



Acquiring accurate and adequate nutrition information is a prerequisite to making informed nutritional choices and maintaining a healthy nutritional status(Reference Quaidoo, Ohemeng and Amankwah-Poku1). Nutrition knowledge (NK) among individuals promotes healthy food habits, enhances nutrition status and reduces risks of developing non-communicable diseases such as diabetes, obesity, cancer, chronic lung diseases, hypertension and CVD(Reference Barbosa, Vasconcelos and Correia2,Reference Triches and Giugliani3) .
More than 50 % of the global burden of disease is attributed to non-communicable diseases, wherein unhealthy diet plays a significant role(Reference Benziger, Roth and Moran4). A similar trend is seen among the Arab population, with IHD being a leading cause of death(Reference Mokdad, Jaber and Abdel Aziz5). The eastern Mediterranean region has the highest mortality caused by diabetes(6), and ranks second in obesity, with 75 % of the population overweight or obese(7). For example, the United Arab Emirates (UAE) has high non-communicable disease-related morbidity and premature mortality rates(8). Similarly, non-communicable diseases are estimated to account for 78 % of all deaths in Jordan(9).
Young adults, such as university students, are prone to making lifestyle changes that pose a significant challenge to healthy eating(Reference Sajwani, Shoukat and Raza10) by their adoption of unhealthy nutritional habits, such as frequently consuming fast food and convenience food(Reference Larson, Perry and Story11) and low personal meal preparation(Reference Larson, Neumark-Sztainer and Laska12). Such behaviours result in negative health outcomes including weight gain and increased risk of chronic diseases(Reference Evenson, Rudnickas and Anderson13). University students in Jordan showed significant differences between BMI and health practices based on the type of diet they followed. Students with lower BMI had higher mean scores for positive health practices than those who had higher BMI(Reference Abu-Moghli, Khalaf and Barghoti14). Similarly, better diet quality and higher physical activity level were reported among normal weight university female students than their overweight and obese counterparts, and a significant negative correlation was found between diet quality and neck circumference (indicator of obesity) in the UAE(Reference Attlee, Hasan and AlQattan15).
A valid NK assessment tool, therefore, is crucial to understand the levels of NK among individuals so that need-based nutrition education interventions can be developed. Several questionnaires have been developed and validated for NK assessment among the adult population(Reference Guadagnin, Nakano and Dutra16–Reference Bradette-Laplante, Carbonneau and Provencher18). Parmenter & Wardle(Reference Parmenter and Wardle19) developed a general nutrition knowledge questionnaire (GNKQ) for the adult population in the UK in the 1990s, which was later adapted and validated in different countries, such as Turkey and Australia(Reference Al Saffar20,Reference Hendrie, Cox and Coveney21) . A study adapting the original GNKQ(Reference Parmenter and Wardle19) highlighted that adults in a university community in the UAE exhibited inadequate NK, particularly regarding diet–disease association, and inadequate application of dietary recommendations in making informed dietary choices(Reference Attlee, Abuqiya and Obaid22). However, new knowledge of the associations between diet and health and advanced developments in the food supply, including the introduction of new types of foods and processing methods, have resulted in frequent updates to nutrition recommendations, which necessitate a periodic re-evaluation of NK assessment(Reference Willett and Stampfer23). Thus, the original GNKQ has been updated, and the revised general nutrition knowledge questionnaire (GNKQ-R) has recently been validated on the adult population in the UK(Reference Kliemann, Wardle and Johnson24). However, no updated tool is available in the Arabic language to assess the level of NK among adults in the Arab region, where lack of nutrition awareness may be an important determinant in the wide prevalence of nutrition-related issues.
For the current study, the GNKQ-R, the updated version of the original questionnaire developed by Parmenter & Wardle(Reference Parmenter and Wardle19), was translated into Arabic to assess its validity and reliability among young adults. The participants comprised students from two universities in the UAE and Jordan. The GNKQ-R has purportedly been employed to develop similar questionnaires worldwide due to its several merits; it includes more than two domains of NK, has reportedly high reliability and validity and specifies the target population(Reference Bukenya, Ahmed and Andrade25).
