


Paranoid ideation is characteristic of psychotic illness, but, like other psychotic phenomena, may be widespread in non-clinical populations.Reference van Os, Verdoux, Murray, Jones, Susser, van Os and Cannon1-Reference Kaymaz and van Os5 Wariness of the intentions of others may be adaptive in some situations, and becomes a clinical problem only when it is excessive, exaggerated or distressing, or interferes with functioning. Given that such ideation may precede delusion formation,Reference Poulton, Caspi, Moffitt, Cannon, Murray and Harrington6,Reference Kaymaz, Drukker, Lieb, Wittchen, Werbeloff and Weiser7 our understanding of delusions should be enhanced by studying paranoid thinking in non-clinical populations. In our cognitive model of persecutory delusions,Reference Freeman, Garety, Kuipers, Fowler and Bebbington8 we hypothesised that even severe paranoia builds on common emotional concerns, particularly themes of interpersonal worry or social anxiety. The interpersonal sensitivities often seen in emotional disorders (e.g. concerns about rejection or about being vulnerable) inform worries about future threat and the intention of others. In some people, these fears lead to ideas that others are watching or talking about them. Ideas of persecution are hypothesised to emerge from these ideas of reference. This process implies a close structured relationship between worry, anxiety and paranoia. It has credence, as all concern the theme of the anticipation of threat,Reference Freeman9 and there is increasing empirical evidence for links between affect and paranoia.Reference Freeman, McManus, Brugha, Meltzer, Jenkins and Bebbington10-Reference Wigman, van Nierop, Vollebergh, Lieb, Beesdo-Baum and Wittchen15
The current investigation employs data from a general population survey to examine the distribution and underlying structure of components of paranoid ideation. Our analyses were driven by the hypothesis that the overall distribution of such ideation should be similar in form to that of affective symptoms, with many people having few such thoughts and a few people having many.Reference Freeman, Garety, Bebbington, Smith, Rollinson and Fowler3,Reference Melzer, Tom, Brugha, Fryers and Meltzer16,Reference Plomin, Haworth and Davis17 Moreover, as with affective symptoms, increasing symptom counts should be characterised by the recruitment of rarer and odder ideas:Reference Sturt18 in other words, a hierarchy of paranoid thoughts underpins an inherent structure within the continuum. In our cognitive model of paranoia,Reference Freeman, Garety, Kuipers, Fowler and Bebbington8 we postulated four subcategories of paranoid experience: interpersonal sensitivities; mistrust; ideas of reference; and ideas of persecution. Moreover, we postulate that this structure arises because the subcategories are linked as part of a hierarchical process. Members of the general population would be classifiable in terms of these factors, and the resulting classification would correspondingly reflect hierarchical relationships between the factors.
These ideas can be formally tested in a number of ways. Given our specific hypotheses, three were appropriate: (1) confirmatory factor analysis (CFA), which establishes the structure of linear relationships between items; (2) latent class analysis (LCA), which attributes individuals to a number of separate classes; and (3) the hybrid procedure, factor mixture modelling analysis (FMMA), which allows the factor structure to be related to the class structure.
Method
The second British National Psychiatric Morbidity Survey was carried out on a representative sample of the British population in 2000.Reference Singleton, Bumpstead, O'Brien, Lee and Meltzer19,Reference Singleton, Lee and Meltzer20
Sample
Because of its good coverage, the British small users postcode address file was used to generate a list of private households.Reference Singleton, Bumpstead, O'Brien, Lee and Meltzer19 Full details of sampling are provided elsewhere.Reference Singleton, Lee and Meltzer20 A total of 15 804 addresses were obtained. Interviewers visited these to identify private households with at least one person aged 16-74 years. One person was selected from each qualifying household using the Kish grid method.Reference Kish21 Just under 70% of those approached agreed to a first phase interview, which the vast majority completed in full, providing 8576 individuals for the current analysis.
Design
The survey comprised two phases.Reference Singleton, Bumpstead, O'Brien, Lee and Meltzer19,Reference Singleton, Lee and Meltzer20 The first was carried out by well-trained non-clinical interviewers employed by the Office for National Statistics. It included the use of screening instruments to determine participants for a further interview by trained clinicians to establish diagnoses of psychosis and personality disorder. To test our hypotheses, we abstracted items from two screening instruments: the Psychosis Screening Questionnaire (PSQ)Reference Bebbington and Nayani22 and the questionnaire version of the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II).Reference First, Gibbon, Spitzer, Williams and Benjamin23 We used data from the 2000 British National Psychiatric Morbidity Survey as it is the only one in the British national survey programme to include both these measures.Reference Jenkins, Meltzer, Bebbington, Brugha, Farrell and McManus24
Measuring paranoia
For current purposes, we used items 2, 3, 3a and 3b from the PSQ, relating to ideas of persecution, conspiracy and interference. From the SCID-II, we used items 2, 3, 4, 6, 10, 25, 26, 27, 28, 33 and 35. These relate to different personality disorders (avoidant, dependent, paranoid and schizotypal), but were chosen a priori in line with our specific interest in cognitive content (progressing from mistrust through reference to persecution). This enabled us to test our ideas of how paranoia builds on certain common worries. Our 15 selected items approximate to those used by Freeman et al.Reference Freeman, Garety, Bebbington, Smith, Rollinson and Fowler3 On theoretical grounds, they were separated into four groups: mistrust, interpersonal sensitivities, ideas of reference, and ideas of persecution (see Table 1). We also summed the item endorsements to produce an overall paranoia score for each individual. Finally, for each item, we calculated the mean difference for the total item count between those with and those without the given item (correcting for the contribution due to that item).Reference Sturt18 We term this the excess item score.
