

Cognitive–analytic therapy (CAT) is a brief focal therapy informed by cognitive therapy, psychodynamic psychotherapy and certain developments in cognitive psychology. It was developed by Anthony Ryle specifically in response to the needs of the National Health Service (NHS) for treatment approaches of short duration. However, it has advanced far beyond its initial aims and is now a well-developed self-contained methodology backed by a fully structured theory of mental functioning and therapeutic change.
Initially, CAT concerned itself with the treatment of neurotic disorders, and it was in this context that the early theoretical and technical elements were established (Reference RyleRyle, 1990, Reference Ryle and Ryle1995a ). For the past 10 years CAT has turned its attention to the treatment of personality disorders, specifically borderline personality disorder. The need to understand and treat people with this disorder has had a major impact on the theory and practice of CAT (Reference RyleRyle, 1997). In particular, CAT incorporated ideas derived from both object relations theory and the work of Vygotsky (the Russian psychologist who founded activity theory (Reference RyleRyle, 1991)).
Basic CAT theory
Two main theoretical structures form the basis of CAT. The first of these is the procedural sequence model, which is an attempt to understand aim-directed action. This model supposes that all aim-directed activity is the consequence of ordered sequences of aim generation, environmental evaluation, plan formation, action, evaluation of consequences and, if necessary, remedial procedural revision (Fig. 1).
Procedural sequences are developed on the basis of experience, and the crucial check step at the end of a sequence means that it is revised if it is not effective. Procedural sequences are therefore usually effective and adaptive. However, some procedural sequences are faulty and they are repeatedly deployed without revision. These cause the repetitive difficulties that characterise some psychological disorders. Procedural sequences include cognitive, motivational, affective and behavioural elements, and Ryle argued that one reason why all psychotherapies have roughly equivalent efficacies is that, for any particular condition, different kinds of psychotherapy may act on different aspects of procedural sequences, but they all beneficially alter a common underlying faulty procedure.
Unrevised faulty procedures
From a review of case notes Ryle described three main kinds of faulty procedure. The first, ‘traps’, represent repetitive cycles of behaviour in which the consequences of the behaviour feed back into its perpetuation. The depressed-thinking trap is a good example of this (Fig. 2). Feeling depressed, the subject acts in ways that make failure and defeat more likely, so that when he or she evaluates the results of the behaviour these are objectively depressing in him or herself. Similar traps describe phobic avoidance, social isolation and other problems.
The second kind of faulty procedure is the ‘dilemma’, which involves the presentation of false choices or of unduly narrowed options. In dilemmas the check step operates but immediately switches the individual to an opposing and equally maladaptive procedure, the check step of which in turn switches back to the first procedure. The placation trap will serve as an example here (Fig. 3). Fearing the consequences of aggression, the individual placates others and allows them to take advantage of him or her; he or she consequently grows more and more cross and eventually switches to an alternative overaggressive procedure with an outburst of anger (often misplaced). The rage, particularly if it is misplaced, often has consequences that are negative or read as negative and the check step switches the individual back to the inappropriate placatory behaviour of the dilemma.
The final kind of maladaptive procedural sequence that Ryle described is the ‘snag’: the subtle negative aspect of goals. Snags are anticipations of the future consequences of actions that are so negative that they are capable of halting a procedure before it ever runs. Then, because the procedure is halted it is never subjected to checks. An example might be a gay man who is frightened to come out to his family because he thinks “If I tell my mother it will kill her.”
Restricted repertoire of procedures
So, CAT supposes that neurotic difficulty results from the operation of unrevised maladaptive procedural sequences. It was soon recognised that a second cause of difficulty was undue restriction in the procedural repertoire. Causes of procedural restriction include: impoverished environmental opportunities for learning new procedures, for example in cases of emotional deprivation and neglect; deliberate attempts by caregivers to restrict procedural repertoires, for example by injunctions to secrecy in cases of sexual abuse; and difficulty in new emotional learning owing to previously learned faulty procedures, as exemplified in case vignette 1.
