



A significant proportion of people with schizophrenia develop obsessive–compulsive symptoms (OCS). Some experience an obsessive–compulsive disorder (OCD) after remission of psychosis, whereas others enter an intermediate state combining psychosis and OCS.Reference Schirmbeck and Zink1 However, there is no clear understanding of this phenomenon.
Schizophrenia and OCS/OCD
OCS and OCD are common among those with schizophrenia, with prevalence increasing from 12.5% in individuals in an at-risk mental state for psychosis to 25% in early schizophrenia and up to 47% in clozapine-treated patients.Reference Mawn, Campbell, Aynsworth, Beckwith, Luce and Barclay2 There is a plausible biological overlap between schizophrenia with OCS and classic OCD. Both feature over-activation of the orbitofrontal cortexReference Schirmbeck, Mier, Esslinger, Rausch, Englisch and Eifler3 and exhibit similar traits of cognitive inflexibility, reduced processing speed and memory deficits.Reference Poyurovsky, Weizman and Weizman4 Further, individuals with schizophrenia with OCS share a genetic background with OCD. Specifically, single nucleotide polymorphisms (SNPs) and other genetic variants in the glutamate pathway, such as SLC1A1 (glutamate transporter) and GRIN2B (glutamate receptor), are associated with OCS in people with clozapine-treated schizophrenia.Reference Guillem, Satterthwaite, Pampoulova and Stip5 However, associations with serotonergic (5-HT) pathways have not been explored, despite the role of SLC6A4 (a serotonin transporter), HTR2A and HTR2C (serotonin receptors) in OCD.Reference Grillault Laroche and Gaillard6 Some authors advocate for including schizo-obsessive disorder as a schizophrenia subtype in which pre-existing OCS or OCD are unmasked after psychosis remission.Reference Poyurovsky, Weizman and Weizman4 However, this hypothesis is undermined by work showing a correlation between OCS and psychosis severity.Reference Guillem, Satterthwaite, Pampoulova and Stip5 Others argue that de novo OCS in schizophrenia are an antipsychotic-related event.Reference Schirmbeck and Zink1 Epidemiologically, de novo OCS are over-represented in patients treated with clozapine, olanzapine or risperidone when compared with patients prescribed aripiprazole, amisulpride or haloperidol.Reference Grillault Laroche and Gaillard6 This likely reflects these drugs’ different 5-HT2A/2C receptor affinity. OCS are also associated with higher clozapine dose and length of treatment and clozapine plasma levels,Reference Gürcan, Şenol, Yağcıoğlu and Ertuğrul7 suggesting a dose-dependent relationship. This is challenged, however, in the literature, with some suggesting that these findings are confounded by the higher antipsychotic doses typically required by those with psychosis of greater severity.Reference Kim, Barr, Stewart, White, Honer and Procyshyn8
Using the habit model to understand the interplay between psychosis, OCS and clozapine
We have previously identified that, in clozapine-treated patients, psychosis severity and length of treatment are distinct risk factors for obsessions and checking compulsions respectively.Reference Fernandez-Egea, Worbe, Bernardo and Robbins9 Most studies show a predominance of compulsions over obsessions in this group, with excessive checking being the most frequently reported repetitive behaviour.Reference Mukhopadhaya, Krishnaiah, Taye, Nigam, Bailey and Sivakumaran10 Informed by models of habit formation developed in cognitive neuroscience, we conceptualised these checking compulsions as arising as the by-product of psychosis. Specifically, repetition in the context of a diminished ability to consider an action's outcome may lead to the automatisation of behaviour (‘habit formation’). Further, decreased 5-HT activity may enhance habit development.Reference Gillan, Robbins, Sahakian, van den Heuvel and van Wingen11 We have applied this framework to hypothesise a two-phase model of OCS and OCD development. First, an initial phase of checking as a goal-directed behaviour may occur due to psychotic hypervigilance. After remission of psychosis, achieved with antipsychotic treatment, a second ‘habit’ phase may occur in which clozapine ameliorates psychosis but promotes checking compulsions via serotonin antagonism in those vulnerable.
In the present study, we investigated the dynamic interplay between psychosis, clozapine dose and OCS. We aimed to test this two-phase hypothesis using a large cohort of clozapine-treated patients assessed longitudinally. Specifically, we hypothesised that:
(a) checking compulsion is related to psychosis severity
(b) checking severity correlates with clozapine plasma levels in those in remission from psychosis.
