings during the first 6 months of the DIRECT (n 28, 24 and 22 for the corresponding Low-fat, Mediterranean and Low-carbohydrate DIRECT participants’ diets). At baseline, their mean age was 50·79 years, and mean BMI was 26·6 (sd 4·72) kg/m2. The characteristics of the wives across the randomised assigned dietary arm of the DIRECT participants are described in Table 1. Characteristics were similar across groups. There were no significant differences between the baseline weights of the wives across the three dietary arms (P = 0·33). Furthermore, no significant differences in demographic characteristics, initial weight and weight loss after 6 months were found between wives who completed the 2-year follow-up and wives who did not (data not shown).
Table 1 Baseline characteristics of the wives of the DIRECT participants (n 74)

DIRECT, Dietary Intervention Randomized Controlled Trial.
*Kruskal–Wallis test for the continuous variables and χ 2 for the categorical variables.
†Physical activity = at least 30 min of vigorous activity a day.
After 6 months, the spouses of the DIRECT participants lost a mean of 2·64 kg (P = 0·002 compared to baseline). Weight loss (Fig. 1a) was 1·48 (sd 2·72) kg for wives of DIRECT participants randomised to the Low-fat diet, 2·30 (sd 2·39) kg for the Mediterranean and 4·62 (sd 6·56) kg for the Low-carbohydrate diet (P < 0·05 for all groups, compared to baseline).

Fig. 1 Weight changes in the Dietary Intervention Randomized Controlled Trial (DIRECT). (a) Changes in weight of wives of participants after 6 months, by randomised dietary arm. Values are means, with an se of 1 from the mean indicated by error bars. *n 74, P < 0·05 within diet group, Wilcoxon Signed Ranks Test, as compared to time 0; **P < 0·06 in the Mediterranean or Low-carbohydrate diet group, as compared to the traditional diet Low-fat diet group. (b) Correlation between weight changes among DIRECT participants and their wives after 6 months: (![]() , Low-fat diet group (n 27, r = 0·418, P = 0·842);
, Low-fat diet group (n 27, r = 0·418, P = 0·842); ![]() , Low-carbohydrate diet group (n 22, r = 0·566, P = 0·005);
, Low-carbohydrate diet group (n 22, r = 0·566, P = 0·005); ![]() , Mediterranean diet group (n 23, r = 0·322, P = 0·16)
, Mediterranean diet group (n 23, r = 0·322, P = 0·16)
We compared the results of the alternative diets (Mediterranean and Low-carbohydrate) to the traditional diet (Low-fat). Weight loss among wives whose husbands were in the Mediterranean diet group (P = 0·064) and the Low-carbohydrate diet group (P = 0·058) tended to be greater, compared to the Low-fat diet-group. Overall, there was significantly greater weight loss among the spouses of the husbands in the two alternative diet-groups combined (Mediterranean + Low-carbohydrate), compared to the traditional Low-fat diet (P = 0·031). Wives’ BMI decreased significantly after 6 months (ΔBMI = 0·80 (sd 1·91) kg/m2; P = 0·001 compared to baseline), with ΔBMI of 0·46 (sd 1·03), 0·62 (sd 1·06) and 1·47 (sd 3·16) kg/m2 for wives of participants randomised to the Low-fat, Mediterranean and Low-carbohydrate groups, respectively (P = 0·013, 0·024 and 0·059, respectively, compared to baseline).
Overall weight loss at 6 months among the overweight spouses (n 40) with BMI ≥ 25 kg/m2 at baseline (mean BMI = 29·5 (sd 4·04) kg/m2) was 3·54 kg (sd 5·14) (P < 0·05 compared to baseline). For the corresponding Low-fat, Mediterranean and Low-carbohydrate dietary arms, weight loss of overweight spouses was 1·75 (sd 3·19), 2·96 (sd 2·58) and 5·36 (sd 7·45) kg, respectively (P = 0·068 (n 12), P = 0·08 (n 14) and P = 0·042 (n 14), respectively, compared to baseline).
A significant correlation (Fig. 1b) was found between weight changes of the seventy-four DIRECT participants and their wives during the first 6 months of the intervention (r = 0·42; P < 0·001). The strongest and only statistically significant correlation was for the Low-carbohydrate diet group (r = 0·57; P = 0·005).
The 6-month weight changes among the seventy-four DIRECT participants whose wives took part in the group sessions was −5·15 kg, compared to the −3·54 kg among the 248 DIRECT participants whose spouses did not take part in these sessions (P = 0·020).
We analysed the changes in the wives’ diets (Fig. 2). In all three groups the wives reported lower consumption of saturated fat and trans fat, meat and poultry, bread and pastry, grains, pasta and potato, fruit, sweets and sweetened beverages. In all three groups the wives reported an increased consumption of fish and vegetables. There was a significantly larger decrease in the consumption of grains, pasta and potatoes among wives whose husbands were on the Low-carbohydrate diet, compared to the Low-fat diet (P = 0·013). Similar trends were reported at 24 months.
