



Clonal hematopoiesis (CH) is defined as any clonal outgrowth of hematopoietic progenitor cells (Genovese et al., Reference Genovese, Kähler, Handsaker, Lindberg, Rose, Bakhoum, Chambert, Mick, Neale, Fromer, Purcell, Svantesson, Landén, Höglund, Lehmann, Gabriel, Moran, Lander, Sullivan and …McCarroll2014). The prevalence of CH depends on the sensitivity of detection methods, and increases with age (Evans & Walsh, Reference Evans and Walsh2023). Clonal hematopoiesis is associated with an increase in the risk of all-cause mortality, hematological malignancy and nonhematological malignancy, chronic kidney disease, and cardiovascular diseases due to accumulation of somatic mutations. Although risk factors of CH include male sex (Jaiswal et al., Reference Jaiswal, Fontanillas, Flannick, Manning, Grauman, Mar, Lindsley, Mermel, Burtt, Chavez, Higgins, Moltchanov, Kuo, Kluk, Henderson, Kinnunen, Koistinen, Ladenvall, Getz and …Ebert2014), germline mutation (e.g., 8-bp intronic deletion in TERT; Zink et al., Reference Zink, Stacey, Norddahl, Frigge, Magnusson, Jonsdottir, Thorgeirsson, Sigurdsson, Gudjonsson, Gudmundsson, Jonasson, Tryggvadottir, Jonsson, Helgason, Gylfason, Sulem, Rafnar, Thorsteinsdottir, Gudbjartsson and …Stefansson2017) and cigarette smoking (Levin et al., Reference Levin, Nakao, Zekavat, Koyama, Bick, Niroula, Ebert, Damrauer and Natarajan2022), potential causal risk factors for CH are still unclear.
Rheumatoid arthritis (RA) is one of the most common chronic inflammatory and autoimmune diseases with synovial inflammation and hyperplasia of joint tissue (McInnes & Schett, Reference McInnes and Schett2011; Scott et al., Reference Scott, Wolfe and Huizinga2010; Smolen et al., Reference Smolen, Aletaha and McInnes2016). Approximately 0.5–1.0% of the population in Europe (van der Woude & van der Helm-van Mil, Reference van der Woude and van der Helm-van Mil2018) and 0.32–0.36% in Asia (Tong et al., Reference Tong, Xu, Zong, Pan, Teng and Xu2020) are affected by RA, which leads to joint pain, swelling and stiffness (van der Woude & van der Helm-van Mil, Reference van der Woude and van der Helm-van Mil2018). Since RA has multi-organ and mulri-system involvement, the brain, heart, lung, kidney and hematologic system can be invaded by the disease exposure (Scott et al., Reference Scott, Wolfe and Huizinga2010; Smolen et al., Reference Smolen, Aletaha and McInnes2016). Although previous observational studies reported that the RA patients have increased risk for vertebral osteoporotic fractures (Tong et al., Reference Tong, Xu, Zong, Pan, Teng and Xu2020), low bone mineral density (Lee et al., Reference Lee, Park, Park, Kim, Choi, Lee, Kim, Lee, Kim, Lee, Lee and Baek2012), and bone fracture (Xue et al., Reference Xue, Wu, Jiang, Feng, Guo and Zhao2017) due to abnormal inflammatory and autoimmune exposure, whether RA has an impact on CH is still unknown.
Several researchers have found that RA affects the proliferation of hematopoietic progenitor cells in vitro, including myeloid and lymphoid cells (Colmegna et al., Reference Colmegna, Pryshchep, Oishi, Goronzy and Weyand2012), which is the one of main characteristics of CH. Meanwhile, CH with a typical mutation profile occurs in RA (e.g., DNMT3A and TET2 mutations; Savola et al., Reference Savola, Lundgren, Keränen, Almusa, Ellonen, Leirisalo-Repo, Kelkka and Mustjoki2018), implying that long systemic inflammation could increase the rate of CH by accumulation of somatic mutations. However, only one previous observational study found that the prevalence of CH was not markedly increased in RA patients (Savola et al., Reference Savola, Lundgren, Keränen, Almusa, Ellonen, Leirisalo-Repo, Kelkka and Mustjoki2018) in a very small cohort (N =59). Thus far, it is unknown whether RA is causally associated with CH.
