


It has been established that both medical and psychiatric out-patients have a high prevalence of hypochondriasis and its related new diagnosis, health anxiety. Reference Tyrer, Ferguson, Fowler-Dixon and Kelemen1,Reference Tyrer, Cooper, Crawford, Dupont, Green and Murphy2 Patients attending out-patient clinics also have a high prevalence of personality disorder, usually between 25 and 35%, and in some cases these personality characteristics could in themselves be regarded as hypochondriacal. Reference Tyrer, Ferguson, Fowler-Dixon and Kelemen1 In addition, there is robust evidence that the presence of personality disorder impairs response to treatment and worsens outcome in depression Reference Newton-Howes, Tyrer and Johnson3,Reference Newton-Howes, Tyrer, Johnson, Mulder, Kool and Dekker4 and to a lesser extent in anxiety and obsessive–compulsive disorders. Reference Tyrer, Seivewright and Johnson5–Reference Thiel, Hertenstein, Nissen, Herbst, Külz and Voderholzer8 Personality disorder has also been found to be a predictor of higher costs in the long term among people with depression. Reference Knerer, Byford, Johnson, Seivewright and Tyrer9 To date, there are no published studies examining the effect of personality disorder on the outcome of health anxiety or on the response to treatment. In the presence of personality disorder, the benefits of cognitive–behavioural therapy (CBT) for anxiety and depression may not be as marked as those from antidepressant drug treatment. Reference Tyrer, Seivewright, Ferguson, Murphy and Johnson10,Reference Fournier, DeRubeis, Shelton, Gallop, Amsterdam and Hollon11 Hypochondriacal personality features may also impair the outcome of common mental disorders in the long term. Reference Tyrer, Seivewright and Seivewright12 The status of health anxiety in current psychiatric classifications has also been a subject of debate, particularly as the diagnosis of hypochondriasis has been removed from DSM-5, Reference Starcevic13–Reference Tyrer and Tyrer15 and partly replaced by ‘illness anxiety’. 16 In ICD-11 health anxiety may or may not be a formal diagnosis in its own right, and the diagnosis of hypochondriasis (together with illness anxiety) could still be retained. Because of this uncertainty we used a two-stage process of recruitment to a planned randomised study of psychological treatment to ensure that we recruited those who not only had hypochondriasis but also significant associated anxiety, so that those who were primarily depressed and hypochondriacal were not included. At the time the trial began there was only limited evidence of the efficacy of psychological treatments for this condition. Reference Clark, Salkovskis, Hackman, Wells, Fennell and Ludgate17 In addition, because of the strong associations between personality disorder and anxiety, confirmed recently in another study, Reference Fallon, Harper, Landa, Pavlicova, Schneier and Carson18 the assessment of personality status was included in the planned protocol. This was a randomised controlled trial (RCT) of the cost-effectiveness of a modified form of cognitive–behavioural therapy for health anxiety (CBT-HA). Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 Two hypotheses related to personality were given in the published protocol. Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 First, that CBT-HA would be less effective in patients who had additional personality disorder and second that such comorbid personality disorder would be associated with increased costs over a period of 2 years.
Method
Study design
The Cognitive behaviour therapy for Health Anxiety in Medical Patients (CHAMP) trial was a pragmatic RCT (ISRCTN14565822); full details of the trial are given elsewhere. Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 In brief, the study recruited patients attending medical out-patient clinics and randomised them to either 5–10 sessions of CBT-HA (from initially naive but subsequently trained therapists) or to standard care in primary and secondary care clinics. Patients attending cardiology, endocrine, gastroenterology, neurology and respiratory medicine clinics were included from six hospitals in London, Middlesex and North Nottinghamshire. The recruitment process was as follows: patients, with their consent, who were attending clinics completed the short form of the Health Anxiety Inventory (HAI), Reference Salkovskis, Rimes, Warwick and Clark20 a self-rated scale of 14 questions with a score range of 0–42. Those that scored 20 or more on the scale (a point that has previously been shown to discriminate between those who have persistent worries over health and those who show normal variation Reference Salkovskis, Rimes, Warwick and Clark20,Reference Seivewright21 ) were invited to take part in the trial and an information sheet about the study was given. In addition, the initial assessment involved asking key questions from the Structured Clinical Interview for DSM-IV Reference First, Spitzer, Gibbon and Williams22 covering the formal diagnosis of hypochondriasis. The inclusion criteria were patients aged between 16 and 75 years, living in the area covered by the hospital, with sufficient understanding of English to read and complete study questionnaires and interviews, and who had given written consent for interviews, audiotaping of 50% of treatment sessions, and for access to their medical records. Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 All those who satisfied the inclusion criteria and hypochondriasis diagnosis were then offered randomisation to the trial, and, if they agreed, full baseline assessments were completed and written informed consent obtained. This ensured a population who had anxious hypochondriasis primarily. Follow-up data were collected at 3, 6, 12 and 24 months. The study was approved by the North Nottingham Ethics Committee (08/H0403/56) before the start of data collection.
