


Dyslipidaemia, a major systemic disorder, is one of the key risk factors of CVD, and its morbidity is high and it is a leading contributor to mortality worldwide( Reference Murray and Lopez 1 ) including China. The prevalence of dyslipidaemia is increasing in China( Reference Murray and Lopez 1 , Reference Wu, Yao and Zhao 2 ).
Tea, from the plant Camellia sinensis, is a widely consumed beverage in the world, especially in Shantou, southern China. People have a special way of preparing tea, called Gongfu tea. The teapot is as big as a fist and the teacups are as small as tiny liqueur glasses (30 ml). Gongfu tea is prepared by brewing dried tea leaves with hot water. Drinking Gongfu tea is a pastime and a social activity to promote friendship and business negotiations in the region. These features might help us determine the relatively large variation in tea intake and measure tea intake with high reliability.
Tea contains many compounds, especially polyphenols, depending on the degree of fermentation. Tea can be classified into three major types: non-fermented green tea; partially fermented oolong tea; fully fermented black tea( Reference Negishi, Xu and Ikeda 3 ). The composition of partially fermented oolong tea is somewhat similar to that of green tea. During the fermentation process, catechins are converted into the major black tea polyphenolic components theaflavins and thearubigins and other high-molecular weight components( Reference Yang and Koo 4 ).
Epidemiological studies have shown that polyphenolic compounds present in tea could reduce the risk of CVD( Reference Mukamal, Maclure and Muller 5 – Reference Peters, Poole and Arab 7 ). Tea may protect against CVD by affecting lipid and lipoprotein levels. Animal studies have demonstrated blood levels of lipids to be lowered by the consumption of tea extracts( Reference Yang and Koo 4 , Reference Akinyanju and Yudkin 8 – Reference Bursill and Roach 10 ), but results of clinical trials on the effect of tea consumption on serum lipid concentrations in human subjects have been inconsistent( Reference Nagao, Komine and Soga 11 – Reference van het Hof, de Boer and Wiseman 15 ). Although intervention studies had examined relatively large differences in tea intake among the groups compared, the duration of interventions was, in general, short and long-term tea consumption was not assessed( Reference Bingham, Vorster and Jerling 16 – Reference Duffy, Vita and Holbrook 18 ). The effect of tea consumption on dyslipidaemia requires a long duration to develop, so information on long-term tea exposure is important. To our knowledge, only a few epidemiological studies have shown an inverse relationship between green tea consumption and lipid levels( Reference Frank, George and Lodge 19 – Reference Kono, Shinchi and Ikeda 21 ), but not for oolong tea consumption. Oolong tea contains oolong tea polymerised polyphenols (OTPP), derived from the process of semi-fermentation, which are not present in green tea. OTPP have stronger inhibitory effects on lipase than the total extracts of green tea in vitro ( Reference Nakai, Fukui and Asami 22 ). Studies in mice have shown that oolong tea leaves have the strongest lowering effect on TAG levels( Reference Kuo, Weng and Chiang 23 ). The Shantou population mainly uses the semi-fermented oolong tea, so epidemiological evidence of an association with reduction of lipid levels is needed for this population.
The present population-based case–control study aimed to ascertain the association between consumption of tea, especially oolong tea, and risk of dyslipidaemia in Shantou, southern China.
Methods
Study participants
A population-based case–control study of dyslipidaemia was conducted in Shantou in southern China, from January 2010 to December 2010. The survey involved a questionnaire, medical examination, anthropometric parameter measurement and venous blood tests. All the participants aged 20–80 years had resided in Shantou for at least 5 years. The participants were randomly recruited from a cross-sectional survey of chronic diseases in Shantou, which was conducted in the health care centres of the First Affiliated Hospital of Shantou University Medical College and Chaonan Minsheng Hospital of Shantou. The required sample size was determined by assuming that 20 % of southern Chinese adults drank 2 paos of tea daily with the relative risk of dyslipidaemia being 0·7 at such a level of intake, which was evaluated by our preliminary investigation. For a one-to-one case–control ratio at the 5 % level of significance, the sample size needed to attain 90 % power was 1170 per group as calculated by NCSS–PASS 2005. To further account for refusal and withdrawal, 1800 eligible cases and 1800 control subjects were approached and invited to participate in the study. A total of 1651 patients with dyslipidaemia and 1390 control subjects completed the entire interview, representing an eventual response rate of 91·7 and 77·2 %, respectively. Cases were diagnosed by the recommendations of the National Cholesterol Education Program( 24 ). Selection criteria for cases were newly diagnosed dyslipidaemia with no history of dyslipidaemia and those for eligible controls were no history or clinical evidence of dyslipidaemia. Exclusion criteria for both cases and controls were major health problems such as heart diseases, stroke and cancer and use of medications that could interfere with lipid metabolism. The present study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethics Committee of the First Affiliated Hospital of Shantou University Medical College and Chaonan Minsheng Hospital. Written informed consent was obtained from all the subjects.
