


Malnutrition is a public health problem among low-income families in Iran( 1 , Reference Sheikholeslam, Naghavi and Zarati 2 ). To deal with this problem, a multidisciplinary programme was initiated in 2005 to improve the nutritional status of children under 5 years of age. This programme is led mainly by the Department of Community Nutrition of the Ministry of Health and Medical Education and has two major sections, namely collaborative and supportive. The collaborative section has an intersectoral approach with some ongoing parts that are not included in our discussion.
The supportive section has a targeted approach and its main goal is to improve food intake and weight status of malnourished or growth-retarded children in poor families who were suffering from nutritional deficiencies. Supplementary food was distributed as foods or food vouchers according to programme instructions. Weight and height of the children were measured based on the national Integrated Management of Childhood Illness protocol through growth monitoring visits( 3 , Reference Mason 4 ). The supplementary food was funded and provided by the Imam Khomeini Relief Foundation (IKRF). The protection and relief of poor and deprived families is the main responsibility of this organization. This programme was implemented through the primary health-care network of Iran. The food basket was valued at $US 16 per child per month.
The current study is part of the first comprehensive evaluation of the national, community-based, food supplementary programme in Iran which was carried out in 2014. The present paper reports findings on process evaluation concerning the extent to which the supportive section of the programme was implemented as intended and received by the recipients.
Methods
Study design and setting
The process evaluation was carried out using qualitative and quantitative methods from March to September 2014 in Qazvin and Semnan provinces of Iran.
Data sources
Document reviews
Data on the contents of the food basket, which was designed by the Nutrition Department in the deputy of health within each of the two provinces, were collected through reviewing available documents. Children’s health files in health houses/centres were also reviewed to determine whether mothers/caregivers had attended training classes on child nutrition, feeding practices and child growth monitoring.
Survey
The sample size with a power of 90 %, an expected risk ratio equal to 2·5 and at 5 % significance level was calculated to be 324. Assuming a 10 % dropout, a total of 362 children under 6 years of age were selected by multistage random sampling (details of sampling are provided elsewhere)( Reference Ghodsi, Omidvar and Eini-Zinab 5 , Reference Ghodsi, Omidvar and Rashidian 6 ). Health houses/centres in each urban/rural area were selected randomly. In the last stage, children were randomly selected from the list of malnourished or growth-retarded children under the coverage of the programme. In each stage, samples were selected by probability proportional to size. The study was carried out from June to September 2014. Data were obtained from mothers/caregivers who were invited by community health workers (CHW) and agreed to participate in the study.
A list of food and non-food items received by families within the last two months was obtained using a food checklist. In addition, data on the proportion of distributed food consumed by the target child or other family members were obtained using another checklist. Data on the intervals of supplementary food distribution were obtained using a questionnaire.
Semi-structured interviews
Senior nutrition officers, the head of Hygiene, Remedy and Insurance Affairs at IKRF and CHW in urban and rural areas of Qazvin and Semnan with at least 6 months’ experience within the programme were purposively selected for interviews. The first author conducted fifteen in-depth, semi-structured interviews from March to September 2014 using an interview guide. All interviews were prearranged and were undertaken at a convenient time. Each interview lasted between 45 and 60 min. Questions were semi-structured, but the interviewer could ask follow-up or probing questions based on participants’ responses to previous questions( Reference Turner 7 ).
Focus group discussion
Mothers/caregivers with at least one child under 6 years of age covered by the programme were selected through convenience and purposeful sampling and invited to focus group discussions. Twelve focus group discussions were undertaken with six to ten mothers from May to September 2014. Each one lasted between 45 and 90 min. Questions were asked regarding the mother’s experience with the programme and its objectives, the content of the food basket and distribution methods, and the effects of the programme on child and family health status( Reference Liamputtong 8 ). Interviews and focus group discussions were continued until data saturation( Reference Sandelowski 9 ).
