


There has been a large amount of research, debate and speculation about the classification of internalising disorders including major depression, generalised anxiety disorder, phobia and panic disorders (Reference Kovacs and DevlinKovacs & Devlin, 1998; Reference Zahn-Waxler, Klimes-Dougan and SlatteryZahn-Waxler et al, 2000; Reference LilienfeldLilienfeld, 2003; Reference WatsonWatson, 2005). A central issue in these debates has concerned the extent to which internalising disorders are reflections of a common underlying disorder of internalising and the extent to which these disorders are distinct diagnostic entities (Reference Kendler, Neale and KesslerKendler et al, 1992; Reference Brown, Choi pita and BarlowBrown et al, 1998; Reference Krueger, Caspi and MoffittKrueger et al, 1998; Reference KruegerKrueger, 1999; Reference Hartman, Hox and MellenberghHartman et al, 2001; Reference Vollebergh, Iedema and BijlVollebergh et al, 2001; Reference Hudson, Mangweth and PopeHudson et al, 2003; Reference Hettema, Prescott and KendlerHettema et al, 2004; Reference KendlerKendler, 2004; Reference Khan, Jacobson and GardnerKhan et al, 2005; Reference Schoevers, Deeg and van TilburgSchoevers et al, 2005; Reference WatsonWatson, 2005). Resolution of this issue is central to both the development of methods for classifying internalising disorders and for understanding the aetiological processes that underlie these disorders (Reference Kendler, Neale and KesslerKendler et al, 1992; Reference Brown, Choi pita and BarlowBrown et al, 1998; Reference Kovacs and DevlinKovacs & Devlin, 1998; Reference Krueger, Caspi and MoffittKrueger et al, 1998; Reference KruegerKrueger, 1999; Reference Hudson, Mangweth and PopeHudson et al, 2003; Reference LilienfeldLilienfeld, 2003; Reference Hettema, Prescott and KendlerHettema et al, 2004; Reference ClarkClark, 2005).
In this paper we develop a structural equation model of the underlying structure of internalising disorder symptoms, and we fit this model to data gathered on a birth cohort of nearly 1000 young people studied on three occasions from the ages of 18 to 25 years. The general aims of this model were to examine the role of generalised and disorder-specific factors in the within-time comorbidity of disorder and the across-time continuity of disorders. Underlying this model is a general concern with estimating the fractions of variance and covariance between internalising symptoms which can be explained by a generalised tendency to internalising, and how much of this variance and covariance is disorder-specific.
