


The Mediterranean diet is the typical dietary pattern of the Mediterranean countries. The first reference to this type of diet as such was in 1938, when Leland Allbaugh studied the inhabitants of the island of Crete and their eating habits. Later, in 1957, Ancel Keys developed the concept of the Mediterranean diet in the Seven Countries Study( Reference Keys, Menotti and Aravanis 1 , Reference Keys, Menotti and Karvonen 2 ). In that study, Keys et al. analysed the relationship between deaths from CHD and serum cholesterol in fifteen populations in seven countries, at the individual level and for the population as a whole. The Mediterranean diet is characterized by daily consumption of fruit, vegetables, wholegrain cereals and pulses; a high consumption of MUFA, primarily from olive oil; moderate consumption of fresh fish and dairy products (especially cheese and low-fat dairy products), poultry and eggs; a moderate daily consumption of alcohol, normally red wine with meals; and a low consumption in frequency and quantity of red meats and sausages( Reference Gonzalez, Argilaga and Agudo 3 – Reference Buckland, Bach-Faig and Serra Majem 6 ). The basic characteristics of this dietary pattern are common to all countries of the Mediterranean basin, despite certain variations.
Diet is known to be a major determinant of an individual's health status and inadequate eating habits (excessive, deficient or both) are associated with numerous pathologies that may have high mortality rates. At present, a number of benefits of the Mediterranean diet are acknowledged, specifically with regard to mortality from all causes( Reference Trichopoulou, Costacou and Bamia 7 , Reference Sofi, Cesari and Abbate 8 ), CVD( Reference Serra-Majem, Trichopoulou and Ngo de la Cruz 9 – Reference Serra-Majem, Roman and Estruch 12 ), type 2 diabetes mellitus( Reference Martinez-Gonzalez, de la Fuente-Arrillaga and Nunez-Cordoba 13 – Reference Salas-Salvado, Bullo and Babio 15 ) and obesity( Reference Schroder, Marrugat and Vila 4 , Reference Buckland, Bach-Faig and Serra Majem 6 ), as well as some types of cancer including breast, endometrial, ovary and prostate cancer( Reference Benetou, Trichopoulou and Orfanos 16 – Reference Trichopoulou, Lagiou and Kuper 19 ), according to the results of many epidemiological studies and clinical trials. In addition, there are known benefits of the Mediterranean diet on pregnancy outcomes( Reference Timmermans, Steegers-Theunissen and Vujkovic 20 – Reference Chatzi, Mendez and García 22 ).
Nevertheless, this healthy dietary pattern is on the wane in Southern European countries. In the population of Spain, a decrease in adherence to the Mediterranean diet was corroborated using FAO food balance sheets for two periods, 1961–1965 and 2000–2003( Reference da Silva, Bach-Faig and Raido Quintana 23 ). This decrease is associated with a trend towards more sedentary or unhealthy lifestyles( Reference Buckland, Bach-Faig and Serra Majem 6 , Reference da Silva, Bach-Faig and Raido Quintana 23 , Reference Galán, Rodríguez-Artalejo and Tobías 24 ). The decrease in adherence to the Mediterranean diet affects all age groups. One particularly important group is women of fertile age: first because of the impact of diet on the health of the woman, the pregnancy and the newborn; and second because women of this age are more prone to accept advice regarding their health( Reference Cuco, Fernandez-Ballart and Sala 25 – Reference Phelan 28 ). This indeed points to a need to promote the Mediterranean diet among pregnant women and women of childbearing age. We surmise that identifying the factors associated with decreasing adherence to the Mediterranean diet would be key in developing programmes aimed at improving the level of adherence. No previous studies look at this particular aspect of healthy diet promotion. The aim of our study was therefore to analyse the factors associated with low adherence to a Mediterranean dietary pattern in healthy Spanish women before pregnancy.
Experimental methods
We conducted a prospective series of 1175 pregnant women in the catchment area of Virgen de las Nieves University Hospital of Granada (southern Spain). This regional hospital has three units: a General Hospital, a Hospital of Orthopaedic Surgery and Rehabilitation, and a Maternity Hospital; it provides coverage for the northern half of the province of Granada, Spain, with a population of 400 000 and approximately 4000 births per year( 29 ).