Field observations
Twenty-six health houses/centres and five stores were observed in different urban and rural areas in both provinces to collect information on mothers’ training sessions, as well as the adherence of delivered food items to the designed food basket and the protocol of the programme. A checklist was developed for this purpose and all observations were recorded as field notes by the first author.
Ethical considerations
The purpose of the study and questions were explained to the participants. They were also informed that they could leave an interview at any time or ask for the termination of the interview. Confidentiality and anonymity were assured and maintained throughout the study. The protocol of the study was approved by the ethics committee of the National Nutrition and Food Technology Research Institute, Tehran, Iran (contract number 450.88, 2014.05.21).
Data analysis
Quantitative data
The nutrient content of the designed food baskets (obtained from document reviews) was analysed using Nutritionist IV software. Results on the amount of food delivered (information derived from field observation checklists and the survey) and adherence to the designed food basket and the programme protocol were calculated as proportions. Regularity of food basket distribution (survey data) was also compared with the programme protocol. The proportion of foods consumed by target children within the studied households was derived from the food checklist. Data analysis was conducted using the statistical software package IBM SPSS Statistics version 20.
Qualitative data
The recorded interviews and focus group discussions were transcribed verbatim and checked with field notes soon after each interview for the accuracy of transcriptions. All transcripts were imported into MAXQDA software version 2010( Reference Schönfelder 10 ) for analysis. Qualitative content analysis was used to analyse qualitative data. To establish content validity, 30 % of interviews were independently coded by another team member.
Results
The mothers’ mean age was 32·36 (sd 6·47) years. All participants in focus group discussions were unemployed and most of them (78 %) were illiterate or had not finished primary school. The results are presented in five implementation steps: (i) supplementary food basket content; (ii) food basket distribution methods; (iii) selection of eligible children; (iv) distributed food consumption; and (v) child growth monitoring and nutrition training sessions for mothers.
The process of registration and supplemental food distribution was developed for ease of understanding of the programme process by the authors (Fig. 1).
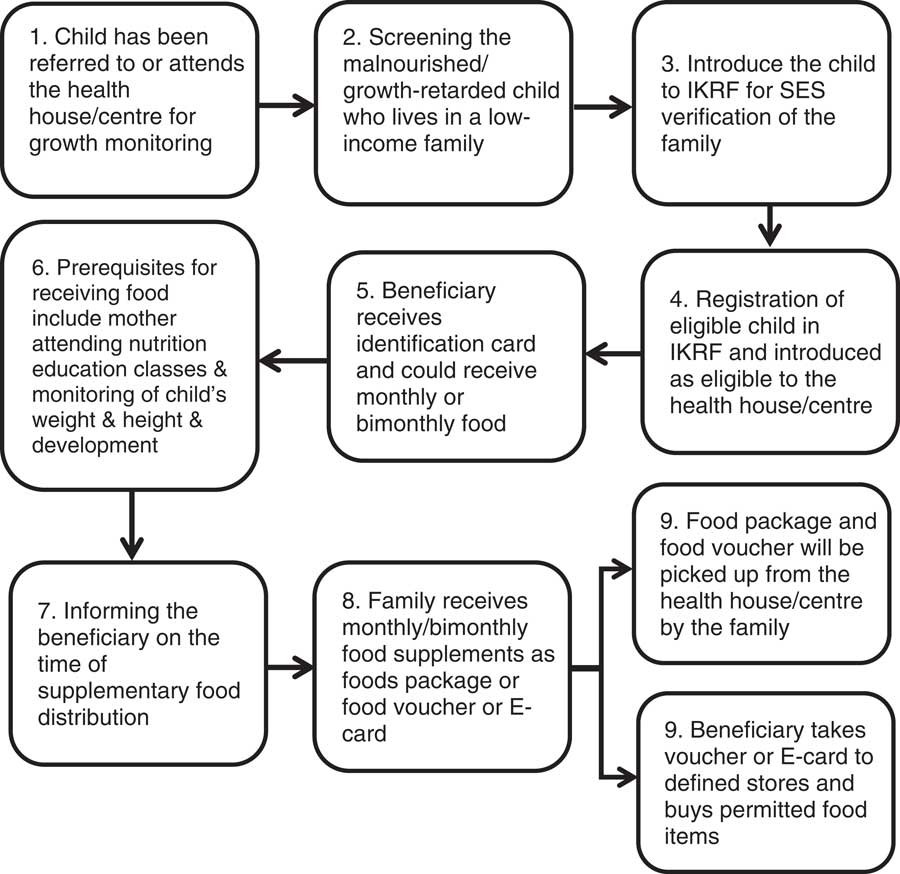
Fig. 1 Beneficiary registration and supplementary food distribution process of the national, community-based, food supplementary programme for improving the nutritional status of children in Iran (IKRF, Imam Khomeini Relief Foundation; SES, socio-economic status)
Supplementary food basket content