METHOD
Background to the model
Fig. 1 shows a conceptual model of the within- and across-time structures of internalising symptoms (major depression, generalised anxiety disorder, phobia, panic) assessed at three time periods (t1, t2, t3). The structure of the model can be thought of as comprising two linked components.
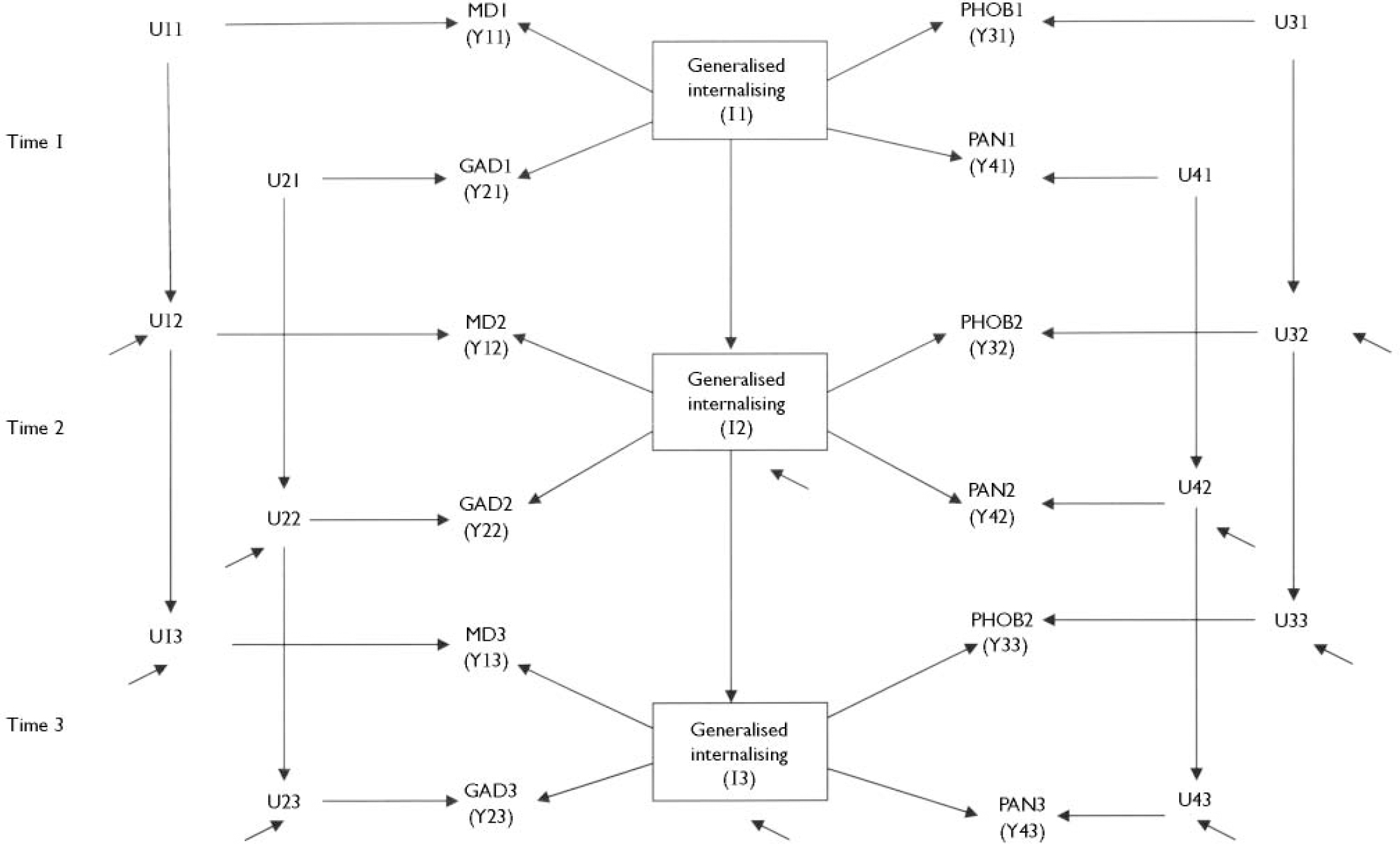
Fig. 1 Hypothetical model of within-time and across-time structure of internalising symptoms at three times. MDt, major depression symptom score at time t; GADt, generalised anxiety symptom score at time t; PHOBt, phobia symptom score at time t; PANt, panic symptom score at time t; It, generalised internalising score at time t (t=1, 2, 3). A detailed description of the model specification is given in the statistical analysis section. In this specification the Yit (i=1, 2, 3, 4; t=1, 2, 3) represents the observed symptom score for the i-th symptom type (MD, GAD, PHOB, PAN respectively) at time t, and Uit is the disorder-specific component of Yit that is not in common with generalised internalising.
-
(a) The within-time model assumes that the observed symptom measures of major depression, generalised anxiety disorder, phobia and panic at each time t are linked by a common factor model in which the variance in the symptom scores reflects variation due to a generalised internalising factor (It), and variation specific to each disorder (Uit).
-
(b) The across-time model assumes that continuities between disorders can arise by two routes: mediated via the continuity of the generalised internalising factor across time, and disorder-specific.
If it is assumed that all relationships within the model are linear and additive, then the model in Fig. 1 may be written as a structural equation model. The full specification of the model is given in the statistical section below.
The major advantage of the conceptual model in Fig. 1 is that it resolves the lumper/splitter debate by partitioning the variance of the symptom scores into components reflecting generalised internalising and disorder-specific variance. Further, the across-time model makes it possible to examine the extent to which continuities in internalising symptoms are mediated by the across-time stability of generalised internalising or via disorder-specific pathways. Finally, the model has the advantage of being testable, since the number of model parameters is smaller than the number of observed variances and covariances (see discussion of the identification status of the model below).
