


Obsessive–compulsive disorder (OCD) is a chronic disorder that often starts in childhood. The prevalence of OCD in childhood and adolescence has been shown to be between 0.5 and 4% in epidemiological studies. Reference Flament, Whitaker, Rapoport, Davies, Berg and Kalikow1–Reference Heyman, Fombonne, Simmons, Ford, Meltzer and Goodman3 Childhood OCD is associated with high rates of persistence, Reference Geller4 and a high risk of adult OCD. Reference Fullana, Mataix-Cols, Caspi, Harrington, Grisham and Moffitt5 Among adults with OCD 30–50% report the onset of their symptoms prior to 18 years of age. Reference March, Franklin, Nelson and Foa6 Paediatric OCD is a treatment-responsive condition, yet few longitudinal studies are available and numbers of young people followed up have been small. Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7 In addition, little is known about the long-term course and impact of paediatric OCD on subsequent adult life, and psychosocial outcomes have received little attention. Paediatric OCD appears to be associated with increased risk of other psychiatric disorders in adulthood, including other anxiety and affective disorders. Reference Wewetzer, Jans, Müller, Neudörfl, Bücherl and Remschmidt8
In view of the prevalence, morbidity and functional impairment associated with paediatric OCD, a better understanding of the natural history and the long-term psychiatric and social outcomes of the disorder is needed. This prognostic information is important for clinicians, as well as young people with OCD and their families. There is also a need to investigate the extent of unmet need within this population. Such longitudinal knowledge may assist in the development and improvement of paediatric OCD services, in particular by improving the prediction of outcome in individual cases and tailoring treatment accordingly. The aims of this study were to follow up a cohort of young people with OCD, whose clinical features and demographics had been assessed in detail at first assessment, and to determine: the prevalence of OCD and other psychiatric disorders at follow-up; levels of functional disability and quality of life at follow-up; service use since discharge from a specialist service and perceived need for further treatment; and baseline predictors for persistence of OCD and other psychiatric disorders at follow-up.
Method
Participants
All young people seen at the National and Specialist OCD Clinic for Young People at the Maudsley Hospital, London, UK, between July 1996 and June 2005 who received a diagnosis of OCD at assessment were included in the study. This clinic provides specialist assessment and treatment for young people with OCD from across the UK. The sample consisted of 276 young people. After ethical approval was obtained from the South London and Maudsley NHS Foundation Trust (LRECs no. 04/Q0705/7) and the Institute of Psychiatry (no. 117/04) research ethics committees, the families of all participants were contacted by letter, followed by a telephone call, and invited to participate. Of the 276 families, 45 (16%) were not contactable, despite using multiple tracing methods. A total of 231 were therefore eligible, contacted and invited to participate. Of these, 89 (38.5%) declined participation. The most common reason given for refusal to participate was not having time/family difficulties (n = 11, 12.5%). Sixty-four families (71.6%) gave no particular reason for declining participation. Therefore, 142 (61.5%) of the young people eligible participated in the follow-up study (Fig. 1).
Baseline data
Initial clinical assessment was carried out by experienced clinicians specialising in the diagnosis and management of OCD; ICD–10 criteria were used to make psychiatric diagnoses. 9 The Children's Yale–Brown Obsessive Compulsive Scale (CY–BOCS) Reference Goodman, Price, Rasmussen, Mazure, Delgado and Heninger10 was used to measure impact and severity of the disorder. The Strengths and Difficulties Questionnaire (SDQ) was administered as a general measure of childhood emotional and behavioural symptoms. Reference Goodman, Ford, Simmons, Gatward and Meltzer11

Fig. 1 Study participation.
Demographic and other relevant clinical data were obtained during clinical assessment and ongoing treatment in the clinic. These data were collected as part of routine clinical practice and ongoing clinical audit. The whole baseline data-set is used in this study to enable as complete a comparison as possible between those who were followed up and those who either declined or were untraceable. The data are non-disclosive and their use optimises the chances of accurate interpretation of the findings. All patient records were of a high standard.
