



Introduction
Most market-oriented welfare states including Canada, the United States, Australia and the United Kingdom rely on a market model of early childhood education and care (ECEC) with little direct government service delivery (White & Friendly, Reference White and Friendly2012). Within such systems, legislation and regulation tend to be premised on the assumption that parents are informed consumers who are capable of exercising quality assurance and ‘voting with their feet’ should they be unhappy with the quality of their child's care. However, extant research finds that parents often lack information and are unable to accurately engage in assessments of quality care (Zellman & Perlman, Reference Zellman and Perlman2006; Howe et al., Reference Howe, Jacobs, Vukelich and Recchia2013). More specifically, numerous studies have shown that parents tend to overestimate the quality of care their children receive, and their ratings of their child's programme are unrelated to observed quality characteristics (Cryer & Burchinal, Reference Cryer and Burchinal1997; Mocan, Reference Mocan2007; Bassok et al., Reference Bassok, Markowitz, Player and Zagardo2017).
In this article, we present the results of an experiment that tests whether providing parents with information about the regulation and oversight of different types of ECEC options influences their decisions for types of care. Using a choice-based conjoint survey methodology, our intervention aims to influence parental selection of types of ECEC (Laurin et al., Reference Laurin2015). Choice-based conjoint analyses provide insight into participants’ quasi-behavioural choices, as they are provided hypothetical choices for ECEC based on real-life scenarios. After receiving information about regulation and oversight, we expected that parents would be less likely to select ECEC settings that are unlicensed (and therefore have no proactive oversight) which are generally of poorer quality and have been associated with higher risks to child safety (Japel et al., Reference Japel, Tremblay and Côté2005; Li-Grining & Coley, Reference Li-Grining and Coley2006; Bassok et al., Reference Bassok, Fitzpatrick, Greenberg and Loeb2016).
Given the importance of high-quality ECEC on various developmental outcomes (Arteaga et al., Reference Arteaga, Humpage, Reynolds and Temple2014), especially in children from lower-income families (Weiland & Yoshikawa, Reference Weiland and Yoshikawa2013), it is important to understand the informational constraints parents face when choosing ECEC. Market-driven ECEC policies assume that parents are informed consumers of ECEC, able to navigate the regulatory system and with the capacity to detect aspects of quality they hope for their children. However, research has found that parents are largely misinformed or uninformed about quality (Howe et al., Reference Howe, Jacobs, Vukelich and Recchia2013) and even what types of care (licensed or unlicensed) their children attend (Varmuza et al., Reference Varmuza, Perlman and White2019). Prior research has demonstrated information effects on participant preferences in other areas, such as modifying their selection of environmental and educational policies and programmes (Shpancer et al., Reference Shpancer, Bowden, Ferrell, Pavlik, Robinson, Schwind, Volpe, William and Young2002; Lergetporer et al., Reference Lergetporer, Schwerdt, Werner, West and Woessmann2018). Other research has found that information is only useful when direct assistance is also provided (Bettinger et al., Reference Bettinger, Long, Oreopoulos and Sanbonmatsu2012). Thus, it is important to understand the barriers parents face in making these informed decisions and to assess whether information can assist parents in selecting higher quality care for their children.
This study was carried out in the city of Toronto, Canada. We evaluated the effectiveness of information given to half of our survey group of 682 parents aged 25–51. The treatment condition informed parents about the basic features of the main three types of regulated ECEC options: licensed ECEC centres, licensed home childcare and unlicensed home childcare. Parents were recruited through the City of Toronto's website and drop-in centres in lower-income neighbourhoods. Before beginning the survey, participants were randomly assigned into either a treatment (information) or control (no information) group.
We found that, on aggregate, receiving information did not affect parents’ choices for types of ECEC. However, we find a treatment effect on lower income and lower income/education parents. For these parents, receiving information about the regulation and oversight of the different types of ECEC providers altered the parents’ rank-ordered choices of different types of care, preferring the most regulated care available.
This study makes three primary contributions. First, it contributes to the literature on human decision-making in information and other resource-constrained environments (Ariely, Reference Ariely2000; Pedroni et al., Reference Pedroni, Frey, Bruhin, Dutilh, Hertwig and Rieskamp2017), including decisions around ECEC (Harbach, Reference Harbach2016) through the use of a quasi-behavioural conjoint survey (Kensinger Rose & Elicker, Reference Kensinger Rose and Elicker2008). This method, in combination with the randomized experimental intervention, allows for causal inferences about the effectiveness of nudges (Leeper et al., Reference Leeper, Hobolt and Tilley2020; Mertens et al., Reference Mertens, Herberz, Hahnel and Brosch2022). Second, we contribute to the literature on information effects in particular on learning and informed choice (Synder et al., Reference Synder, Hamilton, Mitchell, Kiwanuka-Tondo, Fleming-Milici and Proctor2004; Roberto et al., Reference Roberto, Larsen, Agnew, Baik and Brownell2010; Allcott, Reference Allcott2011; Ferraro et al., Reference Ferraro, Miranda and Price2011; Dunlop & Radaelli, Reference Dunlop and Radaelli2013), investigating the promise of information as a source of influence on decision making for different groups of individuals. Third, we contribute to the limited literature on lower-income parent's choices for types of ECEC (Tang et al., Reference Tang, Coley and Votruba-Drzal2012; Lin & Dunnett, Reference Lin and Dunnett2018) by examining whether providing information to this group changes their quasi-behavioural choices. We discuss the implications of our findings for policymakers and future research in the conclusion.
