



Breast-feeding and healthy complementary feeding are essential practices for the health promotion in children under 2 years of age(Reference Som, Van Der Hoeven and Laillou1). Evidence shows that the beneficial effects of these practices can extend into adulthood(Reference Klingelhöfer, Braun and Quarcoo2). On the other hand, inadequate feeding practices in early life can increase the risk of morbidity and mortality, as they contribute to the adherence to poor dietary practices in other life stages as well as the development of non-communicable chronic diseases(Reference Klingelhöfer, Braun and Quarcoo2–Reference Schwartz, Issanchou and Nicklaus5).
The WHO began to recommend that babies be exclusively breastfed in 1990(6), and since 2001 has stated that the optimal duration is 6 months (180 d)(Reference Meira, Buccini and Azeredo7). Overall, the increase in breastfeeding prevalence has been reported in various studies worldwide, especially for exclusive breastfeeding in children under 6 months(Reference Neves, Barros and Baker8–Reference Ghosh, Rohatgi and Bose10). In 2019, the UNICEF stated that exclusive breastfeeding had increased from 35 % in 2005 to 42 % in 2018 in eighty low- and middle-income countries(Reference Neves, Vaz and Maia11). In Brazil, the latest national survey on breastfeeding in 2019 and 2020 showed that the recommendation of the WHO has not been met, as 45·8 % of children received breast milk in the country(12). This observation is particularly apparent for exclusive breastfeeding and continued breastfeeding in the second year of life. The WHO goal for 2030 is that at least 70 % of children under the age of 6 months are breastfed exclusively(Reference Lozano, Fullman and Abate13).
The WHO and UNICEF recognise the considerable impact of inadequate feeding practice on poor early nutrition(14). Therefore, they endorse exclusive breastfeeding in the first 6 months of life, followed by the safe introduction of complementary foods, with continued breastfeeding until 2 years of age(Reference Jones, Ickes and Smith15). In order to guarantee healthy complementary feeding practices, it is important that children consume foods with the appropriate consistency, diversity and frequency for their age. These conditions are represented in some of the main indicators of feeding practices for infants and young children recommended by the WHO and adopted by the Ministry of Health in Brazil(6,16,17) . These are (a) Introduction of solid, semi-solid or soft foods, (b) Minimum dietary diversity, (c) Minimum meal frequency, (d) Minimum acceptable diet and (e) Consumption of Fe-rich or Fe-fortified foods.
In contexts of socio-economic inequalities, the use of these indicators could be crucial, considering the immense threat that these extreme conditions may represent to ideal feeding practices(Reference Davis, Li and Adams-Huet18–Reference Simpson, Carson and Kurinczuk22). This inability to provide adequate nutrition to small children (6–23·9 months) has a direct impact on their micronutrient status and growth(Reference Jones, Ickes and Smith15). In Brazil, the monitoring of nutritional status is part of the Food and Nutrition Surveillance (VAN), provided for in the law that created the Unified Health System (SUS), which consists of the continuous description of the food and nutrition conditions of the Brazilian population(23). Despite the actions taken by the Ministry of Health regarding the expansion of Food and Nutrition Surveillance (VAN), the increase in the population at levels of serious poverty, high inflation on food prices and expenditure restraint on essential public policies, such as education and health, have severely compromised the food and nutrition security of Brazilian families, especially women and children(23–25).
As with many developing countries, overcoming inadequate feeding practices remains a challenge for Brazil. According to the National Study of Infant Food and Nutrition, the prevalence of minimum food frequency was 39.2 %, and the prevalence of minimum dietary diversity was 57.1 % among Brazilian children aged 6–23 months(12). This is a worrisome condition, as adequate and healthy food is a fundamental right of every child and a duty of the Brazilian State(26). We were motivated to explore the theme because of the lack of a systematic assessment of feeding indicators in infants and children under age 2 in Brazil, along with the relevance of assessing feeding trends over time to understand what changes have occurred, and to subsidise the planning of strategies to promote healthier diets for Brazilian children. Thus, the aim of this study is to describe the temporal trends in the prevalence of breastfeeding and complementary feeding indicators among children assisted by primary health care services in the Sistema Único de Saúde (SUS) between 2008 and 2019, according to the Brazilian deprivation index (BDI).
Methods
Study design and population
This is a time series study. Data were obtained from the Food and Nutrition Surveillance System (SISVAN) which includes data on food consumption of children under 2 years of age who assisted SUS primary care services between 2008 and 2019.