Case vignette 1
Jenny (18) had spent her entire life in a children's home. She presented with a complaint of compulsive promiscuity, and at the first interview her intense loneliness was also apparent. She had few friends, only acquaintances. The interpersonal procedural sequences that had served her well in the home, where staff often came and went, favoured both rapid and relatively non-discriminating attachment and equally rapid detachment. Indeed, she was actively discouraged from making close friendships with members of staff. Now, in ‘normal’ life, she continued to deploy these procedural sequences and, ironically, by deploying them she subjected herself to the same experience of loneliness among a shifting population of uncaring others that she had experienced as a child.
Borderline personality disorder
While the original formulation of CAT proved effective for a variety of neurotic disorders, more severe personality disorders did not respond well to the piecemeal approach of defining and trying to mediate individual maladaptive procedural sequences. Patients displayed bewilderingly diverse states of mind and induced powerful mental states in their therapists. To improve CAT's capacity to deal with these patients the theory of reciprocal roles was developed.
Ryle described how our early learning about the social world is stored in the form of internalised templates of reciprocal roles. These consist of a role for self, a role for other and a paradigm for their relationship. Reciprocal roles may be benign and functional or harsh and dysfunctional. Examples include caregiver/care receiver, bully/victim, admiring/admired and abuser/abused. In general, reciprocal roles are commonly shared templates. Therefore, when an individual takes up one pole of a reciprocal-role pairing, the person with whom he or she is relating feels pressure to adopt the congruent pole. When the roles in use are moderate and socially congruent this pressure to reciprocate remains largely unnoticed and is generally appropriate. However, in the therapeutic situation, where fewer environmental cues guide role choices and where the patient's own reciprocal-role repertoire is both unusually harsh and emotionally extreme, the therapist can feel a strong pressure to reciprocate in ego-alien ways. This has been explained in psychoanalytic theory by the concepts of countertransference and projective identification. Ryle (1994a) has argued that although these concepts lock on to important phenomena, the explanations associated with them are unduly mystifying. He believes that the theory of reciprocal roles offers a less complicated, more complete and more transparent explanation of the pressure involved.
Levels of deformity
In its theory of personality disorders, and borderline personality disorder in particular, CAT suggests typical deformities of the internalised reciprocal-role structure. Ryle (1997) allocates these to three levels.
The first level is the reciprocal-role repertoire. In normal individuals a wide range of flexible and adaptive reciprocal-role templates is deployed as needed. In people with borderline personality disorder only a small number of highly maladaptive reciprocal roles are available for deployment. This means that within any social situation these people have only limited and often inappropriate templates to call on when planning action.
The second level is that of switching between reciprocal roles and their graceful deployment. In normal individuals there are smooth transitions between roles, for example, in a teacher's relationship to children in the classroom and to colleagues in the staffroom. In borderline disorder, people are poor at switching between states and often show an oversensitive (‘hair-trigger’) response to small stimuli, resulting in unwarranted state changes. One patient left a psychotherapy session apparently in a reasonable state of mind. However, on her way home the bus took her past a graveyard; seeing it, she at once felt suicidally depressed and was later found wandering along railway track.
On Ryle's third level are our capacities for conscious self-reflection and self-control. These capacities allow us to act intelligently in unfamiliar situations and also deliberately to revise ways of acting that have proved unprofitable. Unsurprisingly, self-reflection is the main point of action for psychotherapeutic intervention. It is linked with abilities such as narrative competence and reflective self-functioning, which are increasingly thought to be important in borderline states (Reference Fonagy and TargetFonagy & Target, 1997).
In normal individuals, self-reflective functioning can be employed with reasonable ease and frequency. In people with borderline personality disorder, it may be entirely absent. The reasons for this are not difficult to see. Self-reflective capacities are acquired in childhood and reinforced by later development. Self-reflection is learnt chiefly in social interaction with others: the child experiences him- or herself as being reflected upon by others and observes others as they reflect upon themselves. For many adults with the most severe borderline disorder, abuse of various kinds in childhood, combined perhaps with constitutional difficulties in self-soothing that made achieving a calm state of mind more problematic than for normal children, deprived them of the key emotional and social learning experiences that would have laid down strong level-three capacities.