Methods
Participants
The current study included students aged 18 years and above from two prominent universities, the United Arab Emirates University (UAEU), Al Ain, UAE and Hashemite University (HU), Zarqa, Jordan. Participants were invited through emails, social media platforms and advertisements posted around the university campuses. A student registered in any undergraduate programme during the period of the current study was eligible for participation. The survey was administered in two formats: on paper (hard copies) and online (via Google documents). A total of 805 students (290 from UAEU and 515 from HU) agreed to participate in the study. Participants from the programmes of Nutrition/Dietetics (n 84), Agriculture (n 62), Social Sciences (n 181), Medicine (n 45), Education (n 281), Science (n 25), Engineering and Information Technology (n 82) and Economics and Law (n 45) volunteered to participate. No incentives or rewards were offered for participation. Informed consent was obtained from all participants before commencing the study. Written consent was obtained from students who completed the hard copy questionnaires, whereas clicking on ‘Next page’ after the brief instruction to start the online survey was considered consent for online questionnaires. Online questionnaires were administered for UAEU students and hard copies for HU students.
A pilot study was conducted using a crossover-counterbalanced design on thirty-one students from Jordan. Each student was asked to complete the questionnaire twice, once on paper and once online with a gap of 1 week between the two. No significant differences were evident in the response scores (total score out of 86) irrespective of the questionnaire format (paper 40·6 ± 3·5 v. online 40·4 ± 3·6; t = 1·044, P = 0·305; r 0·971, P < 0·001). Furthermore, the pilot study revealed that the students required 17·6 ± 2·1 min to complete the questionnaire. These results were not included in the final analysis of the actual study. The participants of the pilot study were instructed to answer all questions and provide written comments on the clarity and difficulty of the items.
Students’ demographics in terms of age, gender, marital status, academic level and study discipline in the university, self-perceived health status and self-reported BMI category were recorded.
Development of the Arabic version of the adapted revised general nutrition knowledge questionnaire
The Arabic version of GNKQ-R was adapted from the English version of the recently validated eighty-eight-item GNKQ-R(Reference Kliemann, Wardle and Johnson24) consisting of four sections evaluating NK: Section 1: Dietary recommendations (eighteen questions), Section 2: Food groups and nutrient sources (thirty-six questions), Section 3: Healthy food choices (thirteen questions) and Section 4: Associations between diet–diseases and weight (twenty-one questions). The questions were in multiple choice format, and check marks were used as responses. Answers were scored by assigning one point for each correct response and zero points for an incorrect response; scores from the four sections were added to obtain the overall general NK score among the participants. The English version of GNKQ-R was translated into Arabic and then reviewed for forward-and-back translations. Furthermore, two original items (Section 1, Question 6: Approximately how many alcoholic drinks is the maximum recommended per day (The exact number depends on the size and strength of the drink)? and Section 3, Question 10: Traffic lights are often used on nutrition labelling; what does amber represent in the fat content of a food?) were removed as instructed by the Arabic and/or English speaking expert panel because of cultural sensitivity and applicability. The scale was then reviewed for content clarity, difficulty and accuracy by twelve faculty members from Nutrition and Dietetics, two faculty members from Arabic Language and five licensed dieticians from the two universities. The final Arabic version comprised eighty-six items from the English GNKQ-R. The adapted Arabic GNKQ-R is available in the online supplementary material.
Reliability and validity of the adapted Arabic revised general nutrition knowledge questionnaire
To examine the psychometric properties of the adapted Arabic version of GNKQ-R, four studies were conducted. Studies 1, 2, 3 and 4 examined the internal and external reliability, construct validity, convergent validity and responsiveness to nutrition information, respectively.
Study 1: Internal and external reliability
Data of all students (n 805) from the first-time completion of the questionnaire were combined to assess the internal reliability (Cronbach’s α) of the questionnaire. A test–retest approach was used to examine the external reliability of the questionnaire over time. Two weeks after the administration of the questionnaire for the first time, 106 participants completed the same questionnaire for the second time. None of the participants who completed the questionnaire for the second time received nutrition information between trials. Data from the second administration were not included in the internal reliability assessment(Reference Kliemann, Wardle and Johnson24).
