


It is well known that the growth patterns of twins and triplets during pregnancy differ from those of singletons. Studies on the birth weight of twins or triplets have been conducted in many countries (Arbuckle et al., Reference Arbuckle, Wilkins and Sherman1993; Buckler & Green Reference Buckler and Green1994; Glinianaia et al., Reference Glinianaia, Skjaerven and Magnus2000; Kato, Reference Kato2004; Min et al., Reference Min, Luke, Gillespie, Min, Newman, Mauidin, Witter, Salman and O'Sullivan2000; Min et al., Reference Min, Luke, Misiunas, Nugent, de Ven, Martin, Gonzalez-Quintero, Eardley, Witter, Mauldin and Newman2004; Orlebeke et al., Reference Orlebeke, Boomsma and Eriksson1993). Triplets are typically born prematurely, and 40–50% of them weigh less than 1,500 g at birth (Kato, Reference Kato2004; Ziadech, Reference Ziadech2000). In the meanwhile, a number of studies on the postnatal growth of twins have been conducted (Akerman & Fischbein, Reference Akerman and Fischbein1992; Alfieri et al., Reference Alfieri, Gatti and Alfieri1987; Luke et al., Reference Luke, Leurgans, Keith and Keith1995; Buckler & Green, Reference Buckler and Green2004; Ooki & Yokoyama, Reference Ooki and Yokoyama2004; Silventoinen et al., Reference Silventoinen, Bartels, Posthuma, Burk, Willemsen, Beijsterveldt and Boomsma2007; Wilson, Reference Wilson1976; Wilson, Reference Wilson1979). The weight deficit of twins is greatest at birth but decreases dramatically during the first year of life because of rapid catch-up growth, reaching as little as approximately 2% for weight, by 4 years of age (Buckler & Green, Reference Buckler and Green1994; Ooki & Yokoyama, Reference Ooki and Yokoyama2004). However, there are few previous studies on the postnatal growth of triplets in the world.
The special features of multiple pregnancies have potential effects also on the further life of twins and tripletons since it is indicated that low birth weight is a risk factor for adverse health and neurodevelopmental outcomes (Arnoudse-Moens et al., Reference Arnoudse-Moens, Weisglas-Kuperus, van Goudoever and Oosterlaan2009; Bhutta et al., Reference Bhutta, Clevels, Casey, Cradok and Anand2002; Wadhawan et al., Reference Wadhawan, Oh, Vohr, Wrage, Das, Bell, Laptook, Shankaran, Stool, Walsh and Higgins2011). In addition, children who demonstrate catch-up growth are found to be at greatest risk for alteration in metabolism, hormonal output, and distribution of cardiac output, which result in obesity, diabetes, and cardiovascular disease in middle age (Cianfrani et al., Reference Cianfrani, Germani and Branca1999; Fall, Reference Fall, Osmond, Barker, Clark, Hales, Stirling and Meade1995; Forsen et al., Reference Forsen, Eriksson, Tomilehto, Osmond and Barker1999; Law, Reference Law2001). Studies of the long-term growth of low birth weight infants including triplets, the majority of whom experience intrauterine and/or neonatal growth failure, may yield important information in this regard (Bukowski et al., Reference Bukowski, Gahn, Denning and Saade2001; Ehrenkranz et al., Reference Ehrenkranz, Younes, Lemons, Fanaroff, Donovan, Wright, Katsikiotis, Tyson, Oh, Shankaran, Bauer, Korones, Stoll, Stevenson and Papile1999; Hack, Reference Hack, Merkatz, Gordon, Jones and Fanaroff1982).
Physical growth of triplets was found to be behind singletons even in mid-childhood in spite of the rapid catch-up growth during the first year of life (Luke et al., Reference Luke, Brown, Hediger, Misiunas and Anderson2006; Yokoyama et al., Reference Yokoyama, Sugimoto and Ooki2008; Yokoyama et al., Reference Yokoyama, Sugimoto, Kaprio and Silventoinen2009). However, there have been no reports of weight growth of triplets after 6 years of age. The purpose of this study was to analyze the characteristics of weight growth in Japanese triplets until 12 years of age by extending the follow-up time of our prior study (Yokoyama et al., Reference Yokoyama, Sugimoto and Ooki2008).