The reference population consisted of all the healthy pregnant women living in this area and attending their 20th gestational week visit at the hospital during the recruitment period, from June 2004 to March 2007. According to the Andalusian Maternal and Neonatal Health Programme, apart from routine prenatal visits to the primary health-care centre, all pregnant women should attend a prenatal visit at the hospital around the 20th week of gestation for ultrasound examination. The study was conducted according to the guidelines laid down in the Declaration of Helsinki. Ethical approval was given to the study by the Ethics Committee of the University of Granada and Virgen de las Nieves Hospital. All women signed a written consent form before participating.
The selection criteria were as follows: singleton pregnancy, Spanish nationality, 18 years of age or older, absence of complicated pregnancies that required rest, and absence of metabolic, chronic or acute diseases that might limit daily activities. From the original set of women, one in every five was systematically recruited, selected according to the order of their hospital visit for the ultrasound examination at week 20–22 of gestation, with a mean of 21·0 (sd 3·7) weeks. During the recruitment period a total of 1222 women were selected from the reference population, although finally 1175 women fulfilled inclusion criteria and chose to take part in the study.
All the pregnant women were contacted by two previously trained interviewers just before the ultrasound examination. After agreeing to participate, each woman was interviewed face to face and a structured questionnaire was used to collect the information. A pilot sample of fifty women (not included in the present study) had previously been interviewed during a 2-month period to train the interviewers and check the consistency of the information gathered.
Information about sociodemographic, obstetric and lifestyle variables (tobacco, diet, alcohol and physical activity) was collected. The information on diet was gathered by means of an FFQ that had previously been translated, adapted and validated in a sample of 147 Spanish women aged 18–64 years( Reference Martín-Moreno, Boyle and Gorgojo 30 ) and used in other studies in Spanish populations( Reference Razquin, Martinez and Martinez-Gonzalez 31 – Reference Garaulet, Hernandez-Morante and Tebar 34 ). Participants were asked about the frequency and amount of intake of 118 types of food during the year previous to the pregnancy; the frequency of intake of these foods (with reference to a table of equivalent portions) was then recorded as daily, weekly or monthly.
Dietary pattern was assessed using the Mediterranean Diet Adherence Index developed by Serra-Majem et al. ( Reference Serra-Majem, Ribas-Barba and Salvador 35 ). This index is based on Spanish dietary guidelines and includes the usual intake of fifteen food groups: (i) Fresh fruit and fruit juice; (ii) Vegetables, tomato juice (gazpacho) and lettuce; (iii) Nuts and olives; (iv) Fish and pulses; (v) Yoghurts and cheeses; (vi) Wine and cava; (vii) Olive oil; (viii) Other oils; (ix) Bread, pasta and rice; (x) Wholegrain bread, pasta and rice; (xi) Meats, sausages and cold cuts; (xii) Potatoes; (xiii) Baked goods, cookies and sweets; (xiv) Salty snacks; and (xv) Alcoholic beverage consumption and frequency. Dietary variables were energy-adjusted before scoring by using the residuals from the regression of nutrients v. total energy intake (residual method)( Reference Willett 36 ).
We calculated the mean intake per day for each food group. Ratings were assigned to each based on the tertile of consumption and on whether or not the group is considered characteristic of the Mediterranean diet. For the healthy food groups (items 1 to 7, 9, 10 and 12 of the index), the woman received 1 point if she was in tertile 1 (lowest consumption), 2 points for tertile 2 and 3 points for tertile 3 (highest consumption). The computation was inversed for non-healthy food groups. Accordingly, the maximum score was 45 points (the most beneficial effects). Recording by tertiles allowed us to distinguish between women with a low, mid or high level of adherence to the Mediterranean diet.
Our physical activity questionnaire was based on the Paffenberger Physical Activity Questionnaire( Reference Pereira, FitzerGerald and Gregg 37 ), which identifies the type, frequency and duration of different physical activities during leisure time, household tasks and care-giving, occupational and other activities (watching television, using a computer, driving, sleeping, going out with family and friends). We focused on leisure-time physical activity before pregnancy, assigning each kind of activity reported in the questionnaire a specific intensity score (metabolic equivalent of task; MET) based on Ainsworth's Compendium of Physical Activity. This information was converted into MET hours per day (MET-h/d) scores( Reference Ainsworth, Haskell and Whitt 38 ), divided into tertiles, and graded as minimal physical activity (tertile 1), medium physical activity (tertile 2) and maximum physical activity (tertile 3).
