



Consumption of sugar-sweetened beverages (SSB) is associated with weight gain, increased risk of hypertension, type 2 diabetes mellitus, CHD and stroke(Reference Hu and Malik1–Reference Xi, Huang and Reilly6). Findings from the Framingham Heart Study suggest that soft drink consumption is associated higher incidence of adverse metabolic risk factors among middle-aged adults(Reference Dhingra, Sullivan and Jacques7). More recent evidence from US cohort studies indicates that SSB consumption is associated with CVD mortality and exhibits a dose–response association(Reference Malik, Li and Pan8). Consumption of SSB may increase mortality by inducing cardiometabolic risk and various chronic disorders(Reference Malik, Li and Pan8–Reference Siqueira, Pereira and Velasquez-Melendez11).
Meta-analyses demonstrate that SSB may be surrogates for specific food preferences(Reference Kelishadi, Heshmat and Mansourian12–Reference Rodríguez-Monforte, Sánchez and Barrio14). The relationship between SSB consumption and obesity risk may arise partially mediated by unhealthy dietary behaviours(Reference Grimes, Riddell and Campbell15). Thus, high SSB consumption may be a proxy for clustered unhealthy dietary habits and lifestyles(Reference Narain, Kwok and Mamas13). A westernised diet is marked by increased consumption of SSB, snacks, baked desserts and liquid carbohydrates in added sugars. Adopting this dietary pattern is associated with an increased risk of metabolic disorders(Reference Martínez-González and Martín-Calvo16). Studies linking western dietary pattern to metabolic risks(Reference Rodríguez-Monforte, Sánchez and Barrio14,Reference Esmaillzadeh, Kimiagar and Mehrabi17–Reference Suliga, Kozieł and Cieśla19) primarily utilise cluster analyses, exploratory factor analyses and principal component analyses to assess dietary patterns reported on FFQ. However, the role of SSB consumption in dietary practices leading to metabolic risks remains unclear(Reference Malik and Hu20).
Westernisation of local diet in Asian countries has increased over the past few decades, resulting in greater intake of high-sugar and energy-dense foods(Reference Peng, Lin and Guo21,Reference Pingali22) . Taiwan, an increasingly industrialised Asian country experiencing rapid economic and income growth, has demonstrated more widespread adoption of westernised dietary patterns than other Asian countries(Reference Peng, Lin and Guo21). While this gradual westernisation of the cuisine may reflect successful economic development, it simultaneously carries significant public health implications. In SSB, in addition to Western-style coke, soda and energy drinks, hand-shaken beverages (e.g. tapioca milk tea, fruit juice and fruit tea) are also popular in Taiwan. A recent qualitative study revealed that hand-shaken drinks are common for daily SSB consumption among Taiwanese adolescents(Reference Wang, Chen and Chan23).
In Taiwan, previous studies of adolescents aged 12–18 years have linked high SSB consumption to metabolic risk components(Reference Chan, Lin and Huang24,Reference Lin, Lee and Tsai25) and elevated serum uric acid levels(Reference Shih, Chang and Wu26). A private health screening and management institution collected data from screening centres in four major cities in Taiwan, generating further repository studies. One such study of adults over 35 years of age indicated that meat-rich and highly processed diets characterised by high levels of animal protein, saturated fat, sweetened foods and SSB, were associated with metabolic syndrome components(Reference Syauqy, Hsu and Rau27). Another study using the same data source found that westernised dietary patterns were no longer associated with high TAG or low HDL cholesterol in adults between 20 and 50 years of age after adjusting for covariates(Reference Lin, Hsu and Lee28).
For sex differences, meta-analysis has stratified sexes for the association between SSB intake and cardiovascular outcomes (e.g. myocardial infarction and stroke)(Reference Narain, Kwok and Mamas29); however, there is a shortage of information regarding differential associations between SSB consumption and metabolic risks across sexes(Reference Malik and Hu20,Reference Kang and Kim30) . Although health promotion policies in Taiwan have heavily focussed on tobacco and alcohol abuse prevention, the adverse health effects of SSB consumption have not received the same attention(31). An enhanced understanding of the sex differences in the association of SSB consumption with metabolic risks may provide valuable insights for designing health promotion strategies. Thus, the objective of this study was to examine the relationship between SSB consumption and metabolic risks for men and women.