Data access, processing and analysis were conducted at the Centre for Data and Knowledge Integration for Health (CIDACS) of the Oswaldo Cruz Foundation (FIOCRUZ)(Reference Barreto, Ichihara and Almeida27). All children under 2 years of age with at least one entry record and a measure of food consumption were included. The most recent record per year of each assisted child was considered to estimate the prevalence of breastfeeding and complementary feeding indicators (Fig. 1).

Fig. 1 Selection of the study population. Food and Nutritional Surveillance System, 2008–2019
Indicators of infant and young child feeding practices
Food consumption records from SISVAN were used to calculate the following child feeding practice indicators: exclusive breastfeeding; mixed breastfeeding; continued breastfeeding; introduction of solid, semi-solid or soft foods (ISSSF); minimum meal frequency; minimum dietary diversity (MDD); minimum acceptable diet (MAD); consumption of meat and/or eggs; consumption of sweetened beverages; consumption of ultra-processed foods (UPF); consumption of Fe-rich foods; consumption of foods rich in vitamin A and zero consumption of fruit and vegetables(6,16) . Food consumption was evaluated using a standardised form with specific questions to qualitatively measure feeding practices the day before(16). The summary of the indicators is provided in Chart 1. The forms used in SUS primary health care services to obtain food consumption information were based on a document on indicators for assessing infant and young child feeding practices published by the WHO and revised by the Brazilian Ministry of Health in late 2014, with the aim of simplifying data collection and analysis of the information(16,17) . Accordingly, we opted to analyse the indicators of child feeding practices in two periods of time (2008–2014 and 2015–2019). For questions which did not change over time, or were equivalent, the analysis was conducted over the total study period (2008–2019). To evaluate the percentage of children that are monitored by SISVAN per year, the coverage was calculated from the ratio between the number of individuals with food consumption records and the total population under 2 years old, multiplied by 100.
Chart 1 Indicators in infant and young child feeding practices. Food and Nutrition Surveillance System (SISVAN)

Demographic and socio-economic variables
The socio-demographic data were obtained from SISVAN to characterise the study population: sex (female/male); age range (0–5 months/6–23 months) and geographic region of residence (North/Northeast/Central-West/Southeast/South). The BDI was used to evaluate the influence of the socio-economic profile of the child’s municipality of residence on indicators of feeding practices. The BDI is a measure that measures levels of material deprivation or, more generally, levels of socio-economic positions in different geographic areas of Brazil. This index was calculated based on three variables – (1) percentage of homes with a per capita income of ≤ 1/2 minimum salary; (2) percentage of illiterate people over the age of 7 and (3) average percentage of people with difficult access to sewage, water, waste collection, and do not have a bath/shower – in a single measure(Reference Allik, Leyland and Ichihara28). The measure was organised in descending order from the first quintile (less deprivation) to the last quintile (greater deprivation). The measure was validated by comparing it to other similar indices measuring health and social vulnerability at the census sector level in states and municipalities, and at the municipal level for across the whole of Brazil(Reference Portella, Mendes and Santos29). At the municipal level, the deprivation measure was also compared to health outcomes. The different validation exercises showed that the developed measure produced expected results and could be considered validated.
Statistical analysis
The descriptive analysis of the study population’s characteristics was conducted through absolute and relative frequencies. The prevalence of indicators of feeding practices was estimated annually by demographic and socio-economic variables. Area graphics were used to illustrate how breastfeeding practices progressed as children grow. This graph is useful to understand exclusive breastfeeding patterns in different age ranges in the 0- to 5-month window and provides information on the types of other food introduced in this period in addition to breast milk for each age.
Prais–Winsten estimation was used to analyse the time trends in the prevalence of indicators of feeding practices. This generalised linear regression method has been widely used to correct serial correlations in time series(Reference Antunes and Cardoso30). The annual prevalence for each indicator was converted into a logarithmic scale to reduce heterogeneity of variance in the regression model. The prevalence values transformed into a logarithmic scale were defined as dependent variables, while the year was defined as the independent variable. The annual percentage variation (APC), and respective 95 % CI, were calculated in accordance with the following formula: APC = (–1 + 10β) × 100, where β is the Prais–Winsten regression coefficient(Reference Antunes and Cardoso30).
The ratio between the estimates of the extreme groups (quintiles) of the deprivation index was calculated. This is a simpler measure of relative inequality. This was calculated by dividing the prevalence values corresponding to the group with less deprivation (BDI/Q1) by the group with more deprivation (BDI/Q5). It produces the surplus percentage of one category in relation to the other, or how many times prevalent one group is compared to the other. All data were processed and analysed using Stata version 15·1 software (StataCorp. 2017. Stata Statistical Software: Release 15. StataCorp LLC).
