


Seasonal affective disorder (SAD) is a subtype of bipolar or major depressive disorder characterised by typical (i.e. lowered mood, energy loss and fatigue) and atypical (i.e. weight gain, carbohydrate craving and hypersomnia) depressive symptoms and a distinct seasonal nature (Reference Rosenthal, Sack and GillinRosenthal et al, 1984). SAD appears to be relatively common in general population samples in the US (Reference Kasper, Wehr and BartkoKasper et al, 1989; Reference Rosen, Targum and TermanRosen et al, 1990). However, deriving an accurate estimate for the condition is complicated by the fact that many previous studies have used the overinclusive Seasonal Patterns Assessment Questionnaire (SPAQ) (Reference Rosenthal, Genhart, Sack, Hudson and PopelRosenthal et al, 1987) as a diagnostic instrument, rather than gold-standard structured diagnostic interviews. For example, in a study of primary care attenders in Scotland (Reference Eagles, Naji and GrayEagles et al, 1998), 9.3% of patients satisfied SPAQ screening criteria for SAD. However, studies utilising diagnostic interview protocols have shown much lower community prevalence rates of 1% in the USA (Reference Blazer, Kessler and SwartzBlazer et al, 1998) and 3.5% in Scotland (Reference Eagles, Wileman and CameronEagles et al, 1999). There remains a paucity of epidemiological data concerning the prevalence of SAD in the general population of the UK, and its detection and treatment in primary care.
METHOD
Background
The research reported here was conducted in conjunction with the Outcomes of Depression International Network (ODIN) project, designed to assess the prevalence of and risk factors for depression in urban and rural areas within the European Union, and the efficacy of two psychological interventions (‘Problem-Solving Treatment’ and the ‘Coping with Depression’ course) in ameliorating depression and in reducing service utilisation and costs (Dowrick et al, Reference Dowrick, Casey and Dalgard1998, Reference Dowrick, Vázquez-Barquero and Wilkinson1999). For the purposes of the study, ‘rurality’ was defined as a geographic area having no centre of population greater than 15 000 people, and having at least 20% of the economically active population directly or indirectly employed within agriculture.
Sample frame
The sample was made up of adults aged between 18 and 64 years registered on the North Wales Health Authority's general practice database residing within the former Glyndwr council district in North Wales.
Case finding
A two-phase sampling method was adopted as a research strategy for the ODIN project (Reference Pickles and DunnPickles & Dunn, 1995) using a self-rating postal survey to identify potential cases of depressive disorder, followed by structured diagnostic interview and more detailed questionnaires with those participants scoring above threshold.
In North Wales, the initial screening package also included a sub-scale of the SPAQ from which a ‘global seasonality score’ (GSS) for a given individual was derived. This score ranges from 0 to 24, and indicates the degree of change an individual experiences between the seasons in their sleep, mood, weight, appetite, energy and social activity, and requires that the individual describe whether these changes represent a mild, moderate, marked, severe or disabling problem for them. Beck Depression Inventory (BDI; Reference Beck, Ward and MendelsonBeck et al, 1961) scores, short measures of social support, recent life events and basic demographic questions were also incorporated into the screening package in the normal course of the ODIN project. The bulk of the package was available in both English and Welsh, and non-responders were contacted up to three times by letter and telephone to encourage participation.
The second diagnostic interview stage of assessment was conducted with all consenting participants who possessed: (a) a GSS of 11 or more with seasonal changes amounting to at least a ‘moderate’ problem; and (b) a randomly selected 5% sample. For the GSS sample, interviews were conducted during the winter of 1997-1998 by a trained research worker (E. E. M.) according to the revised version of the Structured Interview Guide for the Hamilton Depression Rating Scale — Seasonal Affective Disorder Version (SIGH—SAD; Reference Williams, Link and RosenthalWilliams et al, 1992). Diagnostic criteria utilised were a minimum score of 15 on the Hamilton Rating Scale for Depression (HRSD; Reference HamiltonHamilton, 1960), with a score of at least six on the supplementary atypical item scale. Diagnosed cases of SAD were those participants who fulfilled SPAQ, SIGH—SAD and DSM—IV (American Psychiatric Association, 1994) criteria. Additional questionnaires and data concerning participants' previous diagnoses of depression, SAD and treatment history were also obtained at the time of interview.
Weighted prevalence estimates, taking into account the two-phase sampling strategy, were obtained using the ‘svyprop’ and ‘logit’ commands of STATA as described in Dunn (Reference Dunn2000).