Table 1 Frequency of individual items related to paranoia and associated excess item scores (n = 8576)

| Item | Question | Frequency % | Excess item score |
|---|---|---|---|
| Interpersonal sensitivities | |||
| PD2 | Do you avoid getting involved with people unless you are certain they will like you? | 12.6 | 3.56 |
| PD4 | Do you often worry about being criticised or rejected in social situations? | 27.7 | 3.07 |
| PD6 | Do you believe that you're not as good, as smart, or as attractive as most other people? | 25.4 | 2.49 |
| PD10 | Do you find it hard to disagree with people even when you think they are wrong? | 20.3 | 1.97 |
| Mistrust | |||
| PD3 | Do you find it hard to be 'open' even with people you are close to? | 20.8 | 2.44 |
| PD26 | Do you spend a lot of time wondering if you can trust your friends or the people you work with? | 15.5 | 3.96 |
| PD25 | Do you often have to keep an eye out to stop people from using you or hurting you? | 28.1 | 2.70 |
| PD27 | Do you find that it is best not to let other people know much about you because they will use it against you? | 21.3 | 3.13 |
| Ideas of reference | |||
| PD28 | Do you often detect hidden threats or insults in things people say or do? | 19.0 | 3.57 |
| PD33 | When you are out in public and see people talking, do you often feel that they are talking about you? | 6.5 | 5.07 |
| PD35 | When you are around people, do you often get the feeling that you are being watched or stared at? | 9.7 | 4.69 |
| Ideas of persecution | |||
| PSQ3 | Over the past year, have there been times when you felt that people were against you? | 20.9 | 3.00 |
| PSQ2 | Have you ever felt that your thoughts were directly interfered with or controlled by some outside force or person? | 9.0 | 2.03 |
| PSQ3a | Have there been times when you felt that people were deliberately acting to harm you or your interests? | 9.0 | 3.98 |
| PSQ3b | Have there been times you felt that a group of people was plotting to cause you serious harm or injury? | 1.5 | 5.52 |
PD, Structured Clinical Interview for DSM-IV Axis II Disorders, personality disorder; PSQ, Psychosis Screening Questionnaire.
Strategy of analysis
We first analysed the frequency distribution of individual paranoia scores in our total sample. We hypothesised that, as with affective symptoms,Reference Melzer, Tom, Brugha, Fryers and Meltzer16 this distribution would be exponential.
We used Mplus version 6Reference Muthén and Muthén25 for Windows to conduct the latent variable modelling. Confirmatory factor analysis is used to test specific hypotheses about the content and the number of dimensions (factors) that underlie a set of variables purporting to measure a given phenomenon (here paranoid ideation). The resulting factors help to explain the nature of the interrelationships between the observed variables (the individual paranoia items). Latent class analysis, in contrast, explores whether individuals can be classified into groups (classes) based on their particular endorsement of the paranoia items. The basic difference between the two procedures lies in the underlying latent variable - in CFA, paranoia is viewed as a continuous latent variable, whereas in LCA, it is categorical. Hybrid models, as in FMMA, incorporate both continuous and categorical latent variables - these models propose that there may be one (or more) dimension(s) of paranoia, and at different points along the dimension(s), there are groups of people (classes) who are homogeneous within class, and heterogeneous across classes, in relation to their paranoia symptoms. Hybrid models can be estimated in a variety of different ways, and the exact make-up of each model should be based on pre-existing theory, of the type we test here.
Three CFA models were tested: (1) a one-factor model representing ‘severity of paranoid ideation’; (2) a four-factor model representing our a priori factors ‘interpersonal sensitivities’, ‘mistrust’, ‘ideas of reference’ and ‘ideas of persecution’; and (3) a higher-order factor model, representing a second-order factor of ‘severity of paranoid ideation’ underpinned by the four first-order factors outlined in the previous model. Figure 1 illustrates these models. The ovals represent the latent variables or factors and the square boxes represent observed binary variables. The arrows connecting the factors to the categorical indicators (u1-u15) represent factor loadings. The curved connections between the factors represent correlations. The default estimator for this analysis was a robust maximum likelihood (WLSMV) estimator. All factor loadings were estimated, with factor variances fixed at one.
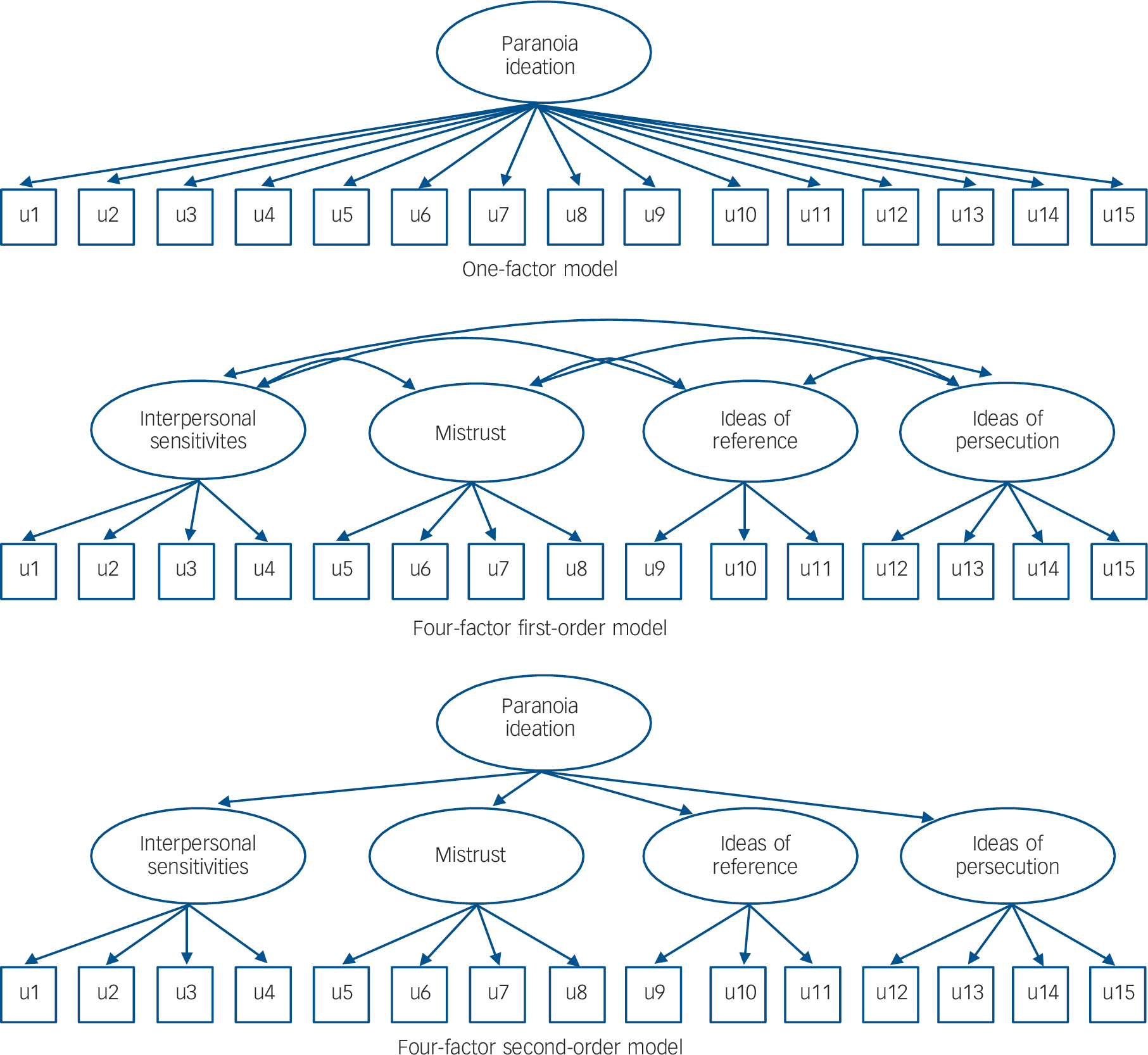
Fig. 1 Alternative factor models conceptualising the dimensionality of paranoia items.
