


Vegetables are rich in nutrients, dietary fibre and phytochemicals, and likely have protective effects against obesity, CVD, multiple cancers and other chronic diseases among children and adults( Reference Boeing, Bechthold and Bub 1 – 8 ). In addition, higher diet quality, including increased consumption of vegetables, has been associated with improved academic performance in children( Reference Florence, Asbridge and Veugelers 9 ). Consuming vegetables is an important part of a healthy diet and lifestyle, yet levels of vegetable consumption are generally low, below dietary recommendations( 10 , Reference Krebs-Smith, Guenther and Subar 11 ). The estimated percentages of young children not meeting recommended levels of total vegetable intake were high according to 2001–2004 national data: 80·3 % of children aged 2–3 years and 92·0 % of children aged 4–8 years had inadequate vegetable intake( Reference Krebs-Smith, Guenther and Subar 11 ).
Establishing vegetable intake early in life is important, especially because vegetable and other food consumption patterns in childhood track into adolescence and adulthood( Reference Cutler, Flood and Hannan 12 – Reference Singer, Moore and Garrahie 14 ). Development of young children’s dietary behaviours is partly influenced by parents and their parenting practices( Reference Nicklas, Baranowski and Baranowski 15 – Reference O’Connor, Hughes and Watson 17 ), yet many parents of pre-school children report challenges to getting their child to eat vegetables. Some challenges include availability, cost barriers and negative parenting practices( Reference Cullen, Baranowski and Rittenberry 18 ). Specifically, behaviours that parents use to influence a child’s long-term vegetable intake are vegetable parenting practices and have been classified as effective or ineffective based on professional judgement of long-term vegetable consumption( Reference O’Connor, Watson and Hughes 16 ). Recent research confirmed separate vegetable parenting practices dimensions for effective and ineffective vegetable parenting practices( Reference Baranowski, Chen and O’Connor 19 ), suggesting the importance of promoting parents’ use of effective vegetable parenting practices (EVPP) while reducing use of ineffective vegetable parenting practices( Reference Baranowski, Beltran and Chen 20 , Reference Baranowski, Beltran and Chen 21 ). EVPP are vegetable intake-related parenting practices that provide structure, non-directive control and are responsive; examples include praising a child when he/she eats vegetables (responsiveness), eating together as a family (structure) and allowing a child to self-serve vegetables (non-directive control)( Reference O’Connor, Watson and Hughes 16 ). Parental feeding structure, control and responsiveness categories were conceptualized based on the general parenting style paradigm( Reference Darling and Steinberg 22 – Reference Slater and Power 24 ) to provide a comprehensive taxonomy of parents’ role in children’s eating( Reference Hughes, O’Connor and Power 25 ). Understanding EVPP use could inform future interventions and research.
Behavioural theories provide a framework for understanding and systematically studying feeding behaviours( Reference Cerin, Barnett and Baranowski 26 , Reference Shaikh, Yaroch and Nebeling 27 ). Specifically, the Model of Goal Directed Vegetable Parenting Practices (MGDVPP) provides a useful model for understanding and predicting parenting practices shown to encourage pre-school children’s vegetable intake( Reference O’Connor, Hughes and Watson 17 , Reference Baranowski, Beltran and Chen 20 , Reference Baranowski, Beltran and Chen 21 , Reference Baranowski, Beltran and Chen 28 , Reference Hingle, Beltran and O’Connor 29 ). Based on the Model of Goal Directed Behavior and Self-Determination Theory, MGDVPP was adapted for vegetable parenting practices (see Fig. 1)( Reference Hingle, Beltran and O’Connor 29 ). The Model of Goal Directed Behavior is an expansion of the Theory of Planned Behavior, adding ‘anticipated emotions’ as a psychosocial predictor and inserting ‘desire’ between the psychosocial predictors (i.e. attitudes, subjective norms, perceived behavioural control and anticipated emotions) and ‘intention’( Reference Bagozzi, Baumgartner and Pieters 30 – Reference Taylor, Bagozzi and Gaither 33 ). As originally in the Theory of Planned Behavior, there is then a possible direct effect of perceived behavioural control on behaviour( Reference Ajzen 34 ). Intention is hypothesized to also lead to actual behavioural performance( Reference Ajzen 35 ), although there has been evidence of an intention–behaviour gap( Reference Rhodes and Dickau 36 – Reference Sniehotta, Scholz and Schwarzer 38 ). With the extra constructs, the Model of Goal Directed Behavior has shown enhanced behaviour predictiveness over the Theory of Planned Behavior( Reference Bagozzi, Baumgartner and Pieters 30 – Reference Taylor, Bagozzi and Gaither 33 ). In addition, because desires embody intrinsic motivation, Self-Determination Theory constructs that contribute to intrinsic motivation (i.e. autonomy, competence/self-efficacy and relatedness)( Reference Ryan and Deci 39 ) were added to the Model of Goal Directed Behavior to directly predict desire. Lastly, habit (or automated behaviour) and barriers to performing a behaviour are related to behaviour( Reference De Bruijn, Keer and Conner 40 , Reference Lytle, Varnell and Murray 41 ), and thus were added to enhance predictiveness of EVPP.
