


The role of nutrients, foods and food groups in the causation of many chronic diseases has been extensively studied, and several foods and nutrients with beneficial or adverse effects have been identifiedReference Riboli and Norat1, Reference Willett2. Fewer studies have focused on whole diets or dietary patterns, which may also play an important role in the aetiology of many chronic diseasesReference Hu3–Reference Newby, Muller, Hallfrisch, Andres and Tuker5. An important reason for this paucity of evidence is the difficulty in assessing or even defining a dietary pattern. Dietary pattern analysis, which reflects the complexity of dietary intake, has recently received considerable attentionReference Trichopoulou and Critselis6.
Research on dietary patterns is warranted on several grounds. It has the ability to integrate the complex and subtle interactive effects of many dietary exposures and more closely approximates the biological activities of interdependent nutrients in vivo. Such research may resolve the problems generated by the multiple testing and high correlations that regularly occur in the analysis of individual foods or nutrients. Recommendations for disease prevention implicitly reflect the dietary pattern approach by emphasizing the simultaneous change of several dietary behaviours, such as increasing fruit and vegetable intake and decreasing meat intakeReference Ledikwe, Wright, Mitchell, Miller and Jensen7, Reference Kant, Schatzkin, Graubard and Schairer8.
The primary goal of the present study is to define dietary patterns among a cohort of Chinese men between 40 and 74 years of age using data collected from a validated FFQ and to identify factors that correlate with those dietary patterns.
Methods
Subjects
The current study is based on cross-sectional survey data obtained from the baseline survey of the Shanghai Men's Health Study (SMHS). SMHS is an ongoing population-based prospective cohort study of 61 582 men with a primary focus on the relationships of diet with cancer and other chronic diseases. The study has been conducted in eight communities in urban Shanghai since 2002. Subject recruitment started in March 2002 and was completed in June 2006. Using a roster provided by the community office, a total of 83 125 permanent male residents between 40 and 74 years of age in the study communities were approached for the study by a trained interviewer (retired nurse or physician). The study was explained to each participant and consent to participate in the study was obtained. Afterwards, the interviewer administered a face-to-face interview (about 60 min long; mean 59·75 min) using a structured questionnaire, which included information on socio-economic status, living habits, physical activity and dietary habits. Also, study participants were asked whether they had ever been told by their doctors they have diabetes, hypertension, CVD, benign tumours or other chronic diseases. Of the eligible men approached for the study, 61 582 participated, with a participation rate of 74·1 %. Among non-participants, there were 17 513 refusals (21·1 %), 1360 men who had a serious health problem (1·6 %), 2252 men who were absent during the study period (3·1 %) and 118 subjects with other miscellaneous reasons (0·1 %). Non-participants were a little younger (51·3 (sd 8·4) years) than participants (54·9 (sd 9·7) years). The response rates were slightly varied by study districts (69·7–78·2 %). In the present study, the disease group was defined as having diabetes, hypertension, CVD or benign tumours, based on disease history at the baseline survey.
Dietary information
Dietary information was collected using a validated FFQReference Villegas, Yang, Liu, Xiang, Cai, Zheng and Shu9. The FFQ included eighty-one food items and covered 88·8 % of the commonly consumed foods in urban Shanghai. For each food item or food group, subjects were asked how frequently (daily, weekly, monthly, yearly or never) they consumed the food or food group, followed by a question on the amount of consumption in lians (1 lian = 50 g) per unit of time over the past 12 months. For seasonal food consumption (mainly fruits and vegetables) an additional question about months of food consumption per year was asked. The daily nutrient intake used for analysis was then derived from the FFQ using the Chinese Food Composition TablesReference Yang, Wang and Pan10. In addition, subjects were asked whether their intake of red meat, vegetables and fruits had changed during the past 5 years.
Dietary pattern derivation
Dietary patterns were derived using factor analysisReference Kleinbaum, Kupper and Muller11, with eighty-one individual foods or food groups entered into the analysis as the absolute amount of intake in g/d. The PROC FACTOR procedure in SAS version 9·1 (SAS Institute, Cary, NC, USA) was applied to perform the analysis. This procedure uses factor analysis and orthogonal rotation (varimax option in SAS) to derive non-correlated factors and to render it more easily interpretable. To determine which number of factors to retain, we examined both the scree plots and the factors themselves to see which set of factors most meaningfully described distinct food patterns. From these analyses, three factors were extracted. Factor loadings were calculated for each food or food group across the three factors (dietary patterns). Factors were thereby interpreted as dietary patterns and named after the food groups having the higher loading (loading >0·30). These loadings can be considered as correlation coefficients between food groups and dietary patterns and they take values between − 1 and +1. A factor score was then calculated for each subject for each of the three factors, in which the standardized intakes of each of the eighty-one foods or food groups were weighted by their factor loadings and summed. The sums were standardized again ((score − mean score)/standard deviation of score).