Choice, information and parental decision-making in ECEC
Children across OECD countries spend a substantial proportion of their day being cared for by someone other than their parents. In 2017, on average, 35% of children ages 0–2 were enrolled in early childhood education and care services (ECEC) in OECD countries, as were 87% of children ages 3–5 (OECD, Family Database, 2019, PF3.2.A; PF3.2.E). Access to high-quality ECEC provides opportunities to enhance children's health, wellbeing and developmental outcomes (Arteaga et al., Reference Arteaga, Humpage, Reynolds and Temple2014), particularly for children from families of lower socioeconomic status (SES; Weiland & Yoshikawa, Reference Weiland and Yoshikawa2013). However, the options from which parents can choose from vary by jurisdiction. Whereas many European countries both finance and deliver ECEC services, market-oriented welfare state jurisdictions have ECEC policies and programmes that include more limited public finance and a wider range of permitted forms of care, including home childcare services that also tend to be much more variable in their quality and safety. Even among similarly market-oriented ECEC systems, the amount of regulation is variable. Australia, the UK (including Scotland and Wales) and New Zealand all regulate home childcare arrangements. Meanwhile, in Canada, the United States and Ireland, a large portion of children are regularly cared for in unlicensed and generally unregulated ECEC settings. While quality care is possible in both licensed and unlicensed environments, research has shown that regulated providers are generally rated as providing higher quality care (Pence & Goelman, Reference Pence and Goelman1991; Galinsky et al., Reference Galinsky, Howes, Kontos and Shinn1994; Bassok et al., Reference Bassok, Fitzpatrick, Greenberg and Loeb2016) and unlicensed providers have been shown to provide some of the worst care (Galinsky et al., Reference Galinsky, Howes, Kontos and Shinn1994; Japel et al., Reference Japel, Tremblay and Côté2005).
What does this mean for the intersection of information and parent decisions? In ECEC systems that regulate all care providers (including at-home care providers/childminders), parent decision-making can be disentangled from basic questions of quality and safety. By comparison, in most North American jurisdictions, the regulatory framework relies on parents-as-consumers as a source of quality assurance. In the absence of a strong regulatory and compliance system, parents are responsible for monitoring and evaluating the services being delivered, and the identification of unsafe ECEC environments is largely complaints driven (White et al., Reference White, Perlman, Davidson and Rayment2019).
Preserving parent choice, as a rationale for under-regulation, is based on an assumption that parents make decisions about child care as comprehensively rational consumers of ECEC (Cryer & Burchinal, Reference Cryer and Burchinal1997). A pure market-based approach suggests that parents make ECEC decisions through the optimization of cost by balancing the benefits and possible shortcomings of pursuing each or any ECEC route; yet, behavioural economics and psychology research, as well as a growing literature in behavioural public policy, challenges this assumption.
Regardless of the policy area, there is systematic evidence that individuals face psychological constraints that impair their ability to engage in comprehensively rational decision making within market-based systems. This is particularly true when consumer assessments of a good or service is based, in whole or in part, on the relationship they form with that service (Aggarwal, Reference Aggarwal2004). While some consumer decisions are based solely on the quid pro quo of an economic exchange (e.g., purchasing gum), and as such not imbued with emotional or social characteristics, decisions about ECEC are highly emotive. In trust relationships, as opposed to an exchange relationship, consumers develop some affinity or reciprocal relationship with the good or service being provided (Aggarwal, Reference Aggarwal2004). As such, consumers may not be able to effectively assess risk or judge quality (Kahneman et al., Reference Kahneman, Knetsch and Thaler1991; Gilovich et al., Reference Gilovich, Griffin and Kahneman2002).
Once parents decide about ECEC care, they may be less likely to update their preferences and decisions to reflect new information; the social relationship that develops with providers may lead parents to suspend or delay rational cognitive assessments of risk. Parents are likely to be subject to motivated reasoning (Kunda, Reference Kunda1990) they may be motivated to think favourably of their child's provider as it is likely psychologically difficult for them to think that they have provided their child with anything but good quality care. Sunk cost factors may also play a role: after conducting a full search and placing a child with a provider, it may be psychologically difficult to pull a child from that provider (Arkes & Blumer, Reference Arkes and Blumer1985).
Research suggests that parents are more like ‘constrained consumers’ when selecting ECEC for their children (Varmuza et al., Reference Varmuza, Perlman and White2019). Parents face considerable constraints that shape their decisions beyond that of cost, including informational constraints, logistical constraints (e.g., work schedule, location of care relative to work or home) and issues of scarcity (Shah et al., Reference Shah, Mullainathan and Shafir2012).
Extant research has consistently found that parents are often uninformed or misinformed on a range of aspects relating to ECEC such as the types and importance of developmental programming (Botey et al., Reference Botey, Vinturache, Bayrampour, Breitkreuz, Bukutu, Gibbard and Tough2017; Varmuza et al., Reference Varmuza, Perlman and White2019), leading to investigations of why parents are uninformed (Shpancer et al., Reference Shpancer, Bowden, Ferrell, Pavlik, Robinson, Schwind, Volpe, William and Young2002). One of the possible mechanisms is the complexity and range of factors parents must consider, which are layered on top of any structural barriers they may face.
One of the most important aspects of ECEC settings is the quality within it. Parents have been found to rate their care as higher quality than the trained observers using standardized measures assessing ECEC quality (Cryer & Burchinal, Reference Cryer and Burchinal1997). For example, Zellman and Perlman (Reference Zellman and Perlman2006) found that parents consistently ranked their child's ECEC provider highly across domains of quality although quality assessment measures reported significant problems. Therefore, the lack of understanding related to the aspects of quality within an ECEC context can act as a barrier.