Participants and Methods
The participants of this study were recruited from the Osaka City University Higher Order Multiple Births Registry (Yokoyama, Reference Yokoyama2002; Yokoyama et al., Reference Yokoyama, Shimizu and Hayakawa1995; Yokoyama et al., Reference Yokoyama, Sugimoto and Ooki2005), which consisted of 578 mothers with triplets who were born between 1978 and 2006. Mothers and their triplet children were enrolled also from several other sources, such as various Japanese Mother's Organizations for Higher Order Multiple Births and referrals from public health nurses.
Data were collected through a mailed questionnaire sent to the mothers asking for information available in medical records. For these births, data on triplets’ weight growth, gestational age, sex, parity, and maternal age at delivery were obtained from the records in the Maternal and Child Health Handbooks. This handbook was established by the Maternal and Child Health Law in Japan and is provided to the expecting mother by the authorities after the report of pregnancy. The purpose of this handbook is the maintenance of maternal and child health, and it includes information on health check-ups during pregnancy, the condition of the newborn, the progress of infant growth, and periodic medical check-ups for the infant and vaccinations recorded by obstetricians or pediatricians. In addition, information on maternal weight/height and infertility treatment was obtained. We used body mass index (BMI) categories according to Japan Society for the Study of Obesity based on the definitions given by WHO (World Health Organization) BMI of less than 18.5 kg/m2 as underweight; BMI of 18.5–24.9 kg/m2 as normal weight; and BMI of more than 25 kg/m2 as overweight or obese.
In Japan, the health check-up system after birth differs according to life stage. Until 6 years of age, children participate in health check-ups administered by the Ministry of Health, Labor and Welfare based on age, which is counted as actual weeks, months, or years after birth. The weight data of children based on health check-ups are routinely recorded in the Handbook. After 6 years of age, Japanese children receive health check-ups administered by the Ministry of Education, Culture, Sports, Science and Technology under the School Health Law. The weight measures from these school-based health check-ups are routinely recorded in the school records and made available to each family. Mothers have access to the school records from every grade and can check them directly. Mothers participating in this study were advised to refer to these records when completing the questionnaire. The weight growth data were assigned to the appropriate age groups on the basis of time (in days) since birth, which was calculated as the date at the check-up minus the child's birthday.
The response rate was 67.0%. We had 1,164 triplet children having information on growth, but 36 triplets with unknown sex were excluded from the analyses. Ultimately, the subjects of this study were 376 mothers and their 1,128 triplet children. The mothers gave written informed consent to participate in the present study.
The significance of differences between mean values of gestational age was tested using analysis of variance ANOVA and multiple comparison posttest (Tukey pairwise comparisons) where the comparison was between the three groups of maternal BMI. The means and standard deviations of weight from birth to 12 years of age for triplets were calculated according to gestational age, very low birth weight, sex, parity, birth order, maternal age at triplet delivery, maternal height, and maternal BMI. The significance of differences between mean values of weight was tested using mix-model ANOVA where the comparison was between two or more groups in order to adjust for familial clustering (i.e., sets of triplets) as a random effect factor.
The statistical significance of regression coefficients of the covariates (factors), where assessed from the fixed effects and these were adjusted for familial clustering (i.e., sets of triplets) by introducing random effect in the linear mixed model. The associations of the factors with weight at 6, 8, 10, or 12 years of age were explored by the linear mixed-effects model. The factors associated with weight at 6, 8, 10, or 12 years of age were explored by the linear mixed-effects multiple regression analysis. This was done in order to adjust for familial clustering as a random effect factor. We fitted separate models for body weight at 6, 8, 10, and 12 years of age as dependent variables. The independent variables were very low birth weight, sex, birth order of triplets, gestational age, maternal BMI, or maternal height.