We also explored the moderating effects of specific genetic variants on the development of psychosis-related obsessions and compulsions.
Method
Study design and setting
This naturalistic longitudinal observational study used anonymised electronic records gathered by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). CPFT is the primary public mental healthcare provider for approximately 890 000 people in a mixed urban/rural area in the East of England, UK.
Ethics, participants and electronic records
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
We used the Clinical and Research Database (CRD) for Persistent Schizophrenia under NHS Research Ethics Committee (REC) approvals (ref. 13/EE/0121; 18/EE/0239). This database contains anonymised routine clinical data from the CPFT Clozapine Clinic.
Extracted data maintained patient anonymity by removing all identifiable data. All clinical assessments in the CRD were performed by an experienced psychiatrist (E.F.E.) and the database also contained self-rated measures that the patients completed during routine clinical appointments. This study covers information from 24 August 2012 to 31 December 2022. The CRD includes 3126 face-to-face assessments of 254 patients taking clozapine. For this study, we included only assessments that had a standardised evaluation of OCS and scores on the positive subscale of the Positive and Negative Syndrome Scale (PANSS-positive) (see below).
Routine clinical assessments
All annual Care Programme Approach (CPA) assessments in the electronic record include sociodemographic data (age, gender, age at illness onset, clozapine start date), a review and confirmation of prescribed medication (with dose), current smoking habit (average number of cigarettes per day), alcohol use (average number of alcohol units per week) and latest clozapine and norclozapine plasma levels results (including date of test). All patients are evaluated on all the scales.
For this study, relevant psychopathology scales included in the CRD were the Obsessive–Compulsive Inventory – Revised (OCI-R), self-reported annually from 2016 (and completed independently of other scales), and the PANSS-positive, rated every 2 years since 2017.
Psychopathology scales
Severity of OCS was measured using the OCI-R,Reference Foa, Huppert, Leiberg, Langner, Kichic and Hajcak12 an 18-item self-reported measure featuring six subscales: washing, checking, ordering, obsessing (e.g. having obsessional thoughts), hoarding and mental neutralising. The impact of each item on a respondent's function is reported via a 5-point scale, ranging from ‘not at all’ (0) to ‘extremely’ (4). The total score, therefore, ranges from 0 to 72, with higher scores indicating greater OCS severity. As in previous work,Reference Fernandez-Egea, Worbe, Bernardo and Robbins9 we considered a total score ≥21, or ≥5 on any subscale, as clinically significant.
Psychosis severity was measured using the positive subscale (items P1–P7) of the PANSSReference Kay, Fiszbein and Opler13. The PANSS is a clinician-rated scale that includes 7 items referring to psychotic (‘positive’) symptoms rated on a 7-point scale (1 absent, 7 extreme). Patients were considered in remission from psychosis when none of these items scored ≥3, as the main goal of the study was to explore whether active symptoms (PANSS score of ≥3) were associated with OCS/OCD.
Assessment of clozapine load
We used blood clozapine levels as a measure of clozapine load, rather than clozapine dose, as dose (typically ranging from 75–900 mg/day) is an inaccurate measure of clozapine load.Reference Rostami-Hodjegan, Amin, Spencer, Lennard, Tucker and Flanagan14 This is because clozapine metabolism is influenced by various factors, including medication adherence, gender, cytochrome polymorphisms, concurrent medication and smoking habits. Blood levels, therefore, represent a more precise measure.
Genetics of clozapine-induced OCS
One hundred patients of the final sample of 196 also consented to participate in the ethically approved ‘Genetics of common clozapine-induced side effects’ study (REC reference 18/NW/0581). The study aimed to replicate previously described genetic variants associated with clozapine side-effects, including OCD and metabolic complications.
Specifically, we explored genetic variants in the serotonin pathway, including single nucleotide polymorphisms (SNPs): SLC6A4 (rs4795541, rs25531), HTR2A (rs6313, rs6314) and HTR2C (rs3813929, rs1414334). Variants within the glutamate pathway were also included: SLC1A1 (rs2228622) and GRIN2B (rs890). Samples were collected during routine blood monitoring at the clozapine clinic, using Whatman® FTA® (Flinders Technology Associates) cards by Sigma-Aldrich, allowing storing, transporting, stability and DNA purification from samples at room temperature.