Follow-up data
The main outcome variables were the presence of OCD and other Axis I disorders, and the severity of OCD at follow-up. Participants and their parents were asked to complete the computerised version of the Developmental and Well-Being Assessment (DAWBA) Reference Goodman, Ford, Richards, Gatward and Meltzer12 to establish the presence/absence of ICD–10 Axis I diagnoses at follow-up. The DAWBA is a well-validated interview (face-to-face or web based) for parents and young people, used across the world, that generates IDC–10 and DSM–IV 13 diagnoses algorithmically, which are then cross-validated by trained clinicians after review of the responses. The DAWBA has been used for young adults as well as adolescents. Reference Meltzer, Gatward, Corbin, Goodman and Ford14 For parents who had difficulties using the web-based DAWBA, a trained researcher facilitated completion of the assessment over the telephone. All participants that had fully completed the DAWBA (either parent or young person version or both) were included. Anonymised computer ratings were reviewed by a clinical trained rater (N.M.) to generate final ICD–10 diagnoses.
The self-report version of the CY–BOCS Reference Storch, Murphy, Adkins, Lewin, Geffken and Johns15 was administered to measure the severity of OCD at follow-up. This measures OCD severity as rated over the past week, and therefore only provides an indication of OCD severity at a particular point in time. To establish a sense of overall functioning at this long-term follow-up, three additional instruments were used.
The Patient's Global Impression (PGI), Reference Guy16 a widely used seven-point Likert scale, assessed participant's perception of illness severity at follow-up. Scores range from 1 (very much improved) to 7 (very much worse).
The Work and Social Adjustment Scale (WSAS) Reference Marks17 was used to assess impairment in five areas of life (work/school, home management, social leisure, private leisure, family and relationships) and total impairment. A total score of 20 or above on this scale reflects moderately severe or severe psychopathology/impairment. Scores between 10 and 20 have been associated with functional impairment but less severe clinical symptomatology. Reference Mundt, Marks, Shear and Greist18
An additional questionnaire was developed for the study in order to obtain information regarding treatment received for OCD since discharge from the specialist service, current education/employment, living circumstances, friendships and relationships. The questionnaire also asked about perceived need for further treatment for OCD.
Data analyses
Group comparisons used parametric (ANOVA) and nonparametric tests as appropriate, after testing for normality. Chi-squared tests were used to compare proportions across groups. Binary logistic regression models examined predictors of binary outcomes. All analyses were performed using Stata (Version 9 for Windows). All statistical tests presented are two-tailed. Statistical significance was defined as a P of less than 0.05.
Results
Attrition
Baseline characteristics of participants (n = 142) were compared with those of young people who declined to participate (n = 89) and those who were not traceable (n = 45). Young people in each of these groups were comparable on all sociodemographic and baseline variables of interest (Table 1).
Table 1 Comparison of available participants with non-participants

| Unable to trace (n = 45) | Declined (n = 80) | Agreed (n = 142) | F/χ2a | |
|---|---|---|---|---|
| Age at baseline: years, mean (s.d.) | 13.5 (2.5) | 13.6 (2.4) | 13.5 (2.6) | 0.1 |
| Boys, n (%) | 28 (62) | 51 (57) | 88 (62) | 0.56 |
| Duration obsessive–compulsive disorder: years, mean (s.d.) | 3.5 (2.9) | 3.4 (2.7) | 3.7 (2.8) | 0.42 |
| Family history of obsessive–compulsive disorder, n (%) | 6 (14) | 7 (8) | 12 (9) | 1.3 |
| Children's Yale–Brown Obsessive Compulsive Scale, mean (s.d.) | ||||
| Score on obsessions at baseline | 9.9 (4.7) | 9.4 (5.2) | 10.1 (4.8) | 0.48 |
| Score on compulsions at baseline | 10.7 (4.3) | 11.7 (4.4) | 11.4 (4.1) | 0.71 |
| Total score at baseline | 20.3 (8.0) | 21.0 (8.4) | 21.6 (8.1) | 0.37 |
Sociodemographic characteristics and length of follow-up
The mean length of follow-up was 5.1 years (s.d. = 2.7, range 1–11). Mean age at follow-up was 18.6 years (s.d. = 3.5, range 11–28). As shown in Table 1, the majority of young people who participated in the follow-up were boys (n = 88, 62%). The mean duration of OCD at first assessment in the clinic was 3.7 years (s.d. = 2.8) and the mean CY–BOCS score at baseline was 21.6 (s.d. = 8.1), indicating moderate OCD.