In the present study, we used a two-sample Mendelian randomization (MR) analysis to evaluate the causal association of RA on CH, based on a genomewide association study (GWAS), which selected single-nucleotide polymorphisms (SNPs) as instrumental variables (IVs) to evaluate the potential causal effects of exposures on outcomes. Our study illustrated the link between RA and CH, highlighting potential mechanisms in genetics of the RA-CH relationship.
Materials and Methods
Study Design
In this study, we utilized a two-sample MR to evaluate the causal association between RA and CH using data based on publicly available GWAS. The genetic variants (SNPs) were used as IVs to estimate potential causal effects of RA on CH. To conduct a valid MR analyses, three important hypotheses must be confirmed during the whole process (Lawlor et al., Reference Lawlor, Harbord, Sterne, Timpson and Davey Smith2008). In brief, (a) the IVs are strongly associated with RA; (b) RA and CH are independent of any known confounders; (c) the IVs affected CH only through RA. There was no participant overlap between the exposure and outcome datasets.
Data Source and IVs Selection
The summary-level statistics for RA were currently derived from the published studies (Eyre et al., Reference Eyre, Bowes, Diogo, Lee, Barton, Martin, Zhernakova, Stahl, Viatte, McAllister, Amos, Padyukov, Toes, Huizinga, Wijmenga, Trynka, Franke, Westra, Alfredsson and …Worthington2012), which involved 13,838 cases and 33,742 controls of European participants. Summary statistics for CH were obtained from a previously published GWAS study (Kar et al., Reference Kar, Quiros, Gu, Jiang, Mitchell, Langdon, Iyer, Barcena, Vijayabaskar, Fabre, Carter, Petrovski, Burgess and Vassiliou2022) that contained 10,203 cases and 173,918 controls from Europe (https://zenodo.org/records/5893861). The SNPs were strongly associated with RA (p < 5e–8) with low linkage disequilibrium (LD, R 2 < .001, clumping distance = 10000 kb), and large F values (F statistics > 10). We then manually searched the PhenoScanner database (http://www.phenoscanner.medschl.cam.ac.uk/phenoscanner) to exclude variants that were associated with confounders or outcomes. Finally, the SNPs with relative common frequency in population (minor allele frequency > 0.01) were selected as IVs.
MR Analysis and Sensitivity Analysis
The MR analysis was conducted in R 4.2.0 using the TwoSampleMR v0.5.7 (https://mrcieu.github.io/TwoSampleMR/news/index.html). Orienting the causal relationship was determined by Steiger test. Five different methods were used to assess the causal effects of CH outcomes, including weighted mode, simple mode, weighted median, Mendelian randomization-egger (MR-Egger) and inverse-variance weighted (IVW). The MR-Egger method allows for horizontal pleiotropy of instrumental SNPs, but the method is not capable of distinguishing between causal effects and pleiotropy (Burgess & Thompson, Reference Burgess and Thompson2017), and is easily affected by ‘weak instrument bias’ (Pierce & Burgess, Reference Pierce and Burgess2013). Simple mode and weighted mode methods were set as a complementary MR analysis strategy. The IVW method combines the estimates of each SNP and provides a consistent estimate of the causal effect, which is the most reliable method when there is no horizontal pleiotropy of the instrumental SNPs (Bae & Lee, Reference Bae and Lee2018; Bowden et al., Reference Bowden, Davey Smith, Haycock and Burgess2016). Additionally, MR pleiotropy residual sum and outlier (MR-PRESSO) was conducted to exclude any potential pleiotropy (https://github.com/rondolab/MR-PRESSO), and p < .05 was regarded as statistical significance. Meanwhile, the MR-Egger and IVW methods were conducted to evaluate the heterogeneity quantified using Cochran’s Q-test. The horizontal pleiotropy was analyzed by the MR-Egger method. In addition, the leave-one-out analysis was used to verify whether outliers existed that affected the result.