Methods
Data source
This study used data collected between 2005 and 2014 during a large-scale community-integrated health screening project conducted in Changhua County, including Changhua City, Taiwan. Changhua County (population, 1·3 million; area, 1074 km2) is located on the west coast of Taiwan, and Changhua City is situated in the northern part of the county. Changhua County is less urbanised than Taipei and comprises two suburban cities, six suburban townships and eighteen rural townships. The Changhua County Health Bureau implemented the community-integrated health screening service in 2005 and has since conducted screenings annually from April to September. The integrated service provides citizens 30 years of age and older with comprehensive health check-ups that include cancer and chronic disease screenings and blood serum tests.
Public health practitioners and medical professionals conducted face-to-face questionnaire interviews with patients. Information on eating habits, health practices, lifestyle behaviours and personal medical history was recorded. If screenings show adverse findings, citizens receive health screening reports and subsequent referrals to public health or health care services. Between 2005 and 2014, the integrated health service screened 92 724 individuals in Changhua County, approximately 10 000 people annually. In alignment with our study objectives, we limited our analysis to the working-age group, ultimately including 75 278 individuals between 30 and 64 years of age. The data included demographics, health practices, lifestyle behaviours, dietary patterns and blood serum results. The Institutional Review Board of Taipei Medical University approved using this data (N2011611014).
SSB consumption
The health screening questionnaire assessed respondents’ dietary patterns over 6 months. The SSB item included carbonated beverages (e.g. soda and coke), milk tea and juice, including juice derived from asparagus. Respondents categorised weekly SSB intake frequency as seldom or never, 1–2 times, 3–4 times, 5–6 times or 7 or more times. Given the small proportion of participants consuming SSB 7 or more times/week (4·5 %), we combined the last two categories as ‘5 or more times’ in the analysis.
Metabolic risks
Health screening procedures included blood serum tests, which generated metabolic risk data. We characterised metabolic risk indicators dichotomously as ‘normal’ or ‘abnormal’ following International Diabetes Federation (IDF) and the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) definitions (Alberti et al., 2005; National Cholesterol Education Program, 2002). Abnormal values included unhealthy waist circumference (≥90 cm in men and ≥80 cm in women in Taiwan) and elevated TAG (≥150 mg/dl), total cholesterol (≥200 mg/dl), LDL (≥130 mg/dl), fasting plasma glucose (≥100 mg/dl) and blood pressure (systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg).
Covariates
Covariates employed in this study included sex (male, female), age (years), educational attainment (less than elementary school, junior high school, high school, college, and advanced degrees), occupation (unemployed, professional careers, service industry/sales, agriculture/forestry/fishing/animal husbandry or unskilled labour), tobacco use (smoker or non-smoker), alcohol use (drinker or non-drinker), engagement in regular physical exercise (yes/no), weight monitoring habits (yes/no) and history of health check in the preceding year (yes/no). Systematic reviews and meta-analyses studies demonstrate that covariates are crucial for generating meaningful study results(Reference Rodríguez-Monforte, Sánchez and Barrio14). Although most studies link dietary patterns and metabolic risk adjust for sex, age and physical activity level, most studies do not account for BMI, a well-known risk factor for metabolic syndromes(Reference Narain, Kwok and Mamas13,Reference Rodríguez-Monforte, Sánchez and Barrio14) . Therefore, to ensure the robustness of our results, we further controlled for BMI in addition to other covariates. Additionally, we considered specific dietary patterns and food items (e.g. snacks, seafood, beans, egg products, breakfast, fruit, milk and tea) reported in FFQ as potential confounding variables in the association between the SSB consumption and metabolic risks(Reference Martínez-González and Martín-Calvo16).
Statistical analysis
To illustrate participant demographics, we presented mean and SD values for continuous variables while providing number and percentage values for categorical variables. In addition, we conducted sex-stratified logistic regression models to examine the relationship between SSB consumption and metabolic risks in males and females. In the analysis, we designated SSB intake frequency as a dummy variable while using the ‘seldom/never’ intake response as a reference group. We first controlled for demographics, health practices, lifestyle behaviours, and other dietary patterns in Model 1, then adjusted for BMI in Model 2 (except when waist circumference was the dependent variable). To check the robustness, we dichotomised BMI into nonobese (BMI < 27) and obese (BMI ≥ 27) categories and performed subgroup analyses. We conducted all statistical analyses using SPSS (version 25.0; SPSS) and considered P values below 0·05 statistically significant. All analyses were two-tailed.