In the remainder of this paper we will fit the model in Fig. 1 to data on DSM–IV (American Psychiatric Association, 1994) internalising symptoms gathered on a birth cohort of young adults studied at ages 18, 21 and 25 years. The aims of this analysis are to determine the extent to which the model in Fig. 1 provides an adequate account of within- and across-time relationships between internalising disorder symptoms, and to examine the implications of the model for diagnostic classification and the understanding of the origins of internalising disorders.
Participants
The data were gathered during the course of the Christchurch Health and Development Study. In this study a birth cohort of 1265 children (635 boys and 630 girls, born in the Christchurch, New Zealand urban region in mid-1977) was studied at birth, 4 months, 1 year, annually to 16 years, and at 18, 21 and 25 years (Reference Fergusson, Horwood and ShannonFergusson et al, 1989; Reference Fergusson and HorwoodFergusson & Horwood, 2001). The present analyses are based on the sample of 953 study participants who were interviewed on measures of internalising disorders at the ages of 18, 21 and 25 years. This sample represented 75% of the initial cohort of participants enrolled in the study. All study information was collected on the basis of signed and informed consent from participants.
Internalising symptoms
Study participants were interviewed at the ages of 18, 21 and 25 years on a structured mental health interview designed to assess aspects of mental health and psychosocial adjustment since the previous assessment. All interviews were conducted in private by trained lay interviewers at a location convenient to the respondent. As part of the mental health assessment at each age, components of the Composite International Diagnostic Interview (CIDI; World Health Organization, 1993) were used to assess DSM–IV symptom criteria for a range of internalising disorders, including major depression, general anxiety disorder, social phobia, specific phobia, and panic disorders with or without agoraphobia. Using these data, summary measures of the extent of internalising disorder symptoms were constructed for each of the periods 16–18 years, 18–21 years and 21–25 years in the following ways.
Major depression
At each interview, participants were questioned about major depressive symptoms occurring in the past month, the past 12 months and the period back to the previous assessment. Participants who at any time reported a depressive episode involving either of the two core symptom criteria for major depression (feeling sad, miserable or depressed, or loss of interest in daily activities) were further questioned about the occurrence of other DSM–IV symptoms. For the purposes of the present analysis, a depressive symptoms score was constructed for each assessment period based on a count of the number of DSM–IV major depression symptoms reported at any time during the assessment period.
Generalised anxiety disorder
At each interview, participants were questioned about the occurrence of episodes of feeling tense, anxious or worried most of the time since the previous assessment. Young people who reported an episode lasting at least 1 month or longer were further questioned about the duration and source of the anxiety and associated DSM–IV criterial symptoms. For the purposes of the present analysis, a generalised anxiety disorder symptom score was constructed for each assessment period, based on a count of the number of anxiety symptoms reported from the following list of DSM–IV criterial symptoms: feeling restless, keyed up or on edge; getting tired very easily; having difficulty concentrating; feeling irritable; muscles feeling tense, sore or aching; having trouble getting to sleep or staying asleep.
Phobia
Participants were questioned about DSM–IV criterial symptoms for social and specific phobia, including the nature of the fear, the level of distress experienced, avoidant behaviours, the extent of impairment of functioning and the extent of anxiety symptom experienced upon exposure to the source. For the purposes of the present analysis, a phobia symptoms score was computed for each interview period, based on a count of the number of anxiety symptoms that the young person reported experiencing when exposed to any social or specific phobia stimulus. These symptoms included: feeling nervous and panicky; sweating; heart beating faster; shortness of breath; blushing or shaking; feeling like vomiting; concern that they might do something embarrassing.
Panic
At each interview, participants were questioned about panic attacks occurring since the previous assessment, and CIDI items were used to assess relevant DSM–IV criterial symptoms. As part of this questioning, participants were asked to describe their most serious panic attack occurring during the interview period and any associated symptoms. For the purposes of the present analysis, a panic symptoms score was created for each interview period, based on a count of the number of panic attack symptoms reported for the most severe attack out of the list of 13 DSM–IV criterial symptoms. In view of the low base rate of panic, no attempt was made to distinguish between panic attacks occurring in the presence or absence of agoraphobia.