RESULTS
A 63% (n=1250) response rate was obtained from the 1999 people who were sent screening questionnaires. Younger people were significantly less likely to respond to the screening questionnaire than older people (t=5.7, d.f.=1440, P <0.001), the mean age of non-responders being 40 and that of responders being 43 years. Men were significantly less likely to respond than women, with a response rate of 58.6% compared with 67.4% (χ2=16.5, P <0.001).
Sixty-six respondents (5.3%) screened positive for SAD according to SPAQ criteria. Fifty-five (83%) of this sample agreed to undergo diagnostic interview and 25 were diagnosed with SAD according to the outlined criteria. The statistical package STATA-5 (StataCorp, 1997) was used to calculate a prevalence rate of 2.4% (s.e.= 0.7, 95% CI 1.4-4.3) for SAD (see Fig. 1).
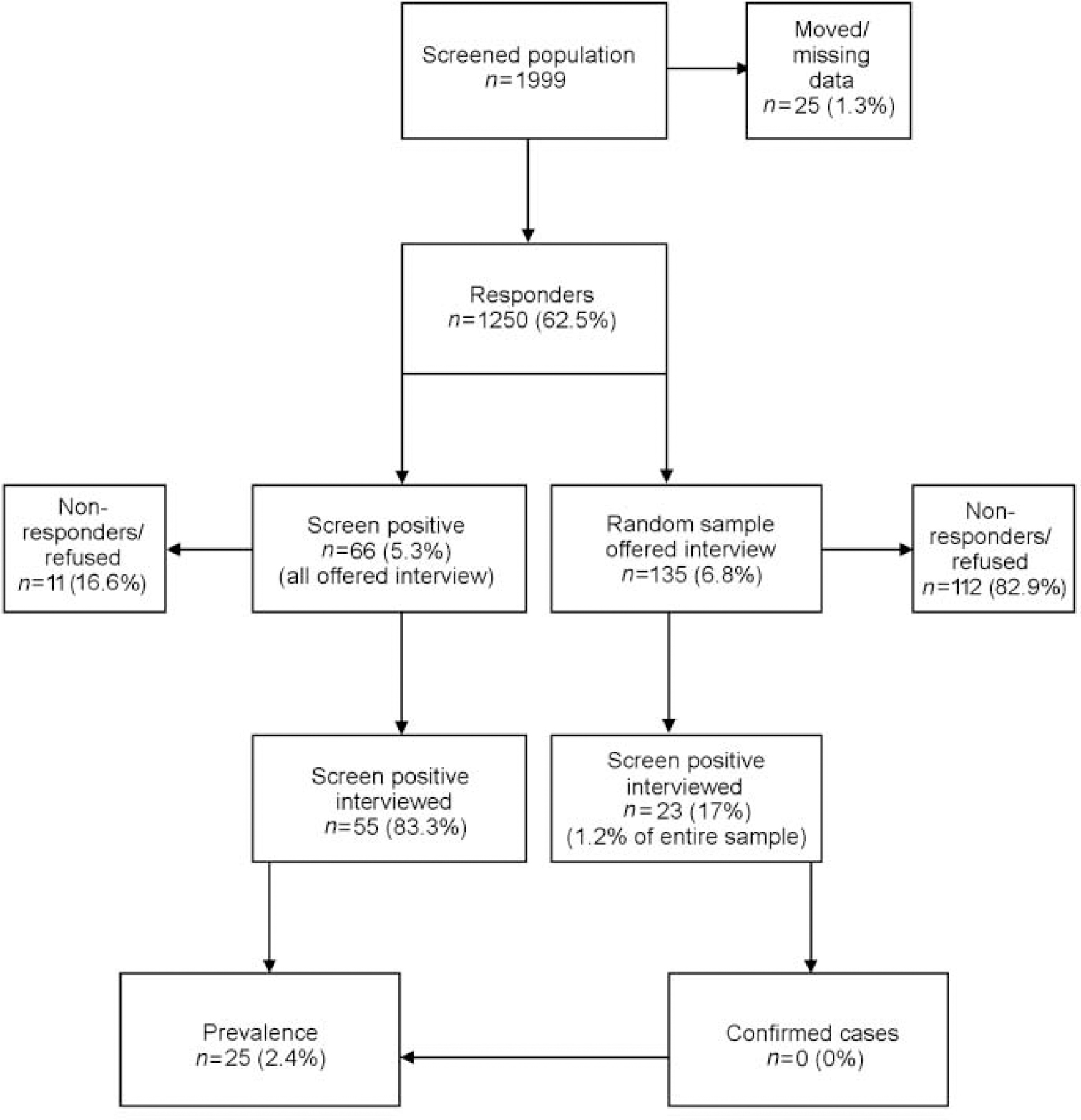
Fig. 1 Flow chart showing the prevalence of seasonal affective disorder as derived from general population sample.