Next, a series of successive latent class models, varying the number of classes from 1 to 8, were estimated. Latent class analysis evaluates whether a group of associated observed variables can be related to an underlying categorical variable, comprising two or more classes (levels).Reference Hagenaars and McCutcheon26 Latent class analysis, as used here, allowed us to consider not only the number of items endorsed, but also their overall pattern of distribution.Reference Shevlin, Adamson, Vollebergh, de Graaf and van Os27 Decisions regarding the most appropriate model should be guided both by statistical fit indices and by conceptual considerations, that is, the meaningfulness and distinctiveness of the latent class profiles. The default estimator for this analysis was a robust maximum likelihood (MLR) estimator. Further details outlining how these models were estimated and evaluated are provided in the online supplement.
One limitation of LCA is that it fails to account for individual difference within classes. Factor mixture modelling analysisReference Lubke and Muthén28 combines the latent class model and the common factor model, and has a single categorical, and one or more continuous, latent variables. In FMMA, continuous latent variables are used to explain the variation and covariation in a set of observed items, while the categorical latent variable represents heterogeneity at the factor level.Reference Shevlin, Adamson, Vollebergh, de Graaf and van Os27 Thus, the superiority of factor mixture models over other conventional models is that they permit simultaneous classification of people into diagnostic groups, while also modelling the severity of disorder.Reference Clark, Muthén, Kaprio, D'Onofrio, Viken and Rose29 Use of FMMA models is increasing in psychiatry. However, it is still relatively uncommon, and procedural conventions are not yet fully established. In the current study we chose to estimate five different model types, varying in terms of restrictiveness, as outlined by Clark et al Reference Clark, Muthén, Kaprio, D'Onofrio, Viken and Rose29 (Table 2).
Sampling weights and other variables that account for the complex survey design of National Psychiatric Morbidity Survey 2000 were used in all analyses to enhance the reliability and validity of the parameter estimates, standard error and model fit calculations. The default estimator for the FMMA was an MLR estimator.
Results
The prevalence of individual paranoia items
The endorsement of individual paranoia items was considerable, ranging from 1.5% to 28% (Table 1).
The total number of paranoia items could range from 0 to 15, although in the event no one scored 15 (weighted mean 2.3, s.d. = 2.6). The distribution of total scores is displayed in Fig. 2. The data could be fitted by a single continuous distribution model (16), following an exponential curve with a correlation between observed and model estimated scores of 0.99.
Table 2 Overview of five different factor mixture models (FMM) estimatedFootnote a
| Restrictiveness | Model | Factor variance | Factor covariance | Factor mean | Factor loadings | Item thresholds (latent classes) |
|---|---|---|---|---|---|---|
| FMM-1 | Fixed at zero | Fixed at zero | Varies across classes | Equal across classes | Equal across classes | |
| FMM-2 | Freely estimated | Freely estimated | Set to zero | Equal across classes | Equal across classes | |
| FMM-3 | Freely estimated, but equal across classes | Freely estimated, but equal across classes | Set to zero | Equal across classes | Allowed to vary across classes | |
| FMM-4 | Allowed to change across classes | Allowed to change across classes | Set to zero | Equal across classes | Allowed to vary across classes | |
| FMM-5 | Allowed to change across classes | Allowed to change across classes | Set to zero | Allowed to vary across classes | Allowed to vary across classes |
a. Models based on recommendations outlined by Clark et al.Reference Clark, Muthén, Kaprio, D'Onofrio, Viken and Rose29
Non-reflexive relationships between items
As predicted, positive excess item scores were associated with each item, confirming that the relationship between items was not random (Table 1). The mean excess score was 3.5 (s.d. = 1.0). However, the excess score varied between the items, ranging from 2.0 to 5.5. If the relationship between items is non-reflexive (i.e. their endorsement follows a hierarchical arrangement), the rarer items should be associated with a greater excess score than the more frequent ones. This is what we found. Thus, the excess symptom score associated with each item was significantly and strongly associated with the frequency of endorsement of that item (r = −0.79, P<0.001). For example, worry about people using or hurting the participant (frequency 28%) was associated with an excess symptom score of 2.7, whereas a belief about plots designed to cause serious harm (frequency 1.5%) was associated with an excess symptom score of 5.5.