Statistical analysis
Partial Pearson's correlation coefficients adjusted for energy intake were calculated between factor scores and food or nutrient intakes. The association of dietary factor scores with other lifestyle and anthropometric factors were estimated using a logistic regression model. Dietary factor scores were categorized into two categories by their medians, and lifestyle factors were categorized into quartiles or tertiles based on the distribution of the study population. To determine the relationship between dietary factors and lifestyle factors, as well as the prevalence of some chronic diseases, we estimated the adjusted OR and 95 % CI for each quartile compared with the lowest quartile of each lifestyle factor. In these analyses, adjustment for age, education, income per person in a family, smoking status, alcohol consumption, physical activity, waist-to-hip ratio (WHR) and energy intake was made as appropriate (see footnotes to tables for details).
Results
A total of 61 582 men aged 40–74 years were included in the present study. Among them, 22 505 men had a history of selected disease, including diabetes (3874), hypertension (18 392), CVD (5156) and benign tumours (1968). The basic characteristics of the study population are shown in Table 1. The average age of these participants was 55 (sd 9.7) years and 23·6 % of the study participants had a college education. About 55 % of subjects had per capita family income of less than 1000 yuan per month, and approximately half worked as manual labourers (mainly manufacturing workers). A majority of the men (59 %) were current smokers and one-third consumed alcoholic beverages regularly (at least three times per week for more than 6 months), while 36 % participated in regular physical activity (at least once a week for a continuous 3 months).
Table 1 General characteristics of all participants in the Shanghai Men's Health Study
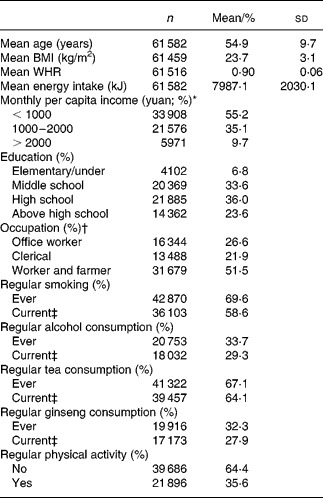
WHR, waist-to-hip ratio.
* 1 US$ = 8·2 yuan.
† Office worker: professor, technician, lawyer, doctor, teacher, administrators. Worker and farmer: manual labour workers in factories, construction and farms.
‡ Men in ‘Current’ group were included in the ‘Ever’ group.
We identified three major dietary patterns. Factor-loading matrices for the three dietary patterns are listed in Table 2. The higher the factor loading of a given food item, the greater the contribution of that food item to the specific factor. Dietary pattern I was heavily loaded with vegetables, such as legumes and leaf vegetables, and was labelled the ‘vegetable diet’. Pattern II was mainly rich in fruits and was labelled the ‘fruit diet’. Pattern III was characterized by high loadings on meat, poultry and animal parts (including heart, brain, tongue, intestine, etc.) and was labelled the ‘meat diet’. These three patterns explain 79 % of the variance of food intake.
Table 2 Factor loading for three major food patterns at baseline for 54 195 male adults in the Shanghai Men's Health Study*

* Factor loadings are multiplied by 100 and rounded to the nearest integer. Only factor loadings >30 are listed.
† If the powdered kind is used to make the drink, the amount consumed will be the amount of the drink.
Factor scores were calculated for all participants using factor loading of eighty-one foods or food groups. Their associations with food intake or nutrients are examined in Table 3. Correlation coefficients between factor scores and most of the nutrient or food intakes differed across the three dietary patterns. All dietary patterns were positively correlated with total energy intake. Therefore, correlations of other nutrients and food groups were adjusted for energy intake. All three dietary patterns, the fruit diet, the vegetable diet and the meat diet, showed high correlations with intake of their corresponding food groups, i.e. total fruit (r 0·81), total vegetable (r 0·90) and total meat (r 0·77). The meat diet had the strongest correlation with energy intake, a positive relation with consumption of fat and protein, and a negative relation with consumption of carbohydrates and dietary fibre. This diet also had relatively weak correlations with vitamins and minerals (r < 0·31, except sodium), as compared with the other two dietary patterns. The vegetable diet showed a very weak association with fat, but strong positive correlations with dietary fibre, vitamin A, vitamin C, vitamin E, folic acid, calcium and iron. The fruit diet had a moderate positive association with vitamins and minerals.