Results
IVs for RA
A total of 2386 SNPs were found significantly associated with RA in European population (p < 5 × 108). After clumped analysis, funnel plots analysis and calculation of F statistic, 15 SNPs were selected as IVs to evaluate the causal relationship between RA and CH; the detailed information of IVs is shown in Table 1. In addition, no significant association was found between these SNPs and CH or related confounders according to the Phenoscanner database (Table S1).
Table 1. Genetic variants used as instruments for rheumatoid arthritis.
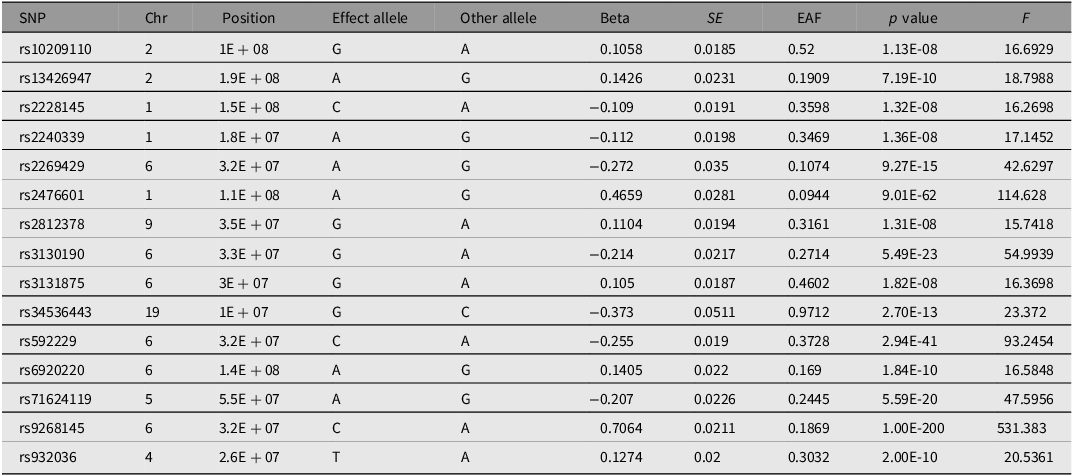
Note: SNP, single nucleotide polymorphism; Chr, chromosome; EAF, effect allele frequency.
MR Analysis
By performing IVW analysis (Table 2, Figure 1), we found causality of RA with CH, and RA was associated with increased risk of CH as indicated by IVW (OR = 1.002311673, 95% CI [1.000110757, 1.004517433], p = .039706) and weighted median (OR = 1.002311673, 95% CI [1.000110757, 1.004517433], p = .039518447) methods. As for the MR-Egger regression (MR-Egger, OR = 1.001021956, 95% CI [0.99816608, 1.003886003], p = .0495823), simple mode (OR = 1.002411974, 95% CI [0.997456772, 1.007391792], p = .356839342) and weighted mode (OR = 1.002630923, 95% CI [1.000336062, 1.004931049], p = .041255472), since the beta value of all two major MR approaches (IVW and weighted median) were ≥ 0 and the OR value was ≥ 1, this suggests a positive causal connection between RA and CH. In addition, we found that the assumption that RA causes CH was valid, as indicated by Steiger p < .0001, using a Steiger test (Table S2).
Table 2. Mendelian randomization estimates of rheumatoid arthritis associated with the risk of clonal hematopoiesis

Note: MR, Mendelian randomization; IVs, instrumental variables. Bold type indicates significance.