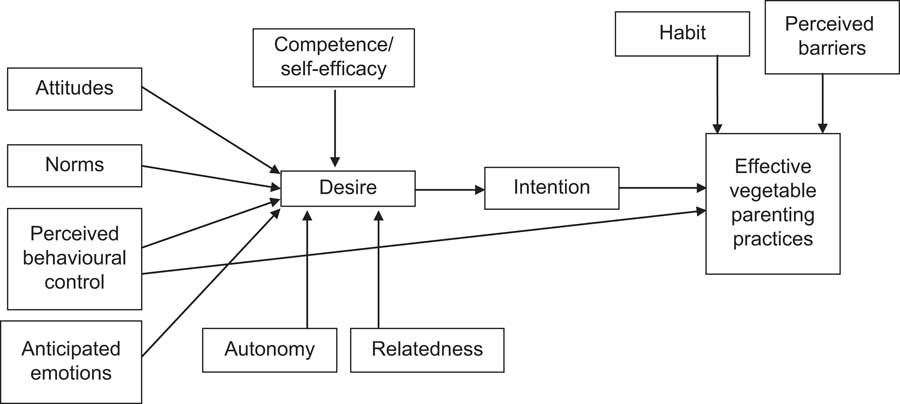
Fig. 1 Hypothesized path model of goal-directed vegetable parenting practices
The present study explored and reported the modelling of EVPP using MGDVPP constructs: intention, desire (intrinsic motivation), perceived barriers, autonomy, relatedness, self-efficacy, habit, anticipated emotions, perceived behavioural control, attitudes and norms. The authors hypothesized MGDVPP constructs to be predictive of EVPP and thereby provide a good model for understanding and predicting parenting practices that are believed to effectively encourage a pre-school child’s vegetable intake. There is no other known model to predict EVPP. If shown to be predictive, the MGDVPP may inform future interventions that help parents adopt effective behaviours for encouraging their child’s vegetable intake.
Methods
Study sample
In 2009, 406 parents initiated an Internet survey assessing their level of agreement with the EVPP and MGDVPP items. Respondents were parents of a child of pre-school age and were recruited through multiple methods, including a notice posted in the Children’s Nutrition Research Center newsletter and the Baylor College of Medicine volunteer website; fliers posted at the Texas Medical Center, public libraries and YMCA; and personal emails to Children’s Nutrition Research Center volunteers. A more detailed description of recruitment methods is available elsewhere( Reference Baranowski, Chen and O’Connor 19 – Reference Baranowski, Beltran and Chen 21 , Reference Baranowski, Beltran and Chen 28 ).
For the present study, only respondents with complete surveys were included in the analyses. Six participants with any missing demographic information were also excluded from the final analyses, making the final sample size n 307. Because demographic questions were included at the end of the survey, no information was available to compare the participants who completed the survey with those who did not. In addition, the authors assumed that (i) if a respondent had more than one child, he/she chose one child and answered questions accordingly and (ii) multiple respondents did not answer separate surveys for the same child. The authors removed duplicates based on IP and email addresses listed, but it is possible that more than one parent completed surveys for the same child from different IP addresses or using different emails.
The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Baylor College of Medicine Institutional Review Board. All participants provided informed consent and were offered a $US 20 gift card upon completion of the survey.
Measures
Respondents completed 227 items related to demographics, MGDVPP scales (i.e. intention, desire (intrinsic motivation), perceived barriers, autonomy, relatedness, self-efficacy, habit, anticipated emotions, perceived behavioural control, attitudes and norms) and EVPP scales. Demographic questions included child age, child gender, parent gender, parent race/ethnicity, highest household educational attainment and annual household income (Table 1). MGDVPP items were generated from intensive qualitative interviews with parents of pre-school children about their motivations to use vegetable parenting practices; details of these interviews have been published( Reference Hingle, Beltran and O’Connor 29 ). Table 2 provides a listing of MGDVPP and EVPP scales, subscales, number of items, means and standard deviations, range of possible scores, Cronbach’s α values and bivariate correlations with EVPP.