Anthropometric parameter measurement
Data were collected in examination centres at the hospitals. Body weight, height, waist circumference and blood pressure were measured by trained observers according to a standard protocol. Body weight and height were measured to the nearest 0·1 kg and 0·1 cm, respectively, with standardised equipment, and BMI was calculated as weight (kg)/height squared (m). Systolic blood pressure and diastolic blood pressure were averaged from three measurements.
Questionnaire and exposure measurements
A double-blind method was used for the questionnaire survey. Both the researchers and participants were blind to the dyslipidaemia status of the participants. Trained research staff used a standard questionnaire to collect demographic information and medical history. Demographic and lifestyle data included those on age, sex, education level (primary school, middle school, college or above), occupation (manual worker, office worker or retired/unemployed), smoking status (non-smoker or former/current smoker) and pack-years, alcohol drinking status (non-drinker or former/current drinker), physical activity (frequency/d per week per month) and sitting time per d ( < 6, 6–9 or >9 h).
Information on the intake of common foods was obtained using a 125-item semi-quantitative FFQ developed for the southern Chinese population( Reference Ke, Toshiro and Fengyan 25 , Reference Song, Toshiro and Li 26 ). This validated instrument covered most of the food items commonly consumed in southern China. Intake frequency (per d/week/month) was recorded in detail. The reference recall period for dietary variables was set at 1 year before the interview process. In addition, we asked specific questions about tea consumption that had established reliability and reproducibility; intra-class correlation coefficients were 0·82–0·95( Reference Jian, Xie and Lee 27 ). The subjects were classified as ‘ever’ or ‘never’ tea drinkers (less than once per month). The ever-drinkers were asked to report their frequency of habitual intake in paos (about 300 ml, ten teacups of Gongfu tea: 1–3/month; 1–6/week; 1–2/d; 2–4/d; >4/d), duration of regular tea consumption (in years), types of tea consumed (green, black and oolong) and average quantity of dried tea leaves used for brewing (in grams) per year. For those who drank more than one type of tea, the reported ratio of consumption was used to estimate the respective frequency and amount of dried tea leaves for each type.
Laboratory methods and definition of dyslipidaemia
All the examinations were carried out in the clinical laboratory at the hospitals. The concentrations of blood plasma total cholesterol (TC), TAG, HDL-cholesterol (HDL-C) and LDL-cholesterol (LDL-C), fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, uric acid and creatinine were measured by an enzymatic method using a Beckman autoanalyser (Beckman DXC800, Beckman Coulter, Inc.). Reagents of the same batch were used. Dyslipidaemia was defined as hypercholesterolaemia (H-TC; TC levels ≥ 5·18 mmol/l (2000 mg/l)), hypertriacylglycerolaemia (H-TAG; TAG levels ≥ 1·70 mmol/l (1500 mg/l)) or lower HDL-C (HDL-C levels < 1·04 mmol/l (400 mg/l)). These cut-offs were selected from the National Cholesterol Education Program recommendations( 24 ).
Statistical analysis
Descriptive statistics were used to summarise the characteristics of the participants and their tea consumption patterns. We examined the effects of tea consumption on dyslipidaemia risk using a logistic regression analysis of frequency of intake, duration of tea consumption and quantity of tea leaves brewed. We converted pao into ml for the analysis; 1 pao equates to ten teacups of Gongfu tea, about 300 ml. The frequency of tea drinking was classified into four levels ( < 300 ml/week, 300–1800 ml/week, 300–600 ml/d and >600 ml/d), with the lowest level of intake being used as the reference category. For total and type-specific tea leaves used, we used the 33rd and 66th percentiles of these continuous variables among drinkers as cut-offs, which resulted in three increasing levels of exposure, with < 1 g/year as the reference category. To further assess the dose–response relationship between long-term tea exposure and dyslipidaemia risk, we used a linear trend analysis of duration of tea consumption and total and type-specific tea leaves brewed. Both crude and adjusted OR and 95 % CI were calculated. Finally, we used multiple linear regression to estimate the association between duration of oolong tea consumption and levels of blood lipids. The variables estimated from the linear regression model were used to calculate the absolute difference from the reference group. Percentage difference was calculated using the absolute reduction divided by the adjusted mean of the reference group. Adjusted mean lipid levels were calculated using least-squares means in the PROC GLM procedure of SAS for each category of duration of oolong tea consumption. Besides tea consumption, independent variables included in the regression models were age, sex, education level, BMI, physical activity, smoking status and pack-years, alcohol drinking status, and presence of hypertension and diabetes, together with weekly dietary intake of meat, fish, poultry, fruit and vegetables, with all being considered potential confounders from univariate analysis. A two-sided P< 0·05 was considered statistically significant. All the data were double entered using Epi Info version 6.0 (Centers for Disease Control and Prevention) and then exported to SAS version 9.10 (SAS Institute, Inc.) for analysis. Power calculations involved the use of NCSS–PASS 2005.