Results
Participant characteristics
Table 1 presents demographics, SSB intake frequency, metabolic risks and lifestyle habits among the 75 278 participants included in the study sample. There were 27·1 % of men (n 20 363) and 72·9 % of women (n 54 915). The mean age among males (52·1 ± 8·8 years) was higher than that of females (49·3 ± 7·3 years). Regarding SSB intake frequency, 62·7 % of men and 68·8 % of women reported that they rarely or never consumed SSB. Conversely, 17·9 % of men and 16·1 % of women reported drinking SSB once or twice/week. Approximately one in ten men (9·8 %) and 7·3 % of women reported consuming SSB more than 5 times/week. In terms of metabolic risk factors, men demonstrated higher rates of elevated serum TAG (34·5 %), fasting glucose (27·5 %) and hypertension (60·2 %). In comparison, women had higher rates of abnormal waist circumference (38·4 %) as well as elevated total cholesterol (43·9 %) and LDL levels (33·9 %). Notably, men were more likely than women to be current smokers (36·2 %), current drinkers (55·0 %) and living with obesity (25·6 %).
Table 1 Participant demographics, SSB intake frequency, metabolic risks and lifestyle habits (n 75 278)
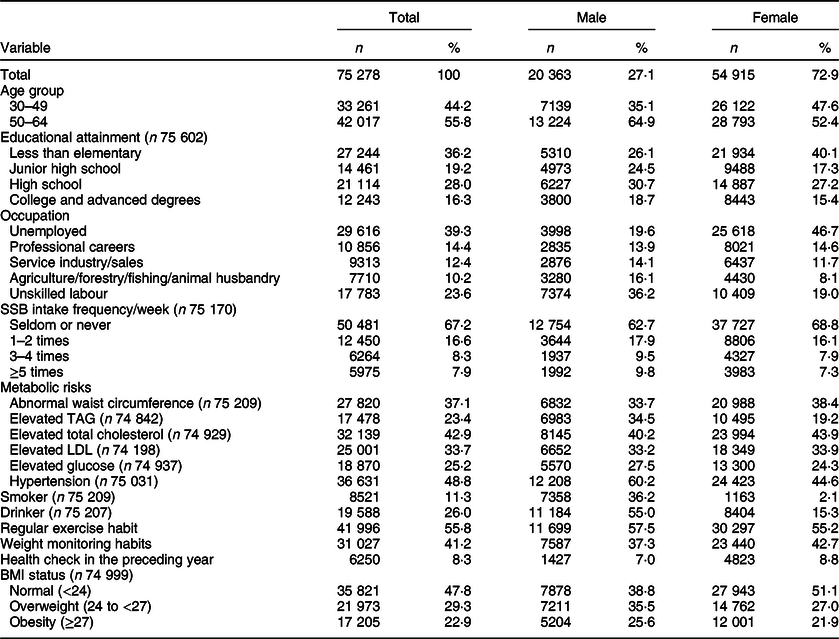
SSB, sugar-sweetened beverage.
Association between SSB consumption and metabolic risks
After controlling for sex, age, education, occupation, health practices, lifestyle behaviours and other dietary habits, logistic regression models demonstrate that SSB intake frequency was associated with metabolic risks (Table 2, Model 1). Compared to those who report rarely or never consuming SSB, participants endorsing greater frequency of SSB consumption displayed increased risk for abnormal waist circumference and elevated TAG, total cholesterol and LDL in both men and women. More frequent SSB consumption was also associated with higher glucose levels and hypertension in women. For women, consuming SSB 1–2 times/week (v. rarely or never consuming SSB) yielded increased OR of 1·244 (P < 0·001) for abnormal waist circumference, 1·068 (P < 0·05). For elevated TAG, 1·083 (P < 0·01) for elevated total cholesterol, 1·115 (P < 0·001) for elevated LDL, 1·119 (P < 0·001) for elevated glucose and 1·127 (P < 0·001) for hypertension. Logistic regression models continue to display similar patterns with BMI as a control variable. However, the relationships appear attenuated (Table 2, Model 2).