OCD and other psychiatric disorders at follow-up
In total, 126 (88.7%) DAWBAs were completed. Of these, 17 had been completed by young people only, 68 by parents only and 41 by both young people and their parents. The majority of participants received an Axis I ICD–10 diagnosis at follow-up (n = 88, 69.8%); 52 (41.3%) had a definite diagnosis of OCD, and 5 (4.0%) had some OCD symptoms, but did not reach threshold for a diagnosis (Table 2 and see online Table DS1 for a more detailed version). The most common diagnoses at follow-up were generalised anxiety disorder (n = 32, 25.4%), followed by a depressive disorder (n = 20, 15.9%) and a tic disorder (n = 20, 15.9%).
Table 2 Psychopathology at follow-upa

| ICD–10 diagnosis | n (%) |
|---|---|
| Any disorder | 88 (69.8) |
| Any emotional disorder | 74 (58.7) |
| Any anxiety disorder | 74 (58.7) |
| Obsessive–compulsive disorder (OCD) | 52 (41.3) |
| Any anxiety disorder other than OCD | 49 (38.9) |
| Any depressive episode | 20 (15.9) |
| Undifferentiated anxiety/depression | 1 (0.8) |
| Attention-deficit hyperactivity disorder | 4 (3.2) |
| Any conduct/oppositional disorder | 9 (7.1) |
| Any pervasive developmental disorder | 13 (10.3) |
| Any tic disorder | 20 (15.9) |
| Psychosis | – |
| Other (trichotillomania) | 1 (0.8) |
OCD severity
The CY–BOCS scores both at baseline assessment and follow-up were available for 98 participants (Fig. 2). At both time points, participants were classified as having subclinical (scores from 0 to 10), mild (scores from 11 to 19), moderate (scores from 20 to 29) or severe (scores >30) OCD symptoms. At follow-up, 33.7% of participants scored below threshold on the CY–BOCS, 34.7% in the mild category, 29.6% in the moderate category, and 2% with scores reflecting severe symptoms. Compared with baseline, the proportions of moderate and severe scores had decreased, with an increase in participants experiencing subclinical or mild symptoms (Fig. 2).
The CY–BOCS total severity scores dropped from a mean of 21.0 at baseline to 14.1 at follow-up (mean change 6.9, 95% CI 4.7–9.1, P<0.0001). Participants who met criteria for OCD at follow-up had higher scores on the CY–BOCS than those who no longer met criteria (Table 3).