Results
Demographic characteristics
Table 1 summarises the demographic characteristics of the participants. The study included 3041 subjects: 1651 with dyslipidaemia and 1390 controls. Among the cases were 1043 individuals with H-TC, 893 with H-TAG and 445 with L-HDL. According to univariate logistic regression, increased age, sex, education level and occupation were associated with dyslipidaemia (all P< 0·05). Patients with dyslipidaemia had higher BMI, waist circumference and blood pressure and higher levels of fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, creatinine and urine acid than controls (P< 0·001) and increased cumulative smoking exposure, alcohol drinking status and sitting time, as well as reduced physical activity (P< 0·01).
Table 1 Demographic characteristics of cases and controls in the present study carried out in Shantou, China (Mean values and standard deviations; percentages, odds ratios and 95 % confidence intervals)
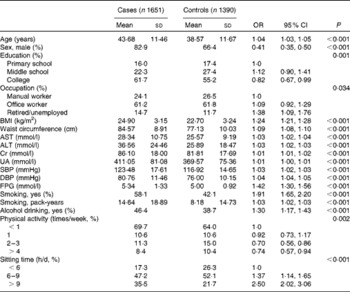
AST, aspartate aminotransferase; ALT, alanine aminotransferase; Cr, creatinine; UA, uric acid; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose.
Dietary characteristics
The consumption of vegetables, fruit, soya food and milk at least once a week was strongly associated with a reduced risk of dyslipidaemia when compared with infrequent consumption or non-consumption (P< 0·01; Table 2). In addition, the consumption of animal offal, lard and pickle at least once a week was strongly associated with an increased risk of dyslipidaemia when compared with infrequent consumption or non-consumption (P< 0·01).
Table 2 Association of dietary components with dyslipidaemia among cases and controls* (Odds ratios and 95 % confidence intervals)
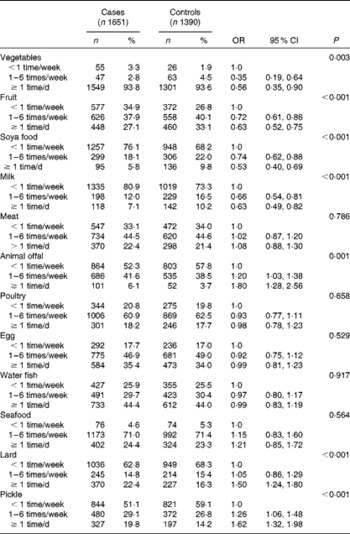
* OR and P values refer to those of the controls.
Tea consumption patterns
Table 3 summarises the results of univariate and multivariate logistic regression analyses of the association between frequency of tea consumption and risk of dyslipidaemia. The probability values were obtained using a likelihood ratio test of the overall significance of each variable of tea consumption in multivariate models. On carrying out a binary multivariate logistic regression analysis, with all the variables found to be significantly associated with dyslipidaemia risk in univariate analysis, drinking at least 300 ml (1 pao) of tea per week was found to be associated with a decreased risk of dyslipidaemia when compared with infrequent consumption or non-consumption (P< 0·001), with the reduction in risk being most effective when drinking more than 600 ml (2 paos) daily (adjusted OR 0·28, 95 % CI 0·20, 0·39). Similar results were obtained for the type of tea consumed (P< 0·05).
Table 3 Association between consumption of tea and risk of dyslipidaemia* (Odds ratios and 95 % confidence intervals)
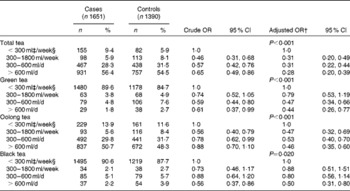
* The crude OR, adjusted OR and P values refer to those of the controls.