Study 2: Construct validity
Construct validity was examined by analysing the responses of two groups of participants who were expected to have different NK(Reference Kliemann, Wardle and Johnson24). The participants were fourth-year students majoring in Nutrition/Dietetics (n 84) and/or Arabic Literature (n 88) from UAEU and HU. Nutrition/Dietetics students were expected to have higher NK than the Arabic Literature students.
Study 3: Convergent validity
Convergent validity was determined based on the data of 750 students by combining the initial response data from study 1 (external reliability, n 106), study 2 (n 172) and data from the additional 472 students recruited to achieve a better representation of both universities’ populations in terms of demographics, such as gender, age, academic level and self-reported health status and BMI categories. The authors anticipated better NK scores among females(Reference Attlee, Abuqiya and Obaid22), students with higher academic level and those with higher self-reported health status(Reference Kliemann, Wardle and Johnson24). NK scores were also expected to improve with age(Reference Barbosa, Vasconcelos and Correia2).
Study 4: Responsiveness to nutritional information
To assess the sensitivity of NK scores to nutritional information, fifty-five students, other than those studying in the Nutrition/Dietetics programmes in both universities, were recruited. Sensitivity was assessed using a pre–post-test design using a nutrition education approach, which was expected to improve NK scores(Reference Kliemann, Wardle and Johnson24). The participants completed the online questionnaire for the first time. After 2 weeks, they were provided with an online Arabic document containing nutrition information related to food-based dietary guidelines in Arab countries. This was obtained from official open access sources of public health organisations(26,27) . The content of this nutritional information was chosen to reflect information related to all of the individual sections of the questionnaire. Each participant received the information document at least 24 h before completing the questionnaire for the second time. The participants were instructed to respond only after reading the provided document and to avoid rereading once they had begun completing the questionnaire.
Statistical analysis
The data were analysed using IBM SPSS statistics 24 (IBM SPSS). All data were presented as means and sd. For internal reliability, Cronbach’s α was obtained (values ≥ 0·7 for the overall score and for each section were considered adequate)(Reference Kliemann, Wardle and Johnson24), whereas dependent samples t test and intra-class correlation coefficients were calculated for external reliability (intra-class correlation coefficient values ≥ 0·7 were considered adequate)(Reference Field28). Construct validity was assessed using dependent samples t test to evaluate significant differences between the two groups of students (Nutrition v. Arabic Literature). For convergent validity, the independent samples t test and one-way ANOVA (followed by Tukey’s post hoc test) were used to detect significant differences in NK scores and students’ demographic variables (gender, age, marital status, academic level, study discipline, self-reported health status and BMI categories). The responsiveness to nutrition information was evaluated using the dependent samples t test to compare and detect significant differences in NK scores before and after acquiring nutrition information. When significance was detected, the effect size (Cohen’s effect (d) with t test and eta squared (η 2) with ANOVA) was calculated and reported, as previously described(Reference Kliemann, Wardle and Johnson24).
The sample sizes for all studies were higher than the minimum sample sizes (n 34, 102, 180 and 34 for studies 1, 2, 3 and 4, respectively. These were calculated using G* Power software (version 3.1.9.2; HHU) to detect a medium effect size, with a significance level of P < 0·05 and power of 0·80.