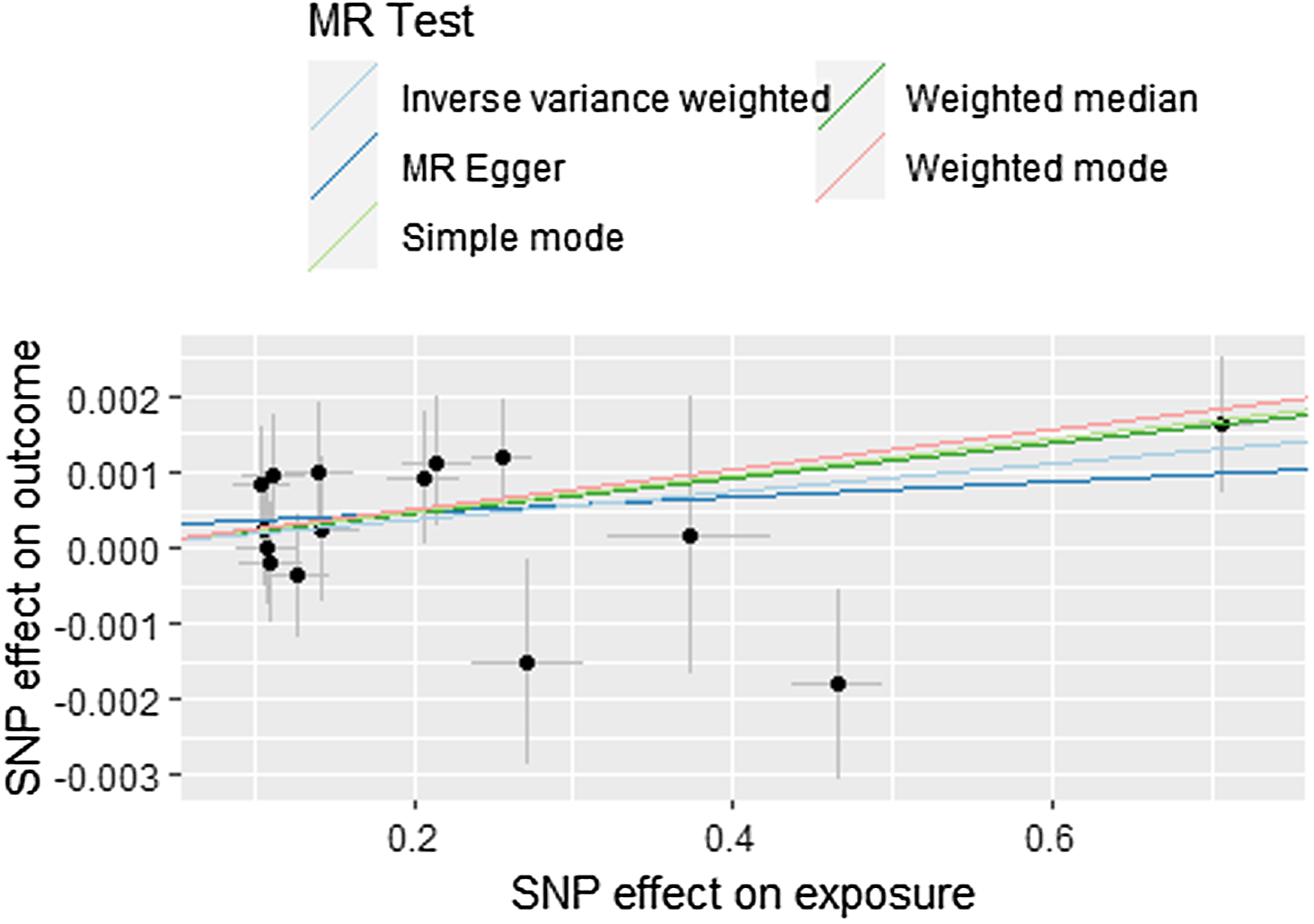
Figure 1. The scatterplot depicts the causal relationship between rheumatoid arthritis and clonal hematopoiesis.
