


Childhood obesity has reached epidemic proportions in most industrialized countries and in several low-income countries, especially in urban areas(Reference Wang and Lobstein1). Currently, Greece has one of the highest rates of paediatric obesity worldwide(Reference Lissau, Overpeck and Ruan2), with an alarmingly increasing trend observed between 1997 and 2004, which has apparently been levelling-off since the last half of the decade(Reference Tambalis, Panagiotakos and Kavouras3). Obese and overweight children are more likely to exhibit components of the metabolic syndrome, such as increased blood pressure and abnormal glucose and lipid metabolism(Reference Weiss, Dziura and Burgert4). In addition, childhood obesity in most cases tracks into adulthood and thereby has lasting adverse health effects(Reference Whitaker, Wright and Pepe5, Reference Berenson and Srnivasan6).
Parental obesity plays an important role in predicting children's risk of obesity in adulthood. It is estimated that a family history of obesity more that doubles the risk of adult obesity among both obese and non-obese children under the age of 10 years(Reference Whitaker, Wright and Pepe5). Parental, especially maternal, obesity has also been identified as a significant predictor of obesity in the offspring during childhood(Reference Strauss and Knight7). Family members share both genes and environmental factors. More than 600 genes, markers and chromosomal regions have been currently identified to be involved in body weight regulation and obesity development according to the latest version of the Gene Obesity Map(Reference Perusse, Rankinen and Zuberi8). However, this gene effect seems to account for as much as 40 % of the variation in BMI or fat mass(Reference Marti and Martinez9). Environmental influences including parental modelling of eating behaviours, food choices, child feeding practices and socio-economic factors seem to play an important role in the development of obesity in every family member. However, these environmental factors have not been exclusively studied in families in which all members are overweight and/or obese.
The objective of the present study was to identify Greek families in which all members were overweight or obese (XXL families) and to describe their profile with regard to their socio-economic status and their eating behaviours and practices, further aiming to determine the best approaches for preventing interventions.
Subjects and methods
We recruited children aged 11 and 12 years and their parents from volunteers between September 2008 and May 2009. All participants resided in the Kavala metropolitan area and were recruited from twelve primary schools that were randomly selected and located in both urban and rural regions within the prefecture of Kavala, northern Greece. The sole inclusion criterion was enrolment in the fifth or sixth grade of a primary school; there were no exclusion criteria. A letter explaining the aim of the study was provided to each parent and an informative speech was made on the day before the measurements were to be taken. Written informed consent, in accordance with the revised version of the Helsinki Declaration regarding research involving human subjects, was obtained from all parents or legal guardians. The study was approved by the Ministry of National Education and Religious Affairs, by Kavala's public school supervisor and by the head principal and teachers of the schools included.
Auxologic measurements of the children were obtained in the school setting with the participants wearing light clothing and no shoes. Height was measured using a regularly calibrated, wall-mounted ruler (Minimetre; Raven Equipment Limited, Dunmow, UK) and expressed in centimetres rounded to the nearest 0·5 cm. Weight was measured on a portable electronic scale (model 901; Seca, Hamburg, Germany) and expressed in kilograms to the nearest 0·5 kg. BMI was calculated as weight in kilograms divided by the square of height in metres (kg/m2, Quetelet index). Overweight and obesity were determined according to the International Obesity Task Force (IOTF) standards for age and sex developed by Cole et al.(Reference Cole, Bellizzi and Flegal10). For adults, overweight was identified as BMI ≥25·0 kg/m2 and obesity as BMI ≥30·0 kg/m2, according to standard definitions laid down by WHO(11).
A structured questionnaire consisting of twenty-one multiple choice or open-ended questions was filled in by one of the parents of each child at home. The aim of the questionnaire was to collect information on the socio-economic status of the family, as well as anthropometric values (weight and height) and the educational status of parents, their diet history, dietary habits, the availability of various food products and beverages at home, dietary intake, physical activity, time spent sleeping and time spent watching television.
For statistical analysis the SPSS for Windows statistical software package version 17·0 (SPSS Inc., Chicago, IL, USA) was used. Percentages were compared using the χ 2 test, whereas means were compared using the unpaired Student t test. A P value <0·05 was considered statistically significant. Finally, logistic regression models (univariate and multivariate, stepwise) were used for the identification of parameters that predict an XXL family.
