


The offspring of parents with bipolar disorder have an approximately fourfold increased lifetime risk of developing a mood disorder (Reference Lapalme, Hodgins and LaRocheLapalme et al, 1997; Reference Delbello and GellerDelbello & Geller, 2001). Several studies have established associations between stressful life events and symptoms of depression (Reference Williamson, Birmaher and FrankWilliamson et al, 1998; Reference Goodyer, Herbert and TamplinGoodyer et al, 2000) and other emotional and behavioural disorders (Reference Goodyer, Kolvin and GatzanisGoodyer et al, 1987; Reference Sandberg, Rutter and PickelsSandberg et al, 2001). The temporal process of onset of psychiatric disorders following stressful life events remains poorly understood. Surtees & Wainwright (Reference Surtees and Wainwright1999) showed clear evidence for the progressive decay in the adverse effects of stressful life events over time. The aim of this study among an adolescent high-risk cohort was to investigate the relationship between stressful life events and the onset of mood disorders, with different models for the degree to which the presumed effects of stressful life events diminish over time. In addition, it was examined whether this relationship was modified by family loading for mood disorders.
METHOD
Design
The study presented here is part of an on-going prospective high-risk cohort study among adolescent offspring of parents with bipolar disorder in The Netherlands. In this paper we discuss the findings from the first assessment. The study design, study population and prevalence of psychopathology among the offspring have been described by Wals et al (Reference Wals, Hillegers and Reichart2001). In brief, 86 parents with bipolar disorder and their spouses and 140 offspring aged 12-21 years were examined between November 1997 and March 1999. In the offspring, 38 (27%) were diagnosed with a lifetime mood disorder according to DSM-IV criteria (American Psychiatric Association, 1994), 23 (16%) had any other lifetime DSM-IV diagnosis and 79 (56%) did not have any DSM-IV diagnosis. We report the results of an analysis of retrospectively collected data from this cohort on the relationship between lifetime life events and subsequent lifetime mood disorder.
Stressful life events
The investigator-based Bedford College Life Events and Difficulties Schedule (LEDS; Brown & Harris, Reference Brown and Harris1978, Reference Brown, Harris, Brown and Harris1989) is a semi-structured interview for assessing life events and long-term difficulties in adults. The LEDS covers ten domains: education, work, reproduction, money/possessions, housing, crime/legal, health, romantic relationships, other relationships and miscellaneous events (including deaths). It collects detailed information about the event itself, the timing of its occurrence (date) and relevant contextual information for each event. Based on the contextual information, the threat for each event is rated via standardised rating procedures. The threat score represents the severity of the event, ranging from mild (1) to severe (4). Several studies have supported the reliability (e.g. interrater) and validity (e.g. multiple informant) of the LEDS with adults exhibiting a variety of psychiatric symptoms (Brown & Harris, Reference Brown and Harris1978, Reference Brown, Harris, Brown and Harris1989; Reference Ormel, Oldehinkel and BrilmanOrmel et al, 2001).
Monck & Dobbs (Reference Monck and Dobbs1985) originally adapted the LEDS methodology for use with adolescents. They developed a teenage LEDS manual with accompanying event dictionaries based on a study of 67 British female adolescents aged 15-20 years. We modified the Dutch adult LEDS interview and manual and translated the teenage event dictionaries into Dutch: the Kiddie LEDS (K-LEDS). The K-LEDS interviews were conducted by psychologists who had received K-LEDS training prior to interviewing. Because this K-LEDS interview covered the life cycle (childhood and early and late adolescence), all events and difficulties were dated on a yearly basis. In our analysis we used only the life event data because it was possible to date them more accurately than the long-term difficulties. We calculated the percentage fall-off of severe events recalled per annum, which appeared to be 11%. The events were rated from written transcriptions of the interview by three independent raters who had not been involved in the interviews and were masked to the respondents' mental health status. A panel consisting of the three raters and two of the authors (M.H., M.W.) reached consensus on the events that raised rating problems.
Schedule for Affective Disorders and Schizophrenia for School-Age Children - Present and Lifetime Version
All children were evaluated using the Schedule for Affective Disorders and Schizophrenia for School-Age Children - Present and Lifetime Version (K-SADS-PL; Reference Kaufman, Birmaher and BrentKaufman et al, 1997). The K-SADS is an interviewer-oriented diagnostic interview designed to assess current and past DSM-IV symptoms resulting in diagnoses in children and adolescents, by interviewing the parent(s) and child separately. The timing of illness episode onset was determined in cases where the DSM-IV criteria were fully met. If parents and child disagreed on the presence of a symptom, greater weight typically was given to parents' reports of observable behaviour and children's reports of subjective experiences (Reference Kaufman, Birmaher and BrentKaufman et al, 1997). The K-SADS-PL was conducted by three of the authors (M.H., M.W. and C.R.) and by five intensively trained interviewers with graduate degrees in psychology.