The reasons for parents being mis/uninformed are more multi-faceted. Examples of relevant factors likely include the quality of communication between ECEC providers and parents (Shpancer et al., Reference Shpancer, Bowden, Ferrell, Pavlik, Robinson, Schwind, Volpe, William and Young2002), how much access parents are granted to ECEC sites, or how much time parents have to spend observing the interactions between their children and their providers (Perlman & Fletcher, Reference Perlman and Fletcher2012). ECEC providers themselves might not be making information publicly available, especially in unlicensed settings.
It is thus important to understand how information barriers might be related to parents’ choices in selecting types of ECEC. Experiments that present information on the importance of a decision can nudge participants to be more accurate in their decision making by motivating them to engage in more complex decision making (Kunda, Reference Kunda1990, p. 481). Providing information has been found to change public preferences on a range of important decisions, including the environmental policies people support (Shpancer et al., Reference Shpancer, Bowden, Ferrell, Pavlik, Robinson, Schwind, Volpe, William and Young2002), the distribution of public spending for educational resources (Lergetporer et al., Reference Lergetporer, Schwerdt, Werner, West and Woessmann2018) and even preferred travel destinations (Lavín et al., Reference Lavín, Gelcich, Lerdón and Bustos2016). However, there is also evidence that more information does not shift prior attitudes in citizens (Nyhan & Reifler, Reference Nyhan and Reifler2010) or political officials (Blom-Hansen et al., Reference Blom-Hansen, Baekgaard and Serritzlew2016). Bettinger et al. (Reference Bettinger, Long, Oreopoulos and Sanbonmatsu2012) found that providing information related to receiving college financial aid did not increase their children's rate of college attendance without providing direct assistance on the process. In the case of parent decision-making around ECEC, even in instances where providers have been found to be violating the rules, some parents respond with concern at the possibility of closure (Monsebraaten & Ballingall, Reference Monsebraaten and Ballingall2013). Given some parents’ constrained choice set, they may be forced to accept suboptimal options even when informed of them.
Parental choices for ECEC may change if parents are more informed of their options for ECEC; however, to date, little research has focused on the effects of information on parental decision-making related to the type of ECEC chosen for their children. In this article, we present the results of an experiment where parents are provided information about the differences between types of ECEC arrangements, as they relate to staff training, child-to-staff ratios and provider oversight. We investigate whether the provision of information changes parental decision-making for the type of ECEC in a simulated decision environment.
The market for ECEC in Canada
In Canada, nearly half of parents report sending their children to some form of out-of-home care (Sinha, Reference Sinha2014). As in several other liberal welfare states, ECEC services are regulated such that a portion of legal childcare is provided by unlicensed home care providers. ECEC services outside of the home can be legally provided in a (1) licensed childcare centres or ECEC centres; (2) licensed home childcare or (3) unlicensed home childcare. ECEC centres operate in a variety of locations (e.g., churches, schools, private locations and so on), whereas both licensed and unlicensed home childcare operate within the provider's place of residence (Ferns & Friendly, Reference Ferns and Friendly2014; Government of Ontario, 2019). Licensed ECEC – whether at home or in a centre – requires providers to follow clear regulations including health and safety requirements and other structural indicators such as educator qualifications (Government of Ontario, 2018). Licensed care environments are also subject to regular oversight to ensure compliance, although there are differences in how frequently and how comprehensive oversight is across the two types of licensed ECEC settings. In Ontario, where this study took place, licensed ECEC centres are reviewed directly by the Ministry of Education to ensure that both safety and quality standards are maintained. Licensed home care providers are indirectly monitored, as they are inspected by home childcare agencies that are licensed through the ministry (Government of Ontario, 2019). Meanwhile, unlicensed home care providers are not subject to any regular oversight and monitoring unless a complaint is made to the ministry. Little is known about the quality of unlicensed care but research in both the US and Canada has suggested that licensed centres have less variability in quality ECEC provision compared to both licensed and unlicensed home care (Goelman et al., Reference Goelman, Pence, Lero, Glick and Berkowitz1993; Japel et al., Reference Japel, Tremblay and Côté2005; Li-Grining & Coley, Reference Li-Grining and Coley2006; Bigras et al., Reference Bigras, Bouchard, Cantin, Brunson, Coutu, Lemay, Tremblay, Japel and Charron2010; Bassok et al., Reference Bassok, Fitzpatrick, Greenberg and Loeb2016).
Across all provinces in Canada unlicensed home care is legal so long as providers adhere to minimal standards (White et al., Reference White, Perlman, Davidson and Rayment2019). In Ontario, the most substantive requirements is that providers are restricted to providing care for a maximum of five children, with no more than two under the age of two (Government of Ontario, 2019). Because these providers operate without a license and are not required to register with the government, it is not clear how pervasive they are in the ECEC market and how many children are in unlicensed care (White et al., Reference White, Perlman, Davidson and Rayment2019). However, recent research finds that many more parents report that their children are in licensed settings than is possible, suggesting at least a modestly sized market for unlicensed care (Varmuza et al., Reference Varmuza, Perlman and White2019).