Confirmatory factor analysis
Table 3 outlines the standardised factor loadings, factor correlations and goodness-of-fit indices for the competing CFA models. Despite moderate to strong factor loadings, the one-factor model did not generally fit the data well. Both the first- and second-order four-factor models provided a good fit to the data, with strong factor loadings (first-order ranging 0.514-0.978; second-order ranging 0.629-0.953). A chi-squared difference test for nested models (see online supplement) revealed that the first-order four-factor model was a superior fit to the one-factor model (χ2 diff = 1245.355, d.f. diff = 6, P<0.001) and the second-order four-factor model (χ2 diff = 24.656, d.f. diff = 2, P<0.001). Collectively, these model results provided strong confirmation of our a priori grouping of items.
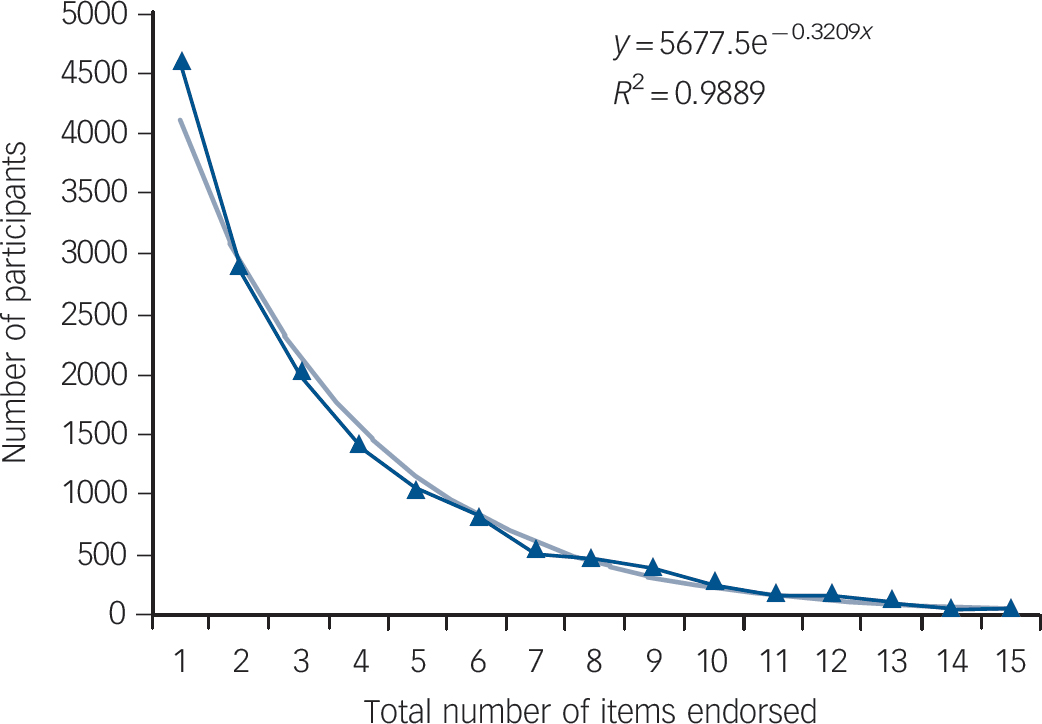
Fig. 2 The distribution of total paranoia scores in the general population.
Latent class analysis
The results for the competing latent class models are presented in Table 4. The fit indices did not identify clearly which model provided the best explanation of the data (the log-likelihood value, Akaike and Bayesian information criteria and sample size adjusted Bayesian information criterion continued to decrease as the number of classes in the models increased). This was not unexpected, given that we had hypothesised a priori that underlying the categorisation of classes is a dimension of severity. This is not captured by LCA, but can be modelled using FMMA.
Factor mixture modelling analysis
This is often useful in reducing the number of classes into more meaningful subgroups, especially if the classes are modelling differences in severity. The FMMA results presented in Table 5 should be interpreted in the light of our theoretical model of paranoia, specifically that the items are related non-reflexively, with the more extreme paranoia items being associated with a greater overall severity, as indicated by the item count. Based on the goodness-of-fit indices, two models stand out (shown in bold in Table 5): both were one-factor models with four latent classes. Following the notation of Clark et al,Reference Clark, Muthén, Kaprio, D'Onofrio, Viken and Rose29 the best-fitting model in terms of the Bayesian information criterion was the four-class variant of FMM-3 (FMM-3, 4C). This model proposes that: (1) people in the survey can be categorised into four groups (or classes): the people in each class experience a similar type of paranoid ideation, distinct from that experienced by people in the other classes; and (2) underlying each class, there is a single dimension of ‘paranoia’, which is conceptualised identically in each class (as indicated by the invariant factor loadings; range of standardised loadings 0.394-0.850). In other words, the level of paranoia ('severity') is the same in each class (as indicated by the invariant factor variance). On both theoretical and empirical grounds, this assumption is, however, implausible - people in the community with different types of paranoid experiences will vary in terms of the severity of those experiences.
We therefore considered model 4C of the FMM-4 type to be the best conceptual model overall. This provided a good explanation of the data, very similar to its FMM-3 equivalent, and was less restrictive, in that the factor variances were allowed to vary across classes. This implies differences in terms of the severity of paranoid ideation, both between classes and within each class, i.e. between the class members (see Muthén & Asparouhove30).