Results
Reliability and validity of the revised general nutrition knowledge questionnaire
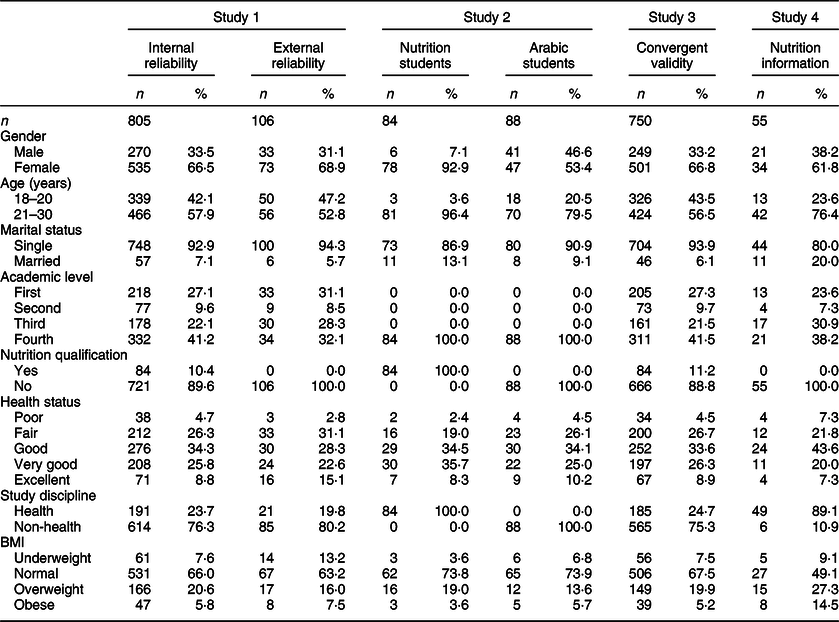
Demographic characteristics of the participants in each of the four validation studies are shown in Table 1. The assessment of internal reliability (n 805) included undergraduate university students: 535 females (66·5 %) and 270 males (33·5 %) with a mean age of 21·3 ± 1·9 years. A smaller proportion of students were from a health discipline (23·7 %) than from non-health disciplines (76·3 %), and first- and second-year students were fewer (36·7 %) than third- and fourth-year (63·3 %) in the study. Moreover, approximately 10 % of the participants were registered in the Nutrition/Dietetics programmes at the two universities. Almost, two-thirds of the students reported good to excellent health status (68·9 %) and BMI (66 %) in the normal category, on self-report measures.
Table 1 Demographic characteristics of the participants (all studies, n 805) in the Arabic revised general nutrition knowledge questionnaire study during 2018–2019 in Jordan and United Arab Emirates
Study 1: Assessment of internal and external reliability
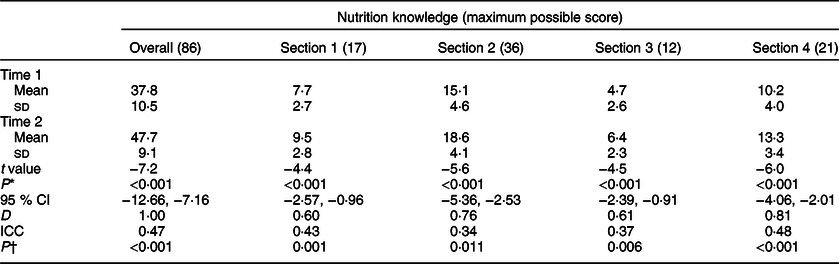
The internal reliability analysis generated higher values than the recommended criteria(Reference Kliemann, Wardle and Johnson24), with an overall reliability of 0·91. Cronbach’s α for individual sections, in the range of 0·70–0·83, also reflected an adequate internal consistency (Table 2). The test–retest reliability outcome was adequate for overall and individual sections as revealed by the dependent t test analysis. NK scores were not significantly different when compared between time 1 and time 2 for overall scores (t = 0·94, P = 0·350) and individual sections (P > 0·05). Moreover, the intra-class correlation coefficient between time 1 and time 2 was higher than the recommended criteria(Reference Field28) for overall scores (0·84) and for all individual sections (0·72–0·74) (Table 2).
Table 2 Internal (n 805) and external (n 106) reliability of the Arabic revised general nutrition knowledge questionnaire (GNKQ-R; Arabic GNKQ-R study 1) during 2018–2019 in Jordan and United Arab Emirates
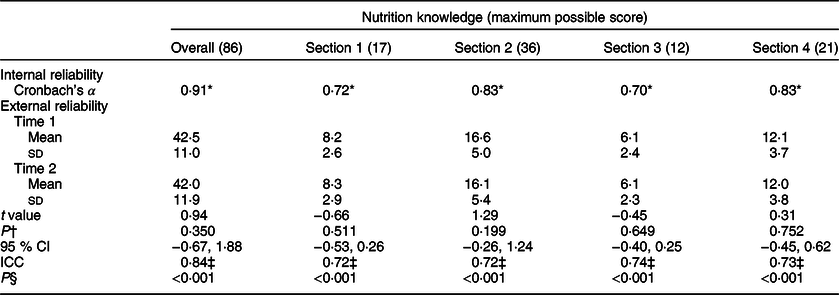
Section 1, dietary recommendation; Section 2, food groups; Section 3, healthy food choices; Section 4, diet, disease and weight association; Time 1, initial response; Time 2, obtained 2 weeks from initial response; ICC, intra-class correlation coefficient.
