


There is an ongoing need to improve eating habits and offer preventive approaches for weight management in the USA(1–Reference Mokdad, Bowman and Ford3). The Internet offers great possibilities in this regard because information can be sent to a very large audience at a relatively low cost. Our nutrition research group, made up of physicians, dietitians and nutritionists from Boston University Medical Center, Duke University Medical Center and the USDA Human Nutrition Center on Aging at Tufts University, has developed an online lifestyle modification programme based on the DASH (Dietary Approaches to Stop Hypertension) diet. The DASH Online Questionnaire (OLQ) was created to capture food intake and provide real-time feedback in the form of progress reports to participants enrolled in the DASHforHealth.com programme. The aim of the DASHforHealth.com programme is to provide easily accessible nutrition education for those seeking to improve their health and/or combat weight issues via the Internet. Data collected using the DASH OLQ showed that participants significantly increased their daily fruit and vegetable consumption after one year in the DASHforHealth.com online programme(Reference Moore, Alsabeeh and Apovian4). The DASHforHealth.com programme is currently being offered to several US corporations as an employee wellness programme, as well as to the general public for individual subscription. We chose the DASH diet as the focus of our web-based educational programme because of its proven benefits in the areas of blood pressure reduction, cholesterol reduction, improvement of bone density, effectiveness when combined in a weight-loss programme, and protection against heart disease and stroke(Reference Appel, Moore and Obarzanek5–Reference Lin, Ginty and Appel12). The DASH diet is a diet rich in fruits, vegetables, whole grains and low-fat dairy products, and reduced in meats, sugary sweets and fat (for example, for an energy intake of 8368 kJ (2000 kcal) the DASH diet would recommend the following servings: 4 fruit, 4 vegetable, 2·5 low-fat dairy, 7 grain, 1·5 meat/fish/poultry, 0·5 nuts/seeds/legumes, 2 added fats and 0·5 sweets)(Reference Moore13). The DASH diet is part of the therapeutic lifestyle changes recommended for patients with hypertension by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure(Reference Chobanian, Bakris and Black14). In addition, the DASH diet is recommended by the US Department of Agriculture (USDA) as a healthy eating pattern for all American adults(15).
Previous reports have demonstrated that subjects who keep track of what they eat (self-monitoring) adhere better to a dietary modification plan(Reference Wing and Hill16). However, existing methods of assessment tend to be cumbersome, discouraging compliance(Reference Kushi17–Reference Blanton, Moshfegh and Baer19). Therefore, we created a self-monitoring tool designed to capture changes made in dietary behaviours as a result of the DASHforHealth.com online programme with the caveat that the tool be quick and easy to use. This tool was designed as a brief online questionnaire that captured the consumption of servings in the various food groups, as recommended in the DASH diet. In order to test the utility of this tool we validated this online questionnaire (the DASH OLQ) v. the Block 98.2 Food Frequency Questionnaire (FFQ) as our gold standard. The present paper describes the design and the results of this validation study.
Subjects and methods
Subjects and recruitment
Subjects were recruited by mass email sent to 4000 faculty and staff of Boston University Medical Center. A total of 235 individuals enrolled in under 3 h using an online process. Among these individuals, 191 completed the criteria for inclusion in the study: completion of four DASH OLQ and one Block FFQ.
Study design
Subjects completed a demographic questionnaire which included questions about age, gender, race and educational level. They consumed their usual, free-choice diets throughout the study period. Study subjects were asked to complete the DASH OLQ once each week for four weeks including one weekend day and to complete the Block 98.2 FFQ once, between weeks 2 and 4 of the study period. Reminder emails were sent to study participants with a link to the online questionnaire. Subjects logged on to the online questionnaire to enter their food items. Subjects were also encouraged to email any questions to the study coordinator. Results of the four DASH OLQ were averaged and then compared with the Block FFQ. Comparison across instruments was conducted both at the nutrient and food group levels. Online informed consent was obtained from subjects at the time of recruitment. The Institutional Review Board at Boston University Medical Center approved the study.