Complementary analysis
Time trend analyses of the prevalence of breastfeeding and complementary feeding practice were conducted by quintiles of the Municipal Human Development Index (MHDI). Education, longevity and income are considered in this index(31), and it varies from 0 to 1. The closer to 1, the higher the human development.
Results
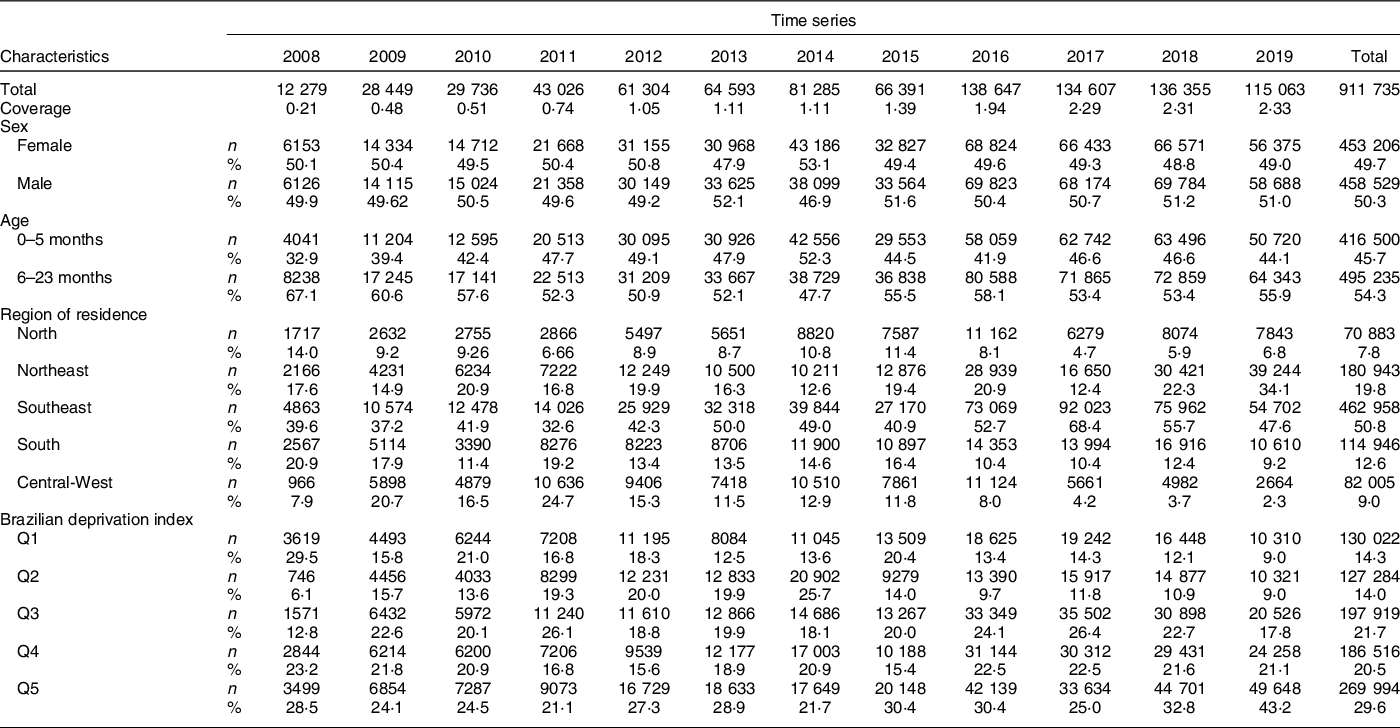
The study included a total of 911 735 children, with a variation of 12 279 in 2008 and 115 063 in 2019. We found a slight increase in the coverage of food intake monitoring over the years, ranging from 0·21 to 2·33 %. Half of the children evaluated were male (50·3 %), and the majority were aged between 6 and 23 months. 8·7 % were from the North, 18·8 % from the Northeast, 14·1 % from the South, 11·6 % from the Central-West and 46·5 % the Southeast region. Regarding the level of deprivation, 29·6 % of the children evaluated were in the quintile of highest municipal deprivation (Q5). Further characteristics of the study population can be found in Table 1.