Deficiencies in levels two and three result in the emotional instability, irritability and unpredictability typical of borderline personality disorder, while deformities of the underlying repertoire of reciprocal-role templates result in many of the emotional features of the disorder such as extreme guilt and self-loathing, rage and hatred, abusive behaviour and idealised overattachment. The therapist's experience of being dragged through a bewildering and intense emotional minefield results from the successive induction of emotionally intense (often exceedingly dysphoric) reciprocal-role states in the therapist as the patient moves in an uncontrolled and unreflective way through his or her own disastrous reciprocal-role repertoire.
Case vignette 2
Paul (32) consulted in a blankly suicidal state of mind after his girlfriend left him when he assalted her yet again. He had set a date to die and was, in effect, challenging the assessor to talk him out of it. The assessor felt cross but overrode her feelings and tried to continue the assessment. In the middle of the interview Paul noticed a book on the shelf, The Severe Personality Disorders. He suddenly became tearful, saying “That's what I am, isn't it? A disorder.” After a moment of genuine grief, Paul became angry and contemptuous of the ‘pathetic’ help being offered.
This snippet of Paul's interview illustrates the roller-coaster emotions he experienced. The assessor formulated the reciprocal roles successively enacted as: rebellious and defiant in relation to challenged authority, followed by miserable and dependent in relation to a (probably) uncaring other, and finishing up with furious and contemptuous in relation to a contemptible and interfering other.
Less severely disorganised personalities and neurotic conditions
The practice of CAT has been shaped by two fundamental considerations. The first is the necessity for therapies to be applicable to the large number of patients who could potentially benefit. To that end, CAT was especially developed with the NHS in mind. As a result, the therapy is brief, focal and relatively easy to teach (at least at a basic level). Also there are very few exclusion criteria and interest among CAT therapists has always centred on treating more severely ill patients. A second consideration has been CAT's self-avowed educational perspective on the process of change in therapy (Reference RyleRyle, 1994b ). CAT therapists see their part as the creation, with the patient, of shared tools for self-reflection, which are then used to understand the patient's difficulties and to make beneficial changes. The key notion therefore is the idea that patient and therapist collaborate in a joint venture in which both bring specialist knowledge to a shared arena. In taking this stance, CAT tried to move away from what it saw as the authoritarian position of psychoanalysis, in which the analyst appears to know the content of the patient's mind and makes interpretations based on a logic that is not necessarily revealed to the patient. At first glance, CAT's educational approach makes it look very like cognitive–behavioural therapies (CBTs), but Ryle is critical of these for being too prescriptive. In fact, CBT practice in relation to the flexibility and type of conceptualisations offered varies. Some CBT therapists offer their patients standard models for anxiety or depression – a practice Ryle would criticise. Others, in the schema-focused tradition, offer conceptualisations very similar to those used by CAT therapists. Ryle's criticisms would be less applicable to these latter variants although, ironically, they share with CAT a lack of empirical validation.
Scaffolding
The work of Vygotsky and the school of activity theory (e.g. see Engestrom et al, 1999) has been extremely important in the development of CAT's approach to therapeutic change. Vygotsky proposed the notion of scaffolding, by which he intended to convey the provision by the teacher of just sufficient support to allow students to do with the teacher what they cannot yet do alone. Vygotsky's scaffolding consists in the provision of theoretical knowledge, which the student assimilates by repeated application in practical situations. In CAT, the shared tools for self-reflection that therapist and patient create are the theoretical scaffolding and are unique to each patient. From a CAT point of view, CBT runs the risk of using scaffolding that is too constrictive, while psychoanalytic therapy provides insufficient scaffolding.
Another element of the scaffolding provided for therapist and patient in CAT is the timetable of therapy.
The timetable of therapy
In the first session, as with most therapies, the therapist concentrates on three key tasks. First, a therapeutic alliance must be built in which the patient is helped to feel that work in therapy will be beneficial and worthwhile and that the therapist can be trusted. Next, the patient's story must be gathered. The final task is to give the patient an understanding of the nature, mechanism of action and process of CAT. CAT therapists use open questioning, descriptive reframing and any other methods that seem appropriate to gather history. They give an open account of the nature of therapy and they tend to check the state of the working alliance by asking what the patient thinks and feels about the session as it progresses. At the end of the first session the therapist is very likely to set homework. This will often involve filling in a questionnaire, known as the psychotherapy file, that describes common maladaptive procedures. It may also involve a number of further tasks (such as the drawing up of a life line) designed to flesh out the patient's history.