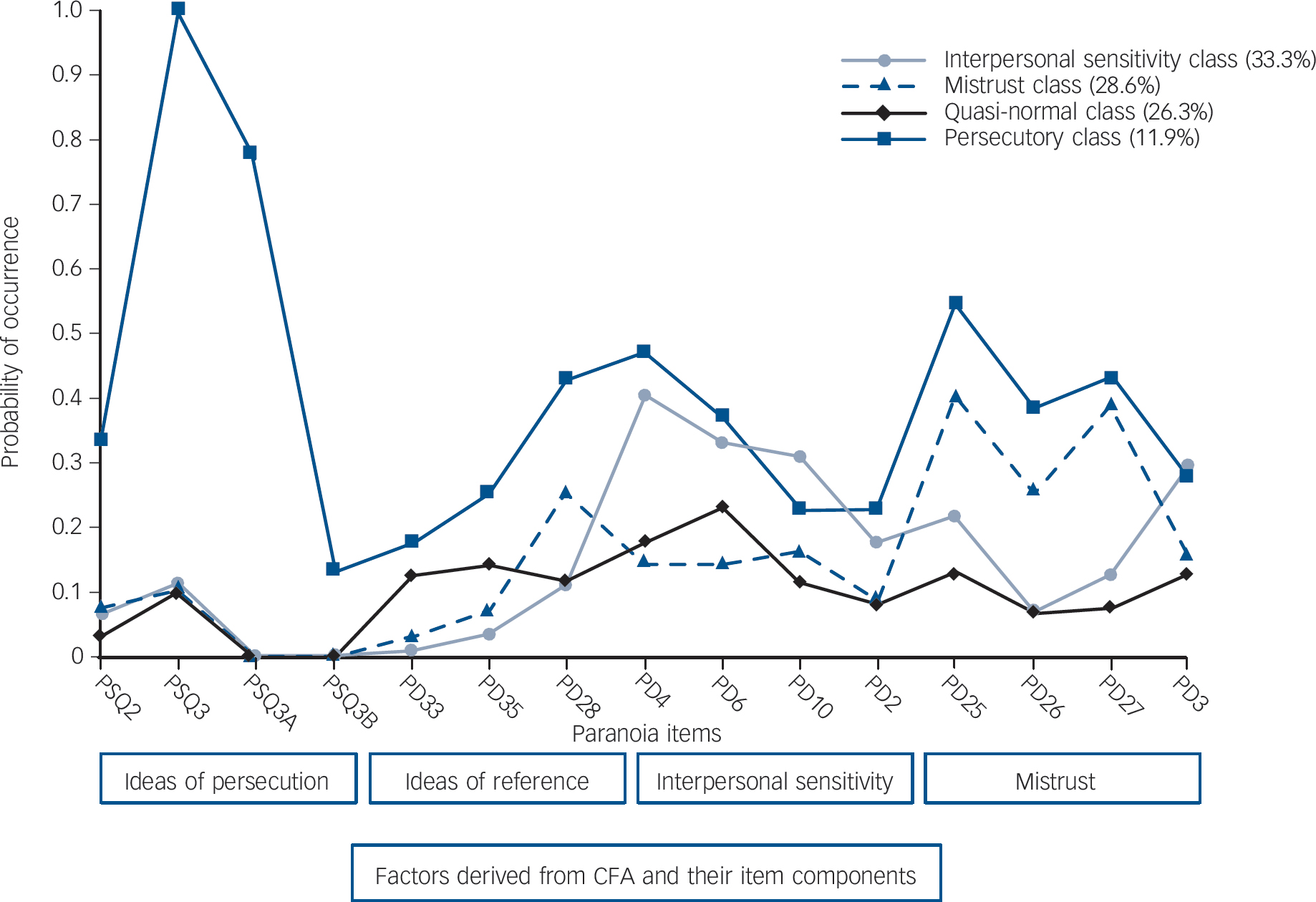
The estimated probabilities for the paranoia items derived from model FMM-4 are illustrated in Fig. 3. The items are grouped within the factors tested by the CFA. The three largest classes between them include nearly 90% of participants (each class accounting for between a quarter and a third), and were characterised by a uniformly low probability of endorsing ideas of persecution. The largest class comprised 33.3% of the sample, and as a group its members scored highly on interpersonal sensitivity and moderately on mistrust: it is best described as the interpersonal sensitivity class. The second class was almost as common (28.6%). It can be termed the mistrust class, as its members scored more highly than the interpersonal sensitivity class on the mistrust items, but lower on interpersonal sensitivity. These two classes both displayed some endorsement of item 28 of the SCID-II in the ideas of reference factor ('Do you often detect hidden threats or insults in things people say or do?'), an item that shares attributes of interpersonal sensitivity. The members of class 3 had roughly equal rates of endorsement of ideas of reference, interpersonal sensitivity, and mistrust. Their endorsement of the items in these three factors was relatively infrequent, varying between 10% and 20%. Consequently, they scored slightly higher on ideas of reference than the first two classes. Nevertheless, given their relatively low rates of overall endorsement of items, they might reasonably be designated the quasi-normal class. The fourth class was much less common than the first three (11.9%). It was also much more symptomatic, characterised by a high probability of perceiving direct threats to personal safety (all of them felt people were against them, three-quarters agreed that people were deliberately trying to harm them, and nearly 15% thought people were plotting against them). It was the only group that scored highly on ideas of persecution, and its endorsement of items from the other three factors was almost invariably higher than that of the other classes. They constitute a clear persecutory class. The ‘severity’ factor variance for the underlying paranoid ideation dimension was lowest in the mistrust class (0.45), followed by the interpersonal sensitivity class (0.48), then the persecutory class, and finally the quasi-normal class (0.97).
Table 3 Standardised factor loadings, factor correlations, and goodness-of-fit statistics for three competing confirmatory factor analytic models of 15 paranoia items from 2000 British National Psychiatric Morbidity Survey (n = 8576)
| Models | ||||||
|---|---|---|---|---|---|---|
| 1-factor | 4-factor first-order model | 4-factor second-order modelFootnote a, Footnote b | ||||
| F1 | F1 | F2 | F3 | F4 | ||
| Item details | ||||||
| PSQ2: Thoughts interfered with/controlled by outside force | 0.532 | 0.644 | ||||
| PSQ3: Felt people were against you | 0.685 | 0.978 | ||||
| PSQ3a: Felt people were deliberately acting to harm you/interestsFootnote c | 0.700 | 0.952 | ||||
| PSQ3b: Felt that a group was plotting to cause you serious harm/injuryFootnote c | 0.672 | 0.904 | ||||
| PD33: Out in public and see people talking, feel they are talking about you | 0.835 | 0.869 | ||||
| PD35: Feel being watched or stared at | 0.839 | 0.881 | ||||
| PD28: Detect hidden threats or insults in things people say or do | 0.764 | 0.817 | ||||
| PD4: Worry about being criticised/rejected in social situations | 0.735 | 0.845 | ||||
| PD6: Not as good/smart/attractive as most other people | 0.600 | 0.681 | ||||
| PD10: Hard to disagree with people even when you think they are wrong | 0.452 | 0.514 | ||||
| PD2: Avoid getting involved with people unless certain they will like you | 0.674 | 0.761 | ||||
| PD25: Keep an eye out to stop people from using you or hurting you | 0.678 | 0.720 | ||||
| PD26: Wonder if you can trust your friends/work people | 0.801 | 0.853 | ||||
| PD27: Don't let people know much about you because they'll use it against you | 0.725 | 0.769 | ||||
| PD3: Find it hard to be ‘open’ even with people you are close to | 0.544 | 0.576 | ||||
| Second-order factor loadings | F1 = 0.825; F2 = 0.934; F3 = 0.953; F4 = 0.629 | |||||
| Goodness-of-fit statistics | ||||||
| Chi-squared | 2850.027 | 938.400 | 951.965 | |||
| d.f. | 90 | 84 | 86 | |||
| P | <0.0001 | <0.0001 | <0.0001 | |||
| Comparative fit index | 0.908 | 0.972 | 0.971 | |||
| Tucker Lewis index | 0.893 | 0.964 | 0.965 | |||
| Root mean square error of approximation | 0.060 | 0.034 | 0.034 | |||
F1, interpersonal sensitivities; F2, mistrust; F3, ideas of reference; F4, ideas of persecution; PD, Structured Clinical Interview for DSM-IV Axis II Disorders, personality disorder; PSQ, Psychosis Screening Questionnaire.