Table 1 Characteristics of the study population. Food and Nutrition Surveillance System (SISVAN), Brazil, 2008–2019
The prevalence of breastfeeding practices in children under 6 months of age in 2015 and in 2019 are presented in Fig. 2. In the first month of life, more than 70 % of children were exclusively breastfed. This prevalence reduced progressively until 4 and 5 months in both years. From 2 to 3 months, there was an expressive increase in the prevalence of ISSSF. In addition, a considerable percentage of the children consumed breast milk and water. Mixed breastfeeding also increased during the period analysed.

Fig. 2 Infant feeding area graphs under 6 months - Food and Nutritional Surveillance System in 2015 and 2019
Time-trend analysis of the prevalence of feeding practice indicators, in accordance with the BDI, can be found in Table 2 and Table 3. Overall, the percentage of children under 6 months in mixed breastfeeding varied from 10·0 % to 11·9 % between 2015 and 2019, corresponding to an annual variation of +10·38 % (P = 0·013). This increase was demonstrated in the extreme BDI quintiles, especially in the municipalities with more deprivation (Q1: APC = +10·60, P = 0·003; and Q5: APC = +21·74, P = 0·002).
Table 2 Prevalence of breast-feeding practice indicators in children under 24 months in accordance with the Brazilian deprivation index. Food and Nutrition Surveillance System (SISVAN), Brazil, 2008–2019

APC, annual percentage change; R2, coefficient of determination.
* Exclusive breastfeeding data could not be used, since information was missing for 2013.
Table 3 Prevalence of complementary feeding practice indicators in children under 24 months in accordance with the Brazilian deprivation index. Food and Nutrition Surveillance System (SISVAN), Brazil, 2008–2019

APC, annual percentage change; R2, coefficient of determination.
With regards to complementary feeding indicators, a low prevalence of MDD and MAD indicators was observed in all years of the series studied. It was also noted that the percentage of children in compliance with the ISSSF indicator reduced in the municipalities with less deprivation (Q1: –1·90, P < 0·001). These results were reversed for MDD (Q1: +1·44, P = 0·006) and MAD (Q1: +5·17, P = 0·004).
A decrease in the percentage of children who consume UPF (Q1: –7·76, P = 0·004; and Q5: –10·56, P < 0·001) and sweetened beverages (Q1: –14·39, P = 0·001; and Q5: –14·84, P < 0·001) was registered, independently of the extreme BDI quintiles. An increase in the percentage of children who consume meat and/or eggs was observed, also independently of the extreme BDI quintiles, although higher in the municipalities with less deprivation (Q1: +6·29, P < 0·001; and Q5: +2·20, P = 0·041). In general, the percentage of children who consume Fe-rich foods reduced over time (–5·67, P = 0·006). The percentage of children who do not consume fruit and vegetables also reduced (–10·53, P < 0·001), especially in the municipalities with more deprivation (Q5: –12·15, P < 0·001).
Similar trend patterns in the indicators of child feeding practices were found when evaluated by the MDHI (online Supplementary Table 1 and Table 2).
Discussion
This study enabled the analysis of time trends in indicators of child feeding practices in Brazil, according to an important marker of social inequality. Our data indicated an increase in the proportion of children under 6 months experiencing mixed breastfeeding, especially in the municipalities with more poverty, and a low prevalence of MDD and MAD indicators. Furthermore, breastfeeding patterns and complementary feeding differed among extreme BDI quintiles. In general, results were more favourable in municipalities with less poverty. Improvements in complementary feeding indicators, such as MDD, MAD and the consumption of meat and/or eggs, were primarily demonstrated in the municipalities with less poverty. The reduction in the proportion of children who did not consume fruit and vegetables were more accentuated in the municipalities with more poverty. The decrease in the consumption of sweetened beverages and UPF, independently of the degree of inequality, was also highlighted.
Despite the recommendation that breast milk should be the only food offered to children under 6 months, we found that almost 30 % of children abandon exclusive breastfeeding in the first month, an alert for the intensification of actions to promote exclusive breastfeeding in primary care in the first weeks of life. Our data did not indicate any trend in the prevalence of exclusive breastfeeding, which remained stable in the 50–60 % range for the entire series, although higher than those found by ENANI, 2019 (45·8 %)(12). The differences in these results can be explained by the type of population to which our study refers. The downturn in the gains which had been observed between 1986 and 2006 is cause for concern. For the first time in a historical series, real increases in the prevalence of exclusive breastfeeding in Brazil were not observed(Reference Boccolini, de Moraes Mello Boccolini and Monteiro32). On the other hand, the increase in the proportion of children experiencing mixed breastfeeding, mainly in the municipalities with a higher level of deprivation, is cause for alarm. This practice has been associated with poor oral health and increased risk of overweight/obesity(Reference Victora, Bahl and Barros33).