In the second session, the therapist continues to gather the patient's history, but also begins to work with the patient on constructing a list of the main problems (known as target problems) that the patient is experiencing. A homework commonly set at the end of the second session is the keeping of a diary that monitors the target problems and looks in particular at behaviours and feelings that trigger them.
By the third session, the gathering of the history should have begun to allow the patient and therapist to gain a sense of the main repetitive maladaptive cycles of thinking and acting that the patient gets into and of the main reciprocal roles that the patient deploys. To the extent that this has been possible, the third session can be spent jointly constructing a reformulation of the patient's difficulties.
In the time between the third and fourth sessions the therapist writes a letter to the patient, called a reformulation, which sets out the patient's difficulties as described to the therapist and the understanding of those difficulties that patient and therapist have reached.
The reformulation letter
The reformulation letter most often begins with a narrative account of the patient's life story, because this account makes clear the developmental origins of repetitive patterns. It moves on to outline the current situation, the main problems and the repetitive maladaptive procedures that underlie them. Many reformulation letters also contain a diagram that lays out the repertoire of reciprocal roles used by the patient, the procedural sequences that they deployed around those roles and the symptomatic consequences of those sequences. Patients respond to reformulation letters in a wide variety of ways, which are often related to their underlying problems. Very many of them find the experience of being written and thought about in this way both arresting and moving. They are, without exception, encouraged to annotate, improve, alter and interact with the reformulation letter in negotiation with the therapist until it can become the basis for the rest of therapy.
The following are extracts from the reformulation letter written to Jenny.
Dear Jenny, you came to therapy complaining that you find yourself having sex with people who you did not want to be having a relationship with. You told me you had no close friends and we agreed that you were very lonely. The home you were brought up in must have been a terrible experience for you. With no one secure that you could turn to it is clear that you grew up very fast and you learnt to get support and love wherever it was available. […]
We have talked about a pattern you learnt of clinging on to anyone who seems to show you affection and then of dumping them quickly as soon as it looked as though they might leave. I think that this pattern, which served you when you were a child, is now a problem for you. As soon as a man seems attracted to you, you cling on and end up having sex. Sometimes you part because neither of you has any great interest in a relationship. Other times (as with Simon) you leave something which could have been promising because of a slight disappointment. […]
Changing maladaptive procedural sequences
Once a reformulation has been established the task of therapy changes. Now the aim is for the patient, at first with the therapist's help but later independently, to become able to recognise the operation of maladaptive procedural sequences or reciprocal roles as they occur in everyday life. A useful feature of maladaptive procedural sequences is that they are frequently employed in a wide range of situations and can therefore be recognised in both major and minor guises. For example, given that most patients present with interpersonal problems it is not surprising that maladaptive procedural sequences come to be operative within the interpersonal setting of the therapy session. CAT therapists try to predict, on the basis of the reformulation letter, the likely transference and countertransference feelings and enactments that will become active during sessions. When accurately anticipated and identified, maladaptive procedures that operate within the session can be used as occasions for learning and change, and the possibility that they will interfere with therapy can be reduced.
Jenny's therapist was a woman, but even so she anticipated that she would be come a figure of both anticipation and disappointment to her patient. She was meticulous about inquiring how Jenny felt about breaks in the therapy and was exceedingly careful to discuss at length the end of therapy and feelings it might arouse in Jenny. Initially, Jenny tended to dismiss this sort of inquiry as “therapy stuff”, but after the therapist cancelled a session owing to illness it was possible to explore feelings of disappointment and a wish to leave therapy and not come back.
As patients improve their ability to recognise the operation of their maladaptive procedural sequences and reciprocal roles, they often spontaneously begin to try out new ways of behaving. The therapist can assist this process by positively encouraging change, using active role-play techniques or brainstorming solutions with the patient. The procedural understanding of the patient's difficulties often suggests ‘exits' in general terms, and the patient and therapist work together to develop these into particular lived out solutions.
By now, therapy is nearing its end (CAT is traditionally 16 or 24 sessions long). As with all brief therapies, termination has been explicitly discussed since the very first session, and CAT therapists handle termination issues in much the same way as other brief therapists. However, the reformulation provides CAT therapists with a major tool for anticipating the likely reactions of the patient to the loss of therapy, and patient and therapist can talk through these anticipated reactions at appropriate points during therapy, as was the case with Jenny.