Based on the results, the content of the designed food basket was low in milk/dairy products, fruits and vegetables, and high in starches and oil (Table 1). According to the protocol of the programme, each medical university must design child supplementary food baskets for three age groups: 6–12 months, 12–24 months and >2 years of age( 11 ). Document reviews showed that recommendations indicated the food basket for infants (6–12 months) should contain a supplement to breast milk and that it should provide 1464 kJ (350 kcal) of energy and 16 g of protein daily. For children aged 12–24 and 24–59 months, the recommendations indicated that the daily nutritional contribution of the supplementary food in the basket should be 3431 kJ (820 kcal) of energy and 37·5 g of protein, and 7531 kJ (1800 kcal) of energy and 71·5 g of protein, respectively( 11 ). However, our observations and survey demonstrated that in practice the food basket content was the same for all children regardless of their age. The analysis of nutrient content of the food baskets observed in each province showed that the daily energy and protein content of a basket in Qazvin and Semnan were 4845 kJ (1158 kcal) and 37 g, and 6393 kJ (1528 kcal) and 48·5 g, respectively.
Table 1 Amount of food groups in the designed supplementary food basket in each province, Iran, 2014

* From Dietz and Stern( Reference Dietz and Stern 19 ); these amounts are suitable for children aged 2–4 years.
Food basket distribution methods
Based on the results of field observations and interviews in one of the cities and all rural areas of Qazvin, food baskets were distributed among eligible children by health staff. In urban areas of Qazvin, the food supplement was distributed as food vouchers and families could obtain the food at assigned food stores/groceries. In Semnan, all families received their food supplements in the form of electronic cards (E-cards). They could go to the assigned food stores/groceries to obtain their food baskets. Surveys showed that distribution of the food supplement was more irregular using E-cards. Most informants in the health sector explained that irregular distribution of funds by IKRF was the cause of irregularity in food basket distribution (Table 2).
Table 2 Characteristics of food supplements in the programme in two provinces, Iran, March–September 2014

Many beneficiaries who participated in focus group discussions and received food vouchers or food baskets reported that they did not like at least one or more items included in the distributed food baskets. Mothers in rural areas complained about transportation costs and long distances to fetch the food.
Interviewees in Semnan province mentioned that giving the opportunity to freely choose the food items caused deviation from the recommended basket. This was also common in areas where food was distributed via food vouchers in Qazvin province. Surveys showed that in Qazvin, only 44·7 % of the families received the same defined food list. Nearly 20 % of the families in both provinces received junk foods for their children with food vouchers or E-cards. CHW who participated in interviews noticed that, due to the shortage in human resources, there was not enough monitoring in stores when the families were being referred to redeem vouchers or E-cards. Thus, families could choose other food or non-food items.
Furthermore, based on field observations, in cities where supervision was in place, food items were packed according to the food lists provided in vouchers one day prior to the distribution. However, in those cities where supervision was not in place, the prices for some food items were higher in some stores.