Statistical analysis
The above measures of internalising, comprising four symptom scores (major depression, generalised anxiety disorder, phobia, panic) assessed at three time periods, formed the input data for fitting the model depicted in Fig. 1. Let Yit represent the symptom score for the i-th diagnostic domain (i=1, 2, 3, 4) at the t-th time period (t=1, 2, 3), It represent the measure of generalised internalising at each time, t and Uit the disorder-specific component of Yit. Then, subject to the assumption that the associations between variables are linear and additive, this model may be represented as a structural equation model defined by the following system of equations.
Within-time model:
Across-time model:
In these equations, the coefficients λit represent the factor loadings of the observed symptom scores (Yit) on the underlying measures of generalised internalising (It). If all variables in the model are standardised, the squares of these coefficients represent the proportion of variance in the observed symptom scores that is accounted for by generalised internalising. The across-time continuities in generalised internalising (It) and disorder-specific components (Uit) are assumed to be related by an autoregressive model with coefficients γt and Bit respectively. The terms Et and Wit represent disturbance terms in the across-time components of the model. These disturbance terms are assumed to be mutually uncorrelated. In addition, the model assumes that both the disorder-specific components Uit and the disturbances Wit are uncorrelated with the measures of generalised internalising It.
The above model may be fitted to the correlation matrix of the 12 observed symptom scores (4 disorder symptom scores at 3 times). A necessary condition for the model to be identifiable (estimable) is that the number of model parameters to be estimated is less than or equal to the number of non-redundant elements (k) of the observed correlation matrix (k=78). The model specification for Fig. 1 has a total of 34 parameters to be estimated (12 factor loadings λit, 8 parameters Bit, 2 parameters γt and 12 variances for the terms Uit and Wit). The model is identified with 44 degrees of freedom. Further, because the number of model parameters is substantially less than the number of non-redundant correlation elements, the model is falsifiable to the extent that an inadequate model may be rejected on the basis of poor fit to the observed data.
In the present analysis, models were fitted to the matrix of polychoric correlations between the observed symptom measures. Model fitting was conducted using LISREL 8 (Reference Joreskog and SorbomJoreskog & Sorbom, 1993a ) and methods of weighted least squares estimation. These methods are more appropriate for the situation in which data are non-normally distributed (Reference Joreskog and SorbomJoreskog & Sorbom, 1993a ), and were used in the present instance because the observed report data were highly skewed. Assessment of model fit was based on evaluation of a number of fit indices including the chi-squared goodness-of-fit index, the root mean-squared error of approximation (RMSEA), the root mean-squared residual correlation (RMSR), the adjusted goodness-of-fit index (AGFI), and the comparative fit index (CFI). A well-fitting model should have an RMSEA of less than 0.05, an RMSR close to zero, and AGFI and CFI indices close to 1 (Reference Joreskog and SorbomJoreskog & Sorbom, 1993b ). Finally, the model was extended to include gender, and tests of gender heterogeneity were conducted using the multiple indicators, multiple causes (MIMIC) modelling approach described by Muthen (Reference MuthenMuthen, 1989).
RESULTS
Correlations
Table 1 shows the matrix of polychoric correlations between the measures of major depression, generalised anxiety disorder, phobia and panic symptom scores assessed at ages 16–18, 18–21 and 21–25 years. This table shows the presence of significant correlations between measures both within and across time periods.