Genotyping was conducted at San Jorge University in Zaragoza and in the Pharmacology Unit of Barcelona University Medical School, both in Spain. Using a paper puncher sterilised with alcohol and flame, 3 mm discs of dried blood were obtained from the card. DNA was extracted following the manufacturer's instructions. The concentration and quality of DNA were measured spectrophotometrically using a NanoDrop™ 2000 (Thermo Fisher Scientific, Surrey, UK). Genetic variants of the SLC6A4 gene, rs4795541 (also known as 5-HTTLPR) and rs25531, were genotyped using an MJ Mini™ thermal cycler (Bio-Rad, Hercules, CA, USA) following polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP) conditions described previously.9 The CFX Connect Real-Time PCR System (Bio-Rad, Hercules, CA, USA) was used to genotype rs6313 and rs6314 (HTR2A) with predesigned rhAmp™ SNP Genotyping Assays (Integrated DNA Technologies, Coralville, IA, USA). The polymorphisms rs3813929 and rs1414334 (HTR2C), rs2228622 (SLC1A1) and rs890 (GRIN2B) were genotyped using an MJ Mini™ thermal cycler (Bio-Rad, Hercules, CA, USA) following PCR and RFLP conditions previously described.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines checklist was followed.
Statistical analysis
For basic description, categorical variables are reported in the format ‘n (%)’ and continuous variables in the format ‘mean (s.d.)’.
Pearson correlation coefficients were used to measure the strength and direction of associations between continuous variables. To account for multiple comparisons, we applied a Bonferroni correction.
A multi-level mediation model assessed the longitudinal association between psychosis severity and checking compulsions, directly and indirectly via obsessing. This is the preferred method for exploring longitudinal changes in samples where the time between assessments is not fixed, as in our study. Psychosis severity (measured by the PANSS-positive subscale) was included as both a fixed-effect and a (per-participant) random-effect variable, and the duration of clozapine treatment was controlled for, as in previous similar studies. Further analyses used PANSS-positive items associated with reality distortion (items P1, P3 and P6).
For assessing the effect of clozapine load on psychosis severity, we selected a subgroup of participants to avoid factors confounding previous research. These individuals (a) were on clozapine monotherapy (no other antipsychotic or antidepressant) for more than a year, (b) were in remission from psychosis and (c) had plasma levels taken within 28 days of the OCS evaluation (without intervening medication changes) that were within the upper limit of the therapeutic range (0.6 mg/L or 600 ng/mL).
Multi-level moderation models were also conducted to explore whether specific genetic variants moderated the association between psychosis severity and checking compulsions via obsessions. The models were fitted with psychosis severity and genetic variant as both fixed-effect and (per-participant) random-effect variables. Duration of clozapine use was controlled for. This was performed in a subgroup of patients for whom genetic data were available (n = 97, with 235 face-to-face assessments).
All statistical analyses were performed using R (version 3.5.0 for Windows), including the packages lmerTest (version 3.1-2) and Mediation (version 4.5.0).
Results
Sample description
The final sample consisted of 196 clozapine-treated patients and 459 OCI-R/PANSS-positive pair assessments, each participant being followed for an average of 2.7 years. Table 1 shows key sociodemographic and clinical variables at baseline: 74 participants (37.9%) had an OCI-R score at or above the OCD cut-off of 21. Obsessing and checking compulsions were the most common OCS. Among those in remission from psychosis (n = 60 out of 196), 25 (12.8% of the total) exhibited significant checking behaviours (indicated by a score >4 on the checking subscale).
Table 1 Baseline sociodemographic and clinical characteristics of the participants (n = 196)

OCI-R, Obsessive–Compulsive Inventory – Revised. PANSS, Positive and Negative Syndrome Scale.
Thirty-five participants (17.9%) exhibited negligible OCS (total score <5 and checking factor <2) after 5 years or more on clozapine treatment. The Supplementary material available at https://doi.org/10.1192/bjp.2024.30 expands on the details of the prevalence of OCS severity by psychosis remission.
The role of psychosis and reality distortion in OCS
Psychotic symptoms significantly correlated with overall OCS severity and with the obsessing and checking compulsion subscales of the OCI-R (Table 2). This association was significantly stronger for obsessing (r = 0.419) than compulsion (r = 0.116). Table 2 also shows the associations with the individual psychotic symptoms.
Table 2 Correlation between obsessive–compulsive symptoms (OCS) and psychotic symptomsa

PANSS, Positive and Negative Syndrome Scale; OCI-R, Obsessive–Compulsive Inventory – Revised.
a. OCS were measured using the OCI-R total score and OCI-R Obsessing and Checking subscales. Psychosis was measured using the PANSS positive subscale (n = 457) and individual PANSS positive symptoms (sum of P1 to P7). Bold indicates significance after correction for multiple comparisons (α = 0.05/24 = 0.002).