Table 3 Obsessive–compulsive disorder (OCD) severity across the total sample and in outcome groups
| Relationship to outcome at follow-up | |||
|---|---|---|---|
| Total sample (n = 142) | OCD at follow-up (n = 52) | No OCD at follow-up (n = 74) | |
| CY–BOCS severity score, mean (s.d.) | 14.4 (9.0) | 21.1 (6.2)* | 10.6 (7.6) |
| PGI OCD severity rating, responders, n (%) | 127 (89.4) | 47 (90.4) | 59 (79.7) |
| Very much improved, n (%) | 43 (33.9) | 4 (8.5) | 31 (52.5) |
| Much improved, n (%) | 34 (26.8) | 11 (23.4) | 19 (32.2) |
| A little better, n (%) | 23 (18.1) | 15 (31.9) | 6 (10.2) |
| Unchanged, n (%) | 14 (11) | 8 (17) | 1 (1.7) |
| A little worse, n (%) | 5 (3.9) | 3 (6.4) | 2 (3.4) |
| Much worse, n (%) | 6 (4.7) | 5 (10.6) | 0 |
| Very much worse, n (%) | 1 (0.9) | 1 (2.1) | 0 |
| Total score, mean (s.d.) | 2.4 (1.5) | 3.2 (1.5)* | 1.7 (1.0) |
| WSAS scores, responders, n (%) | 96 (67.6) | 34 (65.4) | 51 (69.0) |
| Work/studies, mean (s.d.) | 2.6 (2.3) | 3.5 (2.2) | 1.9 (1.9) |
| Home management, mean (s.d.) | 2.2 (2.1) | 3.8 (1.9) | 1.2 (1.4) |
| Social leisure activities, mean (s.d.) | 2.4 (2.3) | 3.8 (2.5) | 1.4 (1.5) |
| Private leisure activities, mean (s.d.) | 2.2 (2.1) | 3.3 (2.0) | 1.5 (1.7) |
| Family and relationships, mean (s.d.) | 1.8 (2.1) | 2.8 (2.2) | 1.1 (1.4) |
| Total score, mean (s.d.) | 11.1 (9.2) | 17.1 (8.2)* | 7.1 (6.4) |
Subjective perception of illness severity
The PGI scores suggest that the majority of participants (60.7%) rated themselves as very much or much improved in relation to OCD symptoms. Only 8.6% of participants reported that their symptoms were a little or much worse. Participants who met criteria for OCD at follow-up had significantly higher scores on the PGI (Table 3).
Adaptive functioning
Ninety-five participants filled in the WSAS at follow-up. Single subscale scores and the total score are shown in Table 3. These scores suggest mild to moderate levels of interference in work/education, home management and social function. As expected, participants who still met criteria for OCD at follow-up had significantly higher WSAS total scores (Table 3).
Regarding functional status at follow-up, 88% were studying or working (Table 4). The majority of participants (78.3%) were living with their parents, reported having close friends (80.3%); and about a third were in a relationship. A higher number of participants without OCD at follow-up compared with those with persistent OCD had a partner and close friends, although the difference did not reach statistical significance.
Table 4 Social outcomes, service use and unmet needs across the total sample and in outcome groups

| n (%) | |||
|---|---|---|---|
| Relationship to outcome at follow-up | |||
| Total sample (n = 142) | OCD at follow-up (n = 52) | No OCD at follow-up (n = 74) | |
| Current occupation, responders | 138 (97.2) | 50 (96.1) | 66 (89.1) |
| Studying | 73 (52.9) | 21(42) | 41 (62.1) |
| Working (full time or part time) | 27 (19.5) | 12 (24) | 11 (16.6) |
| Studying and working | 5 (1.8) | 2 (4) | 3 (4.5) |
| Other | 33 (12) | 15 (30) | 11 (16.7) |
| Current accommodation, responders | 138 (97.2) | 50 (96.1) | 66 (89.1) |
| Living with parents | 108 (78.3) | 38 (76) | 53 (80) |
| Living on their own | 3 (2.2) | 1 (2) | 1 (1.5) |
| Flat sharing | 9 (6.5) | 2 (4) | 6 (9) |
| Living with parents and flat sharing | 12 (8.7) | 5 (10) | 5 (7.6) |
| Other | 6 (4.3) | 4 (8) | 1 (1.5) |
| In a sentimental relationship | 29 (21.3) | 7 (14.3) | 16 (24.6) |
| Any close friends | 110 (80.3) | 38 (76) | 58 (89.2) |
| Service utilisation for OCD since dischargea | 89 (66.4) | 37 (77.1)b | 38 (59.4) |
| Current service utilisationc | 69 (50.4) | 31 (63.3)** | 28 (42.4) |
| Any in-patient admissions | 11 (8.2) | 6 (12.5) | 4 (6.1) |
| Any pharmacological treatment | 69 (51.5) | 33 (70.2) | 26 (40) |
| Current pharmacological treatment | 57 (41.9) | 26 (53.1) | 23 (34.8) |
| Any psychological treatment | 54 (40.6) | 24 (51.1) | 21 (32.8) |
| Current psychological treatment | 33 (24.6) | 16 (33.3) | 12 (18.5) |
| Perceived need for any further treatment: yesd | 65 (49.6) | 38 (79.2)* | 17 (27) |
| Which treatment? | |||
| Psychological | 32 (50.8) | 16 (44.4) | 10 (58.8) |
| Pharmacological | 7 (11.1) | 4 (11.1) | 3 (17.6) |
| Combination | 14 (22.2) | 13 (36.1) | 1 (5.9) |
| Other | 9 (14.3) | 3 (8.3) | 2 (11.8) |
Service utilisation and unmet needs
Two-thirds (66.4%) of participants had accessed services for OCD since discharge from the specialist clinic, and 50% were currently receiving treatment. Of these, the majority (42%) were receiving pharmacological treatment, whereas only 25% were receiving psychological treatment. The percentage of participants who had accessed services since discharge and were currently receiving treatment was higher (albeit non-significantly) in those with current OCD compared with those who did not have current OCD (Table 4).