Understanding influences on parental choices for ECEC types
Despite conceptualizing parents as consumers, little is known about parents’ choices and how their decisions interact with information vis-à-vis options for ECEC. Parents are not homogeneous consumers of ECEC, and parent characteristics, preferences, and constraints (including time and financial constraints) may shape decisions around care. The literature to date has produced often inconsistent findings that may shape decisions around care at least in part due to the methodological challenges associated with capturing parents’ choices and decision-making (Davidson et al., Reference Davidson, Burns, Hampton, White and Perlman2021). Surveys that pool from specific demographics often fall short on capturing the constraints that create discrepancies between what parents say they want and what they choose. For example, research has shown that highly educated parents often place greater importance on ECEC care options that are described as cognitively stimulating and developmentally appropriate; these parents are more likely to opt for centre-based care (Cryer et al., Reference Cryer, Tietze and Wessels2002; Huston et al., Reference Huston, Chang and Gennetian2002). However, it is also the case that these parents are more likely to have the financial resources needed to pay for centre care which is generally more expensive that home care. In addition, these parents are more likely to have the type of white-collar work schedule that aligns with the centre hours of operation (Kimmel & Powell, Reference Kimmel and Powell2006). Meanwhile, lower-income parents are often employed in jobs with variable work schedules or high rates of turnover, making flexible arrangements preferable (Ahituv & Lerman, Reference Ahituv and Lerman2007).
While research shows that there are a range of preferences and structural constraints that shape parental decisions on ECEC care, much less is known about the relationship between the extent to which parents are informed about the ECEC services and their decisions around care. For example, it is possible that parents are unaware of regulatory structures entirely and are unable to distinguish reliably between licensed and unlicensed care, particularly in a home care environment. Pence and Goelman (Reference Pence and Goelman1987), for example, found that parents who report preferences for home-based care report wanting a relationship with the provider in a home-like setting. These parents were also more likely to report feeling guilty about leaving their children but were significantly less likely to indicate that different aspects of quality are an important characteristic in their selection of ECEC services. The effects of access to information have been studied in the context of language proficiency; one study of African immigrant parents in the United States found that immigrant families with more limited English language skills had greater difficulty communicating their care needs and accessing information about local ECEC services. As such, parents in this study were more likely to opt for informal or relative care over centre-based care (Obeng, Reference Obeng2007). Researchers need to start disentangling whether parents are choosing a home-like setting at the expense of quality or whether they are not informed about the importance and implications of different forms of care for ECEC safety and quality.
This study examines the differences in responses to a conjoint exercise on parents’ choices between the randomly assigned treatment and control groups. The intervention group was informed about ECEC types and their regulations through an informational session while the control group was not. The objectives of this research were to test (1) whether there is an effect of providing information about the regulation of ECEC on parent choices for types of ECEC and (2) whether any observed effects of the provision of information differ depending on parent demographic characteristics. Specifically, we hypothesized that the treatment group receiving information on childcare would display different revealed preferences in the conjoint scenarios that followed. We expected that priming parents to think about the differences in types of ECEC would result in them paying more attention to that attribute and preferring the most-regulated care scenario when making quasi-behavioural decisions as part of our conjoint survey. We furthermore expected that information effects would be more pronounced for lower income/lower-education parents.
These hypotheses align with past research has shown that socioeconomic status affects ECEC decisions made by parents. Parents with higher socioeconomic status (including higher levels of education and higher levels of income) are more likely to indicate that the quality of ECEC is the most important factor in their care decisions (Lowe & Weisner, Reference Lowe and Weisner2004; Kimmel & Powell, Reference Kimmel and Powell2006) and are more likely to place their children in high-quality care, even in universalist ECEC systems (Camehl et al., Reference Camehl, Schober and Spiess2018; Alexandersen et al., Reference Alexandersen, Zachrisson, Wilhelmsen, Wang and Brandlistuen2021). Parental preferences are not independent of knowledge, and higher SES parents are generally thought to be informed about the different dimensions of ECEC quality and types of care (Cryer et al., Reference Cryer, Tietze and Wessels2002; Becker & Schober, Reference Becker and Schober2017; Stahl et al., Reference Stahl, Schober and Spiess2018; Alexandersen et al., Reference Alexandersen, Zachrisson, Wilhelmsen, Wang and Brandlistuen2021). Higher SES parents can rely on well-informed social networks to ease access to information (Chaudry, Reference Chaudry2004) and may engage in more effective search strategies when looking for care (Vandenbroeck et al., Reference Vandenbroeck, De Visscher, Van Nuffel and Ferla2008). Meanwhile, informational asymmetries tend to be more pronounced among lower SES parents who are more constrained in their time or ability to search for information about ECEC care options (Cryer et al., Reference Cryer, Tietze and Wessels2002; Mocan, Reference Mocan2007; Camehl et al., Reference Camehl, Schober and Spiess2018).
Experimental design
We employed a conjoint survey to evaluate the treatment effects of information intervention (Hainmueller et al., Reference Hainmueller, Hopkins and Yamamoto2014). We randomized the treatment condition to identify the causal effects of the intervention on parents’ choices for types of ECEC. The treatment included information on the regulatory oversight across the three types of ECEC (Figure 1).