Note: MR, Mendelian randomization; SNP, single nucleotide polymorphism.
Sensitivity Analysis
MR pleiotropy residual sum and outlier (MR-PRESSO) analysis indicated no pleiotropy and outlier SNP in this study (p = .5700). In addition, the intercepts of RA on CH was 0.0002625363 (p = .4892), indicating that IV had no horizontal pleiotropic effect (Table S3 and Figure 1). Meanwhile, no obvious heterogeneity was observed according to Q values based on MR-Egger (p = .5323473) and IVW (p = .5702701) tests (Table S3). The leave-one-out (Figure 2) and funnel plots (Figure 3) demonstrated that there were no obvious or potential outlier IVs, strengthening the robustness of our results, which made our MR results more convincing.
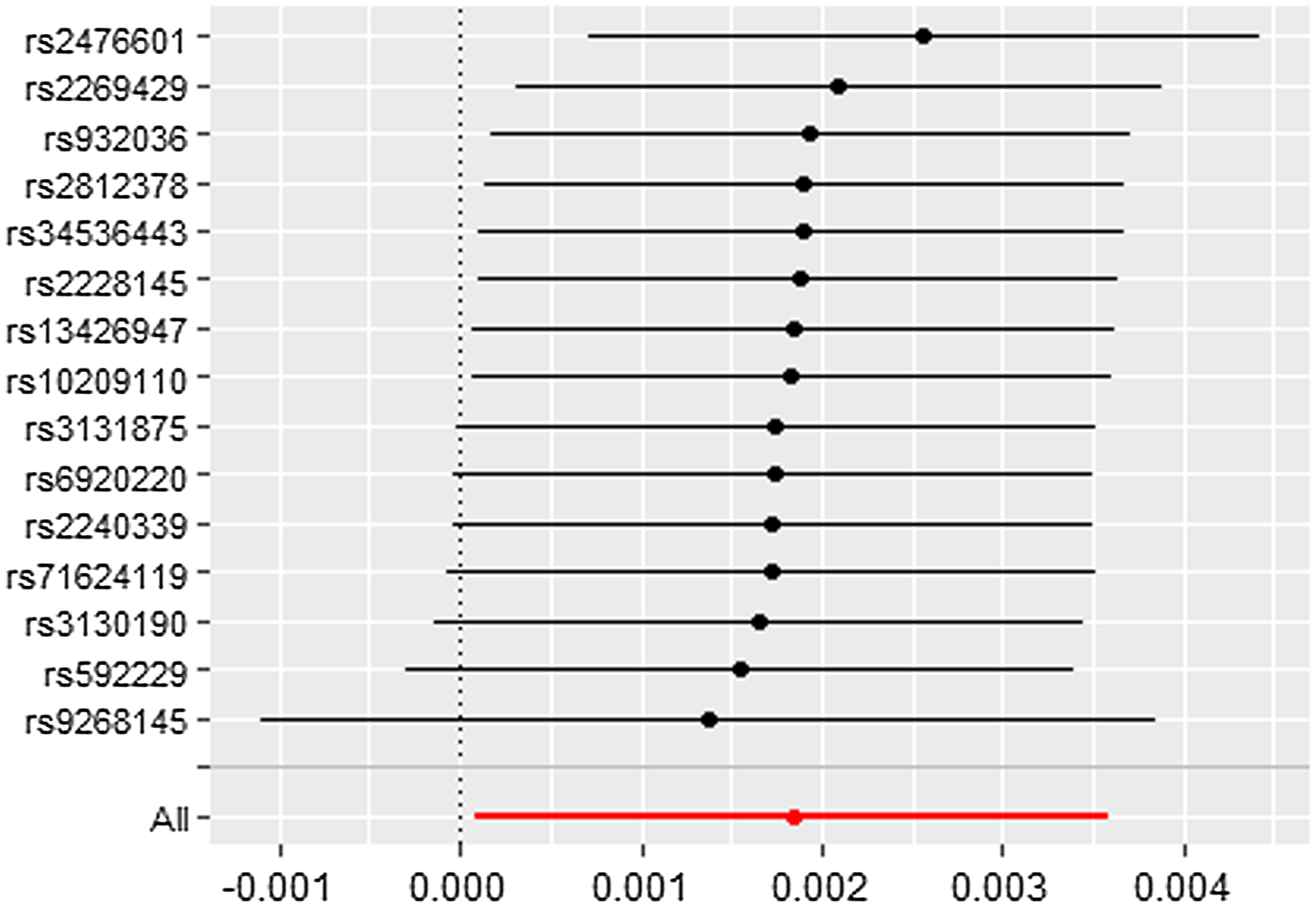
Figure 2. Leave-one-out analysis. Each dot in the forest plot represents the Mendelian randomization estimate (using inverse-variance weighted) excluding that particular instrumental variable.