a. Factor loadings for 4-factor first-order model are the same for the 4-factor second-order model.
b. Second-order factor represents ‘severity of paranoia ideation’.
c. Missing values for PSQ3a and PSQ3b are recoded as zero (not asked of participant because assumed negative).
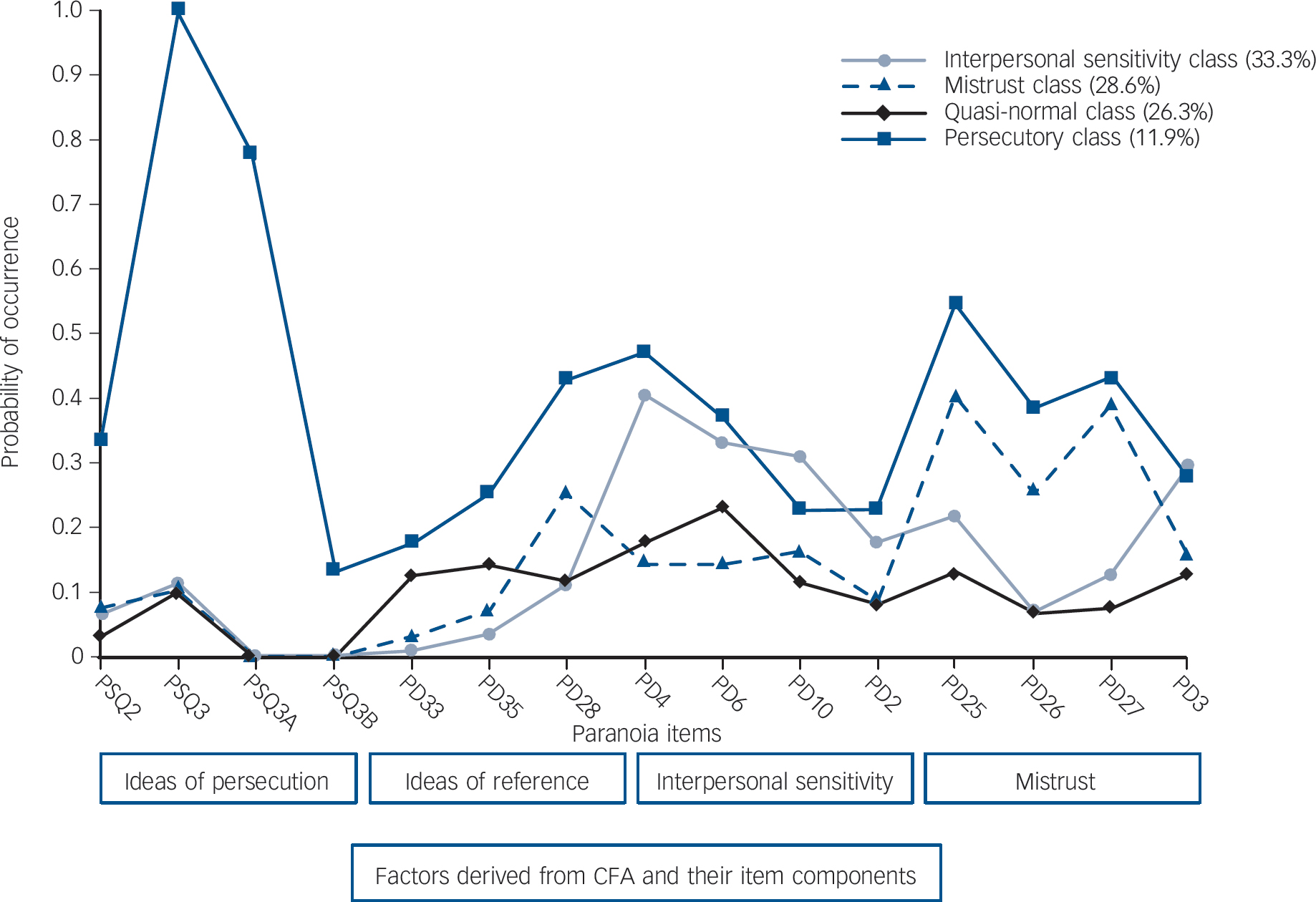
Fig. 3 Estimated probabilities for the occurrence of 15 paranoia items in the one-factor four-class mixture model (FMM-4).
CFA, confirmatory factor analysis; PSQ, Psychosis Screening Questionnaire; PD, Structured Clinical Interview for DSM-IV Axis II Disorders, personality disorder.