Current smokers were defined as those who smoked at least one cigarette daily, and the following categories were established for smoking habit: 0 cigarette/d, ≤20 cigarettes/d and >20 cigarettes/d. The educational level of the woman was registered as: primary academic level (8 years or less of basic education); secondary (4 years of secondary education); and university, undergraduate or graduate studies. Social class was classified based on the classification of the Working Group of the Spanish Society of Epidemiology from lowest (V) to highest (I): Class I (managerial and senior technical staff and freelance professionals); II (intermediate occupations and managers in commerce); III (skilled non-manual workers); IV (skilled manual workers); and V (unskilled manual workers)( Reference Álvarez-Dardet, Alonso and Domingo 39 ). We collected information about occupation for both members of the couples and the social class category was determined by the highest class declared by either one of them. Previous pregnancies and miscarriages were also registered. BMI was calculated as weight (in kilograms) just before pregnancy divided by the square of height (in metres). Both weight and height were obtained from medical records of the women if possible, and self-reported if not. Cut-offs set by the WHO were used to determine overweight and obese women( 40 ). Women with BMI ≥ 30 kg/m2 were classified as obese, and those with BMI from ≥25 kg/m2 to <30 kg/m2 as overweight.
We calculated the mean and standard deviation for the quantitative variables of study. The absolute and relative frequency distributions were estimated for qualitative variables. ANOVA was performed to compare the mean energy and Mediterranean Diet Adherence Index score for each of the independent variables. Significance was set at P < 0·05. Crude and adjusted odds ratios and 95 % confidence intervals were computed by models of polytomic regression to identify factors associated with low or mid level of adherence to a Mediterranean diet. Epidemiological and statistical criteria were used to model variable selection. High level of adherence to the Mediterranean diet was taken as the reference category for dependent variables. Analyses were performed using the statistical software package SPSS version 15.
Results
During the period of recruitment, the 1222 women who met the selection criteria were invited to participate in the study. Of these women, thirteen chose not to participate (1·06 %), and nineteen did not complete the interview face to face, or by telephone at a later attempt (1·55 %). Some basic information was lacking in fifteen cases. Therefore, 1175 (96·2 %) of the eligible women were included in the analysis.
Table 1 shows the Mediterranean Diet Adherence Index score and its distribution in terms of demographic, social and obstetric variables. The lowest and highest values recorded were 20 and 36 points, respectively (45 points being the maximum score possible), and the mean obtained was 28·2 (sd 3·2) points. Figure 1 shows the mean number of daily servings for each of the fifteen food groups established. It is seen that the healthy food groups predominating are vegetables, bread and fruit, although the mean number of daily servings did not meet dietary recommendations. The most frequent unhealthy food groups were meat and sweets. The main source of dietary fat was olive oil, with very low use of other fats (sunflower oil, butter). Moderate consumption of red wine with meals was a relevant finding.