Table 1 Matrix of polychoric correlations between major depression, generalised anxiety disorder, phobia and panic symptom scores (at 18, 21 and 25 years of age)
| Measure | Y11 | Y21 | Y31 | Y41 | Y12 | Y22 | Y32 | Y42 | Y13 | Y23 | Y33 | Y43 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age 18 years | ||||||||||||
| Major | 1.00 | |||||||||||
| depression (Y11) | ||||||||||||
| GAD (Y21) | 0.56 | 1.00 | ||||||||||
| Phobia (Y31) | 0.45 | 0.45 | 1.00 | |||||||||
| Panic (Y41) | 0.55 | 0.58 | 0.57 | 1.00 | ||||||||
| Age 21 years | ||||||||||||
| Major | 0.51 | 0.29 | 0.30 | 0.36 | 1.00 | |||||||
| depression (Y12) | ||||||||||||
| GAD (Y22) | 0.41 | 0.41 | 0.28 | 0.47 | 0.51 | 1.00 | ||||||
| Phobia (Y32) | 0.33 | 0.26 | 0.51 | 0.36 | 0.35 | 0.31 | 1.00 | |||||
| Panic (Y42) | 0.38 | 0.38 | 0.37 | 0.49 | 0.49 | 0.60 | 0.60 | 1.00 | ||||
| Age 25 years | ||||||||||||
| Major | 0.38 | 0.19 | 0.21 | 0.32 | 0.48 | 0.29 | 0.27 | 0.41 | 1.00 | |||
| depression (Y13) | ||||||||||||
| GAD (Y23) | 0.28 | 0.20 | 0.18 | 0.38 | 0.39 | 0.30 | 0.22 | 0.40 | 0.57 | 1.00 | ||
| Phobia (Y33) | 0.28 | 0.18 | 0.42 | 0.34 | 0.27 | 0.22 | 0.56 | 0.40 | 0.37 | 0.32 | 1.00 | |
| Panic (Y43) | 0.17 | 0.15 | 0.21 | 0.26 | 0.34 | 0.21 | 0.36 | 0.48 | 0.52 | 0.53 | 0.44 | 1.00 |
Model fitting
The conceptual model in Fig. 1 showed a generally good fit to the data in terms of measures of goodness-of-fit (RMSEA = 0.032, P-value for test of close fit (RMSEA<0.05)=0.99; RMSR=0.065; AGFI=0.98; CFI=0.98). However, the model chi-square statistic proved to be significant (χ2=85.5; d.f.=44; P=0.0002). Examination of modification indices and model residuals suggested the model fit could be significantly improved by two changes to the original model specification. First, for major depression and phobia an additional disorder-specific pathway from time 1 (age 18 years) to time 3 (age 25 years) was included in the model. Second, the disorder-specific components of major depression and generalised anxiety disorder were permitted to be correlated within measurement periods.