The selected percentiles (10th, 25th, 50th, 75th, and 90th) of weight were calculated according to age and sex. Smoothing of growth curves was performed by cubic polynomial functions. The weight deficit of the triplets was calculated as the percentage difference between the value of the general population and that of the triplets divided by the value of the general population. The weight deficits were calculated using mean values of the growth standards presented by the Ministry of Health, Labor and Welfare (Kato et al., Reference Kato, Okuno and Takaishi2001) and the Ministry of Education, Culture, Sports, Science and Technology (2009). The PASW statistical package, version 19.0 for Windows (2011) was used for the statistical analysis.
Results
Table 1 presents the number of participants according to sex and age at each age when weight data were available. Table 2 summarizes the characteristics of the participants. Gestational age at birth significantly differed by maternal BMI and was 31.8 ± 2.98 weeks in women whose BMI is less than 18.5 kg/m2, 33.4 ± 2.52 weeks in women whose BMI is 18.5–24.9 kg/m2, and 33.2 ± 3.23 weeks in women whose BMI is more than 25.0 kg/m2. Gestational age of women whose BMI is less than 18.5 kg/m2 was significantly shorter than that of women whose BMI is higher.
TABLE 1 Number of Triplet Individuals With Weight Data at Different Ages by Sex
Individuals had a varying number of weight measures.
TABLE 2 Major Characteristics of the Triplet Individuals
The 10th, 25th, 50th, 75th, and 90th percentiles of weight and the mean weight from birth to 12 years of age are presented in Figure 1. The range of 10th and 90th percentile weight at 12 years of age was from 30.4 kg to 52.8 kg in boys and 30.5 kg to 45.3 kg in girls.
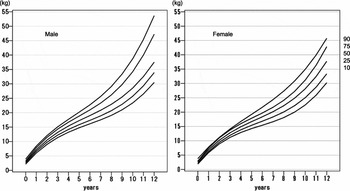
FIGURE 1 Body Weight of Triplets According to Age Percentiles From Birth to 12 Years of Age.
Table 3 shows the mean weight at birth and at 6, 8, 10, and 12 years of age analyzed according to gestational age, very low birth weight, sex, parity, birth order, maternal age at triplet delivery, maternal height, and maternal BMI. Females and triplets whose gestational age was earlier had a lower birth weight and lower weight at 6, 8, and 10 years of age; these differences were statistically significant, except for the sex difference for weight at 10 years of age. Very low birth weight infants had a lower birth weight and lower weight at 6, 8, and 10 years of age. Third-born neonates had a lower birth weight and lower weight at 6 years of age. Triplets born to shorter mothers had a lower weight at 6 years of age than triplet children born to taller mothers. Triplets born to women whose BMI is lower had a lower birth weight and lower weight at 12 years of age than triplet children born to women whose BMI is higher.
TABLE 3 Descriptive Statistics of Birth Weight and Weight at 6, 8, 10, and 12 Years of Age According Among Japanese Triplets and Comparisons Between Factors using ANOVA
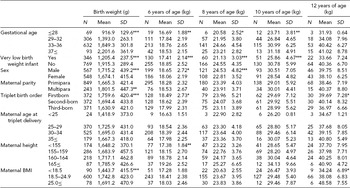
SD = standard deviation. All variables included in the model, *p < .05, **p < .01, ***p < .001.
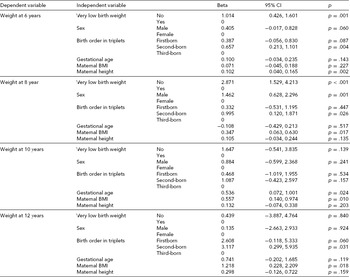
Table 4 shows the results of linear mixed effects multiple regression analysis of weight at 6, 8, 10, or 12 years of age. We also present regression coefficients and p-values for each covariate. Very low birth weight has the strongest contribution on weight of triplets from 6 to 8 years of age, but also birth order affected weight at 6, 8, and 12 years of age. Sex affected weight at 8 years of age. Maternal height affected weight at 6 years of age, and maternal BMI affected weight at 8, 10, and 12 years of age.
TABLE 4 Result of Linear Mixed Effects Multiple Regression Analysis of Factors Associated With Body Weight at Ages 6, 8, 10, and 12 Years
The weight deficit of the triplets was more than 40% at birth relative to the growth standards of the general population (male, –1.32 kg; female, –1.28 kg). The deficit decreased rapidly within the first year of age, but fluctuated between 10% and 17% from 6 until 12 years of age (male, –4.75 kg; female, –6.00 kg) (Table 5).