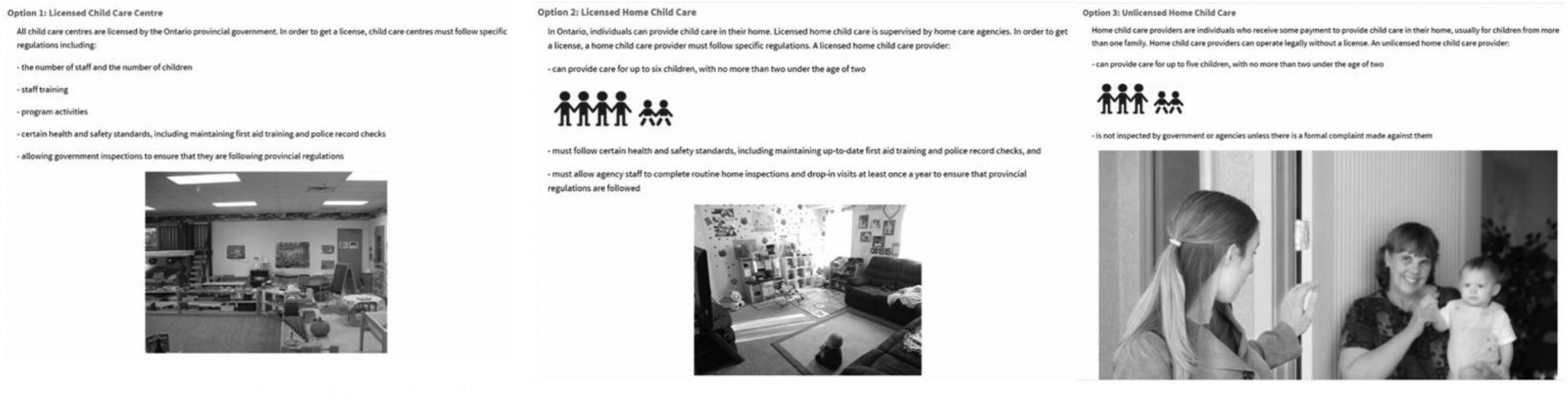
Figure 1. Information intervention, describing the basic features of the three types of legal ECEC options available in the province of Ontario
A conjoint survey was developed to understand parents’ choices for ECEC. It was developed based on an extensive literature review and informal interviews with parents. Early versions of the conjoint survey were piloted with parents accessing assistance at the City of Toronto Children's Services Division to ensure questions were clear and reflected the trade-offs parents encounter when selecting ECEC. In the conjoint survey, participants were instructed to select one of three ECEC scenarios that were provided to them. The ECEC scenarios were based on eight attributes of care and were designed to capture either (1) quality indicators of care such as type, caregiver training, caregiver interactions and physical space; and (2) restrictive indicators for accessing care such as cost, location, flexibility and full/part-time care (Corcoran & Steinley, Reference Corcoran and Steinley2017). Each attribute of care varied across three levels (for example, the attribute ‘location’ was assigned three levels indicating the length of time it would take to reach the ECEC provider – from a 5–14 minute commute on the low end, a 15–29 minute commute as the moderate range and a 30–40 minute commute on the high end). ECEC scenarios were randomly generated using the Sawtooth software; in each turn, three hypothetical ECEC providers were generated based on five of the eight attributes. We limited the number of attributes to five to contain the burden to participants of weighing multiple attributes; however, all participants selected scenarios that included all eight attributes over the course of 12 choice exercises. Of the three hypothetical ECEC settings provided in each choice exercise, participants were asked to select their preferred option. Participants could also select ‘none’ as an option indicating that given available options, they would prefer no ECEC (see Figure 2).

Figure 2. An example of a 'decision scenario' presented to parents during the conjoint survey
In this article, we investigate the impact on information on the attribute of ‘type of care’ and its three levels (i.e., licensed ECEC and licensed and unlicensed home childcare), as this is the attribute most closely aligned with the treatment that was part of the current study. For a full discussion of the broader conjoint results, see Davidson et al. (Reference Davidson, Burns, Hampton, White and Perlman2021), and for an examination of how the quasi-behavioural choices of parents relate to their stated preferences, see Saleem et al. (Reference Saleem, Burns, Davidson, Hampton, White and Perlman2021). In the current study, we examine the results of a randomized intervention relative to participant demographics such as their highest level of education and household income.
Data and methods
This study surveyed parents in Toronto, which is the largest city in Canada, with a population of approximately three million. Toronto is very diverse and multicultural as slightly more than half of the population report being a visible minority (51.5%) or born outside the country (51.2%; City of Toronto, 2017). Accessing ECEC in Toronto is challenging as the cost of ECEC is the highest in the country and waitlists for public subsidies are long (Monsebraaten & Ballingall, Reference Monsebraaten and Ballingall2013). Parents can choose across three types of ECEC options including (1) licensed ECEC, (2) licensed home childcare and (3) or unlicensed care. Both licensed centre and home care spaces are often hard to secure, with long waitlists and high costs associated with care. For the purposes of the study, we limited the options that parents could choose to the three most utilized options within the traditional ECEC ‘market’; other options, such as nannies, occasional care or family care, were not included.
Recruitment and randomization procedure
Participants were recruited through the City of Toronto website between August 2018 and February 2019. To diversify our sample, we also recruited participants attending a drop-in programme located in lower-income neighbourhoods, which took place between June and August 2019. Study participants were randomly assigned to a treatment or control group through the survey design. The participants assigned to the treatment group received a brief explanation of the oversight of the three types of ECEC settings in Ontario (licensed centre care, and licensed and unlicensed home care) before completing the conjoint scenarios and survey. To investigate whether the treatment was administered randomly between participants, a series of chi-square tests of independence were conducted on demographic characteristics (Table 1). There were no differences found in demographic characteristics between the treatment and control groups.
Table 1. Differences in demographic characteristics.

Data analysis plan
Missing data
A total of 1006 participants started the survey. As a minimum criterion for inclusion, participants needed to complete at least 9 out of the 12 conjoint exercises. For those who did so, additional criteria were then imposed for the purpose of ensuring adequate data quality. These included identifying participants who appeared to have disengaged from the choice exercise. Specifically, participants were removed from the sample if they answered ‘None’ for more than eight conjoint scenarios, had a patterned response (e.g., 123123123), had more than five of the same responses in a row (e.g., 11111) or if their last four answers were the same. A total of 282 participants were removed, leaving a total of 724 participants. An analysis of missing data was then conducted on the remaining sample of 724 participants. Missing data analysis was first conducted on the participant level. A total of 42 participants were removed from the dataset because they had data for less than 70% of the variables used in the current study. Missing data analysis was then conducted by variable on the remaining sample of 682 participants. The variables in the dataset had between 0 and 12.2% missing data. The variables that contained the most missing data were participants’ age (11.4%) and income (12.2%). The variables that were used in the analyses addressing the research questions in the study had between 0 and 7% of missing data. A case-wise deletion strategy was implemented and the reporting of the sample sizes for each analysis is included in the results.