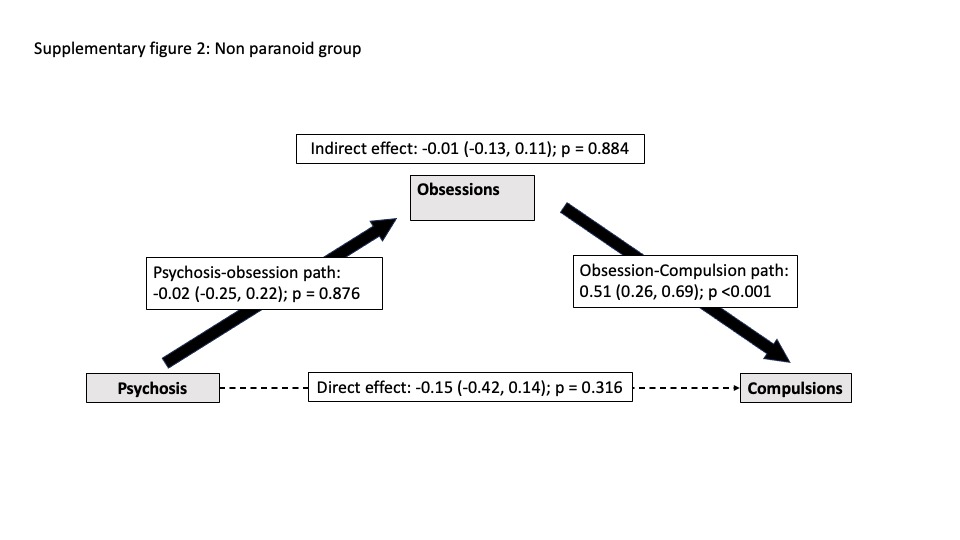
The effect of psychosis on checking behaviour was indirect, mediated by obsessional symptoms. No direct effect of psychosis on checking compulsions was identified (Fig. 1). The length of clozapine treatment was controlled for in this model. In further models (Supplementary Figs 1 and 2), an indirect effect of psychosis on compulsion was found only for participants with active paranoid/psychotic symptoms (n = 198: those for whom the sum of scores on PANSS items P1 + P3 + P6 > 4). Similar results were found when additional confounders, including clozapine dose, were included in the models.

Fig. 1 Obsessive–compulsive symptoms (OCS) and psychosis: mediation model exploring causality (n = 195, with 459 face-to-face assessments).
Psychosis was measured using the positive subscale of the Positive and Negative Syndrome Scale (PANSS). Effects are reported with 95% confidence intervals.
The role of clozapine on the persistence of excessive checking after psychosis remission
Figure 2 shows the significant correlations between checking compulsions and clozapine dose (n = 65; r = 0.378, P = 0.002), clozapine plasma level (r = 0.353; P = 0.004) and norclozapine level (r = 0.270; P = 0.030). There was no correlation between obsessing and either clozapine dose or levels (P > 0.21).

Fig. 2 Correlation of checking severity with clozapine dose and plasma levels in the subgroup (n = 65) on clozapine monotherapy and in remission from psychosis.
Clozapine plasma levels were taken within 28 days of the assessment and with no intervening medication changes. OCI-R, Obsessive–Compulsive Inventory – Revised.
Within this group of patients in remission, we compared those with excessive checking (OCI-R checking subscale score >4; n = 28) with those without checking (n = 37). Those with excessive checking had a higher clozapine dose (t = 2.956; P = 0.04), higher clozapine levels (t = 2.973; P = 0.04) and higher norclozapine levels (t = 2.363; P = 0.021).
Across the whole sample (thus, including those with any severity of psychosis or non-monotherapy; n = 313), there were no significant correlations between checking severity and clozapine dose (r = 0.071; P = 0.213) or plasma level (r = 0.021; P = 0.709).
Genes moderating psychosis-to-obsession and obsession-to-compulsion effects
We found the association of psychosis with obsessions to be moderated by serotonergic genes in uncorrected tests, but this did not survive correction for multiple comparisons. In the uncorrected tests, genotype GC for HTR2C (rs1414334) moderated the effect, and genotype GA SLC6A4 (rs25531) and genotype AA for SLC1A1 (rs2228622) moderated the effect from obsession to compulsion, but none of the other SNPs studied did. Supplementary Table 1 details the eight SNPs studied.