Table 2 Logistic regression model of SSB consumption with metabolic risks in men and women
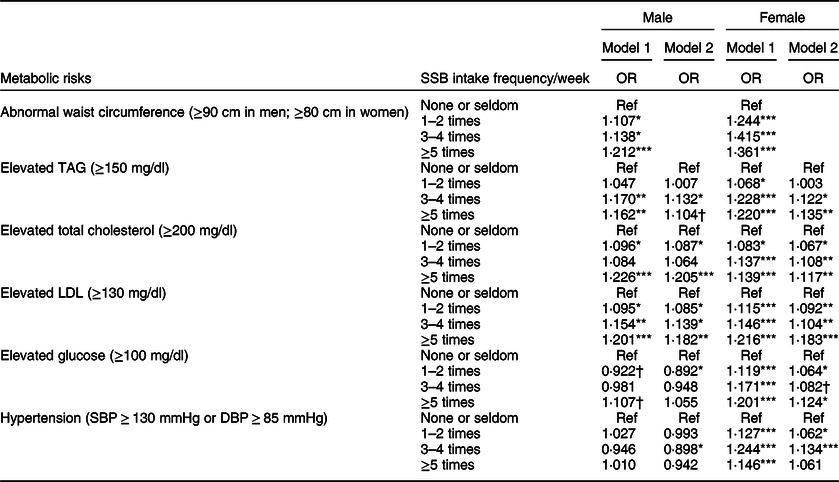
SSB, Sugar-sweetened beverage; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
†P < 0·1; *P < 0·05; **P < 0·01; ***P < 0·001.
Model 1 adjusted for gender, age, educational attainment, smoking status, drinking status, regular exercise habit, check weight habit, health check-up within 1 year and other dietary patterns (snacks, breakfast, seafood, beans, egg products, fruit, milk, coffee and tea).
Model 2 further adjust for BMI in addition to the covariates in Model 1.
Subgroup analyses
We also conducted a BMI-stratified analysis, dividing participants into subgroups with and without obesity while controlling for all covariates except BMI (Table 3). We found that SSB consumption was more strongly linked to metabolic risks in participants without obesity. Among men who consumed SSB 5 or more times/week (v. those who rarely or never drink SSB), the OR were 1·248 (P < 0·001) for excess total cholesterol and 1·234 (P < 0·001) for excess LDL. Notably, among women without obesity, SSB consumption was associated with all metabolic risks. Among women who consumed SSB 5 or more times/week compared to those who rarely drink SSB, the OR for metabolic risks ranged from 1·107 (P < 0·01) to 1·307 (P < 0·001). On the other hand, in participants with obesity, greater SSB intake frequency was associated with elevated fasting glucose levels in men and abnormal waist circumference in women.
Table 3 Logistic regression model of SSB consumption with metabolic risks in samples with and without obesity
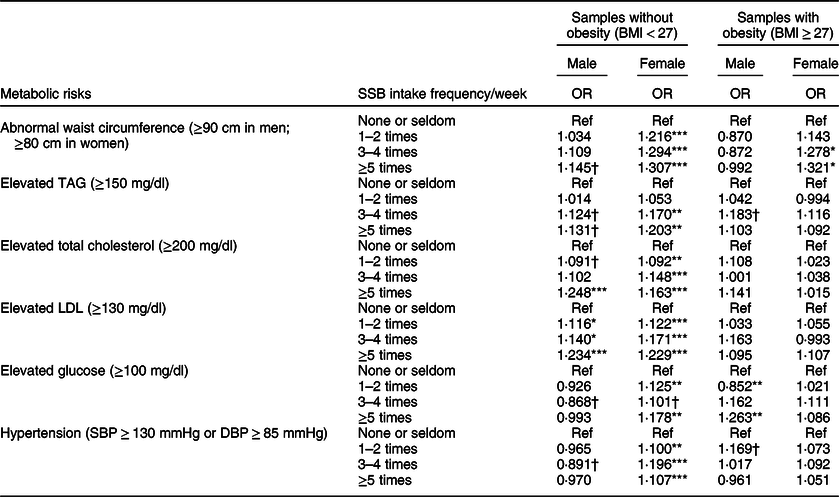
SSB, sugar-sweetened beverage; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
†P < 0·1; *P < 0·05; **P < 0·01; ***P < 0·001.