Table 1 Demographic characteristics of the study participants: parents (n 307) of pre-school chldren, Houston, TX, USA
Table 2 Model of Goal Directed Vegetable Parenting Practices scales and subscales
EVPP, effective vegetable parenting practices.
*P<0·05, ***P<0·001.
The dependent variable was a composite EVPP scale, obtained by summing the values of fourteen items that loaded on to a second-level EVPP factor in a confirmatory factor analysis described elsewhere( Reference Baranowski, Chen and O’Connor 19 ). Items were generated from health professionals’ and dietetics practitioners’ responses to an Internet survey( Reference O’Connor, Watson and Hughes 16 ). Acceptable fit was obtained for the EVPP scale( Reference Baranowski, Chen and O’Connor 19 ).
Details about the EVPP and MGDVPP scales, including item generation and psychometric properties of the scales, have been published( Reference Baranowski, Chen and O’Connor 19 – Reference Baranowski, Beltran and Chen 21 , Reference Baranowski, Beltran and Chen 28 ). Exploratory and confirmatory factor analyses revealed multiple dimensions were necessary to fit most MGDVPP scales’ items( Reference Baranowski, Beltran and Chen 28 ). Tests of construct validity showed that almost all MGDVPP scales (86·2 %) bivariately correlated with composite EVPP or ineffective vegetable parenting practices scales; specifically, fifteen of twenty-nine scales (or 51·7 %) correlated with EVPP. In addition, internal consistency reliability coefficients for MGDVPP subscales ranged from 0·13 to 0·92, with a majority being 0·70 or higher (see Table 2). Many of the subscales with lower reliability coefficients (i.e. below 0·70) comprised only three or four items( Reference Hinkin 42 ). However, these shorter subscales had acceptable average inter-item correlations above 0·20( Reference Clark and Watson 43 ), an alternative reliability indicator for scales with few items( Reference Baranowski, Beltran and Chen 28 , Reference Clark and Watson 43 ).
Analytical methods
The present study involved descriptive statistics and block regression modelling, using the composite score of the EVPP scales as the dependent variable and MGDVPP subscales as predictor variables in separate and sequential blocks. Variance inflation factor and tolerance for each predictor were used to test potential collinearity. Predictors with a variance inflation factor above 10 or a tolerance below 0·10 may merit further investigation( Reference Kutner, Nachtsheim and Neter 44 ).
Modelling started with demographics (i.e. child age, child gender, highest household educational attainment, annual household income and parent race/ethnicity), followed by the intention subscales, desire (intrinsic motivation), perceived barriers, autonomy, relatedness, self-efficacy, habit, anticipated emotions, perceived behavioural control, attitudes and lastly norms. Demographic variables were entered first to understand the extent of their influence without any MGDVPP subscales; thus, the variance due to subsequent MGDVPP subscales would predict variance beyond demographics. Because, theoretically, intentions are the most proximal to behaviour and should be the strongest predictor, they were added next. Variables were then added in order of distance from behaviour – from most proximal to least proximal. Habit subscales were entered relatively late in the testing sequence to prevent drowning out other predictors. All demographic variables remained in all models, but backward deletion was employed at the end of each block entry for any other variables not related to the outcome variable at P<0·10. For the final model, any variables not related to the outcome variable at P<0·05 were deleted. All analyses were performed using the statistical software package SAS version 9·3.
Results
Study sample
Most respondents were female (89·3 %), had a male child (53·1 %), were a college graduate (64·5 %) and had an annual household income of at least $US 60 000 (54·1 %; Table 1). There was representation from the major racial and ethnic groups in Houston, TX, including White (37·1 %), Black/African American (19·5 %), other (19·2 %), Asian (14·0 %) and Hispanic (10·1 %). Most respondents (91·5 %) classified as ‘other’ were of multiple races/ethnicities.