Results
A total of 331 families returned completed questionnaires and were included in the final statistical analysis. In sixty-one families (18·43 %) both parents and child were overweight or obese, and in seven of these families all members were obese. From the 270 families (81·57 %) in which not all members were overweight or obese, more than half (n 140) had two members classified as overweight or obese, whereas an additional 102 families had one member who was overweight or obese. Only twenty-eight families (8·46 % of the total number of studied families) had normal BMI in all members. A total of 165 fathers were overweight (48·04 %) and eighty-three (25·08 %) were obese. The corresponding figures for mothers were 100 (43·20 %) and forty-four (13·29 %), respectively, for overweight and obesity. Overall, overweight was identified in 111 children (33·80 %), whereas obesity was identified in fifty-one (15·40 %). A schematic demonstration of the distribution of overweight and obesity among members of the studied families is presented in Fig. 1.
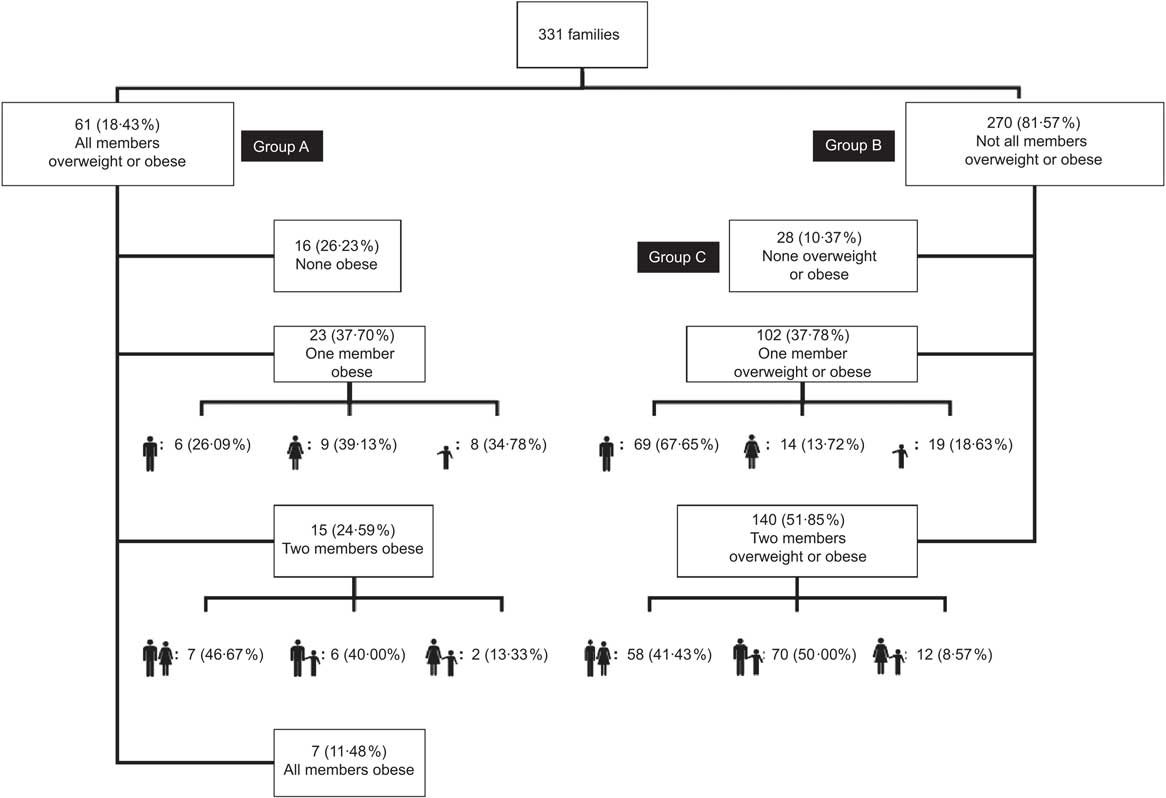
Fig. 1 Distribution of overweight and obesity among members of the studied families
When families were classified on the basis of all members being overweight or obese (XXL family) or having at least one member with normal weight, two groups consisting of sixty-one (18·43 %) and 270 (81·57 %) families were formed (Groups A and B; Fig. 1). The XXL family (Group A) was characterized by a lower educational status of both parents, as a significantly increased percentage of fathers and mothers had only primary-school education compared with parents in Group B (34·42 % v. 18·89 %, P < 0·005 and 29·51 % v. 17·78 %, P < 0·03, respectively; Table 1). In addition, the XXL family was inversely associated with maternal tertiary education as only 8·20 % compared with 30·37 % (P = 0·0006) of mothers in XXL families attained a higher educational level. Although the XXL family seemed to reside more in rural areas than in cities and to have a lower income, these differences did not reach statistical significance. On the other hand, skipping breakfast and spending more than 3 h in front of a screen (mainly television watching) per day were more frequently observed in XXL families (Table 1).