Sixty-five participants (49%) reported that they felt a need for further treatment. Of these, 32 (50%) reported a preference for further psychological treatment, 7 (11%) for medication; 14 (23%) for a combined psychological and pharmacological treatment. Significantly more participants with current OCD reported a need for further treatment (Table 4).
Predictors of disorder at follow-up
Factors known to be associated with persistence of OCD and presence of other psychiatric disorders at follow-up were investigated. Among baseline variables investigated, duration of OCD before assessment was significantly associated with a diagnosis of OCD at follow-up (odds ratio (OR) = 1.2 (95% CI 1.0–1.3). The presence of comorbid tics (Tourette syndrome or tics) at baseline was associated with lower risk for OCD persistence (OR = 0.2, 95% CI 0.1–0.6). Gender, baseline CY–BOCS score, age at assessment, and family history of OCD did not predict OCD diagnosis at follow-up. Total SDQ scores at baseline, for both parents and young people, showed a trend towards significance. In relation to other psychiatric disorders at follow-up, SDQ parent and young person total score and young person emotional score at baseline predicted a psychiatric disorder other than OCD at follow-up (respectively OR = 1.1, 95% CI 1.0–1.1; OR = 1.1, 95% CI 1.0–1.2; OR = 1.3, 95% CI 1.0–1.6) (Table 5).
Table 5 Predictors for persistence of obsessive–compulsive disorder (OCD) and other psychiatric disorders at follow-up: logistic regression, odds ratios (OR) and 95% CI

| Predictors | OCD at follow-up OR (95%CI) | P | Any ICD–10 disorder at follow-up, OR (95%CI) | P |
|---|---|---|---|---|
| Gender, male | 0.7 (0.4–1.5) | NS | 0.5 (0.2–1.3) | NS |
| Age at onset | 1.0 (0.9–1.1) | NS | 1.0 (0.9–1.2) | NS |
| Duration of OCD | 1.2 (1.0–1.3) | <0.05 | 1.0 (0.9–1.2) | NS |
| Family history of OCD | 0.5 (0.1–2.3) | NS | 0.9 (0.1–4.9) | NS |
| CY–BOCS score at baseline | 1.0 (1.0–1.1) | NS | 1.0 (1.0–1.1) | NS |
| Any tics at baseline | 0.2 (0.1–0.6) | <0.01 | 0.6 (0.3–1.4) | NS |
| Strengths and difficulties questionnaire | ||||
| Parent total score at baselinea | 1.0 (1.0–1.1) | 0.1 | 1.1 (1.0–1.1) | <0.05 |
| Parent emotional score at baselinea | 1.1 (0.9–1.3) | NS | 1.2 (1.0–1.4) | 0.08 |