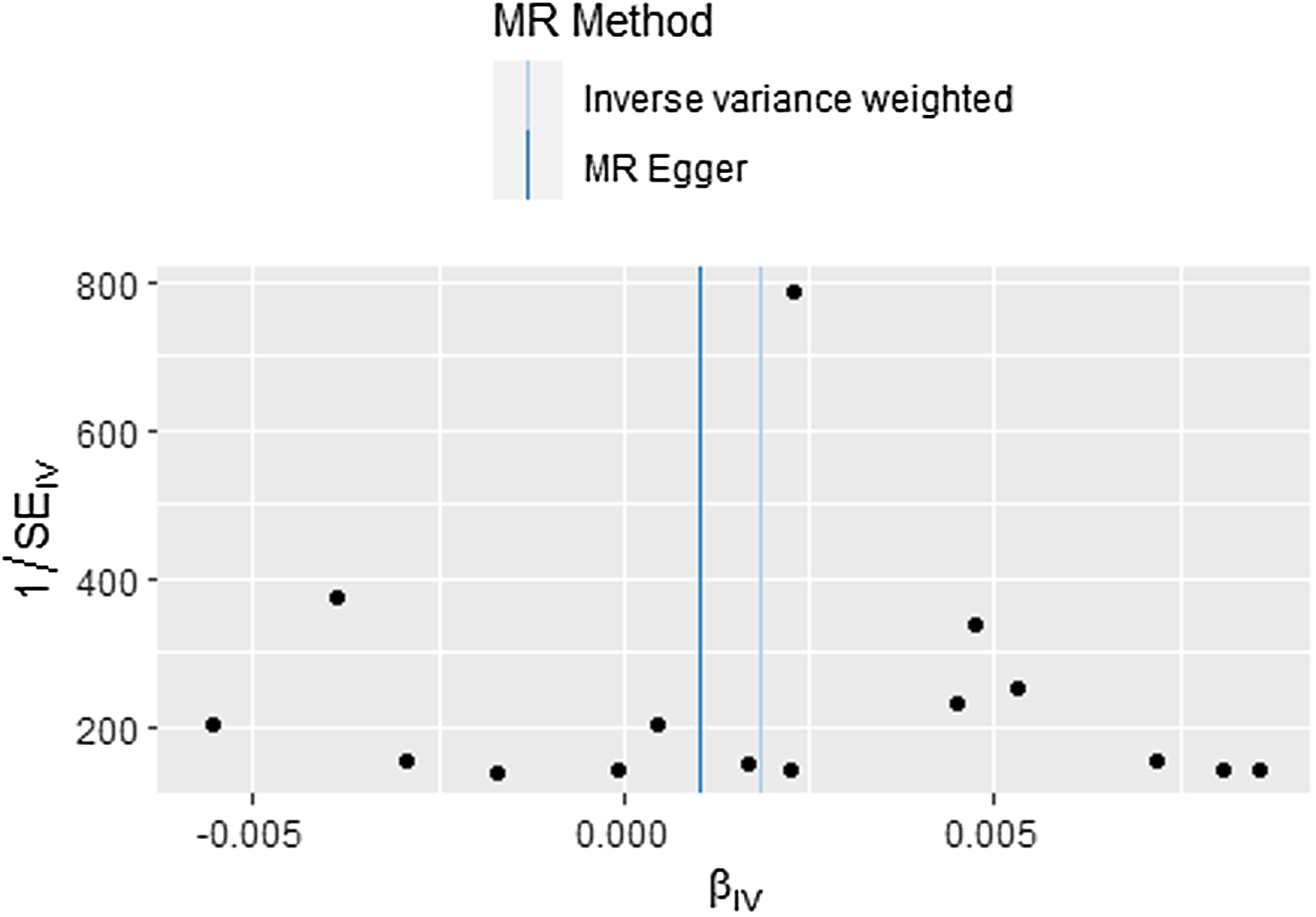
Figure 3. Funnel plots of individual variant effects for the instrumental variables.
Note: MR, Mendelian randomization.
Discussion
This MR study aimed to investigate the causal effect of RA on CH by reanalysis GWAS summary data in European ancestry. Consistent with our hypothesis, a positive causality between RA and CH risk was found in this study (IVW, OR = 1.002311673, 95% CI [1.000110757, 1.004517433], p = .039706); Weighted median, OR = 1.002311673, 95% CI = [1.000110757, 1.004517433], p = .039518447). In the sensitivity analysis, the MR results were robust and reliable. These findings suggested that RA exposure increases the risk of CH.
Recently, MR has become a useful tool to assess the causal relationship between exposure and outcome via genetic markers. Since RA has multi-organ and multi-system involvement, several studies have revealed the causal association between RA and pre-eclampsia (Zhang et al., Reference Zhang, Hu, Guo, Song, Yang, Yang, Ou, Liu and Zhang2022), hepatocellular carcinoma (Zhang et al., Reference Zhang, Zhang, He, Ge, Huo and Qiao2023), glaucoma (Meng et al., Reference Meng, Tan, Su, Li and Chen2023) and cardio-cerebrovascular disease (Qiu et al., Reference Qiu, Li, Jin, Lu and Hu2021), implying that RA has a broad effect on various pathophysiology progresses. In this study, we found a causal association between RA and CH via a robust MR analysis, and that the exposure of RA increases the risk of CH. However, Savola and colleagues reported that RA had a minimum effect on the risk of CH in only 59 RA