Assessments
The primary outcome measure was the HAI score change from baseline after 1 year. Reference Salkovskis, Rimes, Warwick and Clark20 Other measures included generalised anxiety and depression using the Hospital Anxiety and Depression Scale (HADS-A and HADS-D), Reference Zigmond and Snaith23 health-related quality of life using the short Euroqol measure (EQ-5D), Reference EuroQol24 and social functioning using the Social Functioning Questionnaire (SFQ). Reference Tyrer, Nur, Crawford, Karlsen, McLean and Rao25 All measures were recorded at baseline, 6, 12 and 24 months (with the exception of the HAI which was also recorded at 3 months). Assessments were made completely independently by research assistants. Service-use data for the economic evaluation were collected at baseline, 6-, 12- and 24-month follow-up using the Adult Service Use Schedule (AD-SUS), a self-report instrument assessed in interview and designed on the basis of previous economic evaluations in adult mental health populations. Reference Barrett, Byford, Crawford, Patton, Drummond and Henry26
Personality assessment was carried out using the quick version of the Personality Assessment Schedule (PAS-Q), Reference Tyrer and Tyrer27 which records both the severity and the type of personality disorder using a four-point scale (see online supplement DS1). This contains a series of screening questions for each area of personality dysfunction, and those that score positive are asked further questions. The PAS-Q was administered by a trained research assistant, and the assessment forms include both numerical ratings and written comments on each of the sections. During the course of the study the Working Group for the Reclassification of Personality Disorder in ICD-11 completed its initial work on a new system of classification based on severity criteria (April 2010). Reference Tyrer, Crawford, Mulder, Blashfield, Farnam and Fossati28 The ICD-11 classification at that stage is summarised (Appendix). Subsequently, R.S., P.T. and G.L. reclassified the personality status of the patients in the study to convert them to ICD-11 severity equivalents by examining the PAS-Q data and written comments Reference Tyrer, Coombs, Ibrahimi, Mathilakath, Bajaj and Ranger29 as well as interviewing assessors if the data were not clear. For 30 of the assessments R.S. and P.T. completed independent assessments and achieved a good level of agreement (kappa (κ) = 0.84, 95% CI 0.60–1.0). The ICD-11 classification will be published in 2017.
Randomisation and masking
Randomisation to the two treatment groups was carried out by an independently operated computerised system (Open-CDMS), with a computer-generated random sequence using block randomisation with varying block sizes of four and six. The allocation sequence was not available to any member of the research team until databases had been completed and locked.
Statistical analysis
The calculation of the sample size for the main study has been described previously; Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 it was powered to assess the superiority of CBT-HA over standard care after 1 year, with the HAI score as the main outcome measure. The current study was a secondary analysis of the outcomes for different levels of severity of personality disturbance and so no formal sample size calculation was performed. The primary end-point (HAI) was analysed using a mixed model with time, treatment group and time × treatment interaction as fixed effects, baseline measurement as covariate and patient as random effect by personality severity group in order to test for the first hypothesis, that the CBT-HA would be less effective in participants with a personality disorder. The treatment differences between the four ICD-11 personality groups were calculated at each time point (3 months for HAI only), 6 months, 1 year and 2 years). Other secondary end-points were analysed in the same way. All analyses were based on the intention-to-treat principle. At baseline, continuous data were expressed as means and standard deviations and compared using analysis of variance (ANOVA). Categorical data were summarised using number (%) and compared using chi-squared tests.