Table 1 Mediterranean Diet Adherence Index score( Reference Serra-Majem, Ribas-Barba and Salvador 35 ) and total energy intake before pregnancy among healthy Spanish women (n 1175), Virgen de las Nieves University Hospital of Granada, southern Spain, June 2004 to March 2007
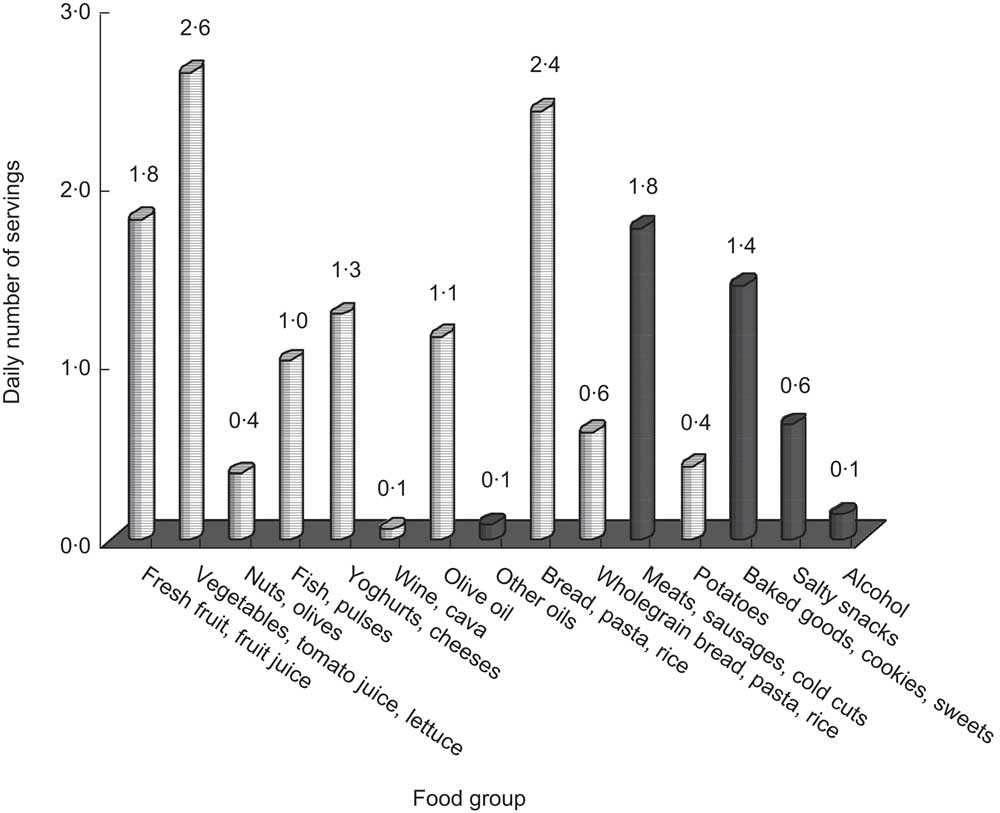
Fig. 1 Average daily number of servings of food groups (![]() , healthy food groups;
, healthy food groups; ![]() , unhealthy food groups) of the Mediterranean Diet Adherence Index(
Reference Serra-Majem, Ribas-Barba and Salvador
35
) before pregnancy among healthy Spanish women (n 1175), Virgen de las Nieves University Hospital of Granada, southern Spain, June 2004 to March 2007
, unhealthy food groups) of the Mediterranean Diet Adherence Index(
Reference Serra-Majem, Ribas-Barba and Salvador
35
) before pregnancy among healthy Spanish women (n 1175), Virgen de las Nieves University Hospital of Granada, southern Spain, June 2004 to March 2007
Table 2 shows the main variables considered depending on the level of Mediterranean diet adherence divided into tertiles: low, middle and high adherence. Greater age, higher educational level and higher social class of the woman were associated with a higher level of adherence to the Mediterranean diet (P < 0·001). On the contrary, sedentary lifestyle and smoking were associated with a lower level of adherence (P < 0·001). This relationship remained after adjusting for potential confounding factors (Table 3).
Table 2 Sample description for each level of adherence to the Mediterranean diet before pregnancy among healthy Spanish women (n 1175), Virgen de las Nieves University Hospital of Granada, southern Spain, June 2004 to March 2007
MET, metabolic equivalent of task.
Differences between low, middle and high adherence groups were significant: ***P < 0·001.
†Minimum age 18 years, maximum age 45 years, arithmetic mean age 29·81 (sd 5·14) years.
Table 3 Factors associated with low and middle adherence to the Mediterranean diet before pregnancy among healthy Spanish women (n 1175), Virgen de las Nieves University Hospital of Granada, southern Spain, June 2004 to March 2007
MET, metabolic equivalent of task.
Association was significant: *P < 0·05.
†Reference category: high adherence to the Mediterranean diet.
‡Adjusted for age, smoking status, physical activity and academic level.
§Energy intake was introduced as a continuous variable. The OR indicates the increase for each 418 kJ (100 kcal) increment in daily energy intake.
A direct relationship was found between age and degree of adherence to the Mediterranean diet; it was observed that as age increased, pregnant females’ adherence increased, and in turn, the younger the age, the worse the adherence (P < 0·001). Smoking habit and sedentary lifestyle had a positive relationship with low adherence. Women smoking >20 cigarettes/d showed a low adherence to the Mediterranean diet 5·36 times more often than women who had never smoked, OR = 5·36 (95 % 1·91, 15·07). The frequency of low adherence was double for women with minimal physical activity, OR = 2·07 (95 % CI 1·34, 3·17). This relationship was also seen for middle adherence and sedentary lifestyle. BMI was not associated with adherence to the Mediterranean diet in either the crude or the adjusted analysis. Factors associated with middle adherence were similar, although the force of association was minor in both the crude and adjusted analyses.