An increasing trend in MAD prevalence in the municipalities with less poverty was confirmed. As an indicator which includes breast milk substitutes, MAD implies that children need to receive both diverse foods (MDD) in a recommended number of meals (minimum meal frequency) such as the consumption of six food groups a day. This condition may not be easy to achieve in poorer regions(Reference Tizazu, Laillou and Hailu34). Certainly, many families still face the challenge of meeting minimum dietary standards for children(Reference Alves Cavalcanti and Boccolini35). This highlights the need for a broader understanding of complementary feeding practices in the context of food and nutrition insecurity(Reference Al Mamun, Saha and Li36,Reference Salarkia, Neyestani and Omidvar37) . Similar negative associations between MAD and low socio-economic status were also found in others studies, which used Demographic and Health Surveys data, conducted in low- and middle-income countries(Reference Gatica-Domínguez, Neves and Barros19,Reference Tizazu, Laillou and Hailu34,Reference Nguyen, Avula and Headey38) .
We observed a reduction in the percentage of children aged 6–24 months who consumed sweetened beverages and UPF, independently of the extreme poverty quintiles. In parallel, an important reduction in the proportion of children who do not consume fruit or vegetables was noted, especially in municipalities with more poverty. Shifts in feeding practices have been observed in recent decades, inserted in the concept of nutrition transition, which is a process of sequential changes in dietary patterns. Therefore, a dietary pattern does not remain stagnant. We can speculate about the emergence of a new stage of the nutrition transition process, as a consequence of the desire to prevent or delay degenerative diseases and extend good health, with the adoption of a better quality diet and higher amount of fruit, vegetables and whole grains(Reference Chong39).
Despite the important reduction in the consumption of UPF and sweetened drinks, their prevalence remain very high in this population, corroborating the findings of previous national and international studies(Reference Cainelli, Gondinho and Palacio40–Reference Spaniol, Da Costa and Souza42). The consumption of UPF in the first 2 years of life is not recommended, since they usually have a high energy density, higher quantity of sugar, Na, saturated fat and lower quantity of essential fibres and nutrients(Reference Campos, Dos Santos and Lopes43,Reference Leffa, Hoffman and Rauber44) . However, the high palatability, availability and ‘aggressive’ marketing of these products challenge conscientious consumption and make them preferential replacements for in natura, or minimally processed foods(Reference Campos, Dos Santos and Lopes43,Reference Martins, Levy and Claro45) . Another aggravating factor is that the introduction of these products has been taking place very prematurely in children’s diets, even before they reach 12 months of age. The consumption of UPF is also related to a higher prevalence of obesity, chronic diseases and nutritional deficiencies in the early years of life and may also compromise the consumption of the healthy foods associated with adequate growth and child development(Reference Rousham, Goudet and Markey46––Reference Fedde, Rimbach and Schwarz48). On account of this, special attention must be given to the consumption of complementary foods in this life stage, in accordance with the Food Guide for the Brazilian population(49), an official document released by the country’s Ministry of Health. The guide provides recommendations and information on feeding practices in the first 2 years of life, with the aim of promoting good health, growth and development, so that they are able to achieve their full potential.
An increase in the proportion of children who consume meat and/or eggs was observed, especially in the municipalities with less poverty. These disparities are probably due to the high cost of these foods(Reference Bai, Alemu and Block50). Inaccessibility and the high cost of protein-rich foods have been a growing area of concern, preventing the adoption of adequate and healthy diets(Reference Headey and Alderman51). A global analysis involving 177 countries showed that a diet which is adequate in protein costs 2·66 times the cost of daily energy subsistence, and this value was much higher in Sub-Saharan Africa(Reference Bai, Alemu and Block50). In Brazil, the price of protein-rich foods has increased significantly in recent years while the price of UPF has remained stable or even declined over the same period(Reference Canuto, Fanton and de Lira52). Therefore, these price changes may further discourage the adoption of a more diverse diet, which partly explains the prevalence of UPF remaining high for all social strata.