These changes in model structure led to a significant improvement in model fit (Δχ2=24.0, d.f.=5, P<0.001) and produced an adequately fitting model on the basis of the fit indices (RMSEA=0.025, P-value for test of close fit (RMSEA <0.05)=1.00; RMSR=0.056; AGFI=0.98; CFI=0.99). The final fitted model is shown in Fig. 2. The figure gives the standardised model parameters. For ease of presentation, non-significant (P>0.05) pathways and some disturbance terms have been omitted from the model. Examination of the figure shows the following.
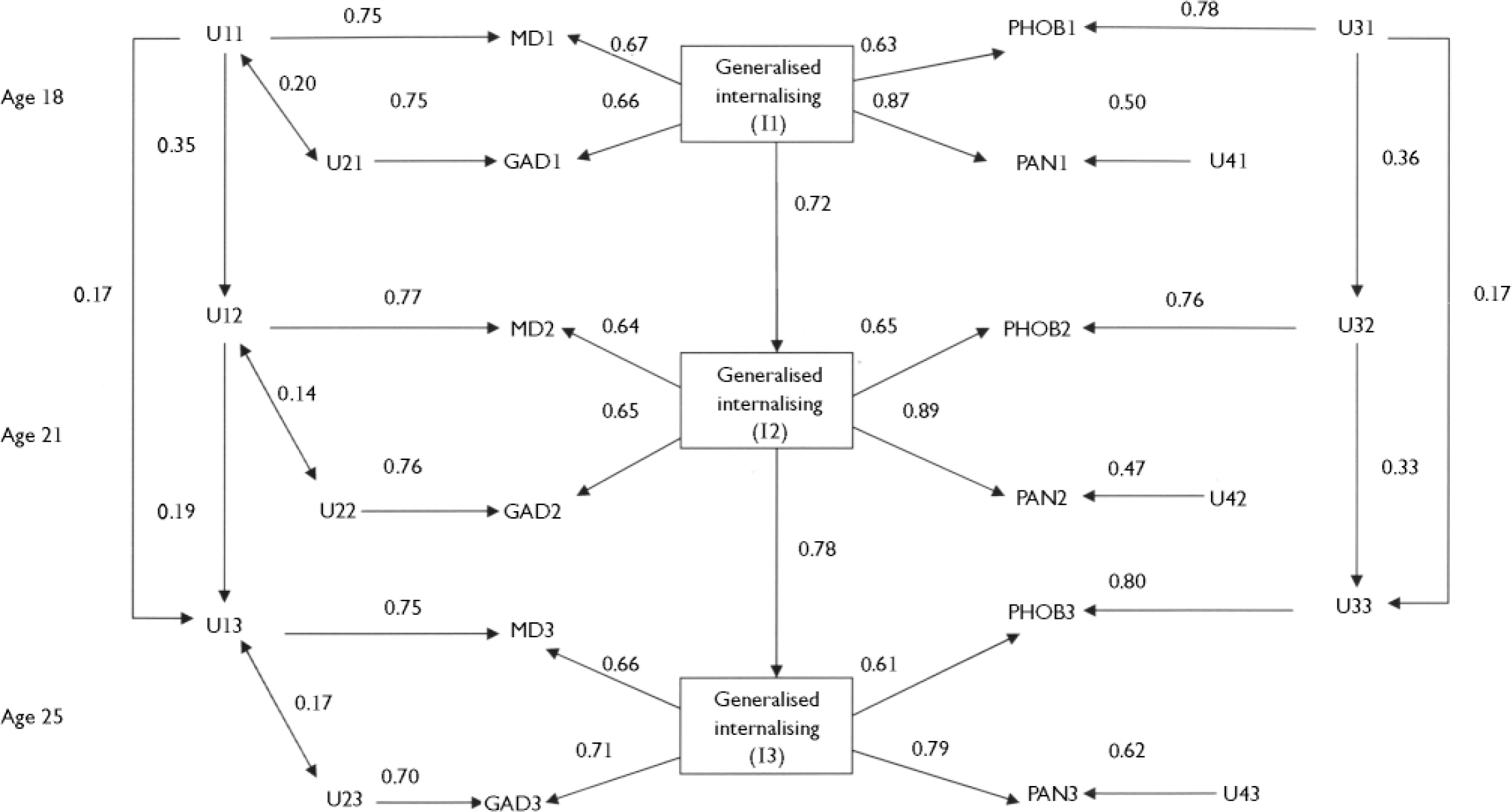
Fig. 2 Fitted model of internalising symptoms at ages 18, 21, and 25 years. MDt, major depression symptom score at time t; GADt, generalised anxiety symptom score at time t; PHOBt, phobia symptom score at time t; PANt, panic symptom score at time t; It, generalised internalising score at time t (t=1,2,3). Uit(i=1,2,3,4;t=1,2,3) represents the disorder-specific component of the observed symptom score for the i-th symptom type (MD, GAD, PHOB, PAN respectively) at time t.
Model interpretation
The within-time structure
The fitted model shows that each of the measures (major depression, generalised anxiety disorder, phobia and panic) had strong and statistically significant loadings on the generalised internalising factor. These loadings ranged from 0.64 to 0.89 with a median value of 0.66. This aspect of the model makes it possible to decompose the variance of each test at each time into two uncorrelated components: the test variance that was in common with the generalised internalising measure, and the test variance specific to the measure. These variance decompositions are shown in Table 2. This table shows that the generalised internalising factor explained in the region of 41% to 45% of the variance in major depression symptoms; 42% to 50% of the variance in generalised anxiety disorder symptoms; 37% to 42% of the variance in phobia symptoms; and 62% to 78% of the variance in panic symptoms. These results suggest that the generalised internalising factor explained from just under a half to just over three-quarters of the observed symptom score variance, with the remaining variance (including error variance) being specific to the test. Furthermore, aside from the small correlation between the residuals for major depression and generalised anxiety disorder, all of the within-time comorbidity of the observed symptom scores was explained by generalised internalising.