| Parent conduct score at baselinea | 1.0 (0.8–1.2) | NS | 1.1 (0.9–1.4) | NS |
| Young person total score at baselineb | 1.1 (1.0–1.1) | 0.1 | 1.1 (1.0–1.2) | <0.05 |
| Young person emotional score at baselineb | 1.2 (1.0–1.5) | 0.1 | 1.3 (1.0–1.6) | <0.05 |
| Young person conduct score at baselineb | 1.0 (0.7–1.2) | NS | 1.1 (0.8–1.4) | NS |
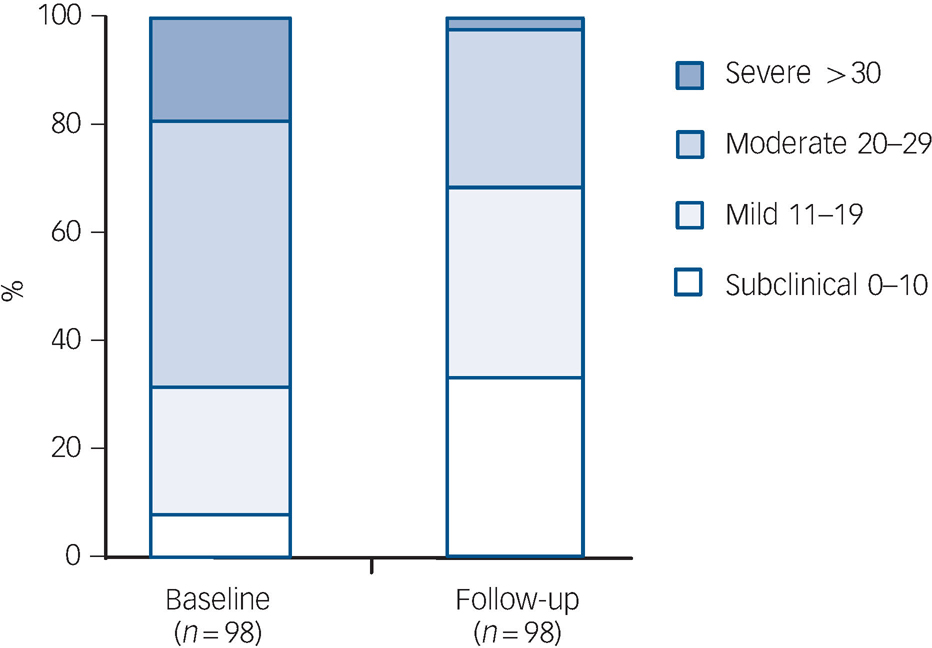
Fig. 2 Children's Yale–Brown Obsessive Compulsive Scale scores at baseline and follow-up.
Discussion
Main findings
This is the largest long-term follow-up study of children and adolescents with OCD. Our findings suggest that approximately 60% of young people with OCD, who were assessed at a specialist paediatric OCD clinic, did not have a full clinical syndrome of OCD at follow-up. Persistence rates of OCD of 41% were found, and only a third had moderate or severe OCD at follow-up. Approximately two-thirds of participants rated themselves as very much or much improved in relation to their OCD. The primary predictor for persistence of OCD at follow-up in this sample was duration of OCD. Severity of OCD at baseline did not predict persistence of disorder.
Approximately 70% of participants who had a diagnosis of OCD in childhood/adolescence received an Axis I ICD–10 diagnosis at follow-up, and the most common disorders were other anxiety disorders (38.9%). Predictors for ICD–10 disorders at follow-up were higher levels of emotional and behavioural symptoms, as measured by self-report and parent-report SDQ total scores, at baseline.
Average levels of functional impairment at follow-up, as assessed on the WSAS, were mild (with a mean of 11.1), suggesting that overall, these teenagers and young adults were functioning reasonably in work and social life. The majority of participants were either in full-time education or working. At a mean age of 18.6 at follow-up, most participants still lived with their parents. There were high rates of service utilisation during the follow-up period, with approximately 66% of participants accessing services for OCD. Indeed, half of the participants were still receiving treatment for OCD, with pharmacological treatment being the most common. Interestingly, half of the participants reported a perceived need for further OCD treatment, and the majority expressed a need for psychological treatment.