Table 4 Results from latent class analysis of 15 paranoia items in the 2000 British National Psychiatric Morbidity Survey (n = 8576)
| Model | Log-likelihood | Replicated log-likelihood | Free parameters, n | AIC | BIC | SSABIC | LMR-LRT (P) | Entropy |
|---|---|---|---|---|---|---|---|---|
| 1c | –53653.224 | Yes | 15 | 107336.449 | 107442.300 | 107 394.632 | NA | NA |
| 2c | –46637.077 | Yes | 31 | 93336.154 | 93554.912 | 93456.400 | 13 936.122 (<0.001) | 0.849 |
| 3c | –45698.149 | Yes | 47 | 91490.298 | 91821.964 | 91672.606 | 1864.986 (<0.001) | 0.751 |
| 4c | –44805.585 | Yes | 63 | 89737.169 | 90181.743 | 89981.540 | 1772.894 (<0.001) | 0.799 |
| 5c | –44467.169 | Yes | 79 | 89092.338 | 89649.819 | 89398.771 | 672.192 (<0.001) | 0.790 |
| 6c | –44190.940 | Yes | 95 | 88571.880 | 89242.268 | 88940.375 | 548.672 (<0.001) | 0.785 |
| 7c | –44068.571 | Yes | 111 | 88359.142 | 89142.438 | 88789.700 | 243.061 (0.0138) | 0.795 |
| 8c | –43970.504 | No | 127 | 88195.008 | 89091.211 | 88687.628 | 194.790 (0.0265) | 0.793 |
AIC, Akaike information criterion; BIC, Bayesian information criterion; SSABIC, sample size adjusted Bayesian information criterion; LMR-LRT, Lo, Mendell and Rubin likelihood ratio test.
Table 5 Results from factor mixture models (FMM) of 15 paranoia items in the 2000 British National Psychiatric Morbidity Survey (n = 8576)Footnote a
| Model | Log-likelihood | Replicated log-likelihood | Free parameters, n | AIC | BIC | SSABIC |
|---|---|---|---|---|---|---|
| FMM-1 | ||||||
| 2c | –46637.077 | Yes | 31 | 93336.154 | 93554.3912 | 93456.400 |
| 3c | –45746.095 | Yes | 33 | 91558.189 | 91791.061 | 91686.193 |
| 4c | –45619.330 | Yes | 35 | 91308.659 | 91555.645 | 91444.421 |
| 5c | –45593.659 | Yes | 37 | 91261.317 | 91522.416 | 91404.837 |
| FMM-2 | ||||||
| 2c | –45596.157 | Yes | 33 | 91258.315 | 91491.187 | 91386.319 |
| 3c | –45562.565 | No | 36 | 91197.131 | 91451.173 | 91336.771 |
| 4c | –45594.967 | No | 39 | 91267.934 | 91543.146 | 91419.211 |
| 5c | –45593.219 | No | 42 | 91270.439 | 91566.821 | 91433.353 |
| FMM-3 | ||||||
| 2c | –44434.219 | Yes | 46 | 88960.438 | 89285.047 | 89138.867 |
| 3c | –44054.713 | Yes | 62 | 88233.426 | 88670.943 | 88473.918 |
| 4c | –43919.327 | Yes | 78 | 87994.653 | 88545.078 | 88297.207 |
| 5c | –43846.883 | Yes | 94 | 87881.766 | 88545.098 | 88246.383 |
| FMM-4 | ||||||
| 2c | –44433.857 | Yes | 47 | 88961.715 | 89293.381 | 89144.023 |
| 3c | –44052.647 | Yes | 64 | 88233.294 | 88684.924 | 88481.544 |
| 4c | –43917.581 | Yes | 81 | 87997.163 | 88568.758 | 88311.354 |
| 5c | –43844.729 | Yes | 98 | 87885.458 | 88577.016 | 88265.590 |
| FMM-5 | ||||||
| 2c | –44419.630 | No | 61 | 88961.261 | 89391.721 | 89197.874 |
| 3c | –43993.243 | No | 92 | 88170.485 | 88819.704 | 88527.344 |
| 4c | –43846.878 | No | 123 | 87939.756 | 88807.733 | 88416.861 |
| 5c | –43795.600 | No | 154 | 87899.200 | 88985.935 | 88496.551 |
AIC, Akaike information criterion; BIC, Bayesian information criterion; SSABIC, sample size adjusted Bayesian information criterion.
a. Specific details about model estimation are outlined in Table 1. Bold print indicates the best fitting models based on fit indices (see Discussion).
Discussion
In this paper we used a secondary analysis of items from the SCID-II questionnaire and the PSQ to identify structural relationships in the spectrum of paranoid ideation. These items have face validity for detecting paranoid ideation, in that, because of the form they take, they seem likely to distinguish both between different thought contents and between people with stronger and weaker paranoid inclinations. They were selected a priori to test our hypotheses and no other items were examined.
Some of the items were endorsed by 20-30% of the general population. These covered a consciousness of a lack of assertiveness, worries over social inferiority, worries over criticism by others, feelings that people were generally against the respondent and might use or hurt them, and a reluctance to reveal too much in case people used it in adverse ways. Ideas of reference involving the detection of hidden threats or insults were almost as common. A sixth of the population spent a lot of time wondering whether they could trust their friends or work colleagues. About 10% of the population sometimes felt that people were watching them, staring at them, deliberately acting to harm them or trying to control their thoughts. Slightly fewer felt that people in public places might be talking about them. Finally, a much smaller proportion, but still nearly 2% of the population, thought that some group was plotting to cause them serious harm or injury.
Our results supported our initial hypothesis that items reflecting paranoid ideation would follow an exponential distribution like that seen with affective symptoms.Reference Melzer, Tom, Brugha, Fryers and Meltzer16 Only one other group seems to have approached attributes relating to paranoia in this way, albeit by using conventional categories of personality disorder.Reference Lyoo, Youn, Ha, Park and Kwon31 They found a slightly different (cubic) curve of distribution for items forming the diagnostic criteria for paranoid personality disorder (the item count with the highest frequency was 2 rather than 0).
Confirmatory factor analysis provided strong evidence in support of our postulated categorisation of paranoid experience, clearly identifying factors representing mistrust, interpersonal sensitivity, ideas of reference, and ideas of persecution. Latent class analysis models offered only an incomplete account of the data. However, LCA does not allow for dimensional aspects of item distribution, and these are very likely to be present. We therefore applied FMMA to our data.