* Adequate value based on the recommended criteria (Cronbach’s α ≥ 0·7).
† P value of the difference between time 1 and time 2 mean nutritional knowledge score values.
‡ Adequate value based on the recommended criteria (ICC ≥ 0·7).
§ P value of ICC.
Study 2: Assessment of construct validity
Overall and individual section NK scores were significantly higher among students majoring in Nutrition (n 84) than students of Arabic Literature (n 88) as revealed by the dependent t test analysis. The difference in the overall mean scores was 28·0 (P < 0·001, 95 % CI −1·2, −24·8), with an overall Cohen’s d effect size of 2·6, which represents a large effect size (Table 3).
Table 3. Comparison of the mean nutrition knowledge scores of Nutrition/Dietetics (n 84) and Arabic Literature (n 88) students to assess construct validity (Arabic revised general nutrition knowledge questionnaire study 2) during 2018–2019 in Jordan and United Arab Emirates
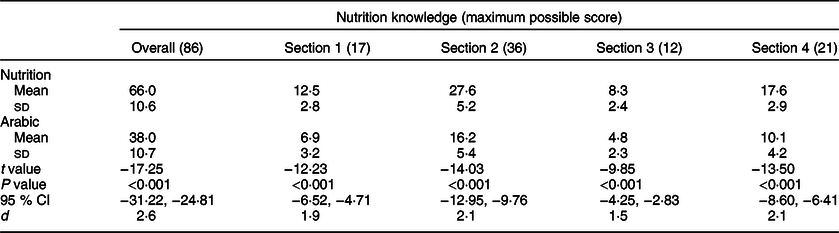
Section 1, dietary recommendation; Section 2, food groups; Section 3, healthy food choices; Section 4, diet, disease and weight association; d, Cohen’s effect size.
Study 3: Assessment of convergent validity
The associations between NK scores and demographic variables of participants (n 750) are shown in Table 4. The NK scores (overall and all individual sections) were significantly higher among females than males, as revealed by the independent t test analysis; Cohen’s effect size ranged from small (Sections 2 and 4) to medium (overall and Sections 1 and 3). Moreover, older students (21–30 years old) achieved significantly higher NK scores (overall and Sections 1, 2 and 4) than younger students (18–20 years old), as revealed by the independent t test analysis, with a small-to-medium Cohen’s effect size. In addition, third- and fourth-year senior students obtained significantly higher NK scores than first- and second-year students on the overall scale and individual sections, as revealed by the independent t test analysis; Cohen’s effect size ranged from small (Sections 1 and 3) to medium (overall and Sections 2 and 4). An independent t test analysis revealed that single/unmarried students achieved comparable NK scores to married students in all sections except Section 3, in which single students scored significantly lower than married students (P = 0·015, small Cohen’s effect size). The students registered in a health discipline achieved significantly higher NK scores (overall and all individual sections) than those in non-health disciplines, as revealed by the independent t test analysis, with a large Cohen’s effect size. However, NK scores were independent of the students’ self-reported health status. Further, ANOVA revealed that BMI categories were only significantly associated with NK scores of Section 3 (F(3746) = 4·45, P = 0·004, small Cohen’s effect size), with students classified as underweight being significantly different from students classified as normal (P = 0·004), but without indicating any further differences.