Family History Research Diagnostic Criteria
Parents were interviewed using the Family History Research Diagnostic Criteria (FH-RDC) (Reference Andreasen, Endicott and SpitzerAndreasen et al, 1977), which were used to calculate a continuous familial loading score for unipolar mood disorder, bipolar disorder and substance use disorder in first (n=177) and second-degree relatives (n=932) of the children. The index of family loading for the bipolar offspring is based on the number and age of the affected first- and second-degree relatives of the adolescent. Every relative examined using the FH-RDC contributed to the index, depending on whether the person was affected and the age at which the person was affected. We arbitrarily divided the continuous familial loading variable into high (> median) and low familial loading (< median). In our analyses we used the familial loading for unipolar mood disorder because all subjects had a first-degree family member with a bipolar disorder, consequently the familial loading for bipolar disorder did not differentiate. For a more detailed description of the calculation of the family loading, see Verdoux et al (Reference Verdoux, van Os and Sham1996) and Wals et al (Reference Wals, van Os and Reichart2004).
Time-dependent life event load
To study the impact of life events on the on-set of mood disorder, a time-dependent (or time-specific) life event load variable was calculated for every year of follow-up. This variable was designed to summarise the exposure load from all adverse events experienced up to a particular point in time, while accounting for number, severity and their lasting effects. The life event load was calculated according to four models. These models reflect different hypotheses concerning the time-related decay of the effect of a life event on the risk of mood disorder. In model I we tested a purely cumulative effect of the impact of life events on the development of mood disorder. Accordingly, the life event load at a particular point in time (year y) was simply calculated as the sum of the threat scores of the life events in year Y and all preceding years. In models II, III and IV, the time-dependent life event load was subjected additionally to an exponential decay function. This reflects the hypothesis that the impact of life events principally accumulates but at the same time gradually decays as time goes by. In model II the decay function implied a 25% loss per year. In models III and IV we subjected the life event load to a yearly decay of 50% and 75%, respectively. In view of the retrospective nature of data collection, we included only severe life events (threat score 3 and 4) that had occurred after the age of 4 years. Consequently, follow-up time started at age 5 years. If more than one life event occurred in the same year, the threat scores for these events were summed.
Data analysis
The relationship between life events and the occurrence of mood disorder was studied using a statistical model relating determinants whose statuses change over time to survival-type (censored) outcome data, i.e. Cox regression with time-varying covariates (Reference CoxCox, 1972). Because the 140 children originated from 86 families, data must be considered correlated through family. Therefore, we used a ‘frailty’ model, i.e. a Cox model with a cluster variable indicating family. Time-varying influence of life events was permitted by including the time-dependent life event load as a continuous time-varying covariate in the model. In this model the dependent variable was time from age 5 years to first mood disorder or, if no mood disorder occurred, time from age 5 years to interview. The results are expressed as hazard ratios indicating the instant relative risk of mood disorder per unit life event load, thus representing the strength of the association. Hazard ratios were presented with 95% confidence intervals (95% CIs). To find out which of the four life event load (decay) functions is optimally in agreement with the observed data, we compared Akaike's information criterion (-2 × maximised log-likelihood+ 3 × number of parameters) between the four regression models (Reference Akaike, Petrov and CsakiAkaike, 1973). This index can be interpreted only in a relative sense, i.e. lower values indicate better agreement. We included familial loading and gender as fixed covariates in the regression models to examine whether they confounded the association between life event load and onset of mood disorder. Confounding was considered present if inclusion of these variables substantially (by at least 10%) changed the hazard ratios for life event load. To investigate whether the relationship between life event load and mood disorder depended on familial loading (i.e. multiplicative interaction or effect modification), we included an interaction term of familial loading variable × life event load variable as a covariate in the model, and tested its statistical significance. Interaction was explored further by presenting separately the life event hazard ratios for children with familial loading above and below the median. The analyses of interaction were performed for the model showing optimal agreement with the observed data only. The level of significance in all analyses was P < 0.05 (two-sided).