At the national level, health and nutrition interventions executed through large scale and multisectoral programmes are essential to address the inequalities shown in our results. Among these initiatives, we highlight the national breastfeeding and complementary feeding strategy (Amamenta e Alimenta Brasil), the Dietary Guidelines for Brazilian Children Under 2 Years of Age, the federal conditional cash transfer programme’s health conditions (monitoring of nutritional status, vaccination and prenatal visits) and the qualification of maternal, prenatal and child health care(23,49,53) . In addition, it may be useful to learn from successful actions implemented by other countries that have adopted an integrated strategy to promote breastfeeding and healthy complementary feeding by focusing on interventions during pregnancy and in the first 2 years of life.
Strengths and limitations
As in all studies that use secondary data, limitations related to incompleteness, underestimation and classification bias should be recognised. Another limitation of this study resides in the fact that SISVAN data is not representative of the total population of Brazil. Primary Care covers around 60–70 % of the population and SISVAN covers less than 3 % of the population of children in the analysed age group. On the other hand, SISVAN constitutes a good data source for food and nutrition surveillance, which has advanced over time in coverage and data quality, representing an important tool for public policy management and the production of evidence in the field of maternal and child health. Another limitation of this study is the differences in the data collection forms in the years the research was conducted. Despite this point, the study provides relevant evidence on breastfeeding and the complementary feeding of Brazilian children over the years studied.
However, this study has the merit of identifying changes in the indicators of food consumption for children under 2 years of age over a 12-year period, using national data produced by an information system used by health care services and managed by the Brazilian Ministry of Health. We have used the indicators suggested by the WHO, and partly adopted by the Ministry of Health, which allows comparability with other national and international studies. Although the data collection instrument does not allow us to detail the frequency and age at which food was introduced, the questionnaire has important advantages such as the easy and fast application by any primary health care professional. The information collection technique also allows for the reduction of memory bias and is used by health teams to monitor the food consumption indicators for the population within the SUS. To the best of our knowledge, this is the first study to evaluate food consumption indicators in accordance with the BDI.
Conclusion
Breastfeeding and complementary feeding patterns differ among the extreme BDI quintiles. In general, results were more favourable in municipalities with less poverty. Data also demonstrated improvements to these patterns over time, especially in municipalities with less poverty. Inadequate complementary feeding practices are the main determinants of malnutrition, development and mortality. Therefore, these findings have the potential to assist in the preparation of targeted actions for high-risk groups. They also contribute towards prevention and control of morbidities associated with diet, thereby supporting attaining the Sustainable Development Goals described in the United Nations 2030 agenda, including efforts to eradicate hunger and malnutrition, and to promote health and well-being.
Acknowledgements
Acknowledgements: We would like to thank the CIDACS/FIOCRUZ data production team’s staff for their work on linking the data used in this study and providing information on data quality. We would also like to thank the IT team for their efforts helping to facilitate our access to data. Authorship: G.R.S., R.C.R.S., M.S.F.M. and N.J.S. conceptualised and designed the study, drafted the initial manuscript, created the analysis plan, and reviewed and revised the manuscript. R.C.S.A., J.P., A.M.S., G.A.B., E.A.F.N., S.A.S., B.H.L., A.S.R., I.R.F., M.Y.T.I., D.R.F. and M.L.B. conceptualised and designed the study and critically reviewed the intellectual content of the manuscript. All of the authors approved the final submitted version of this manuscript and have accepted accountability for all aspects of the work. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Collective Health Institute, Federal University of Bahia (UFBA) (CAAE: 41695415.0.0000.5030). Written informed consent was obtained from all subjects. The analyses were conducted with de-identified data, and several security procedures were adopted to protect data access.
Financial support:
This study was financed by MS-SCTIE-Decit/ CNPq (public notice no. 442948/2019-0). The study also received support from CIDACS, which receives funding from the Bill & Melinda Gates Foundation (grant number OPP1142172), the Wellcome Trust (grant number 202912/Z/16/Z), Coordination for the Improvement of Higher Education Personnel (Capes - grant number: 88887.699346/2022-00), Department of Health Surveillance at the Ministry of Health, State of Bahia (Decentralized Execution Term – TED number 159/2019), State of Bahia Foundation to Support Research (FAPESB) (grant number INT0001/2015), Funding Authority for Studies and Projects (FINEP) (Notice CT-INFRA - FIOESTAT - Agreement number 04.10.0635.00, reference number 811/10) and the State of Bahia Department of Science and Technology (SECTI) (term of assignment of movable property 048/2018, process number 1430150022698). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. The authors received no specific funding for this work.
Conflict of interest:
There are no conflicts of interest.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980023001039









 Open access
Open access