OCD, other psychiatric disorders and relevant predictors at follow-up
There have been few studies examining long-term outcomes for paediatric OCD. These have been usually small (the largest study to date followed up 132 participants Reference Cook, Wagner, March, Biederman, Landau and Wolkow19 and was a pharmacological trial), they have often relied upon in-patient samples, and only six studies have followed forward a group of children who were carefully characterised at baseline. A systematic review of long-term outcomes of paediatric OCD has found pooled persistence rates of the disorder of 41% for full OCD and 60% if subthreshold OCD Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7 is included. Persistence rates in our study are consistent with these previously reported rates. Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7,Reference Bloch, Craiglow, Landeros-Weisenberger, Dombrowski, Panza and Peterson20
Only a few studies have evaluated comorbidity at follow-up. Comorbidity assessment and rates vary greatly across studies, with total comorbidity at follow-up ranging from 55 Reference Reddy, Srinath, Prakash, Girimaji, Sheshadri and Khanna21 to 70% Reference Wewetzer, Jans, Müller, Neudörfl, Bücherl and Remschmidt8 and 96%. Reference Leonard, Swedo, Lenane, Rettew, Hamburger and Bartko22 The most common disorders were anxiety disorders (ranging between 10 and 81%) and mood disorders (ranging between 10 and 43%). Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7 The sample reported here has similarly high rates of other psychiatric morbidity at follow-up especially in relation to emotional disorders.
The review by Stewart et al Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7 identified that admission to hospital for treatment for OCD (rather than community treatment), earlier age at onset and longer duration of OCD all predicted persistence. Similar to previous studies and the meta-analysis by Stewart and collagues, Reference Stewart, Geller, Jenike, Pauls, Shaw and Mullin7 in this sample longer duration of OCD at baseline was a significant predictor of persistence of OCD at follow-up. A possible explanation for this finding is that unremitting OCD occurring during a crucial time of development (childhood or early adolescence) may disrupt specific developmental processes, similar to the developmental disruption resulting from adolescent psychosis. Reference Marshall, Lewis, Lockwood, Drake, Jones and Croudace23 In line with one report, Reference Cook, Wagner, March, Biederman, Landau and Wolkow19 absence of tics at baseline in this sample was predictive of persistent OCD. This might be associated with heterogeneity/subtypes within OCD; alternatively, it has been suggested that OCD in conjunction with tics may be a more neurodevelopmental form of the disorder, which perhaps has more spontaneous remission with development and maturation. Reference Bloch, Peterson, Scahill, Otka, Katsovich and Zhang24 We did not find any other factors that predicted the persistence of OCD. In contrast to the findings of Thomsen, Reference Thomsen25 OCD severity at baseline did not predict persistence of disorder. There was a trend for SDQ scores (both parental and young person) at baseline to predict persistence of disorder, possibly suggesting that higher levels of psychopathology at baseline affect persistence of OCD at follow-up. As expected, higher total SDQ scores at baseline and higher SDQ emotional symptom scores (as rated by young people themselves) were related to the presence of any psychiatric disorder (other than OCD) at follow-up.
Social functioning, service use and unmet needs
Both adult and childhood OCD have been associated with functional impairment and poorer quality of life. Reference Valderhaug and Ivarsson26,Reference Huppert, Simpson, Nissenson, Liebowitz and Foa27 The majority of individuals with paediatric OCD followed up for this study have relatively good social outcomes. About 70% of participants were either in full-time or part-time education/work and functional impairment across work and social life was mild to moderate across this group. This was regardless of persistence of OCD at follow-up, suggesting that many young people can adapt to their illness and lead a fairly normal life despite being symptomatic.