Development of the DASH Online Questionnaire
The DASH OLQ was developed through collaborative efforts of a team of nutritionists and clinical researchers at Boston University School of Medicine, the USDA Human Nutrition Research Center on Aging at Tufts University and Duke University Medical Center. The goal of this team was to design a relatively simple dietary data collection and self-monitoring tool. It was created to be a self-administered assessment of dietary intakes for those enrolled in a web-based nutrition and physical activity education programme (DASHforHealth.com). Unlike traditional FFQ, the DASH OLQ requires individuals to recall intakes over the previous 24 h only, based upon the concept of a 24 h dietary recall. Commonly eaten foods are grouped into eleven categories with additional questions asked to address Na and fat intake (Fig. 1). The programming of the DASH OLQ reassembled the eleven food categories into the eight DASH food groups based on ingredients. For example, the DASH OLQ has a category for drinks. From the drink category, 100 % fruit juice would be analysed as a fruit serving (6 oz equals one serving) whereas sugar-sweetened beverages count as a serving of sweets (6 oz equals one serving). For the validation study, single-day food intake was captured at four time points and averaged in order to assess general dietary patterns to be compared with the Block FFQ.
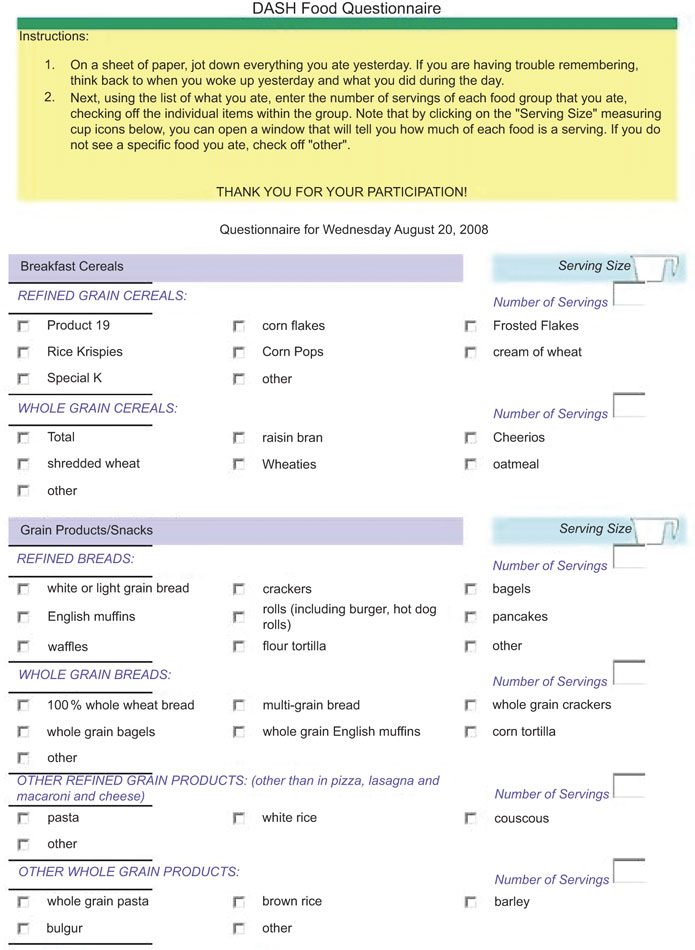
Fig. 1 A sample of the DASH Online Questionnaire
After its development the questionnaire was converted to HTML format with check boxes and entry fields for self-administration and was placed on a secure web server at Boston University’s Data Coordinating Center. Informal testing for ease of use and understandability was done on a subset of ten people.
Administration of the DASH Online Questionnaire
The DASH OLQ was self-administered at the location of choice by subjects once each week for four weeks. To complete the DASH OLQ, participants were asked to recall and record all foods and approximate amounts eaten the day before on paper. They were then instructed to place a check next to the corresponding foods on the questionnaire and indicate the number of servings of each food consumed in designated entry fields. To aid in the estimation of serving sizes, clickable images were created for each food category as a reference; e.g. the fruit illustration showed 1 medium orange, 1/2 cup of sliced fruit or berries, 6 oz of 100 % fruit juice and 1/4 cup of dried fruit (Fig. 2). Food groups included: breakfast cereal; dairy; drinks; fats and oils; fruits; grain products and snacks; meat, fish and poultry; mixed dishes; sweets; vegetables; and nuts, seeds and legumes. These broad food group categories were further broken down into subcategories with individual food items that could be selected by clicking the appropriate check box (Fig. 1).