Table 4 Associations of mean nutrition knowledge scores with gender, age, marital status, academic level, health status, study discipline and BMI categories (Arabic revised general nutrition knowledge questionnaire study 3, n 750) during 2018–2019 in Jordan and United Arab Emirates
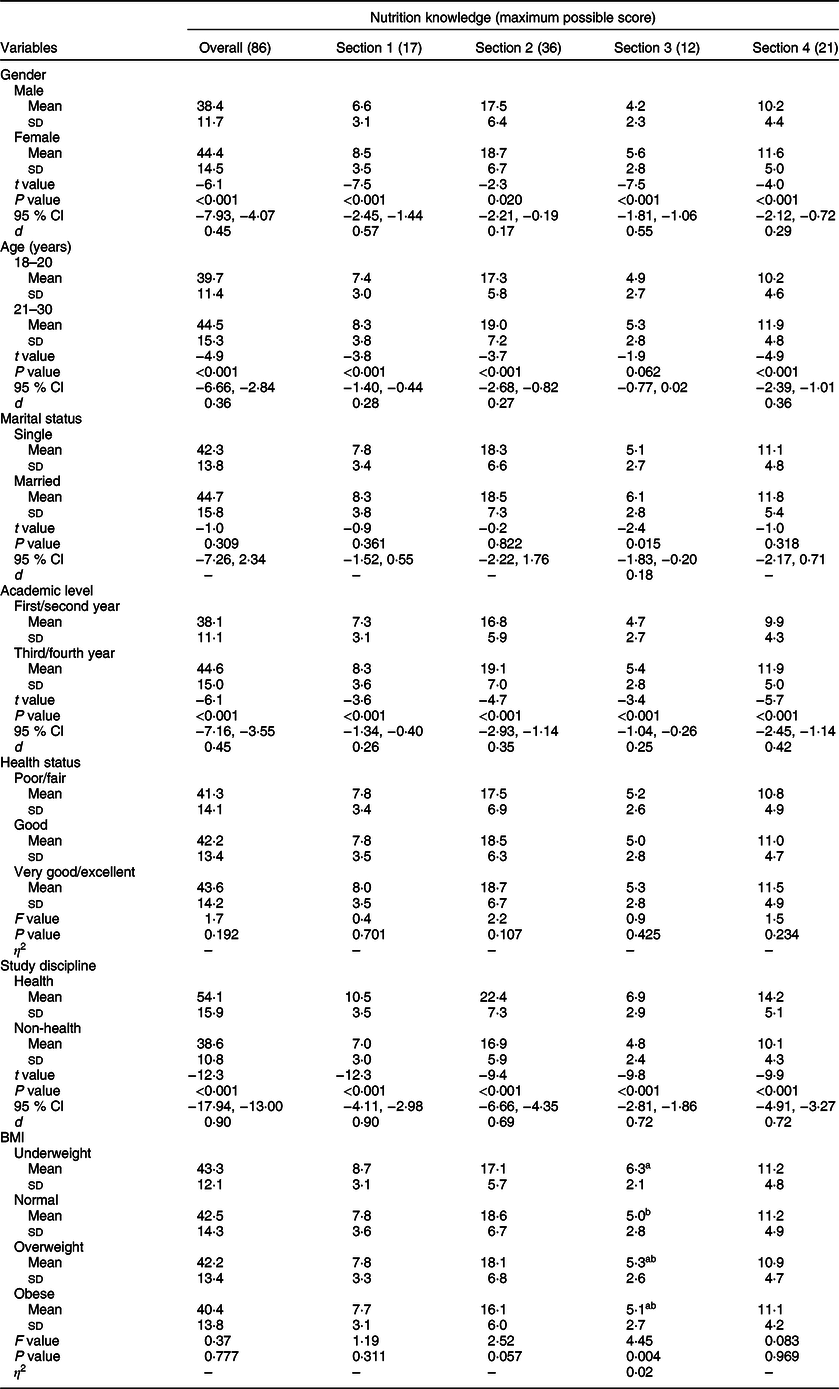
Section 1, dietary recommendation; Section 2, food groups; Section 3, healthy food choices; Section 4, diet, disease and weight association; d, Cohen’s effect size.
a, bMean values within same column with different superscript letters were significantly different (P < 0·05).