Predictors of effective vegetable parenting practices
All tolerance values were greater than 0·10 and variance inflation factor values were less than 10, so there was no problem with collinearity in the data. The strongest predictor of EVPP use was the habit of active child involvement in vegetable selection (β=0·430, P<0·001), followed by habit of positive vegetable communications (β=0·217, P<0·001), barrier of respondent not liking vegetables (β=0·173, P<0·001), perceived behavioural control of positive influence on vegetable consumption (β=–0·147, P=0·001) and habit of positive vegetable environment (β=0·118, P=0·020; Table 3). Of all these predictors, perceived behavioural control of positive influence on vegetable consumption was the only variable negatively related to EVPP. None of the demographic characteristics, intention subscales, intrinsic motivation subscales, autonomy subscales, relatedness subscales, self-efficacy subscales, anticipated emotions subscales, attitudes subscales or norms subscales was significantly related to EVPP use. All related variables produced a final model with an adjusted R 2 of 0·486.
Table 3 Block regression modeling results using the Model of Goal Directed Vegetable Parenting Practices to predict effective vegetable parenting practices
The reference category for child gender is girl; for highest household educational attainment is postgraduate study; for annual household income is ≥$US 60 000; and for parent race/ethnicity is White.
*P<0·05, **P<0·01, ***P<0·001.
Discussion
The current study was the first to test scales to predict EVPP use. The R 2 for the final model (0·486) indicated almost half the variability in EVPP use was explained by the demographic variables, intention subscales, desire (intrinsic motivation), perceived barriers, autonomy, relatedness, self-efficacy, habit, anticipated emotions, perceived behavioural control, attitudes and norms. This suggests the final model used constructs important in predicting EVPP use, even though some of these constructs were from subscales with low internal consistency reliabilities.
The strongest predictor of EVPP use was the parent’s habit of active child involvement in vegetable selection (e.g. automatically asking the child to help select vegetables at the grocery store), followed by habit of positive vegetable communications (e.g. automatically praising the child when the parent sees him/her eating vegetables) and habit of positive vegetable environment (e.g. automatically including vegetables with most meals)( Reference Baranowski, Beltran and Chen 28 ). These three habit subscales are considered effective practices themselves because they provide structure, non-directive control and are responsive( Reference O’Connor, Watson and Hughes 16 ). If parents had effective vegetable-related habits around their children, they reasonably would also employ effective practices to encourage their child’s vegetable consumption. Thus consistent with research on habit( Reference Gardner, Bruijn and Lally 45 ), effective parenting habits( Reference Baranowski, Chen and O’Connor 19 ) strongly predicted use of EVPP.
Perceived behavioural control of positive influence on vegetable consumption had a negative relationship with EVPP. Thus, the easier parents perceived it was to have a positive influence on their child’s vegetable consumption, the less likely the parents were to use EVPP, contradicting what might be expected. The items that highly loaded on this perceived behavioural control subscale identified parent’s perception of how easy it is to get the child to eat more vegetables by asking the child to select vegetables at the grocery store, showing the child they (the parents) enjoy eating vegetables or asking the child to help with vegetable preparations. These items themselves are considered effective parenting practices( Reference Baranowski, Chen and O’Connor 19 ), yet were negatively related to EVPP use in the present study. Perhaps, if a parent finds these parenting practices too easy, he/she may believe they are not effective and therefore not employ them.
The last subscale to be related to EVPP use was the barrier of the respondent (parent) not liking vegetables: the higher the barrier score, the more likely a parent was to use EVPP. The three most highly loaded items on this barrier subscale included the parent not liking vegetables, no one in the family eating vegetables and the parent not liking the taste of vegetables( Reference Baranowski, Beltran and Chen 28 ). While this is contrary to expectations, perhaps parents who did not like vegetables themselves still appreciated the benefits of vegetables and were motivated to obtain the benefits for their child, using effective practices to encourage their child’s vegetable consumption.
Many of the subscales were not statistically significant predictors of EVPP use. For example, intention did not predict EVPP use, as might have been expected based on past literature( Reference Loth, MacLehose and Fulkerson 46 ), but this finding supports other research suggesting an intention–behaviour gap and the weak (or possibly missing) relationships between intention and behaviour( Reference Rhodes and Dickau 36 – Reference Sniehotta, Scholz and Schwarzer 38 ). It is also possible that respondents interpreted the intention of future vegetable parenting practices behaviour to indicate a change in their current practices, and if they were already performing EVPP, the lack of relationship could be understood. In addition, no demographic variables were related to EVPP. Past research showed parents in racial/ethnic minority subgroups, with less than high-school education and with low household income used more controlling food-related parenting practices( Reference Loth, MacLehose and Fulkerson 46 ). Another study found contradicting results regarding education levels: higher levels of maternal education were associated with higher use of controlling feeding practices( Reference Saxton, Carnell and van Jaarsveld 47 ). These control scales included primarily the ineffective control vegetable parenting practices, such as restriction or pressure to eat. The current composite indicators of EVPP in the present study included non-directive control (an effective form of control), responsiveness and structure items, suggesting there may be no relationship of socio-economic status to EVPP. The generally higher socio-economic status of the current sample may also have influenced the lack of relationships. Future research will need to assess when and how socio-economic status influences parenting practices.