† Adjusted for age; sex; education level; BMI; waist circumference; systolic blood pressure; diastolic blood pressure; levels of fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, creatinine and uric acid; physical activity; sitting time; smoking status; smoking pack-years; alcohol drinking status and weekly dietary intake of vegetables, fruit, soya food, milk, animal offal, lard and pickle.
‡ 300 ml equate to 1 pao.
§ Referent.
The relationship between consumption of the three types of tea and components of dyslipidaemia was further analysed by multivariate logistic regression (Table 4). Consumption of all the three types of tea was associated with a reduced risk of H-TC, H-LDL and H-TAG, especially consumption of green tea (adjusted OR 0·26, 95 % CI 0·13, 0·53; adjusted OR 0·24, 95 % CI 0·11, 0·54; adjusted OR 0·22, 95 % CI 0·10, 0·53, respectively; P< 0·001), but only oolong tea, was significantly associated with L-HDL (adjusted OR 0·38, 95 % CI 0·26, 0·56; P< 0·001).
Table 4 Association between frequency of tea type consumed and components of dyslipidaemia (Odds ratios and 95 % confidence intervals)
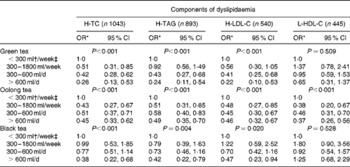
H-TC, hypercholesterolaemia; H-TAG, hypertriacyclglycerolaemia; H-LDL-C, hyper-LDL-cholesterol; L-HDL-C, lower HDL-cholesterol.
* Adjusted for age; sex; education level; BMI; waist circumference; systolic blood pressure; diastolic blood pressure; levels of fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, creatinine and uric acid; physical activity; sitting time; smoking status; smoking pack-years; alcohol drinking status and weekly dietary intake of vegetables, fruit, soya food, milk, animal offal, lard and pickle.
† 300 ml equate to 1 pao.
‡ Referent.
The effect of cumulative tea exposure and quantity of dried tea leaves brewed on dyslipidaemia is summarised Table 5. Long duration of tea consumption, especially for more than 20 years, was associated with a reduced risk of dyslipidaemia (adjusted OR 0·10, 95 % CI 0·06, 0·16, P< 0·001). In terms of the amount of tea leaves used, the dose–response relationship was significant overall (P< 0·001). In particular, mean monthly consumption of green tea leaves of more than 750 g was associated with the largest reduction in dyslipidaemia risk (adjusted OR 0·37, 95 % CI 0·25, 0·54, P< 0·001).
Table 5 Association of duration of tea consumption and amount of dried tea leaves brewed with dyslipidaemia* (Odds ratios and 95 % confidence intervals)
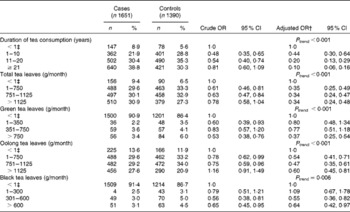
* The crude OR, adjusted OR and P values refer to those of the controls.
† Adjusted for age; sex; education level; BMI; waist circumference; systolic blood pressure; diastolic blood pressure; levels of fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, creatinine and uric acid; physical activity; sitting time; smoking status; smoking pack-years; alcohol drinking status and weekly dietary intake of vegetables, fruit, soya food, milk, animal offal, lard and pickle.
‡ Referent.
Furthermore, we analysed the association between cumulative oolong tea exposure and blood lipid levels using multiple linear regression models, with adjustment for variables significantly associated with dyslipidaemia (Table 6). The duration of tea consumption was linearly associated with blood TC, TAG and LDL-C levels (P< 0·05). Compared with the reference group, oolong tea consumption ≥ 21 years was associated with a decrease in blood TC, TAG and LDL-C levels: 0·16 mmol/l (95 % CI 0·03, 0·28 mmol/l; 3·22 %); 0·19 mmol/l (95 % CI 0·10, 0·39 mmol/l; 11·99 %); 0·19 mmol/l (95 % CI 0·17, 0·41 mmol/l; 6·69 %), respectively, but not with HDL-C levels.
Table 6 Adjusted association between duration of oolong tea consumption (in categories) and levels of blood lipids
TC, total cholesterol; LDL-C, LDL-cholesterol; HDL-C, HDL-cholesterol.
* Calculated by the absolute reduction divided by the adjusted mean of the reference group.