Discussion
We found that OCS are common in clozapine-treated patients and are associated with both psychosis severity and clozapine load, albeit at different phases. Mediation analyses suggested that psychosis severity generates checking behaviour indirectly by inducing obsessions. After remission from psychosis, checking compulsion correlated with clozapine plasma levels. We also found indications that serotonergic and glutamatergic variants might moderate the effect of psychosis on obsessions and compulsions, although our sample was too small for these findings to be considered conclusive.
Limitations
This study has some limitations. First, its naturalistic design is inferior to an experimental study. Experimental methodologies, however, are not feasible here, as the potentially lethal side-effects of clozapine generally prohibit its chronic administration to healthy volunteers. Long-term longitudinal studies in people with schizophrenia after clozapine initiation could provide a more detailed characterisation, but the latency of the onset of OCS (up to a decade) may render such studies impractical. Given this, we consider this study's large sample and longitudinal follow-up to represent a balance between practical feasibility and rigour. Second, OCS were evaluated using a self-rated scale and further work might benefit from replication using a clinician-rated scale such as the Yale–Brown Obsessive Compulsive Scale (Y-BOCS). Again, however, this may be impractical in a clinical environment. Third, the patient sample included in this study's genetic analyses was small (n = 97), and these findings should therefore be taken as exploratory and in need of replication.
Interpretation of findings and comparison with previous research
Our results broadly align with previous research regarding OCS prevalence (here, 37.9%) and the predominance of checking and obsessing symptoms. Our sample is representative of a typical clozapine-treated cohort, with male predominance (79%), an average prescribed clozapine dose of ~330 mg/day and a typical treatment length (~17 years). Importantly, however, this study's sample size (196 participants), longitudinal nature and volume of standardised OCS and PANSS-positive assessments (457 face-to-face assessments) are more extensive than any previous research.
This work builds on a hypothesis established a priori and developed during our previously published cross-sectional publication. We have conceptualised clozapine-associated OCS as a dynamic phenomenon that fluctuates in intensity according to psychosis severity, in line with recent work by Schirmbeck and colleagues,Reference Schirmbeck, Konijn, Hoetjes, Zink and de Haan15 and clozapine load. We uncoupled OCS into its two main components (obsessions and compulsions) and applied a mediation model that identified an association of psychosis severity (particularly the severity of reality distortion symptoms such as delusions, hallucinations or suspiciousness/persecutory beliefs) with obsessive thoughts. Obsessive thoughts, in turn, triggered checking behaviour. This may initially be understood as goal-directed, safety-seeking behaviour in acutely psychotic paranoid patients. As one patient in this cohort reported, ‘I need to check everything is in place as my upstairs neighbour comes to steal my stuff’. Then, in patients achieving psychosis remission, we found checking severity to be significantly correlated with clozapine plasma levels, suggesting a role of clozapine in perpetuating checking as a non-goal-directed action or habit. Indeed, persistently impaired safety signalling has been described in OCD,Reference Schirmbeck, Konijn, Hoetjes, Zink and de Haan15 limiting patients’ ability to assign safety valuations after verification.
Appreciating the distinct roles of psychosis and clozapine in OCS development is essential to understanding the apparent discrepancies in previous cross-sectional studies. The point prevalence of OCS (measured via questionnaire) may fluctuate according to the severity of the psychosis (Fig. 1, Table 2), clozapine load (Fig. 2), concomitant medications (e.g. antidepressants) or even the tools used to assess the symptoms. For instance, psychosis-driven, goal-directed checking might not be considered OCS but part of a delusion. Here we circumvented this risk by using a patient-reported OCS questionnaire.
Our hypothesised two-phase model of OCS developmentReference Fernandez-Egea, Worbe, Bernardo and Robbins9 is based on cognitive neuroscience's framework of habit formationReference Gillan, Robbins, Sahakian, van den Heuvel and van Wingen11 and shows the potential for embedding cognitive neuroscience into clinical practice. In our context, clozapine-treated patients in psychosis remission might experience checking compulsions as an antipsychotic-induced habit. A notable strength of our two-phase model is its integration of present results, previous studies and patients’ narratives, in which psychosis-induced goal-directed behaviour becomes habitual. This model is also flexible regarding the content of the repetitive behaviour, as we found checking whereas others reported washing as the most common compulsion.Reference Poyurovsky, Hramenkov, Isakov, Rauchverger, Modai and Schneidman16 Therefore, it can accommodate other triggers, such as the influence of stressful events, cognitive dysfunctions or affective symptoms (not included in this study as they were not part of the a priori hypothesis).