Selection of eligible children
According to the interviewees’ opinions, after screening the target children by health workers, the recruitment process was relatively smooth for families. They also agreed that because of high workload in urban areas, it was impossible to screen all eligible children. All mothers who participated in focus group discussions also agreed that the process of nomination did not take too long, and they received the first supplementary food basket one or two months after IKRF verification. However, most of the mothers in rural areas felt stigmatized and judged being as poor because of the investigation of their socio-economic status by IKRF in their neighbourhoods.
Based on the interviewees’ opinions, one limitation of the eligibility criteria concerned immigrants. Since only Iranian children with identification cards were considered eligible, Afghan immigrants (both legal and illegal) were not covered by the programme. This is because having an identification card and bank account (which most of them cannot have) are prerequisites for transferring money to E-cards.
Distributed food consumption
As shown in Table 2, less than 5 % of the studied children were the sole consumers of the supplementary foods. Other family members mostly consumed the distributed foods. Almost all mothers who participated in focus group discussions mentioned that they were not able to feed the target children separately. Low economic status of households enforced mothers to share the food with the other family members. As one CHW stated in an interview:
‘Another issue is the quantity of food in the food basket. Its content is very limited. We only considered children and forgot that they are not alone. The food basket does not focus on the family.’
Table 3 presents the proportions of foods consumed by the target children. The survey showed that about 50 % of the target children were the sole consumers of 75–100 % of the distributed milk and cake/biscuit, while about half of them did not eat the honey, canned peas, sugar and dates distributed through the programme. More than 50 % of them consumed less than 50 % of the rice, vegetable oil, pasta, lentils, cheese and soyabeans. None of the distributed food items was sold.
Table 3 Proportion of foods consumed by the target child within the studied households in two provinces (Qazvin and Semnan), Iran, March–September 2014
Child growth monitoring and nutrition training sessions for mothers
The regularity of child growth monitoring and nutrition training sessions is presented in Table 4. The results showed that half of the mothers had never attended a group nutrition training session. Most of the CHW interviewed in both provinces stated that there were no educational classes specifically for these mothers. The review of documents and field observations showed that among fifty-five studied centres in Qazvin, only two held special education sessions during the study period. The situation was almost similar in Semnan; one health house (rural) and one health centre (urban) had special nutritional training classes for these mothers. In other cases, general health training classes held by health houses/centres were not related to the supplementary food programme. One of the mothers participating in a focus group discussion stated:
‘We have not had any classes here [with discomfort]. Which kind of training classes are you talking about? We just receive food basket and bring it home. After that we use our own knowledge.’
Table 4 Regularity of growth monitoring and nutrition education sessions for mothers within the programme in two provinces, Iran, March–September 2014
Most of the interviewees expressed that due to high workload and large number of children in the programme, nutrition training classes were impossible.
Based on the programme protocol, food transfers were conditional on regular attendance at the training classes and child growth monitoring visits. As shown in Table 4, child growth monitoring visits in Qazvin were more regular than in Semnan (75 % v. 54 %). However, most interviewees believed that use of E-cards by IKRF decreased regular attendance of the mothers for child growth monitoring.
Discussion
The current study reports the process evaluation of the supportive section of an ongoing national nutritional programme in Iran. This is one of the successful ongoing national nutritional programmes in the country, which was initiated 10 years ago. There was no corruption/discrimination in distributing food baskets and, despite irregular distribution in some areas, all eligible children received the food baskets. Ease and smooth registration procedure of the programme was apparent; however, stigmatization as poor was also a barrier reported by some families. The target child was not the sole consumer of the distributed foods and there were some junk foods and non-food items in some baskets.