Table 3 Correlation coefficients between dietary factors and food groups or nutrients*
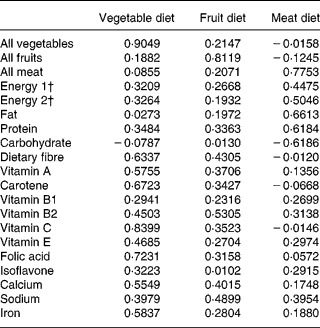
* Correlation for all food groups and nutrients, other than energy 1 and energy 2, are partial correlations, adjusted for energy 2. All correlation coefficients are statistically significant (P < 0·0001).
† Energy 1 came from all foods and food groups. Energy 2 came from both foods and alcohol consumption.
The relationship between the dietary patterns and selected population characteristics were examined by estimating the OR for being in the upper half of the score of each dietary pattern (Table 4). Dietary patterns varied according to socioeconomic and lifestyle factors, with the fruit diet showing the biggest variations. The fruit diet was more commonly consumed by those people who had higher income and higher education. It was also related to healthier lifestyle habits, such as no smoking, no alcohol consumption, more physical activity and low WHR. In contrast, people with higher consumptions of meat were more likely to be smokers and to drink more alcohol. It is interesting that the vegetable diet was not associated with income or education, but was, except for high WHR, moderately related to healthier lifestyle habits, such as no smoking, no alcohol consumption and regular physical activity, as compared with the other two dietary patterns.
Table 4 Dietary patterns in association with demographic and lifestyle factors in the Shanghai Men's Health Study*

WHR, waist-to-hip ratio.
* Adjusted for factors in this table mutually.
† 1 US$ = 8·2 yuan.
Table 5 shows the covariate-adjusted OR of benign tumours and chronic non-communicable diseases, such as diabetes, hypertension and CVD, by dietary pattern. Higher consumption of fruit and meat were more prevalent in the healthy men. However, these two dietary patterns had inverse relationships with diabetes: the OR for prevalence of diabetes in the highest quartile for the fruit diet was 0·39, but for the highest quartile of the meat diet the OR was 1·57, compared to the lowest quartiles of the fruit or meat diets, respectively. The vegetable diet was more commonly consumed by people with all four types of chronic diseases, and the highest OR for diabetes was 2·30 for the highest quartile, compared to the lowest quartile.
Table 5 Relation between prevalence of selected common diseases and dietary patterns*
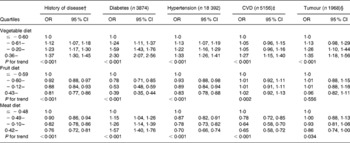
* Adjusted for age, education, income, energy intake, physical activity, ever smoking and ever drinking.
† Disease group was composed of diabetes, hypertension, CVD and tumour.
‡ Including acute myocardial infarction, CHD and stroke.
§ Benign tumour only.
Discussion
In the present study, we identified three distinct dietary patterns from a large group of Chinese men who participated in the SMHS, and we evaluated their relationship with socioeconomic and lifestyle factors. Other studies have reported the same patternsReference Park, Murphy, Wilkens, Yamamoto, Sharma, Hankin, Henderson and Kolonel12 or similar patternsReference Lopez-Garcia, Schulze, Fung, Meigs, Rifai, Manson and Hu13–Reference Bamia, Orfanos and Ferrari15 for men and women, often showing two to three dietary patterns in Western populations. Few studies have considered more than three patternsReference Newby, Muller, Hallfrisch, Andres and Tucker16–Reference Mishra, Ball, Arbuckle and Crawford18.