Economic analysis
The planned economic evaluation is described in detail elsewhere. Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 Total costs were calculated by combining the service-use data collected from the AD-SUS together with hospital use from electronic records with nationally applicable unit costs. Reference Curtis30–32 Costs were calculated and analysed in UK pound sterling for the financial year 2008–2009 and were discounted in the second year at a rate of 3.5% as recommended by the National Institute for Health and Care Excellence. 33 Complete case analysis was used for the economic evaluation. Reference Tyrer, Cooper, Tyrer, Salkovskis, Crawford and Green19 The second hypothesis, that participants with personality disorder would have increased costs was explored through the examination of differences in costs over the 24-month follow-up period between ICD-11 groups. Analysis was performed using ordinary-least-squares regression as is appropriate for cost data, with the robustness of the tests confirmed using bias-corrected, non-parametric bootstrapping. Reference Barber and Thompson34,Reference Efron and Tibshirani35 Differences in all analyses were adjusted for baseline costs and randomised group. We tested for differences between complete cases and missing cases using key baseline characteristics and found no significant difference between groups – only the complete cases appear in the analysis.
Results
In total, 445 patients were randomised in the study but one patient was referred and randomised twice – both times to the standard care group – and the first date was taken for inclusion. All 444 patients had their personality status assessed at baseline (Appendix). Nine patients died during the study, six in the standard care group, three in the CBT-HA group. Of the patients who died one had no personality dysfunction, four had personality difficulty, one had mild personality disorder and three had moderate personality disorder.
Using the ICD-11 classification only 63 (14.2%) had no personality dysfunction but 197 (44.3%) had personality difficulty (a subthreshold condition not qualifying for disorder). Only three people assessed had severe personality disorder and so they were included with the moderate group as their numbers were too low for analysis. No differences in patient characteristics at baseline were identified and there was an even spread of men and women and a similar age profile between the ICD-11 personality groups (Table 1). However, there were significant differences in symptoms of health anxiety and generalised anxiety, depression and social functioning at baseline; participants with moderate to severe personality disorder had significantly higher scores than those with no personality disturbance (Table 1). There were no differences in total cost at baseline.
Table 1 Patient characteristics, clinical ratings and cost at baseline by ICD-11 personality level a
| Personality level | |||||
|---|---|---|---|---|---|
| 0 (n = 63) |
1 (n = 197) |
2 (n = 142) |
3–4 (n = 42) |
Statistics
b
P |
|
| Gender, n (%) | |||||
| Female | 29 (46.0) | 109 (55.3) | 76 (53.5) | 22 (52.4) | 0.642 |
| Male | 34 (54.0) | 88 (44.7) | 66 (46.5) | 20 (47.6) | |
| Age, years | |||||
| Mean (s.d.) | 48.6 (14.8) | 49.5 (13.6) | 47.5 (13.6) | 47.9 (11.3) | 0.592 |
| Minimum–Maximum | 18.3–73.9 | 17.3–74.3 | 17.0–75.5 | 21.7–72.4 | |
| Health Anxiety Inventory, mean (s.d.) | 24.0 (3.2) | 24.8 (4.5) | 25.2 (4.3) | 26.9 (4.9) | 0.006 |
| Hospital Anxiety and Depression Scale, Anxiety: mean (s.d.) | 10.1 (3.6) | 12.1 (3.7) | 13.4 (3.6) | 14.0 (3.6) | <0.001 |
| Hospital Anxiety and Depression Scale, Depression: mean (s.d.) | 6.7 (3.7) | 8.2 (4.1) | 10.0 (4.4) | 12.4 (4.7) | <0.001 |
| Social Functioning Questionnaire, mean (s.d.) | 5.9 (3.4) | 8.6 (4.0) | 11.3 (4.4) | 12.7 (3.8) | <0.001 |
| Total cost (preceding 6 months), mean (s.d.) | 2405.2 (2526.3) | 2601.8 (2837.2) | 2668.1 (2887.1) | 2692.5 (2708.3) | 0.954 |
a. Where 0, no personality dysfunction; 1, personality difficuity; 2, mild personality disorder; 3, moderate personality disorder; and 4, severe personality disorder.
b. χ2 for gender differences, ANOVA for others.