patients based on Illumina’s TruSeq Custom Amplicon technology, which only covered 34 tumor suppressor genes and/or mutational hotspots (Savola et al., Reference Savola, Lundgren, Keränen, Almusa, Ellonen, Leirisalo-Repo, Kelkka and Mustjoki2018). Meanwhile, the diagnosis of CH varied according to the approach and sensitivity of detestation (Evans & Walsh, Reference Evans and Walsh2023). For example, initial studies found the frequency of CH was 10% of individuals over the age of 70 in their white blood cells using whole exome sequencing (Jaiswal et al., Reference Jaiswal, Fontanillas, Flannick, Manning, Grauman, Mar, Lindsley, Mermel, Burtt, Chavez, Higgins, Moltchanov, Kuo, Kluk, Henderson, Kinnunen, Koistinen, Ladenvall, Getz and …Ebert2014); recent studies with deeper sequencing technologies found that CH is ubiquitous by middle age or earlier (Watson et al., Reference Watson, Papula, Poon, Wong, Young, Druley, Fisher and Blundell2020; Young et al., Reference Young, Challen, Birmann and Druley2016). Moreover, genetic drift and fitness shaping the genetic diversity were not detected in the observational study, which are the main characteristics of CH (Watson et al., Reference Watson, Papula, Poon, Wong, Young, Druley, Fisher and Blundell2020). More importantly, Savola and colleagues (2018) also found that CH with a typical mutation profile occurs in RA patients, implying that the reactions induced by RA might have an impact on the development of CH. Taken together, further studies with large cohorts and deeper sequencing technologies will be invaluable in the future.