Conjoint analysis: attribute importance and utility scores
Choice-based conjoint analyses require participants to make selections between randomly generated choice sets, that in this case make-up an ECEC ‘scenario’. Across each scenario, participants must make trade-offs regarding the choices available to them and their internalized preferences for some attributes and dislike towards others. In the ECEC scenarios provided to participants, there are one of three features for each of the five attributes that reflects real-life aspects of ECEC that parents make when choosing child care for their children. Once all scenarios are completed, a Hierarchical Bayesian (HB) estimator (Sawtooth Software, 2021) is used to estimate an individual's utility (i.e., attractiveness for a specific option related to an ECEC scenario) by estimating the sample's overall utility score for a specific feature and then calculating how different the individual is from the sample (see additional information about the analyses used in this article in Appendix A). For example, a respondent who cares a lot about regulatory oversights on the type of care their child receives will consistently select options in which the ECEC is licensed and avoid options in which the care is unlicensed.
The choice-based conjoint design, traditionally used within marketing research, was selected to examine the effects of information on parental selection of ECEC, as an alternative to traditional ranking and self-report surveys largely due to the quasi-behavioural nature of the design and the resulting implications. Experimental studies that allow parents to select actual ECEC settings to send their children would be extremely difficult to implement. As such, creating hypothetical scenarios (i.e., quasi-behavioural choices), that reflect key attributes parents’ trade-off when making actual decisions, to examine the effect of information on their preferences for ECEC provides an informative, more practical alternative. This technique produces a quantifiable score on what attributes (i.e., type of care) and utilities of each attribute (i.e., licensed centre care) are most important, relative to other attributes and utilities to the individual participant.
Effect of regulatory information on parents’ choices for types of ECEC
The following analyses were used to answer our research question about whether there is an effect of providing information about the regulation of ECEC on parents’ choices for types of ECEC: (1) conjoint analyses and (2) a series of independent sample t-tests, with bootstrapping. First, to determine what parental quasi-behavioural choices for ECEC are, a conjoint analysis on 12 scenarios was conducted with the Sawtooth Software that uses a Hierarchical Bayesian (HB) estimator to enable the estimation of individual part-worth utilities. This analysis produced two measures that were used in this study: (1) part-worth utilities and (2) attribute importance. The first measure, part-worth utilities, captures the level of responsiveness a participant has to an attribute. For example, a participant who cares about the cost of ECEC will select options with the lowest cost and void the options with the greatest cost. The calculation of the individual utility models was zero-centered and aggregated across the entire sample to allow comparability across the attributes of the ECEC preferences used in the conjoint scenarios. As the output from this analysis, the scores were produced per individual on the importance placed on the type of care compared to other attributes. In these analyses, the larger the range between the minimum and maximum value of an attribute, the more important it was compared to other attributes. The second measure, attribute importance, indicates the percentage that an attribute contributes to a participant's decision. Attribute importance scores are mutually exclusive; therefore, if one attribute has higher importance, it will decrease the importance of other attributes. To investigate whether the information influenced parents’ quasi-behavioural choices (utility scores), a series of t-tests were conducted on the relationship between the intervention and (1) the overall importance of licensing (Attribute Importance) and (2) choices (Utility Scores) for licensed centre care, licensed home care and unlicensed home care. Bootstrapping was applied to check the stability of our results. Statistical significance is determined based on a p < 0.05 cut-off.
Subgroup selection
To examine whether the effects of providing information on the regulation of ECEC differ for families with different demographic characteristics, we generated subgroups of the participant population. Two subgroups were created: (1) lower-income families (lower income) and (2) lower income with lower-education families (lower income/education; Table 2). Participants were categorized as belonging to the lower-income group if their reported family income was lower than the median family income for Toronto residents. The median family income was identified based on the population's household composition, number of children and annual income (Statistics Canada, 2019). The lower-income/education subgroup was selected from the lower-income subgroup with the additional criteria of falling below the median level of education in Toronto. In 2016, 54% of the Toronto population had a college diploma or bachelor's degree (Statistics Canada, 2019). Therefore, participants were classified into the lower income/education if they had less than the median income of Toronto residents and completed a bachelor's degree or below. Assignment to the treatment vs control group was comparable within each of our subgroups. To address the second research question – a series of t-tests, as mentioned above, were conducted to examine quasi-behavioural choices regarding types of ECEC within these two subsamples.
Table 2. Demographic information for each subgroup.

Results
Our sample consisted of 682 parents aged 25–51 with at least one child between preschool age or younger (0–4 years of age). There was a comparable distribution of parents whose youngest child was an infant (32.4%), toddler (27.7%) and of preschool/early childhood age (39.9%). Slightly more than half of the parents had only one child (52.0%).
Parental choices for ECEC
The summary statistic from the conjoint analysis provides participants’ attribute importance values. Utility scores that were produced for each type of care showed a clear preference in both the positive and negative direction. First, there was a large positive preference placed on licensed ECEC centres with a range of scores between 251.6 and −169.4, followed by moderate positive preference licensed home care with a small range of 111.1 to −45.7 and the largest negative preference placed on unlicensed home care with a large range of 149.8 to −260.8 when choosing ECEC.