Table 1 A comparison of socio-economic and demographic characteristics, as well as eating and television-viewing habits, between families in which all members are overweight or obese (XXL families) and other families
*Statistically significant difference (P ≤ 0·05).
With regard to the availability of various food products and beverages at home, no significant differences were observed between XXL families and the rest of the studied families (Table 2). However, when the XXL families were compared with twenty-eight families in which all members had normal BMI (Group C; Fig. 1), significantly increased availability of sweets and juices was recorded in the XXL families (Table 3). Finally, weekly consumption of fish, vegetables, fruit and, surprisingly, pasta was significantly higher in normal families compared with XXL families. In contrast, XXL families were more frequently consuming products that were not homemade (mainly pizza and meat products).
Table 2 A comparison of home availability of various food products or beverages and weekly food consumption between XXL families and other families
*Statistically significant difference (P ≤ 0·05).
Table 3 A comparison of home availability of various food products or beverages and weekly food consumption between families in which all members are overweight or obese and families in which all members have normal weight
*Statistically significant difference (P ≤ 0·05).
Table 4 shows only parameters with statistically significant odds for predicting XXL families in the univariate analysis. When these statistically significant variables were introduced in a multivariate model, screen time for >3 h/d and reduced meal duration were found to be independent risk factors for overweight or obesity among all members of the family.
Table 4 Logistic regression models (univariate and multivariate, stepwise) for predicting an XXL family

Only statistically significant parameters are presented in the table.
*Statistically significant difference (P ≤ 0·05).
Discussion
Several studies provide compelling evidence of genetic influence on obesity, with some of the strongest support coming from twin and adoption studies(Reference Silventoinen, Rokholm and Kaprio12). When using BMI to quantify adiposity, the twin literature gives fairly consistent estimates of the proportion of within-population variation in adiposity that is attributable to within-population genetic variation, with heritability estimates exceeding 70 %(Reference Maes, Neale and Eaves13). However, the contribution to BMI from shared environmental factors has been less certain. A recently published longitudinal twin study from Finland found that the effect of common environment on BMI variation disappeared in adolescence probably as a result of the increasing independence that leads to a more individualistic eating and exercise behaviour(Reference Lajunen, Kaprio and Keski-Rahkonen14). The common environment also influences food preferences in young children; however, this effect also declines in young adulthood when food preferences are determined mainly by additive genetics and specific environmental factors(Reference Breen, Plomin and Wardle15). In our study we included families having children aged 11 and 12 years, just before adolescence when children become more independent in making their own choices, in whom there was considerable influence of familial environmental factors on the formation of childhood obesity.
It is now widely accepted that obesity is generally inversely correlated to the indicators of socio-economic status in developed countries(Reference Parsons, Power and Logan16), whereas the reverse is true for developing countries(Reference Wang17). This pattern was not clearly visible in the paediatric population in the past(Reference Sobal and Stunkard18); however it has become more apparent in the last 15 years(Reference Shrewsbury and Wardle19). In our study, the XXL family was characterized by a lower educational status of both parents, whereas the mother's tertiary education seemed to act as a protective factor against a family becoming overweight. On the contrary, annual family income and area of residence were not significantly associated with the XXL family. Shrewsbury and Wardle(Reference Shrewsbury and Wardle19) recently reviewed all cross-sectional studies investigating childhood adiposity and socio-economic status that have been published since 1990 and showed that, when the socio-economic indicators were examined individually, parental education was more consistently inversely associated with adiposity, followed by parental occupation and family income. Correspondingly, a study from Greece has shown a significant inverse association between parental education and BMI in a cohort of children aged 6–17 years(Reference Krassas, Tzotzas and Tsametis20), whereas Moschonis et al.(Reference Moschonis, Grammatikaki and Manios21) showed that children whose mothers had a college degree were 0·56 times less likely to be overweight compared with those whose mothers had only lower secondary education or less. Although in some studies differences in child feeding and physical activity have been identified, a greater understanding of how parental education influences dietary intake and lifestyle is needed in order to establish effective preventive interventions.