The outcome data over follow-up by ICD-11 classification are detailed in Table 2 and in Fig. 1. Contrary to our hypotheses the results show that those with no personality dysfunction showed no benefit from CBT-HA compared with standard care at any time point in the study; overall, standard care was superior for the symptoms of anxiety and depression (P<0.01) and for social functioning (P<0.05) but not for health anxiety. For all other groups the picture was different. For participants with personality difficulty and mild personality disorder, there was evidence of much stronger reduction in health anxiety in the CBT-HA group at all time points compared with standard care (P<0.001). For participants with moderate and severe personality disorder the initial benefit was not retained at 2 years resulting in a less strong relationship over follow-up (P<0.05). Clinical symptomatology increased and social dysfunction was greater with each increment of personality pathology (Table 1). The differences in scores between treatment groups were most marked for health anxiety; similar, but lower, differences were found for generalised anxiety and depressive symptoms (Table 2).
Table 2 Summary changes from baseline in the cognitive–behavioural therapy for health anxiety (CBT-HA) group compared with standard care in ICD-11 personality groups a

| ICD-11 personality level, difference (95% CI) | ||||
|---|---|---|---|---|
| 0 (n = 63) | 1 (n = 197) | 2 (n = 142) | 3 and 4 (n = 42) | |
| Health Anxiety Inventory scores | ||||
| 3 month | 2.12 (−1.41 to 5.64) | −1.62 (−3.56 to 0.31) | −3.24** (−5.57 to −0.92) | −3.76 (−8.24 to 0.71) |
| 6 month | −1.29 (−4.9 to 2.31) | −4.80*** (−6.77 to −2.84) | −5.51*** (−7.85 to −3.16) | −8.13** (−12.59 to −3.66) |
| 12 month | 0.47 (−3.11 to 4.05) | −3.55** (−5.54 to −1.57) | −3.32** (−5.69 to −0.96) | −4.42 (−8.99 to 0.14) |
| 24 month | 1.45 (−2.12 to 5.03) | −2.98** (−4.98 to −0.97) | −2.96* (−5.35 to −0.56) | −0.31 (−4.93 to 4.31) |
| At all time points | 0.69 (−2.23 to 3.6) | −3.24*** (−4.84 to −1.64) | −3.76*** (−5.78 to −1.74) | −4.16* (−7.99 to −0.33) |
| Hospital Anxiety and Depression Scale, anxiety scores |
||||
| 6 month | 1.45 (−0.5 to 3.39) | −1.47* (−2.64 to −0.29) | −1.71* (−3.05 to −0.36) | −2.03 (−4.7 to 0.65) |
| 12 month | 2.68 (0.75 to 4.62) | −1.70** (−2.89 to −0.51) | −1.42*s (−2.78 to −0.06) | −1.32 (−4.05 to 1.41) |
| 24 month | 2.21* (0.25 to 4.16) | −1.81** (−3.01 to −0.60) | −1.00 (−2.38 to 0.38) | −1.00 (−3.77 to 1.77) |
| At all time points | 2.11** (0.51 to 3.71) | −1.66*** (−2.62 to −0.70) | −1.38* (−2.56 to −0.20) | −1.45 (−3.79 to 0.89) |
| Hospital Anxiety and Depression Scale, depression scores |
||||
| 6 month | 2.17* (0.11 to 4.24) | −1.33* (−2.49 to −0.17) | −1.1 (−2.49 to 0.28) | −1.42 (−4.32 to 1.48) |
| 12 month | 1.79 (−0.27 to 3.85) | −1.27* (−2.45 to −0.09) | −0.69 (−2.10 to 0.71) | −2.64 (−5.62 to 0.33) |
| 24 month | 3.29** (1.22 to 5.36) | −0.69 (−1.88 to 0.49) | −1.84* (−3.27 to −0.41) | −2.06 (−5.08 to 0.96) |
| At all time points | 2.42** (0.62 to 4.21) | −1.10* (−2.06 to −0.13) | −1.21* (−2.41 to −0.02) | −2.04 (−4.55 to 0.47) |
| Social Functioning Questionnaire scores |
||||
| 6 month | 2.32* (0.19 to 4.45) | −0.42 (−1.57 to 0.73) | −0.31 (−1.68 to 1.06) | −1.89 (−4.54 to 0.77) |
| 12 month | 1.52 (−0.61 to 3.64) | −0.08 (−1.25 to 1.09) | −0.66 (−2.05 to 0.73) | −1.91 (−4.64 to 0.82) |
| 24 month | 2.88** ( 0.75 to 5.01) | −0.19 (−1.37 to 0.98) | −1.49* (−2.9 to −0.08) | −0.88 (−3.65 to 1.89) |
| At all time points | 2.24* (0.41 to 4.07) | −0.23 (−1.19 to 0.73) | −0.82 (−1.97 to 0.33) | −1.56 (−3.83 to 0.71) |
a. All minus scores indicate greater improvement in CBT-HA group except for social functioning (SFQ)). All analyses used a mixed-model approach with time, treatment group and time × treatment interaction as fixed effects, baseline measurement as covariate, and patient as random effect by personality severity group. ICD-11 personality level : 0, no personality dysfunction; 1, personality difficulty; 2, mild personality disorder; 3, moderate personality disorder; and 4, severe personality disorder. Full details of all scores are shown in online Table DS2–4.