Although not investigated in the current study, reducing ineffective vegetable parenting practices is also important to consider for a child’s long-term vegetable consumption. Described elsewhere( Reference Baranowski, Beltran and Chen 20 , Reference Baranowski, Beltran and Chen 21 ), ineffective practices include exerting dominance or restrictive feeding, and may be related to obesity( Reference Morawska and West 48 ). The predictors of ineffective vegetable parenting practices( Reference Baranowski, Beltran and Chen 20 , Reference Baranowski, Beltran and Chen 21 ) differed from predictors of EVPP, so both may be important in future research and practice.
Despite using a broad theoretical framework and validated variables, there are some limitations of the current study. First, the study had a cross-sectional design, which precludes inferences of causality and temporal relationships( Reference Carlson and Morrison 49 , Reference Noordzij, Dekker and Zoccali 50 ). Although there were relationships among MGDVPP constructs and EVPP use, the authors could not conclude that certain constructs caused others. Second, data were not collected on actual vegetable consumption, so the authors could not assess relationships between EVPP and vegetable intake and could not verify findings from another study on parenting practices and vegetable consumption( Reference O’Connor, Hughes and Watson 17 ). Third, because data came from a survey using self-reported measures, they were subject to self-report bias. Relatedly, there may have been self-selection bias of those who agreed to participate. Compared with the population of Houston( 51 ), the current sample included families with higher educational attainment, higher household income than Houston’s median household income and less Hispanic representation; thus, findings cannot be generalized to the population of Houston or to other populations. Lastly, in the current study the authors removed duplicates based on IP and email addresses, and thus assumed that a child was represented only once in the data set, but it is possible that multiple respondents answered separate surveys for the same child. These limitations in design may have contributed to some of the unexpected study findings, such as the higher socio-economic status of participants masking relationships between demographics and EVPP or the cross-sectional nature of the study precluding detection of relationships with future parenting practices. Future research should obtain more diverse samples and use objective measures in a longitudinal design.
Conclusions
The present study contributes to current research regarding vegetable parenting practices using a theoretical framework by testing the MGDVPP and its scales (i.e. intention, desire (intrinsic motivation), perceived barriers, autonomy, relatedness, self-efficacy, habit, anticipated emotions, perceived behavioural control, attitudes and norms) to predict EVPP use. Further research is needed to expand the items in some of the scales to increase the internal consistency reliabilities and assess their predictiveness in longitudinal designs with more diverse samples.
Second, findings have implications for future interventions. Basing dietary interventions on behavioural theory may enhance outcome effectiveness for vegetable consumption( Reference Diep, Chen and Davies 52 ). To increase EVPP use, an intervention would need to target increasing habit( Reference Baranowski 53 ). Future research should employ these scales to assess their utility for documenting parenting and psychosocial change in evaluating EVPP interventions. Innovative interventions targeting these scales may lead to increased EVPP use and ultimately may lead to increased vegetable intake among children.
Acknowledgements
Financial support: This research was funded by the National Institute of Child Health and Human Development (grant number HD058175). This work is a publication of the United States Department of Agriculture (USDA/ARS) Children's Nutrition Research Center, Department of Pediatrics, Baylor College of Medicine, Houston, Texas, and was funded in part with federal funds from the USDA/ARS under Cooperative Agreement No. 58-6250-6001. The contents of this publication do not necessarily reflect the views or policies of the USDA, nor does mention of trade names, commercial products or organizations imply endorsement from the US government. C.S.D. was supported fully by a Primary Care Research Training Grant from National Research Service Award (#T32 HP10031). No funder had a role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: C.S.D. participated in review of analyses and wrote the first draft of the manuscript. A.B. was the project manager. T.-A.C. was the data manager and statistician. D.T., T.O. and S.H. contributed conceptually to the measures. J.B. was the project coordinator. T.B. was principal investigator for the overall project. All authors reviewed, critiqued and approved this manuscript. Ethics of human subject participation: The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Baylor College of Medicine Institutional Review Board.