TABLE 5 Size Deficit of Triplets for Mean Weight Compared With the General Population From Birth to 12 Years of Age
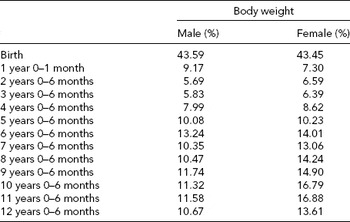
The weight deficit of the triplets was calculated as the percentage difference between the mean value of the general population and the mean of the triplets.
Discussion
In the present study, the weight deficit of the triplets compared to the general population fluctuated between 10% and 17% for weight from 6 to 12 years of age. Moreover, at 12 years of age, the difference of weight between the general female population and female triplets was approximately –6 kg, whereas the difference of weight between the general male population and male triplets was approximately –4 kg. These results are similar to that reported by Powls et al. (Reference Powls, Botting, Cooke, Pilling and Marlow1996) who found that very low birth weight children were significantly lighter than their normal birth weight peers at 12 years of age, with a mean deficit of 2.5 kg. In addition, Hack et al. (Reference Hack, Schluchter, Catar, Rahman, Cuttler and Borawski2003) indicated that catch-up growth in weight occurred between 8 and 20 years among very low birth weight females but not among very low birth weight males who remained significantly smaller than their controls at 20 years of age. Further follow-up is needed to investigate whether triplets achieve normal weight later in life.
Compared with the general population of Japan, the weight deficit of Japanese twins is greatest at birth but decreased dramatically in the first 6–12 months, reaching as little as approximately 2%, around 1 kg for weight, by 6 years of age (Ooki & Yokoyama, Reference Ooki and Yokoyama2004). These trends were consistent with those reported by Buckler and Green (Reference Buckler and Green1994). Meanwhile, the weight deficit of the triplets compared to the general population was greatest at birth: more than 40%. These deficits decreased within the first year of life, but were found to fluctuate between 4% and 9% for weight until 6 years of age (Yokoyama et al., Reference Yokoyama, Sugimoto and Ooki2008; Yokoyama et al., Reference Yokoyama, Sugimoto, Pitkäniemi, Kaprio and Silventoinen2009). The difference of weight between the general population and triplets was approximately 1.8 kg at 6 years of age.
Meanwhile, when adjusting for gestational age and other confounding factors, very low birth weight had the strongest contribution to body weight at 6 and 8 years of age. It is indicated that deficient growth in twins between the age of 2 and 9 years was most evident in those light at birth (Buckler & Green, Reference Buckler and Green2008). Moreover, Powls et al. (Reference Powls, Botting, Cooke, Pilling and Marlow1996) indicated that very low birth weight children had a higher risk of lower weight later in life and this difference was more pronounced in girls. It is probable that very low birth weight affects growth of weight in triplets. Infants with very low birth weight may need careful and extensive longitudinal follow-up.
Sex was a significant factor affecting weight at 8 years of age. Male triplets were heavier than females. This result is in accordance with previous reports on twins at birth (Kato, Reference Kato2004; Ooki & Yokoyama, Reference Ooki and Yokoyama2004) and singletons (Britton et al, Reference Britton, Britton, Jennett, Gaines and Daily1993). The effects of parity and maternal age at triplet delivery were very small and mostly disappeared at early age. In the present study, lasting effects of gestational periods and birth weight on body weight until 10 years of age were observed. However, the growth standards of the general population did not correct the effects of gestational age and birth weight to reflect the actual condition of physical growth. The present data should be treated in the same way in order to estimate the difference between the general population and triplets. Therefore in the present study, the growth charts for the triplets were differentiated only according to sex.