All models adjusted for sex, age, educational attainment, BMI, smoking status, drinking status, regular exercise habit, check weight habit, health check-up within 1 year and other dietary patterns (snacks, breakfast, seafood, beans, egg products, fruit, milk, coffee and tea).
Discussion
Using large-scale health screening data collected from Taiwanese communities, we found that SSB consumption was associated with a greater risk for abnormal waist circumference, elevated TAG, total cholesterol and LDL in men and women. SSB intake was also associated with high fasting glucose and hypertension in women. Compared to participants who rarely or never consume SSB, those reporting intake frequencies of just 1–2 times/week demonstrate increased rates of metabolic risks. Notably, our findings revealed that the relationships between SSB consumption and metabolic risks were more pronounced in subgroups without obesity, especially for women. This finding suggests that SSB intake may increase metabolic problems in the population without obesity.
Our findings were consistent with relevant studies, namely that more frequent consumption of SSB was positively associated with metabolic risks. A noted marker of unhealthy dietary patterns, SSB are considered a primary source of added sugar and liquid carbohydrates. They are associated with increased waist circumference, weight gain, obesity and higher levels of adverse cardiometabolic biomarkers(Reference Narain, Kwok and Mamas13,Reference Martínez-González and Martín-Calvo16,Reference Yu, Ley and Sun34) . Randomised controlled trials have shown that decreasing SSB consumption significantly reduces weight gain among children of average weight(Reference Ruyter, Olthof and Seidell35) and adolescents with overweight and obesity(Reference Ebbeling, Feldman and Chomitz36). A meta-analysis of prospective studies indicated that SSB consumption was associated with a greater risk of CHD(Reference Huang, Huang and Tian2), type 2 diabetes(Reference Malik, Popkin and Bray3,Reference Schwingshackl, Hoffmann and Lampousi37) and overall mortality(Reference Schwingshackl, Schwedhelm and Hoffmann38).
Existing literature supports sex differences in the relationship between SSB consumption and health outcomes(Reference Kang and Kim30,Reference Lin, Hsu and Lee39) . A meta-analysis has suggested that women who consume SSBs have a higher relative risk of ischaemic stroke(Reference Narain, Kwok and Mamas29). In metabolic risks, one Korean study used data from a large-scale community-based cohort (n 10 030 Korean adults, age = 40–69 years) and found that SSB intake frequency was only associated with increased incidence of metabolic syndrome in women(Reference Kang and Kim40). However, another study using the same data source found a positive association between total sugar intake and metabolic syndrome in middle-aged Korean men(Reference Seo, Kim and Kwon41). Another Korean analysis using response data from the 2012–2016 Korean National Health and Nutrition Examination Survey (KNHANES) included respondents between 35 and 65 years of age and only observed an association between SSB and metabolic syndrome in women(Reference Shin, Kim and Ha42). Our study contributed to the literature by revealing that the associations between SSB intake and metabolic risks were more pronounced in women, particularly those without obesity. One possible explanation for the sex differences in the role of sex hormones such as oestrogen(Reference Kang and Kim40–Reference Shin, Kim and Ha42). In women, oestrogen positively affects the renin–angiotensin system, increasing fat transport and promoting serum TAG and lipoprotein levels, whereas, in men, androgen exhibits the opposite effect(Reference Knopp, Paramsothy and Retzlaff43). As a result, lipid levels in men and women may be regulated differently. TAG and lipoprotein levels appear to be more sensitive to changes in dietary carbohydrates or fats in women than in men. Sex hormones may have contributed to a stronger link between SSB consumption and hypertriglyceridaemia and metabolic syndrome in women due to changes in lipid metabolism(Reference Kang and Kim40).