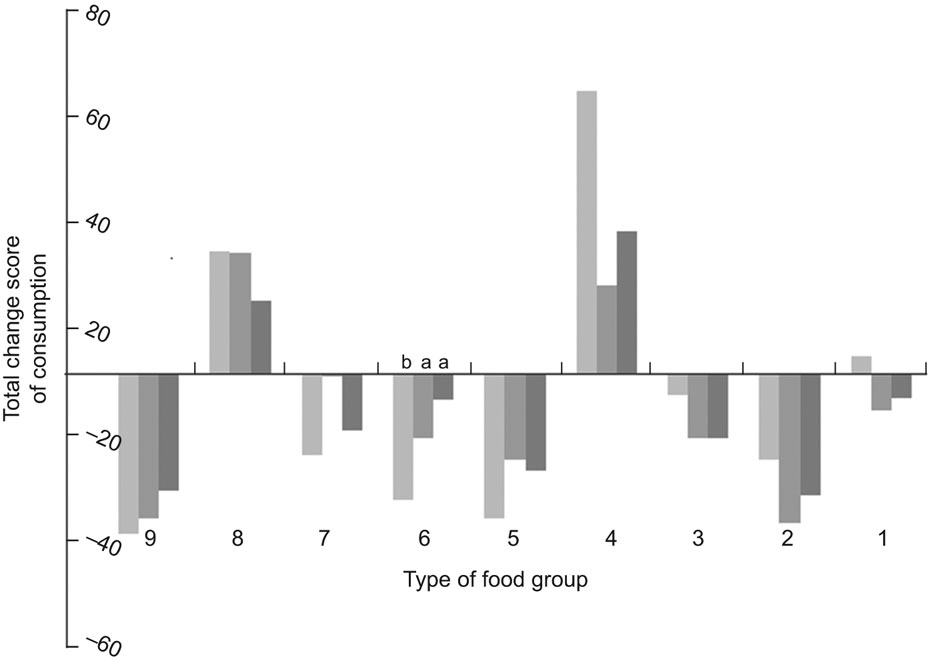
Fig. 2 Changes in nutritional patterns after 6 months among wives (n 74) of participants in the Dietary Intervention Randomized Controlled Trial (DIRECT), by randomised dietary arm: ![]() , Low-fat (n 28);
, Low-fat (n 28); ![]() , Mediterranean (n 24);
, Mediterranean (n 24); ![]() , Low-carbohydrate (n 22). Food groups: 1 = eggs and dairy, 2 = saturated fat and trans fat, 3 = meat and poultry, 4 = fish, 5 = bread and pastry, 6 = grains, pasta and potato, 7 = fruit, 8 = vegetables, 9 = sweets and sweet beverages. The score was calculated for each food item as follows: ‘Increased’ = +1, ‘Decreased’ = −1, ‘No change’ = 0. The score for each food group is the sum of all food items in the specific group divided into the number of food items in the food group according to the food change questionnaire, then divided according to the ‘n’ of each dietary arm, so each score represents the percentage of change. a,bValues for two diet groups within a row with unlike superscript letters were significantly different (P < 0·05)
, Low-carbohydrate (n 22). Food groups: 1 = eggs and dairy, 2 = saturated fat and trans fat, 3 = meat and poultry, 4 = fish, 5 = bread and pastry, 6 = grains, pasta and potato, 7 = fruit, 8 = vegetables, 9 = sweets and sweet beverages. The score was calculated for each food item as follows: ‘Increased’ = +1, ‘Decreased’ = −1, ‘No change’ = 0. The score for each food group is the sum of all food items in the specific group divided into the number of food items in the food group according to the food change questionnaire, then divided according to the ‘n’ of each dietary arm, so each score represents the percentage of change. a,bValues for two diet groups within a row with unlike superscript letters were significantly different (P < 0·05)
After 2 years, weight changes among fifty-three wives were +0·39 (sd 3·71) kg among wives of husbands in the Low-fat group (n 24; P = 0·453, compared to baseline), −3·00 (sd 6·21) kg among wives of husbands in the Mediterranean group (n 14; P < 0·05, compared to baseline) and −2·30 (sd 2·39) kg among wives of husbands in Low-carbohydrate group (n 15; P < 0·05, compared to baseline). Overall, the significantly greater weight loss among spouses of participants in the two alternative diet groups combined (Mediterranean + Low-carbohydrate), compared to the traditional Low-fat diet, remained after 2 years (P = 0·034). For DIRECT participants randomised to the Low-fat, Mediterranean and Low-carbohydrate diets, adherence rates at 2 years were 85·7 %, 58·4 % and 68·2 % (P < 0·05 between groups). However, spouse populations across the three dietary arms were likely to be similar in baseline characteristics such as weight, education, origin, smoking and physical activity patterns.
The baseline questionnaire included a question ‘Regarding the possibility of your husband succeeding and maintaining his diet throughout the DIRECT’ (scale from 1 – don’t agree to 5 – fully agree). An affirmative answer was a significant predictor for the DIRECT participant’s success in losing weight during the first 6 months of the intervention (β = 0·24; P = 0·046).