The goodbye letter
In the penultimate session the therapist gives the patient another letter, known as the goodbye letter. This briefly outlines the reason the patient came to treatment and recounts the story of the therapy. It tries to give an account of what has been achieved during therapy and also to mention things that have not yet been achieved. The letter outlines the therapist's hopes and fears for the patient in the future, sketching out ways that understandings reached in therapy might be used helpfully. Many patients choose to give the therapist a goodbye letter of their own. A follow-up session is booked, generally for 3 months hence. This allows evaluation of the effects of therapy. There is often evidence of continued improvement during that period.
Severe borderline personality disorder
Practising CAT as described above is suitable for less severely disorganised personalities and neurotic conditions. However, when the patient suffers from borderline personality disorder a piecemeal approach to individual maladaptive procedures becomes ineffective. This is because as each procedural sequence is tackled the patient takes flight into different reciprocal-role structures; in effect, patient and therapist chase each other around the patient's diagram.
Nevertheless, these diagrams are particularly useful in adapting CAT for use with patients who have borderline personality disorder. With such patients, the focus should be integration and the therapeutic aim should be to enable patients to gain an overview of the wildly discontinuous self-states they can find themselves occupying. CAT therapists conceptualise this aim as the development of an ‘observing I’, who is concerned and involved but neither overwhelmed nor silenced.
Probably a key therapeutic technique in helping the development of an observing I is modelling. By watching as the therapist (more or less successfully) continues to describe what is going on for the patient without becoming drawn into enacting any of the patient's reciprocal role patterns and by trying to do this him- or herself, the patient builds up an inner state that embodies this stance. This technique of involved non-collusion is similar to a range of therapeutic modalities for borderline personality disorder. But CAT is distinctive in its use of the diagram as a guide for patient and therapist about what is going on in a session. CAT is also distinctive in combining elements of interpersonal and object relations theory in its understanding of the patient with a frank and educative model that supposes that the patient, at least in part, can be an active and cooperating partner rather than a consciously or unconsciously motivated opponent.
Let us return to Paul (case vignette 2). Despite misgivings, Paul was offered therapy. In order to help Paul's therapist, at the very first meeting the assessor drew a sketch of a tentative diagram of reciprocal roles known as a sequential diagramatic reformulation (SDR). There had not been time in the assessment to share this with Paul, but it became immediately relevant in the first therapy session when Paul, upset at seeing a different person from his assessor, began to denigrate and devalue the therapist. After the therapist had shared her version of the diagram, Paul was able to admit that he was frightened of coming to therapy because he thought the therapist would be sneering at him (Fig. 4).
Comparing CAT with other therapies
As its name implies, CAT shares elements of both cognitive and psychoanalytical psychotherapies. Psychoanalytical concepts, particularly those drawn from the independent group, have been central to the phase of CAT marked by the development of the SDR. The theory of reciprocal roles and of reciprocal-role induction allows CAT to conceptualise the psychoanalytical concepts of transference, countertransference and projective identification in ways that Ryle claims are less mystifying and more practically useful (Reference RyleRyle, 1994b , Reference Ryle1998). CAT therapists regard transference phenomena and their countertransferential responses as useful sources of information about the patient's reciprocal-role procedures. Importantly, the reformulation's specification of reciprocal-role procedures can also be used to predict the likely development of the transference–countertransference relationship and hence to anticipate difficulties and developments in therapy.
Another strand in CAT's relationship with psychoanalysis is Ryle's critical struggle with psychoanalytical thinking, especially of the Kleinian school, which has resulted in a key series of papers that engage with both Kleinian technique and theory (Reference RyleRyle, 1992, Reference Ryle1993, Reference Ryle1995b ). Ryle's principal argument with Kleinian theory lies in his view that in severe cases such as borderline personality disorder the symptomatic experiences and behaviours of patients are consequent on psychic “unintegration” and the formation of multiple-self states. This contrasts with the Klein/Bion perspective, in which borderline states are associated with psychic disintegration and attacks on linking (Reference BionBion, 1967). Ryle levels a similar set of criticisms at Fonagy's theory of a mind-based conceptualisation of borderline personality disorder (Reference FonagyFonagy, 1991). In this theory, the self turns on its own mental functions to obliterate the horror of acknowledging that the mind of the abuser conceived of and carried out abusive acts (Reference RyleRyle, 1998).