In Taiwan, studies of adolescents between 12 and 18 indicate that SSB intake is associated with a greater risk of adolescent metabolic syndrome, especially in boys(Reference Chan, Lin and Huang24,Reference Lin, Lee and Tsai25) . On the contrary, a study of 14 087 subjects (age = 20–50 years) with both dyslipidaemia and elevated fasting glucose levels supported the relationship between Western dietary patterns and general adiposity, central adiposity and higher body fat percentage (>30 % for men and >25 % for women) in both sexes(Reference Lin, Hsu and Lee39). A study of middle-aged Taiwanese adults found that the association between westernised dietary patterns and elevated TAG and LDL cholesterol became insignificant after adjusting for BMI and other covariates(Reference Lin, Hsu and Lee28). This finding aligns with a review study that indicates that adjusting for BMI may attenuate the association between westernised dietary patterns and metabolic risk, suggesting that obesity may have a mediating effect in this pathway(Reference Malik and Hu20). Previous meta-analyses also noted that most studies do not control for BMI(Reference Narain, Kwok and Mamas13,Reference Rodríguez-Monforte, Sánchez and Barrio14) , and over-adjustment may lead to underestimating the link between SSB consumption and health risks(Reference Lazzinnaro, Plourde and Johnson-Down44–Reference Schisterman, Cole and Platt46). Our findings expand on existing literature by demonstrating that greater SSB intake frequency was associated with higher rates of metabolic risks even after controlling for BMI.
Strengths and limitations
This study is the first to use a large sample to examine sex differences in the relationship between SSB consumption and metabolic risks in Taiwan. Notably, we derived metabolic risk data from blood serum tests instead of self-reported responses. Our statistical power and objective data measures enable us to provide robust evidence linking SSB consumption and metabolic risk.
This study also has limitations. First, due to the cross-sectional nature of our study design, we were unable to demonstrate a causal association between SSB consumption and metabolic risk. However, most studies indicate that increased SSB intake leads to the development of metabolic risk and that the relationship is not bidirectional. Second, most study participants were from Changhua County communities, limiting the generalisability of study results despite minimising potential confounding variables related to local socioeconomic factors. Lastly, we lacked data for total energy intake and salt intake as control variables; this gap is significant because energy and salt/Na intake are important confounds in associations of metabolic risk(Reference Grimes, Riddell and Campbell15,Reference Chen, Gu and Huang47,Reference Willett, Howe and Kushi48) . However, adjusting for total energy intake may understate the relationship between SSB and metabolic risk because energies may mediate the association between SSB consumption and weight gain(Reference Malik and Hu20). Instead of controlling for total energy intake, we adjusted for BMI and various characteristics (i.e. occupation, exercise frequency, weight monitoring habits, health behaviours and different dietary patterns) to reduce extraneous variation.
Conclusion
In conclusion, this study suggests that SSB intake is linked to abnormal waist circumference, elevated TAG, total cholesterol and LDL among working-age male and female community members. SSB consumption is also associated with high fasting plasma glucose levels and increased blood pressure among women. Women who are not obese may overlook the health risks associated with SSB. These findings indicate the need for health promotion programmes to expand their scope beyond tobacco or alcohol-related interventions and build community awareness of the health hazards associated with SSB. For example, young and middle-aged adults may benefit from social marketing strategies that provide more comprehensive education on the health consequences of SSB consumption. Health policies should also promote healthy alternatives to SSB, such as sugar-free yogurt drinks or milk. Implementing these strategies will necessitate future research evaluating the interventions’ effectiveness in reducing metabolic risk in the working-age population.
Acknowledgements
Acknowledgements: We thank all the participants who helped finish the questionnaire and health check-up. Financial support: This work was financially supported by the Ministry of Science and Technology (grant number MOST 107-3017-F-002-003) and the ‘Innovation and Policy Center for Population Health and Sustainable Environment (Population Health Research Center, PHRC), College of Public Health, National Taiwan University from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan (NTU-107L9003). Authorship: All authors significantly contributed to the manuscript. D.R.C., C.T.K., C.C.C., Y.P.Y. and H.H.C. conceived and planned the study. C.T.K. and D.R.C. analysed the data and drafted the manuscript. D.R.C. and C.T.K. contributed to interpreting results, critically reviewed the manuscript. D.R.C., C.T.K., C.C.C., Y.P.Y. and H.H.C. reviewed and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Taipei Medical University Joint Institutional Review Board (N2011611014). Written informed consent was obtained from all subjects/patients.
Conflict of interest:
There are no conflicts of interest.




 Open access
Open access