Several researchers have reported dietary patterns derived from FFQ in cohort studies using factor analysis. Although several distinct patterns were reported, two patterns were relatively dominant and were first introduced by Slattery et al. in 1998Reference Slattery, Boucher, Caan, Potter and Ma19. The first is a Prudent (Mediterranean, or vegetable–fruit diet) pattern characterized by high intake of vegetables, legumes, fruits and unrefined cereals. The other is a Western (Traditional, or red meat diet) pattern characterized by high intake of fat, meat and refined grain. Harvard researchers also derived these two dietary patterns from two large cohort studies, the Nurses' Health Study and the Health Professionals' Follow-up Study, and examined the relationship between these major dietary patterns and the risk of CHDReference Hu, Rimm, Stampfer, Ascherio, Spiegelman and Willett20, type II diabetesReference van Dam, Rimm, Willett, Stampfer and Hu21, and biochemical markers of obesity and CHD riskReference Fung, Willett, Stampfer, Manson and Hu22. A negative association of the ‘Prudent diet’ was demonstrated in all of these studies. Additionally, ‘Cake and sweet’, ‘Takeaway food’ and ‘Southern’ patterns have been identified in the other studiesReference Mishra, Ball, Arbuckle and Crawford18, Reference Schulze, Hoffmann, Kroke and Boeing23, Reference Tseng, Breslow, DeVellis and Ziegler24.
The meat diet found in the present study is similar to the Western pattern reported in other studies. The other two patterns, the vegetable and fruit diets, appear to be consistent with the set of food items that are part of Slattery et al.'s ‘Prudent’ patternReference Slattery, Boucher, Caan, Potter and Ma19. Interestingly, in the present study fruit and milk were part of the same dietary pattern, while the vegetable pattern did not include any dairy products. This indicates that correlation between fruit and milk is higher than that between vegetables and milk. The present result is consistent with that found in the study of Park et al. Reference Park, Murphy, Wilkens, Yamamoto, Sharma, Hankin, Henderson and Kolonel12, in which three distinct dietary patterns, ‘Fat and meat’, ‘Vegetables’ and ‘Fruit and milk’ were identified by factor analysis.
Food intakes can be handled in different ways in a factor analysis. Some studies have used individual food items and/or pre-defined food groups for factor analysis. Others aggregated food items into food groups based on the similarity of nutrient profiles or culinary usage in order to reduce the number of variables considered and minimize the within-person variation in consumption of individual foodsReference Lopez-Garcia, Schulze, Fung, Meigs, Rifai, Manson and Hu13, Reference Hoffmann, Zyriax, Boeing and Windler25. The resulting number of food group variables used in factor analyses differs widely from eightReference Marchioni, Latorre Mdo, Eluf-Neto, Wunsch-Filho and Fisberg26 to about 100Reference Mishra, Ball, Arbuckle and Crawford18. In the present study we used factor analysis based on pre-defined individual foods or food groups obtained directly from the FFQ, which in turn reflects the specific consumption habits of the Chinese population under study.
In the present study, the relationship between the three dietary patterns and age and health characteristics is similar to what has been reported in some earlier studies. Sanchez-Villegas et al. Reference Sanchez-Villegas, Delgado-Rodriguez, Martinez-Gonzalez and De Irala-Estevez27 reported a negative association between age and a Western dietary pattern, while Tseng & De VellisReference Tseng and DeVellis28 reported a positive association between age and a vegetable–fruit pattern. In the present study, age was negatively associated with the meat diet, but not associated with the fruit-based diet. We found that more educated people had higher scores for all dietary patterns and people with high income had higher scores for the meat and fruit diets, associations which have also been observed in other studiesReference Schulze, Hoffmann, Kroke and Boeing23, Reference Tseng and DeVellis28. No association between the vegetable diet and levels of income and occupation was found in the present study. This may be explained by the fact that vegetables are cheaper and more affordable than fruits and animal foods in China. The most commonly consumed vegetables in the study population are greens, Chinese greens, bean curd and soya products. Although these vegetables are less commonly consumed in Western countries, they contain many phytochemicals that have been shown to be beneficial to cardiovascular health and reduce cancer riskReference Manach, Williamson, Morand, Scalbert and Remesy29. In the present study, the meat diet was positively associated with WHR, current smoking status and alcohol consumption, but negatively associated with being a manual labourer. However, fruit and vegetable diets were negatively associated with having an office job, current smoking status and alcohol consumption, but positively associated with physical activity, similar to findings from earlier studiesReference Slattery, Boucher, Caan, Potter and Ma19, Reference Schulze, Hoffmann, Kroke and Boeing23, Reference Tseng and DeVellis28. Although our fruit and vegetable patterns showed relationships with many socioeconomic and lifestyle factors similar to other studies, only the fruit pattern was negatively associated with WHR and alcohol consumption. It seems that the fruit diet was more strongly associated with healthy lifestyles than the vegetable diet. Thus the ‘healthy diet’ in the present study, the fruit diet, could be extended to a ‘healthy profile’ that included no smoking, no or low alcohol consumption, more physical activity, and that was more frequently observed in men with higher education.