Discussion
Our results show that Mediterranean diet adherence was poor among childbearing women in the northern part of the province of Granada, Spain. Low Mediterranean diet adherence was more frequent in younger women, and it was associated with unhealthy practices such as smoking or physical inactivity, as well as with other possible determinants of health such as social class and educational level.
To our knowledge, the present study is the first one performed in Spain to assess the factors associated with adherence to the Mediterranean diet in healthy young women using the index developed by Serra-Majem et al.( Reference Serra-Majem, Ribas-Barba and Salvador 35 ). While the benefits of good adherence to the Mediterranean diet are well known in the general population, it is important to stress its importance among healthy women of childbearing age( Reference Gonzalez, Argilaga and Agudo 3 – Reference Trichopoulou, Lagiou and Kuper 19 , Reference Mariscal-Arcas, Rivas and Monteagudo 41 , Reference Serra-Majem, Bes-Rastrollo and Roman-Vinas 42 ).
Although we worked with Spanish childbearing women, our results for the Mediterranean dietary pattern are in line with those of observational studies in populations of different characteristics or for other healthy dietary patterns in Spain( Reference Gonzalez, Argilaga and Agudo 3 , Reference Serra-Majem, Ribas-Barba and Salvador 35 , Reference Kourlaba and Panagiotakos 43 – Reference Sánchez-Villegas, Delgado-Rodríguez and Martínez-González 49 ) and Europe( Reference Laaksonen, Prattala and Karisto 50 ). We found a marked protector effect for age: as age increased, the probability of Mediterranean diet adherence increased. Dietary habits among healthy childbearing women are worsening, mainly among younger women. In Spain, consumption of fat, red meat, eggs and dairy products is on the rise, while intakes of cereals, vegetables, pulses, fruits and seafood have decreased, especially in the younger population. Andalusia is no exception to the trend affecting most developed countries.
Sedentary lifestyle( Reference Sanchez-Villegas, Martinez and De Irala 47 , Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera 48 ), smoking habit( Reference Sanchez-Villegas, Martinez and De Irala 47 , Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera 48 , Reference Laaksonen, Prattala and Karisto 50 ), low educational level and social class( Reference Gonzalez, Argilaga and Agudo 3 , Reference Serra-Majem, Bes-Rastrollo and Roman-Vinas 42 , Reference Johansson, Thelle and Solvoll 51 , Reference Erkkila, Sarkkinen and Lehto 52 ) and low adherence to the Mediterranean diet are factors that often accompany unhealthy lifestyles. The positive association we detected between physical activity and Mediterranean diet adherence is noteworthy in this context, suggesting that public health or preventive interventions must address diet and physical activity in conjunction. Poor diet and sedentary lifestyle have been identified as the main risk factors for obesity and chronic diseases, the greatest health problems in our population( Reference Belahsen and Rguibi 53 , Reference Ballesteros Arribas, Dal-Re Saavedra and Pérez-Farinós 54 ). Likewise, a number of previous studies show an association between smoking and unhealthy dietary pattern( Reference Sanchez-Villegas, Martinez and De Irala 47 , Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera 48 , Reference Laaksonen, Prattala and Karisto 50 ), highlighting lower fruit and fresh vegetable intake.
We found no association between obesity and quality of the diet. Other authors underline this lack of association( Reference Kontogianni, Melistas and Yannakoulia 55 , Reference Rossi, Negri and Bosetti 56 ), but in general it is assumed that the Mediterranean diet is associated with a lesser frequency of obesity( Reference Schroder, Marrugat and Vila 4 , Reference Buckland, Bach-Faig and Serra Majem 6 ). This may be because trends in the overall population do not always appear at the individual level, as is the case in the association between diet and cholesterol levels( Reference Pérez-Jiménez, Ros and Solá 57 ), or there may be an information bias in the sense that overweight is associated with under-reporting of food intake. Such a bias is likely to be accentuated regarding unhealthy food intake, and must be acknowledged in view of our study design.
Finally, the association between lower socio-economic level, low adherence to a healthy diet and lower level of education (primary, secondary) supports previous findings: poor dietary habits, sedentary lifestyle and smoking are more common in lower socio-economic strata, reflecting considerable inequalities in the distribution of health determinants( Reference Gonzalez, Argilaga and Agudo 3 , Reference Power and Matthews 58 , Reference Karlsdotter, Martín Martín and López Del Amo González 59 ).