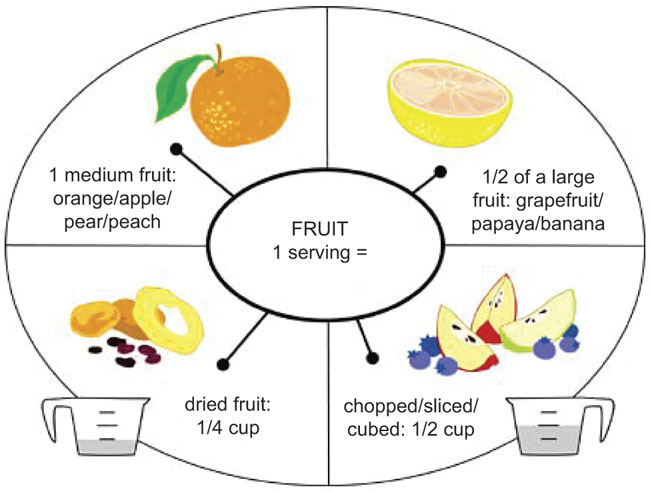
Fig. 2 Fruit illustration for estimating serving size when completing the DASH Online Questionnaire
Administration of the Block FFQ
The paper-and-pencil 110-question Block 98.2 FFQ was self-administered at the location of the subjects’ choice between weeks 2 and 4. The Block 98.2 FFQ measures food intake by asking participants to estimate how often they had eaten foods over the past year. Users were referred to a corresponding illustration of plates of different sizes with differing amounts of food on them to aid in serving size estimation. Completed questionnaires were either mailed back to the research office or hand-delivered to the research coordinator. Upon receipt, the Block FFQ was checked for completeness, and then sent to NutritionQuest (Berkeley, CA, USA) for data scanning and nutrient calculations. These results were returned to the USDA Human Nutrition Research Center on Aging at Tufts University for analysis. A total of 191 subjects completed the Block FFQ.
Statistical methods
The FFQ was scored through a scanning technique. Food frequency, nutrient and serving size data were obtained from the questionnaire through NutritionQuest (www.nutritionquest.com). Both the Block and DASH servings were converted to gram weights and compared using four different levels of adjustment. First, correlations were calculated with no adjustment. Second, deattentuated correlations were calculated using the formula suggested by Willett(Reference Willett20). Intra/inter-individual variance ratios for the four days of reported DASH group intakes were calculated with the VARCOMP procedure in the SAS statistical software package version 9·1·3 (SAS Institute, Cary, NC, USA) to control for day-to-day variability in intake. Third, an energy-adjusted correlation was done, and finally an energy-adjusted, deattentuated correlation was performed. Finally, agreement between the two data collection tools was calculated using kappa statistics.
Comparison of foods by category
To compare the DASH OLQ against the Block FFQ, gram weights of each DASH food group were averaged across all four completed questionnaires. Gram weights were then converted back into DASH servings. Food group analysis was done by calculating DASH serving sizes from gram weights of Block foods and then summing these servings into each of the eleven DASH food groups. These entries were compared with the gram weights reported on the Block FFQ. Subgroups of breakfast cereals and mixed dishes were analysed individually because of the variability of these two items and also because it is difficult to estimate serving sizes from mixed dishes. Pearson correlation coefficients for the within-subject DASH OLQ v. Block FFQ for each DASH food group were computed.
Comparison of nutrients
Nutrient analysis was done by converting food intake reports from the OLQ from DASH servings to gram weights and then calculating nutrient intakes using a 100 g nutrient reference table, built using the USDA National Nutrient Database for Standard Reference version 18 (2001). Pearson correlation coefficients were then computed.
Results
The demographic characteristics of the participants are given in Table 1. The study population was 75·5 % female and 24·5 % male, and the population was multi-ethnic. The study population was highly educated; fifty-nine respondents had some postgraduate work, fifty-nine completed college, twenty-four attended some college, six had a high school degree and one attended some high school. Three respondents did not report their level of education.
Table 1 Demographic characteristics of the study population: volunteers from faculty and staff of Boston University Medical Center (Boston, MA, USA), recruited by email
Comparisons of the DASH Online Questionnaire and Block FFQ by food group
Eleven DASH food groups were compared with the Block FFQ. Significant positive correlations between the Block FFQ and the DASH OLQ were found for all eleven DASH food groups. Correlations were as follows: breakfast cereals (r = 0·67), drinks (r = 0·62), fruit (r = 0·61), nuts, seeds and legumes (r = 0·80) and dairy (r = 0·70). Lower, but still significant correlations were seen for meat, fish and poultry (r = 0·49), vegetables (r = 0·31), fats and oils (r = 0·34), grains (r = 0·41), mixed dishes (r = 0·32) and sweets (r = 0·51). Deattenuated correlations ranged from r = 0·41 for vegetables to r = 0·93 for nuts, seeds and legumes (Table 2). Mean intakes across instruments did not differ significantly for vegetables, drinks or mixed dish groups. However, significant differences were found for the remaining eight food groups.