We did not find any association of a family history of cancer on dietary patterns. However, we did find a negative association between the fruit diet and chronic diseases. Associations of prevalence of chronic diseases showed the opposite trend for the meat diet compared to the vegetable diet. A strongly inverse association was found between the meat diet and all kinds of diseases, and a positive association was found between the vegetable diet and chronic diseases. A possible explanation of the present finding is that men changed their dietary behaviour after the diagnosis of a chronic disease. We found that among those men with a chronic disease, 25·5 % had decreased their red meat intake and 12·6 % had increased their vegetable intake in the previous year, as compared to their food intake 5 years ago. In contrast, among healthy men, 13·7 % had reduced their intake of red meat and 8·4 % had increased their intake of vegetables. Another possible reason is men with high income had more protein intake than those men with low income in the present study. Relative adequacy of protein intake may be a factor contributing to this inverse relationship since some studies found an inverse association between hypertension and protein intakeReference Liu, Ruth, Flack, Jones-Webb, Bruke, Savage and Hulley30, Reference Kihara, Fujikawa, Ohtaka, Mano, Nara and Horie31. In the present study, the association between prevalence of chronic disease and meat diet was attenuated by adjusting for protein intake. Some studies have reported associations between dietary patterns and prevalence or incidence of some chronic diseases, although the findings are inconsistentReference Sieri, Krogh, Pala, Muti, Micheli, Evangelista, Tagliabue and Berrino17, Reference Tseng, Breslow, DeVellis and Ziegler24, Reference Hoffmann, Zyriax, Boeing and Windler25, Reference Mizoue, Yamaji, Tabata, Yamaguchi, Ogawa, Mineshita and Kono32–Reference Fung, Stampfer, Manson, Rexrode, Willett and Hu37. Further investigation of the association of dietary patterns at baseline with subsequent cancer and other chronic disease incidence are planned for the SMHS.
Family income is an important confounding factor in the analysis of association between dietary factor and chronic disease in the present study. We found a positive association of family income and prevalence of chronic disease (OR 1·10, 95 % CI 1·06, 1·13), especially for hypertension. This association was absent when adjusted for age, education, energy intake and physical activity. The present result is slightly different from Colhoun's study in developed countries, in which the conclusion established that lower socioeconomic status adults had higher mean blood pressure and higher rates of hypertension in developed countries, with the gradient stronger and more consistently obtained in women than in menReference Colhoun, Hemingway and Poulter38.
The strengths of the present study include the population-based study design, high response rate and the use of a validated FFQ. There are some limitations in the present study. First, recall error is a problem inherent in the study of dietary intake and responses in the present study may have been confounded by selective under- or over-reporting of particular food itemsReference Lissner, Heitmann and Bengtsson39. The factor analysis approach itself involves several arbitrary decisions, which have been discussed elsewhereReference Hu, Rimm, Stampfer, Ascherio, Spiegelman and Willett20, Reference Schulze, Hoffmann, Kroke and Boeing23 and which include the consolidation of food items into food groups, the number of factors to be extracted, the method of rotation and even the labelling of the componentsReference Hu3, Reference Martinez, Marshall and Sechrest40. We did a sensitivity analysis using the whole data set and using data from only ‘healthy’ men without hypertension, CVD, diabetes or tumours. The same factors were extracted from these two data sets with only minor differences in factor loadings. The present study was based on a study conducted in urban Shanghai, one of most industrialized cities in China. Therefore, the results may not be generalized to other Chinese populations, especially the population in rural areas.
In conclusion, three main dietary patterns were identified for middle-aged men of urban Shanghai. Their dietary patterns were associated with age, education, prevalence of major chronic diseases and health behaviours in the present study. The present findings support the hypothesis that dietary patterns are influenced by interrelated socioeconomic and other lifestyle factors. It is important to consider these variables as potential confounding factors in the future analysis of diet and disease associations in the SMHS and other studies.
Acknowledgements
The study was supported by grant number RO1 CA82729 from the US National Institutes of Health. The authors thank the participants and staff members of the SMHS for their important contributions. The authors also thank Ms Brandy Sue Venuti for her assistance in manuscript preparation. H. C. contributed to the analysis and interpretation of the data, and writing of the manuscript. W. Z. contributed to experimental design, interpretation of the data and critical revision of the manuscript. Y.-B. X., W. H. X., G. Y. and H. L. were closely involved in implementation and performing quality control of this study. X. O. S. contributed to the experimental design and critical revision of the manuscript and also obtained funding. None of the authors had any conflict of interest.