* P<0.05,
** P<0.01,
*** P<0.001.
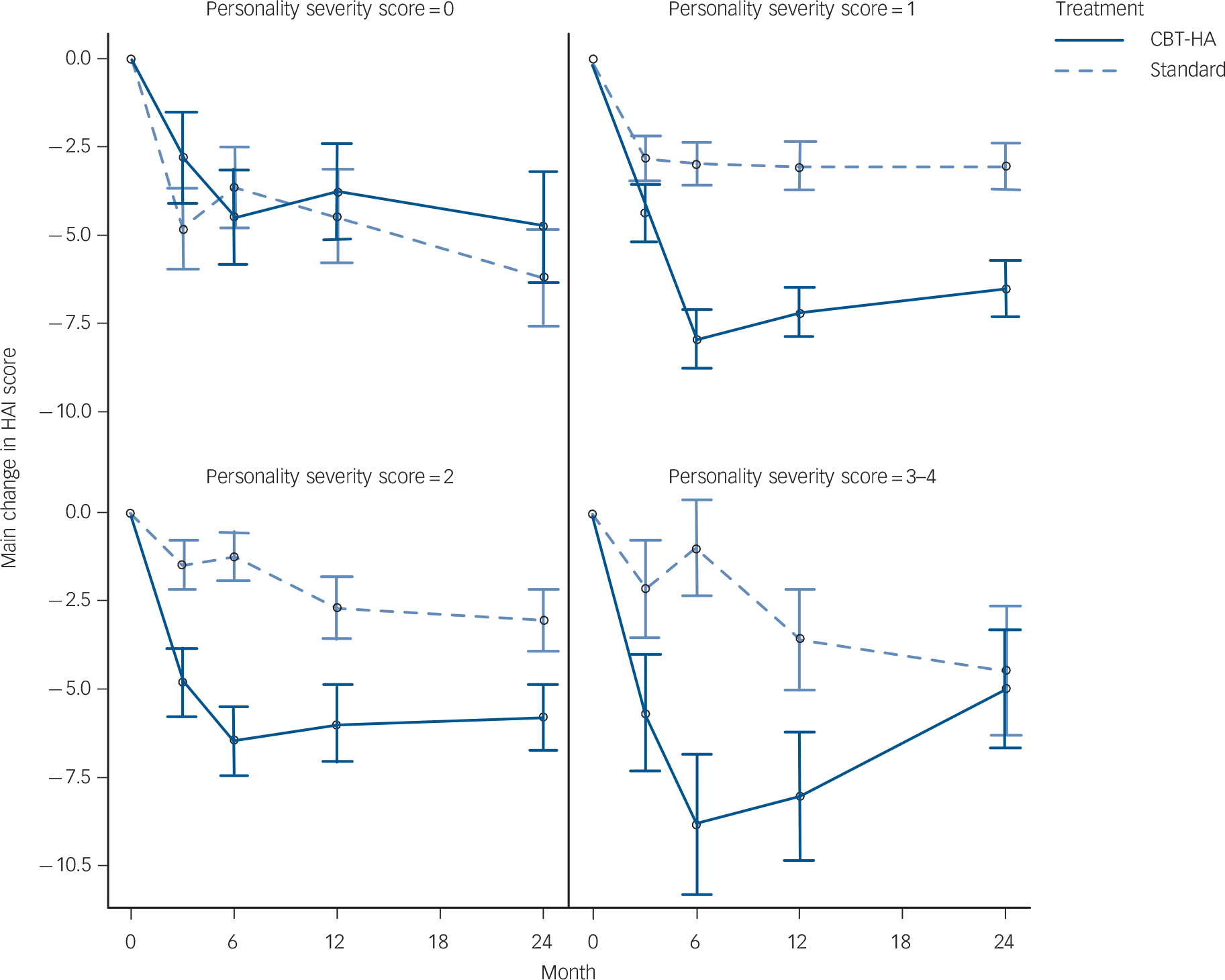
Fig. 1 Mean change in scores on the short form of the Health Anxiety Inventory (HAI) separated by personality status.