RESULTS
The general characteristics of our study population are shown in Table 1. Thirty-eight (27%) of the children developed a mood disorder during follow-up at a median (range) age of 14 (7-20) years. Of these, four had bipolar disorder, eight had major depressive disorder, eight had dysthymic disorder, two had cyclothymic disorder, fifteen had depressive disorder not otherwise specified, one had adjustment disorder with depressed mood and two had mood disorder not otherwise specified. Because one individual could receive more than one lifetime diagnosis, there are 40 diagnoses among 38 individuals. The median of the familial loading scores for unipolar mood disorder and the median of the number of severe life events are also shown in Table 1.
Table 1 General characteristics of study population (n=140)
| Characteristic | |
|---|---|
| Male (n, %) | 72 (51%) |
| Female (n, %) | 68 (49%) |
| Any mood disorder1 (n, %) | 38 (27%) |
| Any non-mood disorder12 (n, %) | 23 (16%) |
| No disorder1 (n, %) | 79 (56%) |
| Age (mean, s.d.) | 16 (2.7) |
| Life events (median, range) | 4.0 (1-16) |
| Familial loading (median, range) | − 0.38 |
| (−1.6 to 3.5) |
The life event load in 5-year age categories is displayed in Table 2, demonstrating the net effect of the summation (model I) and decay functions (models II, III and IV) on the life event load in these age groups for all individuals during the entire follow-up period. As a consequence, life events that had occurred after the onset of a mood disorder also contributed to the life event load. (In the analyses examining the association between life events and mood disorders, only events preceding the onset of the first mood disorder were taken into account.) In models I and II a monotonous increase was found, but in the models with the strong decay functions superimposed an inverse U-shape of the mean life event load with age was observed.
Table 2 Life event load1 according to age category and model
| Model | Age category (years) | ||
|---|---|---|---|
| 5-10 | 11-15 | 16-20 | |
| I (cumulative) | 1.7 (2.3) | 6.6 (5.2) | 11.9 (6.1) |
| II (25% decay) | 1.3 (1.6) | 3.4 (2.7) | 4.0 (3.0) |
| III (50% decay) | 1.0 (1.2) | 2.1 (1.7) | 2.0 (2.2) |
| IV (75% decay) | 0.8 (0.9) | 1.5 (1.2) | 1.3 (1.6) |
The relation between life event load and mood disorder is depicted in Table 3. Irrespective of the model employed, the life event load was significantly associated with an approximately 10% increased risk (hazard ratio=1.1) of mood disorder per unit life event load. Although high familial loading (> median) itself was strongly related to mood disorder, with hazard ratios of 3.05 (95% CI 1.49-6.25), 2.61 (95% CI 1.29-5.30), 2.53 (95% CI 1.25-5.10) and 2.54 (95% CI 1.27-5.11) for models I-IV, respectively, adjustment for this variable hardly had an effect on the life event load-mood disorder association. This indicates that familial loading was no confounder. Adjustment for gender did not change the life event hazard ratios either. According to Akaike's information criterion, model II was most in agreement with the observed data.
Table 3 Relative risk of a mood disorder using four models of events effect decay
| Model | Life event load1 | Life event load1 (FL adjusted) | − 2 log-likelihood +3 |
|---|---|---|---|
| I (cumulative) | 1.069 (1.033-1.106) | 1.073 (1.041-1.106) | 327.2 |
| II (25% decay) | 1.100 (1.064-1.137) | 1.091 (1.053-1.130) | 324.8 |
| III (50% decay) | 1.114 (1.072-1.157) | 1.101 (1.057-1.148) | 325.6 |
| IV (75% decay) | 1.115 (1.069-1.162) | 1.102 (1.053-1.153) | 328.2 |
Figure 1 illustrates the relationship between life event load and mood disorder. It shows that in the majority of follow-up years the life event load was considerably higher for those who developed a mood disorder than for those who did not. Above and below the median of the familial loading variable the hazard ratios in model II for the relation between life event load and mood disorder were similar: 1.090 (95% CI 0.928-1.280) and 1.110 (95% CI 1.059-1.163), respectively. In line with this, the interaction term was not statistically significant (P=0.73), indicating no modification of the relationship between life event load and mood disorder by familial loading.