† Data were adjusted for age; sex; education level; BMI; waist circumference; systolic blood pressure; diastolic blood pressure; levels of fasting plasma glucose, alanine aminotransferase, aspartate aminotransferase, creatinine and uric acid; physical activity; sitting time; smoking status; smoking pack-years; alcohol drinking status and weekly dietary intake of vegetables, fruit, soya food, milk, animal offal, lard and pickle.
‡ Referent.
Discussion
The important role of dyslipidaemia in atherosclerosis and CHD has often been reported. High levels of plasma cholesterol and TAG lead to a high risk of CHD and atherosclerosis. This is the first study to document in detail the association between tea consumption and reduced dyslipidaemia risk in a population in southern China. Accurate measurements of long-term tea exposure involved the use of a validated and reliable questionnaire specifically developed for the southern Chinese population. In addition to recording the frequency of tea consumption, we obtained information on duration of tea drinking and mean quantity of dried tea leaves brewed. These exposure measures are important to determine the effect of habitual tea consumption. Moreover, the Shantou population consumes various types of tea, which allowed us to investigate their individual effects on dyslipidaemia risk, so the habitual tea consumption pattern would not be affected by the case–control status. We found that people who drank green, oolong and black tea daily had a significantly lower risk of dyslipidaemia and the risk was further reduced with long-term and increased-dose exposure to tea. Most importantly, the present results are robust and consistently demonstrate a dose–response relationship between duration of oolong tea consumption and blood TC, TAG and LDL-C levels but not HDL-C levels.
The protective effect of tea that we found is supported by experimental studies( Reference Akinyanju and Yudkin 8 – Reference Bursill and Roach 10 ). The effect is mainly due to the polyphenols present in tea. Tea polyphenols have various biological activities, including anti-inflammatory, anti-mutagenic, antioxidative and anti-tumour effects( Reference Wiseman, Balentine and Frei 28 – Reference Kurahashi, Sasazuki and Iwasaki 31 ). Recent studies( Reference Kuo, Weng and Chiang 23 , Reference Yeh, Chen and Chiang 32 , Reference Huang and Lin 33 ) in human subjects and animals have shown that tea consumption can lower plasma cholesterol and TAG levels. These studies( Reference Kuo, Weng and Chiang 23 , Reference Yeh, Chen and Chiang 32 , Reference Huang and Lin 33 ) have suggested that tea intake may protect against dyslipidaemia by suppressing fatty acid synthase. Tea polyphenols have been demonstrated in human breast carcinoma MCF-7 cells and hepatocellular carcinoma Hep-G2 cells( Reference Yeh, Chen and Chiang 32 ).
Moreover, the order of the effect on the risk of dyslipidaemia for the three tea types is as follows: green tea>oolong tea>black tea. During fermentation, catechins are converted into the major black tea polyphenolic components theaflavins and thearubigins. The content of catechins, especially (–)-epigallocatechin, is higher in non-fermented green tea leaves than in partially fermented oolong tea leaves and fully fermented black tea leaves( Reference Cabrera, Gimenez and Lopez 34 ). Animal studies have suggested that green tea catechins reduce lipid absorption in the intestines, promote faecal excretion of cholesterol and inhibit enzymes involved in hepatic cholesterol synthesis( Reference Ikeda, Imasato and Sasaki 35 , Reference Bursill, Abbey and Roach 36 ).
Although green tea had the largest effect on the risk of dyslipidaemia, only oolong tea could reduce the levels of all lipids: H-TC, H-LDL, H-TAG and especially L-HDL. Besides catechins, oolong tea also contains high-molecular weight polyphenols such as OTPP produced during the process of semi-fermentation. It has been demonstrated that catechins can lower plasma TAG, TC and LDL-C levels but not HDL-C levels by inhibiting the activity of lipase( Reference Kuo, Weng and Chiang 23 , Reference Yang, Wang and Chen 37 ). That oolong tea increases HDL-C levels is inconsistent( Reference Kuo, Weng and Chiang 23 , Reference Yang, Wang and Chen 37 – Reference Matsuda, Chisaka and Kubomura 39 ). A previous animal study has found that oolong tea could increase HDL-C levels( Reference Matsuda, Chisaka and Kubomura 39 ), which may be related to the regulative action of oolong tea high-molecular weight polyphenols in lipoprotein metabolism. HDL can transport cholesterol from the surrounding tissues back to the liver for recycling or excretion in the form of bile acid and thus lower the levels of TC and LDL-C in the blood plasma. High levels of plasma cholesterol, LDL-C and VLDL-cholesterol are associated with a high risk of CHD and atherosclerosis( Reference Mukamal, Maclure and Muller 5 , Reference Jain, Kathiravan and Somani 6 ). CHD risk is positively associated with TC and LDL-C levels and inversely associated with HDL-C levels in middle-aged people( Reference Boshuizen, Lanti and Menotti 40 , Reference Iso, Naito and Sato 41 ).