Table 2 Mean intakes and Pearson’s correlations between the DASH OLQ and the Block 98·2 FFQ for intakes of food by DASH food group: volunteers from faculty and staff of Boston University Medical Center (Boston, MA, USA), recruited by email (n 191)

DASH, Dietary Approaches to Stop Hypertension; OLQ, online questionnaire.
Comparisons of the DASH Online Questionnaire and Block FFQ by nutrients
Comparison of the two assessment methods showed significant positive correlations for all nutrients ranging from r = 0·44 for Zn to r = 0·69 for Mg, P and riboflavin. Deattenuated correlations were even stronger, ranging from r = 0·55 for Zn to r = 0·80 for riboflavin and P. Mean intakes across instruments did not differ significantly for energy, carbohydrate, vitamin A, vitamin C, riboflavin, thiamin, vitamin B6, Fe, Zn or K (Table 3), but were significantly higher for the Block FFQ v. the DASH OLQ for fat, vitamin E and foliate, and higher for the DASH OLQ v. the Block FFQ for protein, Na and P.
Table 3 Mean intakes and Pearson’s correlations between the DASH OLQ and the Block 98·2 FFQ for energy and nutrient intakes: volunteers from faculty and staff of Boston University Medical Center (Boston, MA, USA), recruited by email (n 191)

DASH, Dietary Approaches to Stop Hypertension; OLQ, online questionnaire; RE, retinol equivalents; TE, α-tocopherol equivalents.
All correlations were significant: P < 0·0001.
Weighted kappa statistics were performed to determine the level of agreement the DASH OLQ had with the Block FFQ by energy level. A value of 0·48 (95 % CI 0·38, 0·57; P < 0·0001) or ‘moderate’ agreement was observed.
Discussion
Overweight and obesity in the USA are at an all-time high, mainly due to unhealthy eating patterns as well as little physical activity. Unhealthy eating patterns and obesity are associated with co-morbidities such as hypertension, elevated lipids and type 2 diabetes. Solutions to the rising health-care burden include modification of dietary intake to reduce the costs associated with nutrition-related chronic disease. Research in dietary food patterns requires methods of capturing food intake. Although nutritional biological markers are the most accurate way to detect dietary consumption, they are expensive and impractical for the general public(Reference Potischman and Freudenheim21, Reference Bingham, Gill and Welch22). The low cost and simplicity of self-administered dietary recall questionnaires facilitates their use in large populations and is the primary method of dietary intake data collection in most epidemiological studies(Reference Mellen, Gao and Vitolins23, Reference Buzzard, Faucett and Jeffery24). However, most FFQ are administered on paper and are thus cumbersome to administer and analyse.
The Internet presents a promising mode of disseminating nutrition education on the population level, and an online dietary intake assessment tool would conveniently track change in lifestyle for nutrition research. FFQ are used to measure average long-term dietary patterns rather than to provide an exact estimate of short-term intake(Reference Willett20, Reference Rimm, Giovannucci and Stampfer25). The DASH OLQ was designed to assess both short-term and longer-term changes in food intake by tracking food intake for multiple 24 h periods and averaging them. We theorize that those averages can be compared over time to determine dietary intake change, in addition to capturing short-term improvements to dietary intake, and view this topic as a potential for future research. The DASH OLQ can be administered more frequently than a longer questionnaire because it is less time-consuming to complete. Thus, the DASH OLQ has the potential to be used in a large population repeatedly with relatively low cost for administration and analysis.
We found that repeated use (four days in this case) of the DASH OLQ correlates well with the Block FFQ and is therefore a useful estimate of food intake in those who are attempting to follow the DASH diet. The energy-adjusted and deattenuated correlations for nutrients in our study ranged from 0·31 (Zn) to 0·74 (Mg). On average the correlation for these nutrients was approximately 0·60. Our results are comparable to those reported by similar studies that used the Block 98.2 FFQ(Reference Kumanyika, Mauger and Mitchell26, Reference Boucher, Cotterchio and Kreiger27). The DASH OLQ correlated best with the Block FFQ for breakfast cereals, drinks, fruit, nuts/seeds/legumes, meat/fish/poultry, grains, dairy and sweets, and less well for fats/oils, vegetables and mixed dishes. Owing to day-to-day variation in specific food group intakes, there are inherent limitations in the comparison of four days of intake to the ‘usual’ assessment by the FFQ, which has respondents estimate their intake over the previous year. Therefore, it is likely that correlations may improve with tracking of more days. Deattenuated correlations, controlling for day-to-day variation, support this notion. It is interesting to note that adjusting for energy did not improve correlations, but rather weakened most. This observation is not unique to this validation study, however(Reference Block, Wakimoto and Jensen28). Our belief is that because both the Block FFQ and the DASH OLQ included pre-existing portion sizes in the questionnaires, adjustment for energy intake had less of an effect.