MacFadden et al. used similar approaches to the present study in the evaluation of the Healthy Start programme that delivers food vouchers and vitamin supplements to low-income pregnant women, young parents and low-income families with children up to the age of 4 years in the UK. The experiences of both sides (i.e. the beneficiaries and the CHW in rural and urban areas) were measured in both studies. They showed similar registration barriers, including complex eligibility criteria, inappropriate targeting of information about the programme by health practitioners to those they judge to be eligible and a general low level of awareness among families( Reference McFadden, Green and Williams 12 ). Interestingly, despite the fact that the Healthy Start programme targeted low-income families in a high-income country, the experiences of the participants were similar to those observed in the current study in a middle-income country.
Although all mothers who participated in focus group discussion declared that they had received supplementary foods after their registration, most of them complained about irregular distribution. Based on the interviewees’ experience, there was no funding limitation. The main drawback was irregular fund distribution (every two or three months) that resulted in irregularity in food basket distribution. The quantitative survey also revealed similar findings about the irregularity of food basket distribution. The high degree of consistency in results obtained from the quantitative and qualitative approaches used in the present study provides confidence in the validity of the findings. Seidenfeld et al. reported that all beneficiaries of the Child Grant Programme in Zambia received the designated amount (equivalent to $US 12 regardless of household size) on time, with easy access to money and without any cost( Reference Seidenfeld, Handa and Tembo 13 ). The Child Grant Programme is an unconditional social cash transfer programme targeting any household with a child under 5 years old.
In the present study, the food items received in areas where foods were distributed as in-kind foods were exactly similar to what was designed, contrary to those distributed via E-cards. Qualitative results showed that in-kind food distribution has some difficulties in transportation and storage (e.g. spoilage of some kinds of food items). Therefore, technological advances and the positive emotional effects of independent food selection on families made distribution in the form of E-cards an advanced method of distribution. The evaluation of the World Food Programme in northern Ecuador by Hidrobo et al. also showed that a high percentage of participants prefer to receive cash, not foods or vouchers( Reference Hidrobo, Hoddinott and Margolies 14 ).
Another important issue in implementation of the programme is the training of mothers and retailers, which has an important impact on the selection of food items by these families. Supervising and controlling food stores are the other important factors that contribute to successful implementation of the programme. Programme staff should have enough time to monitor what is offered by retailers as well as food selection by families at the point of purchase. Sufficient human resources should be allocated for monitoring the implementation of the supplementary food programme( Reference Hidrobo, Hoddinott and Margolies 14 ).
In our study, food distribution in the form of E-cards incurred the high expenses of transport to the families, especially in rural areas. Access to the registered retailers was difficult in rural areas( Reference McFadden, Green and Williams 12 ), which was in line with the results of the World Food Programme evaluation in Ecuador, where the cash transfer was the least costly modality in terms of waiting times and transportation costs. Thus, cash was the preferred modality among beneficiaries. Lack of some food items and higher prices in defined stores were common difficulties experienced by the voucher recipients in the present study, which was consistent with the findings of Hidrobo et al.( Reference Hidrobo, Hoddinott and Margolies 14 ). Despite the different setting of the World Food Programme in Ecuador, most of the participants’ experience on different distribution methods was similar to that in our food supplementary programme except for transportation cost and waiting time in cash transfer. Governments and donors in developing countries are increasingly interested in moving away from commodity-based assistance such as food aid and replacing it with alternative transfer modalities such as cash and vouchers( Reference Hidrobo, Hoddinott and Margolies 14 ). In this situation, increasing the knowledge of beneficiaries on nutrition and strong monitoring could affect food and non-food choices by the families.
Based on the quantitative survey, most of the present study participants spent a high percentage of their vouchers/E-cards on food items; however, there were some junk food and non-food items in their baskets. Interviewees believed that when families were unable to afford basic needs, they would spend a small portion of their cash on non-food items or other food items, which could be used by the whole family. To avoid that, two major strategies should essentially be undertaken: (i) inform mothers about the importance of supplementary foods for malnourished children; and (ii) financial empowerment of the families.