Shantou people mainly use locally grown tea leaves, which belong to the semi-fermented oolong tea series. Only this type of tea can offer the colour, fragrance and flavour required for Gongfu tea. The way Gongfu tea is prepared including the use of small tea sets probably contributes to the maintenance of the higher concentrations of polyphenols in Gongfu tea, which might explain why Gongfu tea has a greater lowering effect on lipids. Oolong tea varieties mostly used are Iron Buddha, narcissus and phoenix tea. Oolong tea has many health benefits in humans, such as reduction of CVD risk and antioxidant, anti-obesity and hypolipidaemic effects( Reference Han, Takaku and Li 42 – Reference Kuroda and Hara 44 ). This tea contains numerous kinds of polymerised polyphenols, the characteristic feature of oolong tea components, which are derived from tea catechins by the semi-fermentation process. The polymerised polyphenols present in oolong tea are not found in green tea and are different from those in black tea. In a previous in vivo study, OTPP have been found to significantly suppress both lymphatic TAG absorption and serum TAG elevation when a high-lipid diet is consumed( Reference Toyoda-Ono, Yoshimura and Nakai 45 ). The OTPP can also inhibit lipase activity by influencing intestinal absorption of dietary lipids, which is essential for lipid absorption, and faecal lipid excretion, without the side effects of polymerised polyphenols( Reference Toyoda-Ono, Yoshimura and Nakai 45 ). The inhibitory activity of OTPP on lipase is stronger than that of the total extracts derived from green tea in vitro, which could be explained by the ester-bound galloyl moieties( Reference Nakai, Fukui and Asami 22 ).
Dyslipidaemia is a complex systemic disorder, influenced by both lifestyle and dietary factors. Several randomised trials that did not control for diet did not reveal an effect of tea consumption on lipid levels( Reference Bingham, Vorster and Jerling 16 , Reference McAnlis, McEneny and Pearce 17 ). Therefore, we investigated dietary and lifestyle factors to determine the effect of tea consumption on dyslipidaemia. Dietary assessment was based on subject self-reporting with a 125-item semi-quantitative FFQ developed for the southern Chinese population( Reference Ke, Toshiro and Fengyan 25 , Reference Song, Toshiro and Li 26 ). We found smoking, alcohol drinking status, sitting time, physical activity and dietary intake of vegetables, fruit, soya food, milk, animal offal, lard and pickle to be associated with dyslipidaemia. All these variables were accounted for and adjusted in the multivariate logistic regression analyses when analysing the relationship between tea consumption and dyslipidaemia. We also chose patients with newly diagnosed dyslipidaemia to control for recall bias and used face-to-face interviews to increase the response rate and improve the accuracy of answers. In addition, all the interviews were conducted by the same investigator to eliminate interviewer bias.
Conclusions
Oolong tea is the most widely consumed beverage in Shantou. We found that long-term oolong tea consumption can reduce the risk of H-TC, H-TAG and L-HDL in the Shantou population. Our data will be useful for planning effective education programmes to prevent CHD and other CVD. Nevertheless, further replications of the study are recommended before generalising the findings to other populations and countries.
The present study was supported by grants from Science and Technology Plans of Guangdong Province (2011B031800209), Medical Scientific Research Foundation of Guangdong Province (A2010388), the Joint Research Project of Clinical and Basic Courses, Shantou University Medical College (2010). The contents reflect only the authors' views. The administration of Science and Technology of Guangdong Province, Medical Scientific Research Foundation of Guangdong Province and Shantou University Medical College had no role in the design and analysis of the study or in the writing of this article.
The authors' contributions are as follows: D. Y. and Z. Z. conducted the survey, carried out the statistical analysis and drafted the manuscript; X. T. contributed to the conception and design of the study; Y. C., Y. L., X. L., S. L. and Y. C. coordinated the study and were involved in the questionnaire survey and anthropometric parameter measurement; Q. Z. contributed to the conception and design of the study and revised the manuscript. All authors read and approved the final manuscript.
None of the authors has any conflicts of interest to declare.