Effects of information on parental choices for ECEC
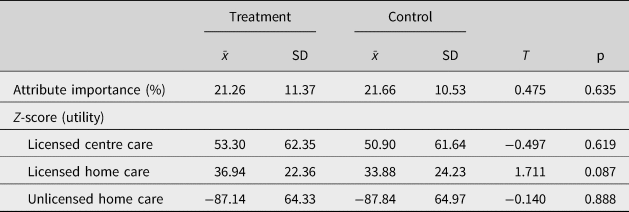
To investigate whether the treatment influenced parent choices of the type of care when accounting for other constraints, we ran independent sample t-tests on the overall attribute importance of the type of care (see Table 3). No effects of treatment were found. There are no statistically significant differences in the relative importance for ECEC type across the two groups, and they exhibit the same rank-ordered importance (licensed ECEC centres > licensed home childcare > unlicensed home childcare). However, as noted in the outset of the article, our sample was both relatively highly educated and high income, a feature of the sample that may undermine the potential effects of information.
Table 3. Quasi-behavioural choices for ECEC by the experimental group (N = 682).
Subgroup analysis: information and parental resources
Subgroup analyses were conducted on the two lower-resourced groups: (1) lower income and (2) lower income/education. We thus investigated whether the information treatment influenced parents who were less ‘well-resourced’ in terms of being lower income and having lower levels of educational attainment, relative to the demographics of the City of Toronto. We conducted a series of independent samples t-tests to determine whether those who received information on ECEC licensing differed in their quasi-behavioural choices related to ECEC types across the two subgroups (Tables 4 and 5). In the absence of information, the control group in the lower income and lower income/lower-education groups preferred licensed home childcare. No statistically significant differences were found in preferences for licensed ECEC centres or unlicensed centres. It is important to note that utility scores are zero-centered at an individual level. Given that the treatment group had lower preferences for licensed home care, they had to have higher preference for one of the other types of care. Therefore, even though the differences between the two groups were not significantly different for the other types of care, the rank-ordered preferences, within the treatment group as compared with the control group, were examined descriptively. Given the qualitative nature of this discussion, we only draw attention to those scores for which the difference between the two groups was not small.
Table 4. Effect of information on choices among lower-income participants (N = 188).

* p < 0.05.
Table 5. Information effects on choices in lower income/education participants (N = 123).

* p < 0.05.
In the absence of information, the control group in the lower income and lower income/lower-education groups preferred licensed home childcare. Specifically, their rank-ordered preferences were: (1) licensed home childcare > (2) licensed centre care > (3) unlicensed home childcare. Within the lower income and education group, the control group had similar preferences for licensed centre and licensed home care, with a clear disfavour of unlicensed care. In contrast, treatment group members, who received information, rank-ordered their preferences as follows (1) licensed centre care > (2) licensed home childcare > (3) unlicensed home childcare. Significant results are limited to licensed home care across both lower income and lower income/education subgroups. This is likely due to greater heterogeneity at the ends of the spectrum (i.e., the most vs least preferred).
Discussion
In market-oriented ECEC systems, parents are expected – and ultimately need – to make informed decisions when selecting ECEC services for their children. We know from existing research, however, that parents often lack information about the degree of regulation and oversight of types of care available to them (Varmuza et al., Reference Varmuza, Perlman and White2019) and are themselves not as discerning of quality as outside observers (Cryer et al., Reference Cryer, Tietze and Wessels2002). This study demonstrates that providing information has different effects on participants’ preferred type of care across different levels of income and education. Parents with lower income and educational attainment who are given information about licensing respond differently than parents with similar income and educational attainment who are not given information.
We surveyed 682 parents aged 25–51 with at least one child between preschool age or younger (0–4 years of age). There was a fairly even distribution of parents whose youngest child was an infant, toddler and of preschool/early childhood age. Information about government oversight of the different types of ECEC available in Ontario, Canada, was provided to the treatment group. We found no effects of the treatment on the entire sample. However, the information did have small but meaningful effects on choices for types of ECEC within the lower income and lower income/education subgroups. Receiving information caused lower income and lower-education parents to prefer licensed home care providers less. In addition, we found some interesting information effects with respect to the nature of the parents’ choices for the type of ECEC care. In both the lower income and lower income with lower-education subgroups, there was a significant decline in the relative choices that participants made regarding licensed home care. This difference points to the most important finding in our study: for our lower-income group, parents exposed to information about licensing placed higher importance for licensed home care, compared with those who did not receive information. This was even more pronounced for the subgroup of lower income, lower-education parents. Furthermore, the rank-ordered preferences in the treatment group preferred licensed ECEC centres more than the other types of care. This finding is particularly notable, as lower income and lower income/education parents face overcoming strong cost preferences away from this type of care; licensed centre care is – across the board – the most expensive form of care (a feature that was maintained in the conjoint scenarios). Further research is needed to uncover why this is so. It is unclear whether there is an information effect – that is, the receipt of information changes parental choices – or a priming effect – that parents make these choices generally, but in the absence of being reminded, are more attuned to other factors such as cost. As well, paradoxically, the information treatment may have worked to somewhat legitimize unlicensed home childcare as an option for parents, reminding parents that unlicensed does not mean illegal. In the first subgroup analysis (lower income), the utility spread between most preferred and least preferred option is less pronounced in the group with the information treatment.