Previous studies demonstrated that chronic inflammation and immune activation may cause mutagenesis via DNA damage by a series of immune-inflammation reactions (Nakad & Schumacher, Reference Nakad and Schumacher2016). Autoimmune response and chronic inflammation are the main features of RA (Smolen et al., Reference Smolen, Aletaha and McInnes2016), which can lead to abundant mutation accumulation in patients with RA. The cellular composition in RA includes innate immune cells and adaptive immune cells involved with a matrix regulatory, aggressive inflammatory and invasive phenotype, which fails to detect DNA lesions, and thus leads to DNA damage and mutation accumulations (Shao, Reference Shao2018; Smolen et al., Reference Smolen, Aletaha, Koeller, Weisman and Emery2007). Meanwhile, outgrowths of mutated blood cells, including two enzymes involved in DNA methylation (DNMT3A and TET2) and a chromatin regulator (ASXL1) as well as cellular growth signaling (GNAS, GNB1, JAK2, CBL) and the DNA damage response (PPM1D, TP53), are the main drivers mutation of CH (Jaiswal & Ebert, Reference Jaiswal and Ebert2019). In addition, the mechanism and function of these mutations in CH remains unknown. Collectively, the exposure of RA for years may cause accumulation of mutation induced by chronic inflammation that leads to development of CH, and therefore more studies to consider this should be conducted in the future.
This study had some limitations. First, only 15 SNPs were selected as IVs in this study with a relatively limited effect on RA as indicated by R 2 (range [%]: 0.05286–15.1647). Therefore, other important factors besides RA that can affect the risk of CH should not be ignored in the next studies, such as smoking (Levin et al., Reference Levin, Nakao, Zekavat, Koyama, Bick, Niroula, Ebert, Damrauer and Natarajan2022). Second, the MR results only involved European ancestry populations in this study, and whether a casual association exists between RA on CH needs to be clarified by further investigations. Third, previous studies reported that male and elderly individuals have an increased risk of suffering CH, but the published summary GWAS data did not provide this information to adjust the bias. Fourth, the SNPs used for analysis may be correlated with other traits due to genetic polymorphisms and thus generate confounding bias, which may affect causal inference. Fifth, the strength of the IV depends on the sample size of the GWAS, and a larger scale GWAS is required to determine more genetic variation for MR. Finally, our study found the risk of CH increased under the exposure of RA for years, rather than for a specific time in life. Thus, additional explorations of the effect sizes between the specific time of RA and CH risks are needed. In addition, RA is a binary exposure (Ding et al., Reference Ding, Jiang, Zhangwang, Li and Lei2024), which might generate biased estimates and yield a spurious causal estimate (Burgess & Labrecque, Reference Burgess and Labrecque2018) between RA and CH. Therefore, the exclusion-restriction assumption was done in our study.
Conclusion
In conclusion, these results support a potentially causal relationship between RA and CH, and the exposure of RA increases the risks of CH. Our findings highlight the importance of chronic inflammation and immune activation induced RA on the risks of CH, and that early intervention for RA patients might reduce the CH risks in RA patients. Moreover, our study provides clues for prediction of risk factors and potential mechanisms of CH.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/thg.2024.24.
Financial support
This study was supported by Guangdong Basic and Applied Basic Research Foundation (2022A1515012549, 2023A1515012667 and 2022A1515012297), and Research Project of Guangdong Provincial Bureau of Traditional Chinese Medicine (20211161).
Competing interests
None.