Personality severity scores: 0, no personality dysfunction (n = 63); 1, personality difficulty (n = 197); 2, mild personality disorder (n = 142); 3–4, moderate and severe personality disorder (n = 42).
Total costs over 24-month follow-up by randomised group and personality score are detailed in Table 3. Costs were broadly similar across groups, although highest in those with personality dysfunction and lowest in those with moderate to severe personality disorder. Regression analysis showed that the differences in cost between groups fell well short of significance.
Table 3 Total costs over 24-month follow-up by randomised group and personality level

| ICD-11 personality score | CBT-HA, mean (s.d.) |
Treatment as usual, mean (s.d.) |
Total, mean (s.d.) | Adjusted mean difference (95% CI) |
P |
|---|---|---|---|---|---|
| No personality disorder, 0 (n = 44) | 6386.5 (5858.1) | 7853.0 (10422.2) | 7153.05 (8490.27) | −1232.8 (−6215.66 to 3749.89) | 0.620 |
| Personality difficulty, 1 (n = 134) | 7215.8 (8140.8) | 8155.8 (9075.8) | 7657.76 (8573.20) | −380.1 (−3167.13 to 2406.93) | 0.788 |
| Mild personality disorder, 2 (n = 86) | 6792.7 (5739.6) | 7667.0 (10012.3) | 7657.77 (8573.20) | 471.8 (−2377.20 to 3300.87) | 0.747 |
| Moderate and severe personality disorder, 3+4 (n = 23) |
6610.2 (3392.4) | 5391.8 (3545.6) | 6080.48 (3435.36) | 1262.4 (−1869.75 to 4394.54) | 0.410 |
CBT-HA, cognitive–behavioural therapy for health anxiety.
Discussion
Surprising nature of findings
The challenging finding of this study was that both the hypotheses concerning personality status were soundly contradicted. These results should be seen in the context of the main primary aim of the trial; in the analysis of outcomes independently of personality status CBT-HA was markedly superior to standard care with respect to clinical symptoms of anxiety (and to some extent depression) but no marked changes were found in social function. Reference Tyrer, Cooper, Salkovskis, Tyrer, Crawford and Byford36 People with no personality dysfunction did not benefit from CBT-HA and as their social functioning deteriorated with CBT this treatment cannot be regarded as effective in this population. By contrast those with any form of personality abnormality (personality difficulty, mild or moderate personality disorder) did benefit from CBT-HA and their improvement was maintained over 2 years except in those with moderate or severe personality disorder. Such a finding has not been reported before and as it contradicted our main hypothesis (with the possible exception of worse outcome in more severe personality disorder) other explanations need to be considered before it can be accepted as valid.
In the report from the original trial Reference Tyrer, Cooper, Salkovskis, Tyrer, Crawford and Byford36 the costs were equivalent in both treatment groups and no clear saving was made with CBT-HA. A large part of the costs was taken up with the care of patients with severe medical illness and this may have disguised any savings made by CBT-HA. Nonetheless, the costs were less, but not significantly so, in all groups receiving CBT-HA compared with standard care, with the exception of those with moderate and severe personality disorder who cost more in the CBT-HA group (mean £1166) (Table 3). This suggests the possibility that for those who have moderate or severe personality disorder there is a greater cost with CBT-HA, for reasons that are not completely clear but seem to be independent of medical status, and, as suggested in a previous paper, Reference Barrett, Tyrer, Tyrer, Cooper, Crawford and Byford37 may be related to poorer social function.