In recent years, CAT theorists have shown reduced interest in the less severe psychological conditions. CAT's chief causal explanation for such conditions appeals to procedural sequences that are malformed and not revised. There is a considerable body of theory within CAT that seeks for reasons why these procedures, which are set up to be self-correcting, are not revised for the better. However, signally absent among these reasons is any appeal to defence against unconscious conflict. It is CAT's resolute rejection of defence as a major mechanism in symptom formation that marks it out from psychoanalytic perspectives.
To these theoretical differences must be added some strong views about technical issues. In relation to psychoanalytical practice, Ryle regards the long intense treatments practised by an ‘invisible’ and studiedly neutral analyst as likely to generate abnormal phenomena, which themselves become the spurious basis for theory-making. A good example of these views appears in Ryle (1996), where he also sets out a key CAT distinction between interpretation and description. For Ryle, psychoanalytical interpretation risks involving the interpreter in claiming special knowledge about the interpreted that is not accessible to direct test by the interpreted subject. Description, on the other hand, he conceives of as a joint process, in which the close inspection of what is available to consciousness can reveal more and more of what is not so easily available. CAT therapists therefore characterise their activities as descriptive rather than interpretive.
CAT shares with cognitive therapy a stress on the detailed analysis of the conscious antecedents and consequences of symptoms, the production and sharing of a detailed descriptive formulation with the patient, the setting of homework and a focus on, and problem-solving approach to, difficulties. Ryle deliberately drew on Kelly's personal construct psychology (Reference KellyKelly, 1955) and his concept of the individual as scientist actively construing the world. This concept chimes well with the setting of behavioural experiments used in CBT. Marzillier & Butler's (1995) review of commonalities and differences between CAT and CBT identifies these similarities among others. They show CAT's commonalities both with schema-focused CBT (Reference YoungYoung, 1990) and with Teasdale & Barnard's (1993) interacting cognitive subsystems (ICS) model. They find few differences other than ones of emphasis in relation to these models, so that their overview of CAT is in favour of classifying it as one of the cognitive therapies.
However, Marzillier & Butler's cognitivist reading of CAT would not be shared by a significant number of CAT therapists. Ryle himself, presented with the ICS model, is sharply critical. He regards it as being far too focused on intra-individual interactions between internal automata, and in consequence inclined to neglect the crucial importance of the external world, particularly the social world, in structuring experience. Thus, for Ryle, CAT is different from CBT, and particularly the ICS model is different from CAT, because the latter emphasises social interaction rather than individual processes as the primary unit of analysis. However, this criticism of the ICS model may not be entirely warranted.
There are powerful points of similarity between schema-focused CBT and CAT, and it is probably more fair to characterise their differences as ones of emphasis. I have explored these differences with a colleague (Reference Allison, Denman, Mace, Moorey and RobertsAllison & Denman, 2001). To my eye the key differences between the two lie in the consistent CAT emphasis on interaction and on social interaction, embodied in the notion of a reciprocal role that is a block of procedural knowledge about how to ‘do’ a particular kind of relationship and what to expect from it. This can certainly be viewed as a kind of schema, although it is more complex in internal structure than a normal CBT schema. Interestingly, in an early paper Young (1986) suggested schema clusters that look very like reciprocal roles but does not seem to have followed this up in later work.
Cognitive therapists who work in the schema-focused tradition often find much to agree with in CAT. A not infrequent comment is that CAT therapists should therefore just get on with doing CBT, which is better validated – although the validation of schema-focused models is debatable. CAT therapists, however, continue to feel that the CAT perspective offers approaches to interpersonal and motivational issues that are better developed and more subtly nuanced than those used by CBT. This certainly would be Ryle's view, as expressed in his review of cognitive approaches to borderline personality disorder (Reference RyleRyle, 1998).
Who is suitable for CAT?