Study 4: Responsiveness to nutritional information
The overall and sectional NK scores were significantly higher after the students had been exposed to the online nutritional information. Medium-to-large effect size differences ranging from 0·60 to 1·0 were observed for the overall and individual section NK scores (Table 5).
Table 5 Comparison of the mean nutrition knowledge scores obtained before and after nutritional information intervention (Arabic revised general nutrition knowledge questionnaire study 4, n 55) during 2018–2019 in Jordan and United Arab Emirates
Section 1, dietary recommendation; Section 2, food groups; Section 3, healthy food choices; Section 4, diet, disease and weight association; Time 1, pre-intervention; Time 2, post-intervention (obtained 2 weeks from initial response); ICC, intra-class correlation coefficient; d, Cohen’s effect size.
* P value of the difference between time 1 and time 2 mean nutrition knowledge score values.
† P value of ICC.
Discussion
The Arabic version was found to have good internal and external reliability, consistent with the reliability of the English GNKQ-R(Reference Kliemann, Wardle and Johnson24). The overall internal reliability of Arabic version was high (Cronbach’s α = 0·91) and comparable to the English GNKQ-R (Cronbach’s α = 0·93)(Reference Kliemann, Wardle and Johnson24). Further, the test–retest reliability of the overall NK score was high (r 0·84) in the Arabic GNKQ-R parallel to the English GNKQ-R (r 0·89)(Reference Kliemann, Wardle and Johnson24). In addition, all sections of NK showed good internal as well as test–retest reliability, suggesting that Arabic questionnaire is consistent in measuring NK. The reliability of the translated version of the NK questionnaires administered to university students in other countries including Uganda (r 0·89) and Turkey (r 0·86) was consistent with the present findings, while relatively higher than that reported in a study conducted in Kuwait (r 0·67)(Reference Al Saffar20,Reference Bukenya, Ahmed and Andrade25,Reference Alkaed, Ibrahim and Ismail29) .
As mentioned earlier, the translated version of the GNKQ-R revealed high construct validity with large effect size (d = 2·6), comparable to the English GNKQ-R (d = 1·2)(Reference Kliemann, Wardle and Johnson24). Significant differences in the levels of NK between the groups of students with (Nutrition/Dietetics major) and without (Arabic Literature major) nutrition background clearly established that the assessment tool was well constructed and showed high validity in the Arabic version as well. The review of literature revealed similar values for validity for the previously translated version of the NK questionnaires administered to university students in Kuwait, Uganda and Turkey(Reference Al Saffar20,Reference Bukenya, Ahmed and Andrade25,Reference Alkaed, Ibrahim and Ismail29) and to adults in an Australian community(Reference Hendrie, Cox and Coveney21).
Expected associations of small-to-medium effect sizes were found between NK scores and most of the demographic variables of the participants (gender, age, academic level and study discipline), demonstrating good convergent validity. Female participants and those in higher academic levels scored significantly higher than their respective counterparts in the overall and section-wise questionnaire, similar to the findings of the English GNKQ-R and previous UAE study(Reference Attlee, Abuqiya and Obaid22,Reference Kliemann, Wardle and Johnson24) . Our study documented small effect size associations between NK scores and age groups. While older students (21–30 years) obtained significantly higher NK scores than younger students (18–20 years) in the overall and section-wise questionnaire, NK scores for healthy food choices (Section 3) were similar in the university students irrespective of their age group. Lack of significant association of mean NK score values of Section 3 with age may be attributed to the narrow age grouping in the current study; university students are expected to make similar food choices in the age group of 18–30 years as reflected in our study. Our findings also showed that NK scores did not differ with marital status. However, a small effect size association was found in healthy food choices (Section 3); the mean score for this section was significantly higher in married than in single/unmarried students (6·1 (2·8) v. 5·1 (2·7)). Earlier, married adults in China had been reported to have obtained higher NK scores than single participants(Reference Liu, Xu and Liu30). As expected, the large effect size associations were established in the NK scores of participants studying in a health discipline (6·9 (2·9)) v. those in non-health disciplines (4·8 (2·4)). We did not find any associations of the NK scores with the self-reported health status of the participants. The English GNKQ-R, however, showed a small effect size association wherein NK scores were lower in adults with poor health status(Reference Kliemann, Wardle and Johnson24). Further, a small effect size significant association of self-reported BMI (highest in underweight BMI category = 6·3 (2·1)) with only healthy food choices (Section 3) in NK scores was observed. Previously, no significant correlation had been found between the levels of NK and BMI. The results from our study suggest that lack of knowledge may not be the sole significant factor in preventing adults with higher BMI from adopting a healthier diet(Reference O’Brien and Davies31).