Table 2 Percentage of within-time variance in disorder symptom scores owing to generalised internalising
| Symptom measure | % of variance owing to internalising | ||
|---|---|---|---|
| 18 years of age | 21 years of age | 25 years of age | |
| Major depression | 44.5 | 41.3 | 43.6 |
| GAD | 43.4 | 41.7 | 50.4 |
| Phobia | 39.3 | 41.6 | 36.8 |
| Panic | 75.0 | 78.3 | 61.8 |
The across-time structure
The fitted model shows that there were two general routes leading to the across-time continuity of symptom scores. First, this continuity was mediated by the linkages between each test and the generalised internalising factor. Second, there was homotypic continuity independently of the mediating effect of generalised internalising. These features of the model make it possible to decompose the across-time correlations of tests into two additive components: the component mediated via generalised internalising, and the component independent of generalised internalising. These decompositions are given in Table 3. The table shows that all of the across-time continuity of generalised anxiety disorder and panic symptoms was mediated by generalised internalising. However, for major depression and phobia there was evidence of further pathways in which the presence of symptoms at one time influenced the same type of symptoms at a later time independently of the effects of generalised internalising. The results show that, for major depression symptoms, in the region of 62% to 69% of the across-time correlations were mediated via generalised internalising and the remainder were specific to depression. For phobia symptoms, between 56% and 58% of the across-time correlations were mediated via generalised internalising and the remainder were specific to phobia.
Table 3 Decomposition of across-time correlations of disorder symptom scores
| Correlation | Estimated total correlation from fitted model | Component owing to continuity in internalising | Component owing to disorder-specific continuity |
|---|---|---|---|
| Major depression | |||
| Age 18-21 | 0.51 | 0.31 | 0.20 |
| Age 21-25 | 0.48 | 0.33 | 0.15 |
| Age 18-25 | 0.38 | 0.25 | 0.13 |
| GAD | |||
| Age 18-21 | 0.39 | 0.39 | NS |
| Age 21-25 | 0.35 | 0.35 | NS |
| Age 18-25 | 0.26 | 0.26 | NS |
| Phobia | |||
| Age 18-21 | 0.50 | 0.29 | 0.21 |
| Age 21-25 | 0.54 | 0.31 | 0.23 |
| Age 18-25 | 0.39 | 0.22 | 0.17 |
| Panic | |||
| Age 18-21 | 0.45 | 0.45 | NS |
| Age 21-25 | 0.52 | 0.52 | NS |
| Age 18-25 | 0.39 | 0.39 | NS |
Supplementary analysis
To examine the extent to which the core model structure varied with gender, the model fitted in Fig. 2 was extended to include gender, and the methods described by Muthen (Reference MuthenMuthen, 1989) were used to test for gender heterogeneity. This analysis showed that gender was significantly correlated with the measures of generalised internalising (r=0.28 to 0.47, P<0.001), reflecting a significant tendency for girls and women to exhibit higher general levels of internalising behaviour. However, there was no evidence to suggest that other aspects of model structure, including the factor loadings for the internalising symptom scores and the continuities of either the generalised internalising or the specific disorder components, varied with gender.
DISCUSSION
The structure of internalising
In this paper we have used data gathered over the course of a longitudinal study to examine the within- and across-time structure of DSM–IV symptom measures of internalising disorders including major depression, generalised anxiety disorder, phobias and panic disorders. The best fitting structural model proved to be a hybrid of two traditions that have dominated the description of internalising symptoms. First, the results support the view that the current DSM disorder classifications represent unique and to some extent non-overlapping domains of internalising behaviours. At the same time, the model also suggests that the within-time comorbidity of these domains of disorder is explained by a common generalised internalising factor. Thus, there is evidence for both the lumper and splitter positions on the classification of internalising disorders, with some fraction of the variance in symptom scores reflecting a generalised dimension of internalising, whereas the remaining variance is disorder-specific. These conclusions are generally consistent with the results of previous models of symptom data that have produced evidence for both lumper and splitter positions (Reference Mineka, Watson and ClarkMineka et al, 1998; Krueger, Reference Krueger1999, Reference Krueger2002; Reference WatsonWatson, 2005).