In height growth of triplets, maternal height was found to have significant effect not only on birth length but also on height during childhood (Yokoyama et al., Reference Yokoyama, Sugimoto, Pitkäniemi, Kaprio and Silventoinen2011). However, our results showed that maternal height affected weight only at 6 years of age and after that the influence disappeared. On the other hand, maternal BMI was found to be a significant factor affecting the weight of triplets from 8 to 12 years of age. Parental obesity has been identified as one of the strongest risk factors for childhood obesity in singletons (Bundered et al., Reference Bundered, Kitchner and Buchan2001; Burke et al., Reference Burke, Bellin and Dunbar2001; James et al., Reference James, Leach, Kalamara and Shayeghi2001; Reilly & Dorosty, Reference Reilly and Dorosty1999), and childhood obesity and longitudinal changes in childhood weight have a major heritable component (Silventoinen et al., Reference Silventoinen and Kaprio2009; Silventoinen et al., Reference Silventoinen, Rokholm, Kaprio and Sørensen2010). In addition, it is indicated that parental leanness confers significant protection against the development of overweight in children (Semmler et al., Reference Semmler, Ashcroft, van Jaarsveld, Carnell and Wardle2009). These results suggest that maternal physique has a significant effect not only on weight in singletons during childhood but also on weight of triplets, probably reflecting the role of genetic factors masked at the early life by the special features of tripleton pregnancies but becoming visible at the later life.
Regarding other factors associated with weight of triplets, we found a small but persistent birth order effect: the third-born triplet was lighter than the second-born or the firstborn triplet. Previous studies in twins have reported similar results at birth (Buckler & Green, Reference Buckler and Green1994; Glinianaia et al., Reference Glinianaia, Skjaerven and Magnus2000) and from 3 to 12 years of age (Silventoinen et al., Reference Silventoinen, Bartels, Posthuma, Burk, Willemsen, Beijsterveldt and Boomsma2007). Moreover, Lamb et al. (Reference Lamb, Middeldorp, van Beijsterveldt, Vink, Haak and Boomsma2011) reported that the third-born trizygotic triplets were lighter than the second-born or the firstborn trizygotic children. The background of this effect needs more detailed research, but in twins, the firstborn (and heavier) twin was found to have a heavier placenta and a more optimal cord insertion (Gielen et al., Reference Gielen, Lindsey, Derom, Loos, Derom, Nijhuis and Vlietinck2007). Possibly triplets higher in birth order are more optimally positioned with respect to nutrients intake. The persistence of this birth order effect suggests that prenatal factors can have long-lasting effects on body weight.
A limitation of the present study was that these data were semilongitudinal. Specifically, data on the same individual were used according to the recorded times. Some of our participants provided most of longitudinal data. On the other hand, others provided data from birth to 6 years of age. Additionally, the number of participants in each age group varied considerably as some children were younger than 12 years at the time of the survey. Consequently, the range of measurements in each group becomes small, especially at 12 years of age. However, since the mothers reported the growth of their children retrospectively based on records, there is no age-related dropout in our data. Data on zygosity, maternal smoking, previous obstetric outcome, and maternal weight gain during pregnancy are also lacking in this study, and it has been suggested that these factors are associated with weight growth (Lamb et al., Reference Lamb, Middeldorp, van Beijsterveldt, Vink, Haak and Boomsma2011; Luke et al., Reference Luke, Nugent, van de Ven, Martin, O'sullivan, Eardley, Witter, Mauldin and Newman2002; Ooki & Yokoyama, Reference Ooki and Yokoyama2003; Vogazianos et al., Reference Vogazianos, Fiala and Vogazianos2005).
In conclusion, triplets are lighter than singletons and the weight deficit of the triplets compared to the general population of Japan remained between 10% and 17% from 6 to 12 years of age. Very low birth weight had the strongest contribution to body weight until 8 years of age. After 8 years of age, maternal BMI was found to be a significant factor affecting the weight of triplets until 12 years of age. Further follow-up of the triplets should reveal whether their growth catches up with singletons before adulthood.
Acknowledgments
The authors would like to gratefully acknowledge the help of Kenka Lee in the data analysis. This research was supported by Ministry of Education, Science, Sports and Culture, Grant-in-Aid for Scientific Research (B), 2008–2012. The Academy of Finland Centre of Excellence in Complex Disease Genetics supported the participation of JK, KS, and JP.