A significant improvement was noted in the overall and sectional NK scores after the administration of the online nutritional information 2 weeks after the initial NK assessment(Reference Kliemann, Wardle and Johnson24), thereby establishing the sensitivity of the Arabic questionnaire to nutritional intervention. Medium-to-large effect size changes were evident in the overall and sectional scores. To elaborate, our findings showed significant, large effect size changes in the NK scores on the overall questionnaire, in food groups (Section 2) and diet–disease relationship (Section 4). However, a similar effect size change was reported only in dietary recommendation (Section 1) of English GNKQ-R(Reference Kliemann, Wardle and Johnson24). Further, contrary to the findings of our study, Kliemann et al.(Reference Kliemann, Wardle and Johnson24) could not document any significant change in the NK scores of healthy food choices (Section 3) post nutritional intervention. The nutrition information provided in our study was based on the recent dietary guidelines from the Arab region(26,27) which might have been better aligned with the required information in all sections of our questionnaire. This might have contributed to the significant improvement in the NK scores for the overall questionnaire and for all four sections, including the healthy food choices section, in our study.
Although the current study established good reliability and validity of the Arabic version of the GNKQ-R, it has certain limitations. For convenience and homogeneity, the study population was restricted to university students in Jordan and UAE, which limits the generalisability of the results to the entire Arab population. University students represent a better-informed section of society than the young population in general. Research supports that higher levels of NK are demonstrated in individuals with higher levels of education(Reference Deniz and Alsaffar32) and among females(Reference Attlee, Abuqiya and Obaid22), indicating that the findings of the current study are limited to the context in which it was undertaken. Further validation of Arabic GNKQ-R is required before being administered on more diverse samples from both genders, such as children, older adults and mixed socio-economic groups within the Arabic populations. Moreover, the possibility that participants guessed or searched online for the correct response was a further limitation. However, to reduce guessing, the participants were instructed clearly to check the ‘not sure’ response provided for all questions rather than guess an answer. Additionally, the participants were not allowed to go back and edit their responses at any point. The average time spent to complete each online questionnaire was similar to the anticipated time, suggesting that most participants did not try to search for correct answers while completing the questionnaire.
Conclusion
Currently, there is an absence of a valid tool in the Arabic language to assess the general NK of adults in middle-eastern Arab countries. The eighty-six-item Arabic version of the English GNKQ-R can be considered a reliable and valid tool for assessing NK among the young adult Arab population. In addition to the overall questionnaire, each section demonstrated adequate reliability and can be employed independently to assess NK in specific areas. Such an assessment tool can be instrumental in determining gaps in NK and developing targeted nutritional interventions to address chronic diseases and other health problems among adults in Arab countries. Future research is required to explore the generalisability and applicability of the Arabic GNKQ-R to different sections of the population such as children and older adults across different Arab countries in the middle-eastern region.
Acknowledgements
Acknowledgements: We thank both the Universities of our affiliations for providing support in conducting the current study and the participants who agreed to be a part of different phases of the study. A special thanks to Dr Helen Croker, Senior Research Associate at University College London for her technical review of the manuscript. We acknowledge Ms. Eiman Mansour Marzouqi for her assistance in the data collection. Financial support: The current research received no specific grant from any funding agency, commercial or not-for-profit sectors. Conflict of interest: There are no conflicts of interest. Authorship: Both authors were equally involved in formulating the research question, designing the study, carrying it out, analysing the data and writing the article. Both authors confirm their final approval of the submitted version to be published. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and the Research Ethics Committees at the UAEU (ERS_2018_5731), and HU (RA/122/1 703 000) approved all procedures involving research study participants. Written informed consent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020002724.