There have been few if any studies of service utilisation in childhood/adolescent OCD. This study suggests rates of service utilisation are high in this population group, about 50% during the follow-up period. The most frequent treatment for OCD at follow-up was medication (42%). Although there are limited data to guide clinical practice regarding duration of medication treatment for OCD, current consensus suggests that young people who have also received psychological treatments should have an attempt at medication reduction/cessation after 1 year of remaining well. 28,29 Studies in adults have suggested high rates of relapse on discontinuation of medication in those treated with medication alone, although this may be reduced if individuals also engage in behaviour therapy. Reference Hembree, Riggs, Kozak, Franklin and Foa30 In this sample of young people with OCD only 25% were receiving psychological treatment at the time of follow-up, despite many individuals indicating that they would like further psychological treatment. Moreover, about half of the participants followed up described wanting/needing more treatment for OCD; this perceived need mainly included psychological treatment or a combination of medication with psychological treatment. Combined with the above finding, this suggests that there is a considerable amount of unmet need in this group.
The evidence-base for the treatment of OCD is reasonably clear and consistent, and forms the basis of both American Psychiatric Association guidelines, and UK National Institute for Health and Clinical Excellence (NICE) guidelines. 28,29 There is consensus that psychological treatment in the form of cognitive–behavioural therapy (CBT) should be available to all individuals with OCD – this follow-up study suggests that teenagers and young adults may be finding it difficult to access these treatments. Issues regarding the long-term outcomes and needs of people with OCD are also considered in treatment guidelines. It is acknowledged that OCD can have a fluctuating or episodic course, or that relapse may occur after successful treatment. It is suggested in the UK NICE guidelines that ‘people who have been successfully treated and discharged should be seen as soon as possible if re-referred with further occurrences of OCD, rather than placed on a routine waiting list’. 29
Availability of psychological treatments is a challenge for health services, and in the UK a government-led scheme, Increasing Access to Psychological Treatments (IAPT), is active in training more therapists and opening more treatment centres. 31 This scheme is being expanded to include the needs of young people, and individuals with early-onset OCD will benefit from the increased access to CBT that this venture should provide.
Strengths and limitations
There are several strengths to this study. This is the largest follow-up to our knowledge of children and adolescents with OCD. Given the length of follow-up (a maximum of 11 years), the participation rate was very good at 61.5%. A range of data were available at baseline to allow comparison of participants and non-participants. Participants did not differ from non-participants or untraceable young people. Participants in the study varied in OCD symptom severity at baseline; therefore the sample is representative of young people attending community services. This has been a limitation in several previous studies that have focused on in-patients only.
The main limitation in this study is that diagnosis at baseline was not made using a structured instrument. However, all diagnoses were made after consensus discussion by an experienced clinical team using ICD–10 criteria, and following a detailed, structured clinical assessment with the young person and their parents. The diagnosis of OCD was made using the CY–BOCS, as well as the clinical assessment, at baseline. A second limitation is that not all participants included in this follow-up study completed all the relevant measures. However, all measures were completed by more than 70% of participants, apart from the WSAS (completed by 67% of participants). We were only able to follow-up 61.5% of all eligible participants; despite a possibility of selection bias, initial attrition analyses showed no difference in sociodemographic and illness characteristics between respondents and non-respondents. This suggests our results are generalisable.
In addition, we were not able to explore associations between initial response to treatment, the quality and quantity of that treatment, and the relationship of that to long-term outcome. These remain key questions for services, as the current assumption incorporated into treatment guidelines is that early recognition, assertive treatment with evidence-based treatments and quick and easy access to ‘top-up’ treatments if relapse occurs, will all contribute to improved long-term adaptation for people who had OCD in childhood.
Implications
A substantial amount of unmet need is evident in this patient group. However, on average, the impact of OCD on functional impairment and quality of life was mild to moderate. The findings suggest that paediatric OCD can be a chronic or relapsing/remitting disorder that has long-term treatment implications. There is evidence that duration of disorder at assessment predicts persistence, therefore suggesting a need for increased recognition at the earliest stages of the disorder.
Funding
Research and Development Fund, South London and Maudsley NHS Foundation Trust.
Acknowledgements
We thank all participants and their families for taking part in the study and Professor R. Goodman for providing advice. Thanks to Christine Tang and Hala Ali for help in carrying out the study.









eLetters
No eLetters have been published for this article.