A plausible mechanism for the persistence of repetitive behaviour following remission from psychosis may be clozapine's antagonism of 5-HT2A and 5-HT2C receptors. A decrease in serotonin neurotransmission causes perseveration in reversal learning tasks, the hallmark of cognitive inflexibility in compulsive behaviours such as OCD.Reference Robbins, Gillan, Smith, de Wit and Ersche17 In humans, dietary tryptophan depletion (which reduces serotonin in the brain acutely) promotes habitual rather than goal-directed control.Reference Worbe, Savulich, de Wit, Fernandez-Egea and Robbins18 Remarkably, a recent mouse-model study showed similar results. Mice receiving clozapine increased their grooming time significantly (as a proxy of compulsion). This behaviour then reverted on the administration of fluoxetine, a selective serotonin reuptake inhibitor. Interestingly, the same effects were seen in both wild-type and Sapap3-knockout mice (a well-known animal model of OCD), albeit with significantly greater intensity in the knockout mice, suggesting a genetic vulnerability to clozapine-induced habit formation.Reference Kang, Noh, Bae, Kim, Lew and Lim19
Nevertheless, it is also interesting to note that individual factors might increase vulnerability. For instance, 35 patients (17.9%) exhibited negligible OCS after 5 years or more on clozapine treatment. Variation in vulnerability was explored in this work, in which we suggest a distinct moderating effect of serotonergic and glutamatergic SNPs on the psychosis-to-obsession and obsession-to-compulsion pathways respectively (Supplementary material). We found evidence to support previous findings involving the glutamate pathway,Reference Cai, Zhang, Yi, Lu, Wu and Chen20 such as SLC1A1. More importantly, we report the first indication of serotonin pathway involvement, as described in pure OCD. However, drawing firm conclusions about the role of specific variants will require work with larger samples. Nevertheless, our identification of several genetic variants in the serotonin pathway (SLC6A4, HTR2C) moderating the psychosis–obsession–compulsion pathway is notable, and may offer clues to future preventive or therapeutic approaches. The converging evidence from this and other studies indicates that interventions directed at enhancing serotonin function are crucial for the effective treatment of clozapine-induced OCS,Reference Englisch, Esslinger, Inta, Weinbrenner, Peus and Gutschalk21 as in pure OCD. Nevertheless, we did not specifically explore the effect of medication modifications on OCS severity, and further research is needed in this area.
A better understanding of the different phases of the phenomenon, in which compulsions arise as a by-product of florid paranoid psychosis and then perpetuated in predisposed subjects by clozapine’s anti-serotonergic action, may inform clinicians' therapeutic decisions.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjp.2024.30.
Data availability
The data that support the findings of this study, together with access to the code and CRD database, are available from the corresponding author on reasonable request.
Acknowledgements
We thank all the patients who contributed to the study and Pedro Fernandez-Bruna for his creative support with the figures presented here.
Author contributions
Conceptualisation of the study: E.F.-E., I.J.-B., Y.W., N.A.F. and T.W.R. Study design: E.F.-E., Y.W., T.W.R., M.B., J.P. and N.S. Clinical assessments: E.F.-E. Genotyping: E.S., P.G., S.M., M.-P.R. and C.B.G. Statistical analysis: E.F.-E., S.C. and R.N.C. Writing article: E.F.-E., S.C., R.N.C. and T.W.R. All authors approved the final version of the article.
Funding
E.S. was supported by an intramural research award from Universidad San Jorge. M.B., I.J.-B. and N.S. were supported by a studentship from Mental Health Research UK. S.C. and R.N.C. received research funding from the UK Medical Research Council (grants MC_PC_19213, MR/W014386/1). E.F.-E. is supported by the 2022 MRC/NIHR CARP award (MR/W029987/1), and this research was supported by the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014, NIHR203312). The views expressed are those of the author(s) and not necessarily of the NIHR or the Department of Health and Social Care.
Declaration of interest
E.F.-E. is the deputy editor of BJPsych but did not take part in this paper's review or decision-making process. E.F.-E. has received consultancy honoraria from Boehringer-Ingelheim (2022), Atheneum (2022) and Rovi (2022–23), speaker fees for Adamed (2022–23) and Otsuka (2023) and training and research material from Merz (2020).








 Open access
Open access
eLetters
No eLetters have been published for this article.