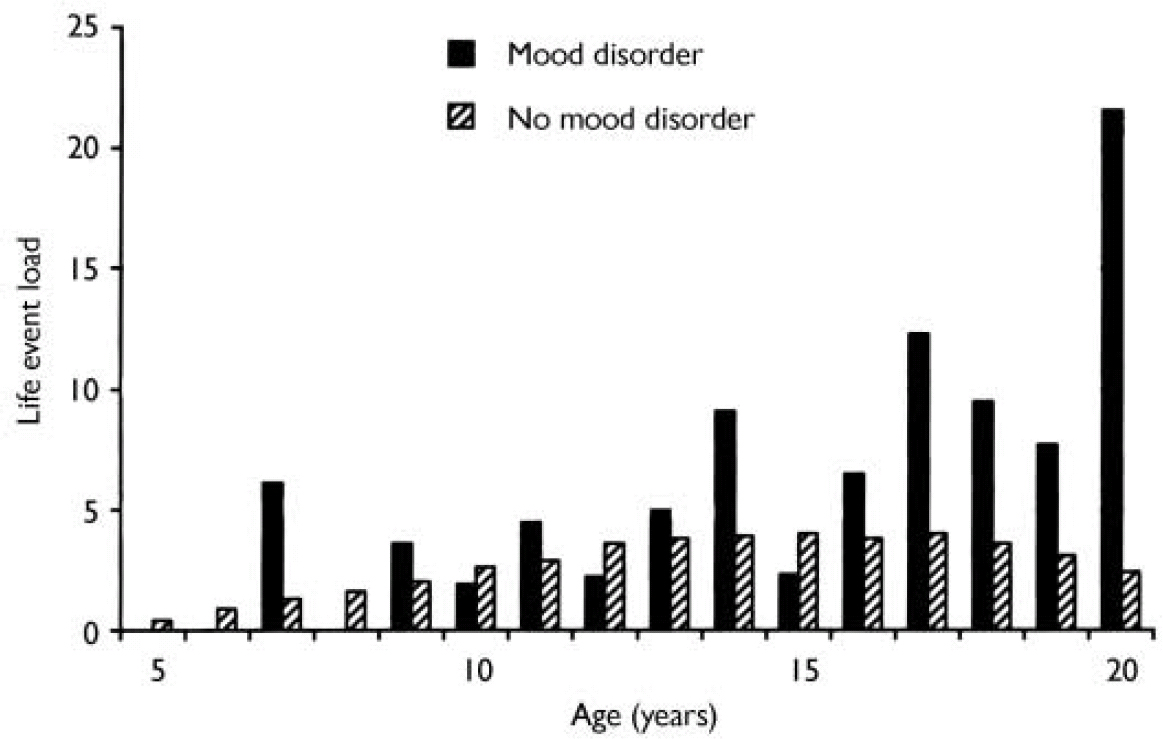
Fig. 1 Difference in life event load according to model II between adolescents with a mood disorder (n=38) and without a mood disorder (n=102) during follow-up. For subjects with a mood disorder, only the preceding life events were included.
DISCUSSION
In the present study a strong relationship between life events and the risk of mood disorder in the offspring of patients with bipolar mood disorder was demonstrated. The relationship was best described using model II, in which the effects of life events steadily decay by 25% per year. Both Delbello & Geller (Reference Delbello and Geller2001) and Lapalme et al (Reference Lapalme, Hodgins and LaRoche1997) found that offspring of parents with bipolar disorder are at increased risk of developing mood disorders and other psychopathology. Familial loading of unipolar disorder was significantly associated with the lifetime prevalence of mood disorders in our sample of adolescent offspring of parents with bipolar disorder (Reference Wals, van Os and ReichartWals et al, 2004). However, familial loading did not confound or modify the relation between life events and mood disorder in this study. Both had independent effects on risk of mood disorders.
Comparison with other studies
Few high-risk studies report the influence of stressful life events as a risk factor for the development of bipolar disorder. Johnson et al (Reference Johnson, Andersson-Lundman and Aberg-Wistedt2000) concluded that patients with bipolar disorder and with high constitutional vulnerability had an earlier age of onset and needed fewer stress factors (early parental separation and life events) to become ill compared with patients with unipolar illness. The Cardiff Depression Study (Reference Farmer, Redman and HarrisFarmer et al, 2002) investigated the suggested co-familiality of depression and life events and whether there might be a common familial factor influencing vulnerability to depression and the experience of life events. Using a sib-pair design, they reported no evidence for a common factor influencing both depression and life events. Kendler & Karkowski-Shuman (Reference Kendler and Karkowski-Shuman1997) showed that, in adults, negative life events were most likely to lead to the onset of major depressive disorder in individuals inferred to have a genetic liability to depression, and also that the genetic liability to depression overlaps with the genetic liability to experience stressful life events. So, through their behaviour, people can to some extent shape and select their environments.