Another important issue was sharing distributed foods with other family members, that could also be due to economic deprivation of families. Hence, low economic status of families is a factor that should be considered in the programme development procedure. The evaluation of distributed food among children in low-income families in Kenya showed that food sharing was common among all voucher recipients. Thus, they allocated a monthly food ration to the families to overcome this problem( Reference Tomedi, Rohan-Minjares and McCalmont 15 ). Distributing monthly food rations or providing cash for purchasing some staple foods for the household could increase the efficacy of the programme. A study by Santos et al. on a milk distribution programme among children aged 6–18 months in Brazil showed that food sharing was the probable cause of unfavourable outcomes. Irregular distribution, frequent gaps in delivering the supplement, no extra milk for siblings and low maternal compliance with recommendations were other possible causes of the outcomes( Reference Santos, Gigante and Coitinho 16 ). A review on supplementary feeding programmes by George et al. showed that food rations provided to households at the time of food insecurity impacted recovery rates in supplementary feeding programmes( Reference George, Menotti and Rivera 17 ).
Regular follow-up is the other important factor for malnutrition treatment, in which CHW could inform mothers about the importance of proper care and treatment( Reference Navarro-Colorado, Mason and Shoham 18 ). Despite the conditionality of attending child monitoring and training classes for receiving food baskets, regular follow-up visits of children were higher when foods distributed through in-kind foods or vouchers compared with cash.
Conclusion
The supportive section of the multidisciplinary programme for improving the nutritional status of children in Iran is an innovative and valuable programme, which aimed to improve the nutritional status of children using supplementary food distribution. The present paper addresses the process evaluation of the programme. It was shown that despite irregular distribution of food baskets, all beneficiaries received their monthly rations and no corruption was reported in food distribution. An important point to note is the inconsistency between the content of the received baskets and the designed one, as well as with nutritional recommendations. Furthermore, a high level of poverty among households may be responsible for the high percentage of intrahousehold food sharing, which calls for family empowerment strategies. Focusing on food items such as eggs or milk in the food baskets that are mostly being used for child feeding may be beneficial to assure that the target child is receiving the distributed foods.
The current study is the first comprehensive process evaluation of such a large-scaled programme using the experience of implementers and beneficiaries in Iran. One of the strengths of this research is the range of quantitative and qualitative data collection techniques used and that the results of both methods point to the same conclusions. The study findings are applicable to other parts of the country and similar communities, and policy makers should consider these results to increase the effectiveness of such programmes. In addition, the process evaluation methods discussed herein could be used as an effective strategy to monitor the implementation of the programme in other parts of the country.
Acknowledgements
Acknowledgements: The authors would like to thank Dr Zahra Abdollahi and Ms Mina Minaee in the Community Nutrition Department of the Ministry of Health and Medical Education for their great support and for facilitating and enabling data gathering. They also are thankful to Mr Mostafa Hosseini, Mr Ali Aziz-Khani and Ms Atiyeh Razzazi who coordinated the surveys in Semnan and Qazvin provinces. The authors thank all those who participated in and/or helped recruit participants for this evaluation in Semnan and Qazvin. Special thanks go to Ms Mariam Aghaian for her helpful collaboration in data collection and data entering efforts. Finally, the authors are grateful to the staff and CHW who assisted with the study. Financial support: This study was carried out with the financial support of the UNICEF office in Iran. The UNICEF office in Iran had no role in the design, analysis or writing of this article. Conflict of interest: The authors disclose no conflicts of interest. Authorship: D.G., A.R., N.O., H.R. and H.E.-Z. designed the research; D.G. conducted the research; D.G., A.R., N.O. and M.E. analysed the data; D.G. wrote the paper; and D.G., A.R. and N.O. had primary responsibility for final content. All authors read and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee of the National Nutrition and Food Technology Research Institute (contract number 450.88, 2014.05.21). Furthermore, permission was granted by the deputy of health in medical universities in each province. Written informed consent was obtained from all subjects.