Our study showed that children in obese families spend >3 h/d in front of a screen, a greater proportion compared with normal families. Watching television is considered as a significant contributor to childhood obesity among pre-school and school-aged children and adolescents and this phenomenon is mediated mainly through increased energy intake and overconsumption of highly advertised junk food(Reference Manios, Kondaki and Kourlaba22) and to a lesser extent through reduced physical activity(Reference Robinson23). In addition, increased television watching has been associated with unhealthy dietary patterns such as lower intakes of vegetables, grains and dairy food(Reference Feldman, Eisenberg and Neumark-Sztainer24) and increased consumption of high-fat and high-sugar foods(Reference Manios, Kondaki and Kourlaba22) and soft drinks(Reference Coon, Goldberg and Rogers25). In our study, a child spending >3 h in front of a screen almost triples the odds for predicting an XXL family in the multivariate analysis. The other significant parameter in the multivariate analysis was the reduced meal duration. Indeed, reduction of meal duration by 5 min increased the odds of predicting an XXL family by approximately 30 %. Rapid eating has not been widely studied as a potential contributor to the development of childhood obesity. Recently, Berkowitz et al.(Reference Berkowitz, Moore and Faith26) investigated the association of children's eating behaviour and parental feeding prompts with excess weight gain in children born at high or low risk of obesity that was determined by maternal BMI. Results showed that child mouthfuls of total energy intake per minute from food predicted an increased risk of overweight or obesity at the age of 6 years, whereas greater active mealtime was associated with a reduced risk of being overweight or obese. More elegantly designed studies have questioned the underlying pathophysiological mechanisms and have shown a higher postprandial response of the anorexigenic hormones peptide YY and glucagon-like peptide-1 after a 30-min meal than after a 5-min meal(Reference Kokkinos, le Roux and Alexiadou27).
In previous studies a consistent association between skipping meals and increased rates of childhood obesity has been documented(Reference Koletzko and Toschke28). In the present study, we have shown a significantly increased prevalence of children having three meals or fewer per day in XXL families compared with normal families. Although breakfast consumption is associated with a reduced risk of overweight or obesity and a reduced BMI in children and adolescents in Europe, it is also the commonly skipped meal(Reference Szajewska and Ruszczynski29). Meal skipping can either have a causative role in obesity or develop as an unhealthy practice of a false dietetic plan.
With regard to weekly consumption of various food groups and the availability of various food products and beverages at home, no significant differences were recorded between XXL families and others. However, these results may have been influenced by methodological limitations such as the subjective nature of collecting data from a questionnaire completed by parents. Thus, this lack of significant ‘unhealthy’ dietary habits in the XXL family could be attributed either to a reverse causative phenomenon or to preventive steps that members of XXL families have been taking towards changing dietary habits. However, when the XXL families were compared with families in which all members had normal BMI, a number of significant deviations were observed.
Parental obesity not only interacts with childhood obesity in a causative manner but also sabotages the likely success of multidisciplinary childhood obesity programmes(Reference Eliakim, Kaven and Berger30). Thus, weight management programmes for treating childhood obesity should be family oriented and should combine dietary, behavioural and physical activity interventions. Future steps to prevent childhood obesity should focus on identifying behavioural risk factors within the family that predispose children to excessive weight gain. Limiting children's and consequently the whole family's television-viewing time and discouraging a rapid eating style, laying emphasis on spending quality time as a family during meals, are two behaviours that conflict with the profile of the XXL family, apart from higher parental educational level, as indicated by the results of our study.
Acknowledgements
No funding was obtained for this study and there is no conflict of interest. A.C. conceived the study, interpreted the results, conducted the statistical analysis and wrote the manuscript; S.B. participated in the collection of the data and helped to draft the manuscript; H.P. participated in the design of the study; M.P. participated in the collection of the data; D.C. participated in the design and coordination of the study. The authors would like to thank the children and their parents for their willing participation in the study.