In the follow-up questionnaires, wives were asked whether their household expenses for food products increased, did not change, or decreased as a result of their husbands’ diet. The proportions of wives who reported an increase in monthly food expenses were 25·9 % for Low-fat, 26·1 % for Mediterranean and 14·3 % for Low-carbohydrate (P = 0·68). The rest reported no change.
Discussion
We evaluated the effect of the DIRECT study on weight loss and nutritional patterns of wives of participants. We found that wives were indirectly affected by the intervention trial of their husbands, by losing weight and improving their nutritional patterns. Overweight spouses at baseline experienced more weight loss. The results suggest that a dietary intervention delivered to one family member may have a beneficial effect on the spouse, and may present a possible ripple effect that may occur as a result of minimal involvement in a weight-loss programme targeting one’s spouse. This may provide additional justification for health promotion and dietary modification programmes to target couples as the unit for intervention, as a shared activity.
Our study has several limitations. First, the weight and height of the spouses were self-reported and not directly measured, as was done with DIRECT participants; although this may introduce a possible bias, other studies have previously validated self-reported weights(Reference Rimm, Stampfer, Colditz, Chute, Litin and Willett23, Reference Weaver, Kushi, McGovern, Potter, Rich, King, Whitbeck, Greenstein and Sellers24). Second, the assignment of the spouses study was not randomised and was based on the willingness of the wife to participate. It is possible that these wives were more supportive of their husband’s weight-loss efforts than spouses who were unwilling to attend group meetings themselves or complete assessments, likely introducing a self-selection bias. Third, we followed wives only, due to the small proportion of women participating in the DIRECT. The influence of a dietary intervention on spouses of both sexes should be further investigated. Strengths of our study include the long duration of follow-up, the comparison of the three diet strategies and the close connection our clinical dietitian had with the wives, enabling close follow-up.
Low-carbohydrate diets without energy restriction have earlier been shown to be at least as effective as low-fat, high-carbohydrate diets in inducing weight loss, and were more favourable in overall metabolic outcomes(Reference Shai, Schwarzfuchs and Henkin15, Reference Dansinger25–Reference Stern, Iqbal, Seshadri, Chicano, Daily, McGrory, Williams, Gracely and Samaha27). The strongest correlation between the weight loss of the DIRECT participants and the weight loss of their spouses was found in those randomised to the Low-carbohydrate diet. The changes in nutritional patterns were in accord with the principles of the three diet strategies of the DIRECT participants(Reference Shai, Schwarzfuchs and Henkin15, Reference Stern, Iqbal, Seshadri, Chicano, Daily, McGrory, Williams, Gracely and Samaha27–Reference Samaha, Iqbal, Seshadri, Chicano, Daily, McGrory, Williams, Williams, Gracely and Stern29), and present the possible ripple effect of the trial on the spouses who reported changing their own eating habits. The DIRECT study(Reference Shai, Schwarzfuchs and Henkin15) found that the Mediterranean and Low-carbohydrate diets may be effective strategies in losing weight and maintaining weight loss. Moreover, it was suggested that these diets might be used as specific prescriptions for certain metabolic targets. The findings among the wives suggest that these two alternative diets may also be adapted by spouses as well as the traditional diet and, therefore, may be considered as suitable effective alternative strategies for couples that undertake a joint diet.
DIRECT participants whose spouses took part in the support group meetings lost significantly more weight than the DIRECT participants whose spouses did not participate. Although the present study was not randomised and therefore one may argue that it is hard to use these data to conclude the benefit of involving the spouse in order to raise the participants’ success in a dietary intervention, these data are consistent with earlier studies that found that a family intervention was more successful in changing eating patterns than worksite intervention alone(Reference Sorensen, Stoddard and Peterson12, Reference Sorensen, Hunt and Cohen13). Moreover, we found that a wife believing in her husband’s ability to succeed in his weight-loss project was a significant predictor for the dieter losing weight during the first 6 months of the intervention. These findings suggest a positive relationship between the involvement of the spouse in the intervention and success in weight loss; such findings are consistent with earlier data which recognised social and family support as factors that may raise adherence and encourage health behaviour change in high-risk individuals(Reference Bovbjerg, McCann and Brief5, Reference Wens, Shepherd and Parchman8) and a recent study reporting the significant role played by the spouse in encouraging the dieter in succeeding in his diet(Reference Paisley, Beanlands, Goldman, Evers and Chappell7).
Our results suggest an approach of designing dietary intervention programmes that focus on the workplace as well as on the household.
Acknowledgements
The present study was funded by the following sources: (i) Nuclear Research Center Negev (NRCN); (ii) The Dr. Robert C. and Veronica Atkins Research Foundation; (iii) The S. Daniel Abraham International Center for Health and Nutrition, Ben-Gurion University, Israel. The first two funding sources were not involved in any stage of the design, conduct or analysis of the study, and had no access to the study results before publication. The authorship responsibilities were as follows: study design and performance – R.G., D.S., M.J.S. and I.S.; data analysis – R.G.; paper drafting – R.G.; paper review – D.S., M.J.S. and I.S. None of the authors have relationships with companies that make products relevant to the manuscript. The authors are thankful to the 322 DIRECT participants for their consistent cooperation.