As potential limitations of our study we should cite its observational nature, with dietary information recorded retrospectively (diet during the year previous to pregnancy self-reported at the 21st week of gestation). This would entail some memory bias, possibly strengthened by the social desirability of avoiding substantial intake of unhealthy foodstuffs. Such a bias would be differential, mostly affecting women with poor dietary habits, decreasing the variability of the sample and the probability of obtaining significant associations. On the other hand, we acknowledge that some confounding variables considered could be measured imperfectly and the likelihood of residual confounding cannot be ruled out. As advantages of our study we should underline that: (i) our sample is representative of all healthy women in the reference area of Virgen de las Nieves University Hospital (southern Spain), meaning that the results can be extrapolated to a greater population; (ii) questionnaires previously validated in Spanish populations were used to measure the physical activity( Reference Pereira, FitzerGerald and Gregg 37 ) and food frequency( Reference Martín-Moreno, Boyle and Gorgojo 30 ); and (iii) trained interviewers collected the information. We opted to use a dietary quality index as a dependent variable for our study because we think it summarizes the quality of the diet better( Reference Ortiz-Andrellucchi, Sanchez-Villegas and Ramirez-Garcia 27 ). Our understanding is that nutrition is derived from combinations of food and elements that interact( Reference Bach, Serra-Majem and Carrasco 45 – Reference Sanchez-Villegas, Martinez and De Irala 47 ), and there is growing interest in using dietary quality indices to evaluate whether adherence to a certain dietary pattern lowers the risk of disease.
On the other hand, the Mediterranean Diet Adherence Index used( Reference Serra-Majem, Ribas-Barba and Salvador 35 ) is dependent on the mean intake of people in the sample, which impedes comparison with other populations. That is, women in the lower Mediterranean diet adherence tertile may show better Mediterranean diet adherence than other populations. Notwithstanding, dietary pattern must be appraised in a cultural context, planning health-care interventions in view of the population, tradition and the availability of certain foods.
The prevalence of sedentary lifestyle and low adherence to the Mediterranean diet in our study population was high, in particular in younger women. This suggests that Mediterranean diet adherence could be decreasing. Our results urge that measures be taken to promote healthier lifestyles and that physical activity and nutritional education should be key components of maternal and child health-care programmes. In our particular setting, Andalusia, recommendations should be set forth to enhance awareness of healthy diet and lifestyle among childbearing women within the framework of a regional nutrition and health policy. Knowledge of the factors associated with low adherence to a Mediterranean diet is crucial for the design and implementation of health promotion and prevention programmes to improve the health status of the population in general, and childbearing women in particular. Modifying dietary habits is a socially and politically difficult task, calling for structural and individual interventions( Reference Serra-Majem, Ribas-Barba and Salvador 35 ).
Childbearing women could be an excellent target group for intervention; such preventive action would have a dual effect, present and future, meaning better health for the mother in future pregnancies and for her offspring. The childbearing years can thus be seen as an ideal time to introduce some stimulus to modify behaviour in a positive way, taking advantage of the motivational factor( Reference Cuco, Fernandez-Ballart and Sala 25 , Reference Benelam 60 ). In conclusion, despite the well-known benefits of the Mediterranean diet, certain factors are contributing to its demise. To design adequate interventions in the future, we must take into account that younger age, low social class, primary educational level and the presence of unhealthy lifestyles, including smoking and lack of physical activity, are associated with low adherence to the Mediterranean diet.
Acknowledgements
Sources of funding: This research was funded by FIS Scientific Research Project PI 03/1207 and Junta de Andalucía Excellence Project CTS 05/942. Ethics: Ethical approval was given to this study by the Ethics Committees of the University of Granada and Virgen de las Nieves University Hospital. Conflicts of interest: The authors have no conflict of interest to declare. Authors’ contributions: R.O.-R., J.G.F and C.A.P collected the information, analysed the data and wrote the first draft of the manuscript. J.M.M. and A.B.-C. participated in the design of the study and critically reviewed the manuscript. J.J.J.-M. coordinated the study and is the main author responsible for the study design and drafting of the manuscript. All authors have seen and approved the content and contributed to the work. Acknowledgements: The authors thank Jean Sanders for improving the use of English in the manuscript.