The results of this study have important implications for our understanding of how (and how well) parents navigate the market for ECEC. This study demonstrates that alleviating information barriers may be a helpful tool for lower income/education parents. Specifically, information helps parents select types of ECEC settings that have higher regulatory oversight. However, the limited and modest effect sizes also highlight that there are additional barriers and considerations that occur when parents select ECEC for their children. For example, although providing information may alleviate some barriers to quality ECEC that often depend on the quality of communication between ECEC settings and parents (Shpancer et al., Reference Shpancer, Bowden, Ferrell, Pavlik, Robinson, Schwind, Volpe, William and Young2002), providing information to parents does not address logistical barriers. Parents – and particularly lower income and/or lower-education parents – face innumerable other barriers to accessing high-quality care in a choice-based ECEC market. ECEC is ripe with market failures, including a general lack of available licensed care spaces (the preferred option of parents; Davidson et al., Reference Davidson, Burns, Hampton, White and Perlman2021). Geographical barriers also disproportionately affect lower-income parents, research from across Canada and the United States, in particular, has shown that lower income and lower-education parents are much more likely to live in childcare deserts, areas where there is a dearth of local licensed care providers (Hertzman, Reference Hertzman2004; Prentice, Reference Prentice2007; Malik & Hamm, Reference Malik and Hamm2017). Even when proximity to available licensed ECEC in not an issue, the type of care may ultimately be a secondary consideration as the cost of care may be the primary factor in determining whether parents choose licensed or unlicensed care. In Toronto, many parents struggle to afford ECEC; licensed ECEC centres are nearly double the cost of licensed home options, with unlicensed options generally even less expensive. Given these constraints, even the most well-informed parents may be forced to select unlicensed care environments or other lower-quality alternative care choices.
Additionally, the estimated effects in our study are lower than predicted. Not well captured, however, was the prior knowledge of parents related to important factors that our information aims to target, including regulatory oversight types, quality within ECEC and the importance of quality on developmental outcomes. For example, we do not know what parents’ perceived benefits of each of the types of ECEC settings are or what they believe are indicators of potentially enhancing developmental growth in children. The modest success of this treatment is likely due to the variability within our sample. In addition to the variation in prior knowledge and experience, parents may have there are also inherent choices for certain types of settings that are not connected to regulations (Davidson et al., Reference Davidson, Burns, Hampton, White and Perlman2021). Therefore, these results illustrate the necessity in identifying settings or communities where information is the primary barrier for parents. Future research should carefully reflect on the complexities and intersectionality of parent vulnerabilities that amplify barriers to accessing quality ECEC.
Our study has other important limitations. First, the participants in this study were recruited as a convenience sample, based on parents who accessed either the City of Toronto website or a drop-in centre staffed by a research assistant. Whether the results of this study are applicable to a broader population is a question for future research. After stratifying our sample to only those with lower income and lower income/education, our sample size was more limited. In addition, the differences in rank ordering of are qualitative (except for the intervention group not wanting licensed home childcare). As noted earlier, utilities are zero-centered (within an attribute). Thus, computationally lower utilities for one level of an attribute by definition, means that utilities for the other attributes in that level must be higher. It is based on this logic that we discussed the rank ordering of preferences where differences were non-trivial. However, future research should be conducted on the preferences for ECEC within lower income/education samples with sufficient size to be able to detect notable differences and have the statistical power to address the heterogeneity.
We also recognize that there is a range of prior knowledge and experiences within the ECEC landscape that may affect the need or novelty of our information. Unfortunately, due to the length and requirements of the survey, incorporating assessment questions to factor in their prior knowledge related to ECEC was not feasible. Another limitation arises from using the conjoint survey. The conjoint analysis has specific requirements in terms of how many aspects of a service or product need to be included and how many times participants need to see different options. Given the complexities of ECEC, we defined 8 attributes of interest and asked parents to choose ECEC in 12 separate conjoint exercises. Participants may have experienced fatigue due to the length of completing the survey, and fatigue may have been more pronounced in participants who have English as a second language.
Conclusion
Our study serves as an example of interesting methods for investigating the behaviours of parents navigating decisions ECEC. The conjoint analysis allows researchers to understand which factors rank as most influential for parent decisions through simulated decision scenarios (Davidson et al., Reference Davidson, Burns, Hampton, White and Perlman2021). Within this study, the conjoint analysis was essential to understanding the effects of information on parent's choices, within the context of real-life considerations. Specifically, it was important to understand if providing information on regulatory oversights of ECEC that range in quality-of-care children receive would influence parent choices when they had to also account for attributes of care such as cost, location and flexibility.
In line with our predictions, providing information on different types of care may slightly influence parental choices and there is likely a need to provide information-based interventions to lower income and education parents. By implementing a conjoint survey, we were able to capture the choices that parents make regarding licensing while considering other important considerations parents must apply in the real world. We found that our treatment appeared to make a difference to the lower income and education parents when examining information effects outside the various other aspects of consideration parents must choose from. This study thus suggests that information can be an effective tool at changing decisions parents make for higher quality types of ECEC when other constraints are not serving as barriers. Our findings suggest that this low-cost intervention is a promising avenue for helping parents become more informed consumers of ECEC services.
Acknowledgements
The authors would like to acknowledge the thoughtful comments of Pankaj Aggarwal, June Cotte and Tanjim Hossain on earlier phases of this research, as well as the research assistance of Sumayya Saleem and to the data collection efforts of our work study students: Caitlin Lynch-Staunton, Hillary Scott, Ava Persadmehr and Sajee Maheswaran. We are grateful as well to the students in Rotman School of Management 2506 for their assistance on the project: Gowtham Ramachandran, Neil Kalita, Revathi Kolagani, Matthew Solda, Chawin Vajanopath and Desmond Yeo. We would also like to thank Maren Katz for her consistent contributions as this project evolved. We gratefully acknowledge the support of the City of Toronto.
Financial support
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is supported by a McCain Foundation research grant.
Competing of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.








 Open access
Open access