Our findings are in line with the work of Wainwright & Surtees (Reference Wainwright and Surtees2002), who developed sophisticated analytical approaches to study adversity-disorder relationships. Their study, like ours, showed that the simplest model involving a single time-dependent covariate was in-appropriate because it failed to capture the decay in the event effects and that an exponential decay of the adverse effects of life events over time had to be modelled. In studying the effects of negative life events on the onset of mood disorders in a high-risk group of adolescents, Silberg et al (Reference Silberg, Rutter and Neale2001) found that there was no effect of independent life events on the adolescents' depression in the absence of parental emotional disorder but there was a significant effect in its presence. In our sample all subjects had a parent with bipolar disorder. As described, high familial loading was based on the number and age of unipolar affected first- and second-degree relatives of the adolescents.
Strengths and limitations
A major limitation of this study is that all data were collected at a particular point in time. Within a cross-sectional design we employed a longitudinal approach by dating the onset of episodes of mood disorders and the occurrence of life events. This approach brings a number of limitations in its wake. First, subjects with a mood disorder could have been more inclined to remember life events than those without this condition, which would result in recall bias; therefore, we restricted our analyses to severe life events and omitted the first 5 years of life. Also, the events were rated from written transcripts of the interview by three independent raters who had not been involved in the interviews and were masked to the respondents' mental health status. To explore the possibility of recall bias we divided the subjects with a mood disorder into current cases (i.e. at the time of the interview) and past cases, and compared the life events reported in the preceding 2 years. If recall bias played an important role, it would probably influence the current cases more than the past cases. The results of this analysis, however, showed that the mean threat scores were similar (4.2 and 4.0, respectively).
Second, one could question the validity of the LEDS used retrospectively to collect the life event data. Most of the studies concerning the validity of retrospective reports collected by the LEDS were restricted to a 12-month period. There have also been studies using the LEDS to test the validity of life events reported over a 10-year period. The ‘fall-off’ in terms of the length of time from the date of the reported event or difficulty to the point of interview was checked and found to be surprisingly low for all events; 4.8% per year (Reference Neilson, Brown, Marmot, Brown and HarrisNeilson et al, 1989). In our sample, as mentioned before, we calculated the percentage fall-off of severe events recalled per annum, which appeared to be 11%. Retrospective reporting of life events using checklist inventories typically declines at a rate of 5% or more each month (Reference Funch and MarshallFunch & Marshall, 1984). This suggests that in an aetiological enquiry it might well be possible to use the LEDS to cover a whole decade.
A further limitation might be that the sample is not population based. Only patients with children aged 12-21 years who were willing to participate were included. A control group of adolescents without a parent with bipolar disorder would have given more data to study the impact of stressful life events on the onset of mood disorders. Because the LEDS interview alone takes about 3 h and the rating takes another hour, financially this was not an option. Another limitation is that the group of adolescents with a mood disorder is relatively small in our sample. Consequently, the statistical power to demonstrate an interaction between life event load and familial loading was limited.
According to our study the impact of stressful life events principally accumulates but at the same time gradually decays (25% per year) as time goes by. This suggests that the effects of stressful life events do not simply add up or rapidly extinguish but, in a gradually fading fashion carry over into the future risk of an epidose of mood disorder. What drives the decay is not known, it might result from coping strategies or the effect of neutralising life events. Although high familial loading for unipolar depression was strongly related to risk of mood disorder, familial loading did not confound the relationship between life event load and mood disorder. There was also no evidence suggesting that familial loading modified the relationship between life event load and mood disorder.
Future directions
Improvements in the specification of stress modelling procedures might facilitate the integration of ideas from competing aetiological models of the onset and subsequent course of mood disorders. There are still many aspects of the stressful life event-illness relationship that should be considered in future studies: the underlying assumption of an additive effect of multiple life events, the possible dose-response effect of adverse life events and the existence of threshold effects. Other interesting topics for further research are the influence of life events on the duration and course of the mood disorders and the effects of comorbidity, temperament and specific coping skills. Goodyer (Reference Goodyer2002) referred also to limbic-cortical neural networks in his framework for future research on this topic.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Stressful life events increase the lifetime risk of a mood disorder in adolescent children of parents with bipolar disorder.
-
▪ The level of familial loading for unipolar disorders does not affect the relationship between stressful life events and the onset of mood disorders in adolescent children of parents with bipolar disorder.
-
▪ The impact of life events principally accumulates but at the same time gradually decays as time goes by.
LIMITATIONS
-
▪ Life event data were collected retrospectively over more than 10 years.
-
▪ No life event or psychopathology data were available for a control group of adolescents without a parent with bipolar disorder.
-
▪ Recall bias as a result of psychopathology might be present.





eLetters
No eLetters have been published for this article.