A qualifying comment is necessary here, as in the trial a large proportion of those screened did not agree to take part in the trial. Reference Tyrer, Cooper, Salkovskis, Tyrer, Crawford and Byford36 It could be argued that the 444 patients seen were not therefore representative of the total population.
ICD-11 classification of personality disorder
It is worth emphasising that this is the first study to report on the effect of personality status using the new ICD-11 coding and so there are no other studies with which this one can be compared. The small number of patients with no personality dysfunction (n = 63) may appear surprising but there are other data suggesting that when personality difficulty is taken into account this subsyndromal group accounts for a large proportion of the total. Reference Yang, Coid and Tyrer38–Reference Hedman, Andersson, Andersson, Ljótsson, Rück and Asmundson41 Patients with health anxiety commonly have symptoms for many years before they present for treatment Reference Hedman, Andersson, Andersson, Ljótsson, Rück and Asmundson41 and people with chronic anxiety conditions have a high prevalence of personality disorder Reference Latas and Milovanovic42 and so the overall prevalence of personality disorder of 42% in this sample is in keeping with other figures. It is also important to stress that the diagnosis of core personality disorder is very little different in ICD-11 from ICD-10, but the great flexibility in diagnosis across the lifespan tends to increase prevalence. Reference Tyrer, Crawford, Sanatinia, Tyrer, Cooper and Muller-Pollard40 Only one other study has examined the effect of personality status on the outcome of health anxiety and hypochondriasis and this is not directly comparable with our data. This was a follow-up of an RCT of paroxetine, placebo, CBT and those who dropped out. In total, 60% were followed up successfully and those who had less harm avoidance and were more cooperative had a better outcome. Reference Greeven, van Balkom and Spinhoven43 No analysis by treatment group was made.
It also could be argued in our study that a proportion of the population may have been misdiagnosed with health anxiety and this could be explained by the cut-off of 20 points on the HAI as being too low. This score equates to around 62 on the long version of the HAI, and a score of 67 on the long HAI has been found to be a good cut-off point for discriminating between severe and less severe health anxiety. Reference Hedman, Lekander, Ljótsson, Lindefors, Rück and Andersson44 But as all patients satisfied the criteria for hypochondriasis it is unlikely the level of health anxiety was too low. The requirement for high scores on health anxiety and the diagnosis of hypochondriasis would only exclude patients with a primary depression component to their symptoms. Third, it could be argued that the patients with no personality dysfunction had appropriate health anxiety because of incipient and concurrent significant medical illness but this view is not supported by the figures as the costs were lower in those with no personality dysfunction compared with those with personality difficulty and personality disorder, although none of these differences was statistically significant.
It is also fair to add that the ICD-11 classification of personality disorder is not yet approved by the World Health Organization and more is currently being done to confirm the cut-off points for the levels of personality disturbance. Reference Tyrer, Reed and Crawford45 The fundamental structure of the reclassification is nonetheless very likely to be approved. The version of the ICD-11 classification used in the study Reference Tyrer, Crawford, Mulder, Blashfield, Farnam and Fossati28 shows some slight differences to the current version, but not to any substantive degree. It is also worth pointing out that if the analysis of this study had been carried out using the old ICD-10 diagnostic system of ‘personality disorder’ v. ‘no personality disorder’, it is unlikely that these important differences would have been found, as the markedly positive value of CBT-HA in mild personality disorder and personality difficulty would have been split between the groups.
There are also other suggestions that personality status may improve during the course of psychological treatment for health anxiety, and although one needs to be aware of the well-established evidence that standard personality measures tend to improve as mood improves Reference Coppen and Metcalfe46 there are some reasons to think that the change is more substantial. Reference Hedman, Andersson, Lindefors, Gustavsson, Lekander and Rück47
Implications for treatment
Taken together, but subject to further replication studies, it is reasonable to suggest that in the absence of personality dysfunction CBT-HA is an inappropriate treatment for health anxiety. It also implies that an assessment of personality status is necessary in the evaluation of people with suspected pathological health anxiety, as those without any personality disturbance may be much more appropriately treated, as at present, with reassurance and support rather than formal psychological intervention. The findings also give some clinical credence to the notion of a subsyndromal form of personality dysfunction in the form of personality difficulty, as the differences in outcome between this group and those with no personality dysfunction were so different.