On occasions, the diagnostic categories reported in nosologies such as DSM–IV are treated as if they represent homogeneous disorders having a common set of aetiological factors. The present analysis suggests that such an interpretation is implausible, in that the origins of these disorders are likely to be complex and heterogeneous, reflecting factors that are common to all internalising and factors that are specific to a given disorder. The model estimates suggest that in the region of half to three-quarters of the variance in disorder symptom scores reflects a generalised internalising factor, with the remaining variance being specific to the specific disorders.
Across-time continuities
It has been well documented that internalising disorders tend to recur, and there is evidence of both homotypic continuity in which the same disorders show recurrence over time, and heterotypic continuity in which the onset of one disorder leads to an increased risk of the later onset of other internalising disorders (Keller et al, Reference Keller, Lavori and Mueller1992a ,Reference Keller, Lavori and Wunder b ; Reference McGee, Feehan and WilliamsMcGee et al, 1992; Reference Angold, Costello and ErkanliAngold et al, 1999; Reference LilienfeldLilienfeld, 2003). An understanding of the development of internalising disorders thus requires models that take into account both homotypic and heterotypic continuity. The model developed in this paper achieves this by permitting continuity of disorder by two routes. First, it is assumed that continuity of disorder may arise via the continuity of the generalised internalising factor across time. Second, the model permits specific homotypic continuity of disorders.
The fitted model leads to two major conclusions about the nature of across-time continuity in internalising disorders. First, much of the across-time continuity in internalising disorders reflects the strong across-time continuity of the internalising factors. This result suggests that much of the homotypic and all of the heterotypic continuity in internalising disorders arises because individuals predisposed to high levels of internalising show the recurrence of the same disorders and the onset of new disorders. At the same time, the results make it clear that not all of the across-time continuity in internalising disorders is mediated via generalised internalising, and there is evidence of disorder-specific homotypic continuity, this being most marked for major depression and phobias. In this respect the findings for across-time continuity mirror the findings for within-time comorbidity, and suggest the presence of both a generalised internalising component and disorder-specific components.
Generalised internalising
In turn, these findings raise speculations about the interpretation of the generalised internalising factors postulated in this analysis. This factor can be interpreted in at least three ways. First, it may be suggested that this factor represents variation in individual predisposition to internalising disorders. Under this interpretation, the generalised internalising factor has a similar interpretation to the personality trait of neuroticism (Reference EysenckEysenck, 1990). As a number of authors have pointed out, the trait of neuroticism may largely or wholly reflect individual variation in stable levels of internalising symptoms (Reference Duncan-Jones, Fergusson and OrmelDuncan-Jones et al, 1990; Reference Ormel, Rosmalen and FarmerOrmel et al, 2004). Second, it is possible that the internalising factor does not represent a dimension of personality or disorder, but rather is a latent variable that summarises the net effects of nonobserved genetic and environmental factors on individual tendencies to internalising symptoms. Finally, the internalising factor could be conceptualised as an underlying dimension reflecting the extent of generalised internalising disorder. This conceptualisation would support the view that there may be value in extending current systems of diagnostic classification to include a category of generalised internalising disorder. At the present time, there is no evidence to determine which of these interpretations is the more correct. None the less, what the analysis does make clear is that there is considerable overlap, correlation and comorbidity between internalising disorders, with this overlap adequately represented by a single, general and highly stable latent dimension.
Limitations
There are a number of important caveats that need to be placed on these results. First and foremost, the findings describe the within- and across-time structures of internalising disorders in a specific cohort, studied at a specific life stage using a specific set of measures. The extent to which the findings generalise beyond this context remains to be explored. A second potential limitation of the analysis is that we have assumed that the current DSM–IV groupings of internalising symptoms into major depression, generalised anxiety disorder, phobias, and panic disorders provides a valid account of symptom variation. Further, to secure sufficient variation for analysis we have combined some disorders (notably phobias). These coding and classification rules may influence the results and conclusions drawn.
Despite these limitations, the model developed in this paper has the major advantage that it provides a resolution to the long-standing lumper/splitter debate by showing that variation in internalising symptoms can be partitioned into generalised and disorder-specific components, with this dissection being evident in both within-time analyses of comorbidity and across-time analyses of continuity.
Acknowledgements
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.






eLetters
No eLetters have been published for this article.