An additional limitation to the current study is the use of a highly educated sample population, and thus the study lacks generalizability to populations of lower socio-economic status with limited access to the Internet. Further research is warranted to address whether or not a self-administered online questionnaire such as the DASH OLQ is effective and understandable to users with a variety of different backgrounds and educational levels.
The DASH (Dietary Approaches to Stop Hypertension) diet has been clinically shown to lower blood pressure, cholesterol and homocysteine concentrations, and may reduce the risk of heart disease, stroke and osteoporosis, and increase antioxidant concentrations in the body, and improve mood and quality of life(Reference Appel, Moore and Obarzanek5, Reference Elmer, Obarzanek and Vollmer8, Reference Lopes, Martin and Nashar10, Reference Lin, Ginty and Appel12, Reference Elmer, Obarzanek and Vollmer29). The DASH diet is low in saturated fat, total fat and cholesterol, has a moderate protein intake, and contains more Ca, K, Mg and fibre than does the average American diet. The results of the DASH trials have proved that such a diet would be beneficial not only for people with high blood pressure, those with pre-hypertension or a family history of high blood pressure, but also for those interested in reducing their risk of heart disease, stroke, osteoporosis and cancer risk, losing weight, and for those with an interest in feeling better, both mentally and physically(Reference Moore, Alsabeeh and Apovian4, Reference Folsom, Parker and Harnack7, Reference Elmer, Obarzanek and Vollmer8, Reference Obarzanek, Sacks and Vollmer9, Reference Fung, Chiuve and McCullough11, Reference Lin, Ginty and Appel12). Because of all of these factors the DASH diet is an ideal eating pattern to recommend to the entire American population. Until recently, information about the DASH diet was available only in written form. Our team has created an online programme based on the DASH diet that could be offered to the entire population, and uses the DASH OLQ as a method of assessing adherence to the DASH diet as a result of this online programme; however, the DASH OLQ can also be used outside the DASH for Health online programme. For the purposes of the present validation the DASH OLQ was administered independent of the DASH for Health online programme. While this tool can be used outside the DASH for Health programme, it is not currently. The DASH diet is now recommended by the USDA along with the Food Guide Pyramid as a healthy way for all Americans to eat. Making this tool more widely available would provide an important evaluation tool both to the public and to researchers.
In summary, our DASH OLQ correlated well with the established Block 98.2 FFQ across all micronutrients and DASH food groups. The Internet offers an important medium for offering an online dietary modification programme such as the DASHforHealth.com online programme and the DASH diet is an eating pattern that would benefit the majority of Americans. In the present study we have shown that the DASH OLQ is an important assessment tool for measuring adherence to the DASH diet.
Summary
The DASH OLQ was created to capture absolute intake of DASH servings of foods after exposure to a web-based nutrition and physical activity programme based on the DASH diet. For an Internet-based nutrition and physical activity programme to reliably receive feedback from those who use the site, a recall-based questionnaire must be accurate yet easy to use and relatively short compared with the typical FFQ, which can take 20–45 min to complete. In the present study, the validity of the DASH OLQ was evaluated by comparison with the Block FFQ. The average of four DASH OLQ was found to correlate well with the Block 98.2 FFQ and can be utilized as a quick measure to capture adherence to the DASH diet. This DASH OLQ may also be useful as a learning tool in employee or school settings, as well as for assessing adherence to the DASH diet in clinical practice and future research.
Acknowledgements
Sources of funding: The development of the online DASH dietary questionnaire was supported by a grant form the National Heart, Lung, and Blood Institute (3 01 HL57156-04S2). Conflict of interest declaration: T.J.M. is Chairman of e-Havior Change, LLC which owns the copyright to the DASH for Health programme. C.M.A., M.C.M., D.C.-D., M.J., K.M.G., P.-H.L. and G.C. have received some salary support from e-Havior Change, LLC. Authors’ contributions: C.M.A., M.C.M., D.C.-D., P.-H.L. and T.J.M. collaborated on the development and testing of the DASH OLQ, with collaboration on design from K.L.T. M.C.M. collected the data analysed for the purposes of this manuscript. G.C. and P.B. performed the analysis of the data for this manuscript with oversight by K.L.T. C.M.A., M.C.M., D.C.-D., K.M.G., M.J. and T.J.M. collaborated on writing and editing of this manuscript, with consultation from K.L.T.