Diagnosis and treatment history data showed that the majority of identified cases had not previously received a diagnosis of SAD or undergone light therapy, although they had frequently received diagnoses of other forms of depression and had taken antidepressant medication (see Table 1).
Table 1 Diagnostic and treatment history of patients with seasonal affective disorder (SAD) (n=25)
| Yes | No | Unclassified | |
|---|---|---|---|
| Previous diagnosis of SAD | 1 | 23 | 1 |
| Previous diagnosis of depression | 13 | 12 | - |
| Previous use of antidepressants | 151 | 10 | - |
| Previous use of light therapy | - | 25 | - |
DISCUSSION
Prevalence implications
The present study found that 2.4% of the general population in one area of the UK might be diagnosed with an episode of SAD under strict diagnostic criteria. This finding is concordant with those of a recent study conducted in Scotland, which found the community prevalence of SAD to be 3.5% (Reference Eagles, Wileman and CameronEagles et al, 1999).
Diagnostic implications
Although SAD does appear to occur fairly widely in the general population, general practitioners are likely to underdiagnose the disorder for a number of reasons. It is thought that general practitioners correctly identify depression in around half of the cases they are presented with (Reference Freeling, Rao and PaykelFreeling et al, 1985). Moves such as the Defeat Depression Campaign (Priest et al, 1991) have concentrated upon further improving the identification and treatment of depression in primary care. However, it may be particularly difficult for general practitioners to recognise forms of depression characterised by somatic symptoms such as weight gain, fatigue and hypersomnia, all of which typify SAD (Reference Goldberg and BridgesGoldberg & Bridges, 1988). Of the 25 patients diagnosed with SAD in the present study, only one had previously received a diagnosis of SAD from their general practitioner, although over half had received diagnoses of other forms of depression and had been prescribed antidepressants. SAD does appear to be underdiagnosed and/or misdiagnosed in this sample. It remains to be seen, however, whether the improved detection of SAD in primary care will in turn result in improved patient outcome.
Treatment implications
Seasonal affective disorder is thought to be related to seasonal variations in natural light levels, and light therapy — daily exposure of the patient to bouts of artificially produced high-intensity light — has been shown to produce amelioration of depressive symptoms (Reference Eastman, Young and FoggEastman et al, 1998; Reference Terman, Terman and RossTerman et al, 1998). Early research has also indicated that antidepressants may be successful in treating SAD (Reference Lam, Gorman and MichalonLam et al, 1995). However, with lightboxes costing in the region of £ 150 for an indefinite treatment period compared to £120 for a winter's supply of fluoxetine, light therapy remains for some clinicians a potentially less expensive and less invasive form of treatment. Furthermore, given that current treatment guidelines suggest that antidepressants be prescribed for non-seasonal depression for a minimum of 6 months, is it also feasible that patients with unrecognised SAD are currently receiving medication for longer than necessary. The cost implications of this potential overprescribing are significant. In this regard, a more targeted approach towards SAD by better-informed primary health care teams is likely to benefit the NHS as well as the patient.
Methodological considerations
The prevalence rate obtained in the present study may have been inflated in two ways. First, a higher response rate was received from women, and women are more likely than men to suffer from SAD. Second, a stage one bias towards response may have occurred in people who experience seasonal problems. Another methodological consideration concerns the decision to offer diagnostic interviews to only a 5% sample of participants. This may have led to considerably higher standard errors (and hence wider confidence intervals) than would have been the case if a larger proportion of participants had been included in the second phase of the community survey.
Furthermore, response rates were particularly poor for this group, resulting in only a 1.2% (n=23) random sample actually being interviewed. It later became evident that the research team had placed less emphasis upon achieving a high response rate in this group than in the screen-positive sample.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
• Seasonal affective disorder (SAD) was found to be common in a general population sample in rural North Wales.
-
• The condition was not well recognised at a primary care level.
-
• SAD may be receiving sub-optimal treatment in UK primary care.
LIMITATIONS
-
• Gender bias in response rates may have resulted in an inflated prevalence rate.
-
• Response bias in people experiencing seasonal symptoms may have inflated the prevalence rate.
-
• Too few participants under cut-off were offered diagnostic interviews.
Acknowledgements
We thank Professor Graham Dunn and Dr Kerry Hood for statistical support, Dave Miller from the North Wales Health Authority for provision of patient information and Victoria Higgin for secretarial support. Special thanks to the primary care teams and patients from North Wales who participated in the study.



eLetters
No eLetters have been published for this article.