Theoretical considerations are regarded as important in the interpretation of FMMA. The two models of best fit obtained by FMMA both included a provision for variations in overall severity. The model FMM-3/4C, in which variations were permitted within classes, but not between classes, was a slightly better fit, but relied on an implausible assumption incompatible with our initial conceptualisation of paranoia. Thus, on theoretical and empirical grounds, we favoured model FMM-4/4C, which did allow for variation in severity between classes.
In our study, the less frequent items had a content suggestive of a greater disturbance in social perception. Our analyses also support our hypothesis of a non-reflexive relationship: that these less frequent, more severe items were relatively more predictive of other paranoia items. This tallies with the idea that paranoid ideation is continuously distributed, with actual paranoid delusions being placed at the extreme end of the continuum. At a single point in time, the continuum is defined by differences between individuals located at individual positions on the curve. However, people are themselves likely to vary in a way that would place them at different positions on the curve at different times, dependent on changing circumstances. In a sense, they would move along the curve, a speculation now with some support from longitudinal investigation.Reference Kaymaz, Drukker, Lieb, Wittchen, Werbeloff and Weiser7,Reference Werbeloff, Drukker, Dohrenwend, Levav, Yoffe and van32
The continuum model was also supported by the FMMA: although this identifies subcategories of individuals, the rarest class (the only one strongly associated with ideas of persecution) almost invariably had the highest rates of the other features of paranoia. The quasi-normal class had low rates of items forming the mistrust, interpersonal sensitivity, and ideas of reference factors, and showed no endorsement of persecutory ideas. Positioned between these classes were two intermediate classes, loaded particularly towards mistrust and ideas of reference respectively. It is possible that these represent alternative routes into more florid ideas of persecution. In general, our analyses supported the existence both of the subcategories of paranoia and of an underlying dimension. Movement between the categories and along the dimension indicate the processes whereby the more extreme forms of paranoia develop, eventually resulting in diagnosable psychotic disorders.
This investigation, based on a random sample of the general population of Great Britain corroborates our study of paranoia in a student population.Reference Freeman, Garety, Bebbington, Smith, Rollinson and Fowler3 The relative frequency of individual items was similar, and there was a continuous exponential distribution of paranoid thoughts, with similar non-reflexive relationships between less and more frequent items.
Limitations
There is inevitably a degree of inaccuracy in the methods feasible in large surveys, but this is traded off against the sample size required in a study of the structure of paranoia. However, self-report items like those used here correlate both with interviewer assessments (e.g. Inacu et al Reference Iancu, Poreh, Lehman, Shamir and Kotler33) and with experimental investigations (e.g. Freeman et al Reference Freeman, Pugh, Antley, Slater, Bebbington and Gittins34).
Questions in the PSQ apply to experiences within the past year, while the SCID-II asks about an implicit general tendency to think in particular ways. Thus, the instruments are potentially discrepant in relation to the timing of the experiences they tap. This may not be crucial, as the propensity to paranoid thought may operate as a mixture of trait and state attributes. We were unable to take account of the possibility that the paranoid ideation of individual participants was grounded in reality, although the capacity of the characteristics of experience to elicit paranoia is itself likely to occur on a dimension.
The models were tested on a single sample, and require replication.
Implications
If we take the rates of endorsement of paranoid items in our study at face value, they suggest that paranoia is so common as to be almost normal. We are certainly obliged to make decisions to trust or to mistrust on a daily basis. The sheer frequency of paranoid beliefs implies that, to some degree, it can be adaptive in social situations.Reference Lyoo, Youn, Ha, Park and Kwon31 Individuals who are trusting, open and never suspicious of the intentions of others may end up as naive objects of exploitation. When surrounded by strangers, it may be better to remain somewhat wary of their intentions until they are definitely seen to be favourable. However, too great a degree of suspiciousness may obstruct the development of the social relationships necessary for the maintenance of well-being.Reference Penn, Mueser, Tarrier, Gloege, Cather and Serrano35 Thus, paranoia leads to isolation that may foster the retention of unusual ideas by removing the possibility of normalising exposure.Reference White, Bebbington, Pearson, Johnson and Ellis36
Our results have implications for the aetiological study of psychosis.Reference Plomin, Haworth and Davis17 Other continua are almost certainly involved.Reference Kaymaz and van Os5 Evidence encourages the separate consideration of paranoia, grandiosity, hallucinations and thought disorder (e.g. Wigman et al Reference Wigman, Vollebergh, Raaijmakers, Iedema, van Dorsselaer and Ormel37). Our findings also imply that in some people movement along these continua results in the emergence of psychosis.Reference Werbeloff, Drukker, Dohrenwend, Levav, Yoffe and van32 Thus, the role of aetiology is to explain exactly why particular people make this journey at particular times in their lives. In the psychological domain, this implies the concatenation of different psychological attributes, some cognitive, some emotional.Reference Krabbendam, Myin-Germeys, Hanssen, de Graaf, Vollebergh and Bak38,Reference Hanssen, Bak, Bijl, Vollebergh and van Os39 In social terms, adverse early experiences in increasing the propensity to paranoia, may have a tonic effect on people's position on the curve, whereas more recent events may be responsible for more immediate movement along it. The role of appraisal in this process is likely to be crucial,Reference Garety, Kuipers, Fowler, Freeman and Bebbington40-Reference Morrison, French and Wells42 and offers an opportunity for focused psychological treatments, as does the normalising implications of the widespread distribution of paranoid thought, which may reduce self-stigmatisation. Our findings would also encourage the consideration of treatment at an early stage.
Finally, the continuum model of psychosis has complex implications for diagnostic systems. We would agree with Linscott & van OsReference Linscott and van Os4 that taxonomic classifications of schizophrenia, while remaining of heuristic value, create pragmatic divisions that do not map onto corresponding latent discontinuities. However, they argue that the empirically demonstrated continua of experience probably do have an underlying structure. Our results are a corroboration of their position with the additional advantage of being based on specific theoretical considerations.
Acknowledgement
Our co-author, colleague and friend Professor Howard Meltzer died on 17 January 2013.









eLetters
No eLetters have been published for this article.