In contrast with studies in depression and anxiety, Reference Knerer, Byford, Johnson, Seivewright and Tyrer9 we found little evidence that personality disorder had an impact on service use and cost. The results in terms of costs present a mixed picture, one which reflects those of the main study. Clear conclusions regarding differences in cost are difficult to make in this group because, irrespective of health anxiety and personality status, study participants often had substantial physical health problems that result in substantial levels of service use and therefore high costs. The relative influence of personality on service-use behaviour may therefore be limited. Previously reported evidence of greater service use at all levels of services in patients with personality disorder, especially at levels of greater severity, Reference Yang, Coid and Tyrer38 is slightly at variance with our findings, which showed lower costs in more severe personality disorder, again illustrating the likely impact of comorbid medical conditions on total cost.
Clinical psychiatry has not yet embraced the importance of twin assessments of mental state and personality status when deciding on treatment but this study, and others across a wide range of conditions Reference Newton-Howes, Tyrer and Johnson3–Reference Thiel, Hertenstein, Nissen, Herbst, Külz and Voderholzer8,Reference Tyrer, Seivewright, Ferguson, Murphy and Johnson10,Reference Fournier, DeRubeis, Shelton, Gallop, Amsterdam and Hollon11,Reference Tyrer and Yang48,Reference Koelen, Luyten, Eurelings-Bontekoe, Diguer, Vermote and Lowyck49 suggest that better judgements can be made when personality status is given as much importance as mental state in clinical practice.
Funding
This research was funded by the National Coordinating Centre for Health Technology Assessment (NCCHTA) programme (project number 07/01/26) and the National Institute for Health Research: Imperial Biomedical Research Centre. The views expressed in this publication are those of the authors and do not necessarily reflect those of the HTA programme, NIHR, NHS or the Department of Health.
Acknowledgements
We particularly thank Simon Dupont, Paul Salkovkis, Steven Reid, David Murphy, Georgina Smith and John Green for facilitating this research, the North London and East Midlands hubs of the Mental Health Research Network, for adopting, promoting and aiding recruitment in the trial. We thank Aaron T. Beck for acting as adviser to the project, and Gene Paykel (chair), Deborah Rutter, Paul Bassett, and John Brazier of the Data Monitoring and Ethical Committee and Richard Mayou (chair), Amrit Sachar, Rosemary Davidson, Devaka Fernando, Roger Mulder of the Trial Steering Committee, Sharandeep Bhogal, Faye Cooper, Rachel Evered, Mary Keeling, Stephanie Kings, Kofi Kramo, Antoinette McNulty, Amy Murphy, Jessica Nagar, Lorraine O'Connell, Richard Seivewright, Carol Sherwood, Julie Sinclair, David Trevor, Gemma Walker, and Charlotte Watson in their roles as research assistants and supervisors in the study, and special thanks to Sandra O'Sullivan for her help in coordinating the local recruitment strategies.
Appendix Summary of ICD-11 classification used in coding personality status
| Diagnostic status in ICD-11 |
No personality disorder |
Subsyndromal (classified as a Z-code) but not as a personality disorder |
Personality disorder | ||
|---|---|---|---|---|---|
| Dimensional level | Level 0 | Level 1 | Level 2 | Level 3 | Level 4 |
| Description | No personality dysfunction |
Personality difficulty | Mild personality disorder | Moderate personality disorder |
Severe personality disorder |
| Main defining features |
No evidence of any personality dysfunction in any setting |
Some problems of personality functioning with distress confined to specific settings only |
Clear evidence of general personality dysfunction but social and occupational roles maintained |
More severe personality dysfunction with major disruption of relationships and function; some risk of harm to self and/or others |
Major personality dysfunction with inability to maintain relationships, and loss of societal roles; high risk of harm to self or others |
(for latest status of classification see Tyrer et al Reference Tyrer, Reed and Crawford45 )






eLetters
No eLetters have been published for this article.