Traditionally, CAT therapists have taken on a very wide range of patients. As a result, CAT has been tried for many conditions, including anxiety disorders and depression, deliberate self-harm, abnormal illness behaviour (particularly in diabetes) and, most particularly, the personality disorders (Reference CowmeadowCowmeadow, 1994; Reference Fosbury and ColesFosbury, 1994; Reference RyleRyle, 1997). With all these conditions there has been some success. One contraindication is current drug or alcohol use to the point of active intoxication (Reference RyleRyle, 1997: p. 86). This is to some extent a matter of degree, the main issue being the difficulty of conducting sessions with an intoxicated patient. Poor or absent motivation, resulting in failure to attend sessions, may be another contraindication, because in a brief therapy missing too many sessions nullifies any effect. Even so, it is often worth seeing whether the reformulation stage of CAT draws the patient in sufficiently to make therapy viable.
The evidence base
There is a growing, but still far from adequate, evidence base in CAT. The current situation is well summarised by Margison (2000), who highlights the lack of randomised controlled trials (RCTs) validating CAT. Nevertheless, some studies do exist. An early paper (Reference Brockman, Poynton and RyleBrockman et al, 1987) showed that CAT conducted by trainees was as effective as Mann's brief psychotherapy (Reference Mann and GoldmanMann & Goldman, 1982). Since then the predominantly NHS base of CAT has made funding for formal trials difficult to obtain. However, a number of promising results have been published (summarised in Ryle, 1995a), and recent uncontrolled series obtained at the United Medical and Dental Schools of Guy's King's and St Thomas' (UMDS) and at Addenbrookes using both CAT-specific and other measures are encouraging in relation to both borderline personality disorder and more general practice in a psychotherapy department. Any current assessment of the status of the evidential basis for CAT must depend on an evaluation of descriptive studies and uncontrolled series. Supporters of RCT methodologies in psychological treatments tend to be less convinced by uncontrolled studies than those who are more sceptical about the unique value RCT research methodology in psychotherapy. A good description of some of the limitations of RCT methodologies can be found in Bateman & Fonagy (2000).
Training and development
Although there are quite severe complexities in some aspects of CAT theory, practising psychotherapists, especially those with experience in both cognitive and psychodynamic approaches, should find much that is familiar. They may be able to acheive a usable level of competence in CAT by reading the key texts and having some supervision. For those with less experience of psychotherapy, formal training programmes exist. Such formal training is usually necessary for anyone wishing to become a member of the Association of Cognitive Analytic Therapists (ACAT), which exists to promote training in and standards of CAT.
Multiple choice questions
-
1. Procedural sequences:
-
a were developed in an attempt to understand aim-directed action
-
b involve only feeling and acting
-
c contain a check step
-
d are always revised for the better if faulty
-
e if faulty are in the form of snags, traps and dilemmas.
-
-
2. Procedural sequences remain unrevised because:
-
a the check step has been avoided in some way
-
b the alternatives are equally unacceptable
-
c the procedure is never enacted
-
d opportunities for learning new procedures have been too plentiful
-
e caregivers have given injunctions that restrict procedural learning.
-
-
3. In borderline personality disorder:
-
a level-one states are more numerous than in normal behaviour
-
b level-two switching displays a ‘hair-trigger’ response
-
c level-three self-reflection is often weak or absent
-
d level-one and level-two difficulties explain much of the changeability characteristic of the disorder
-
e CAT has no distinctive explanation for the affective features.
-
-
4. In CAT:
-
a treatment usually lasts either 16 or 24 sessions
-
b the therapist gives the patient a reformulation letter at about the fourth session
-
c the therapist avoids mentioning termination
-
d therapist and patient exchange goodbye letters at the end of therapy
-
e follow-up sessions are discouraged.
-
-
5. CAT:
-
a is suitable only for a small range of patient problems
-
b is contraindicated if the patient is actively intoxicated
-
c should never be attempted where motivation is poor or absent
-
d has a small evidence base and urgently needs randomised controlled trials
-
e is administered by an organisation called ACAT.
-
MCQ answers
| 1 | 2 | 3 | 4 | 5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| a | T | a | T | a | F | a | T | a | F |
| b | F | b | T | b | T | b | T | b | T |
| c | T | c | T | c | T | c | F | c | F |
| d | F | d | F | d | T | d | T | d | T |
| e | F | e | T | e | F | e | F | e | T |

Fig. 1 A procedural sequence
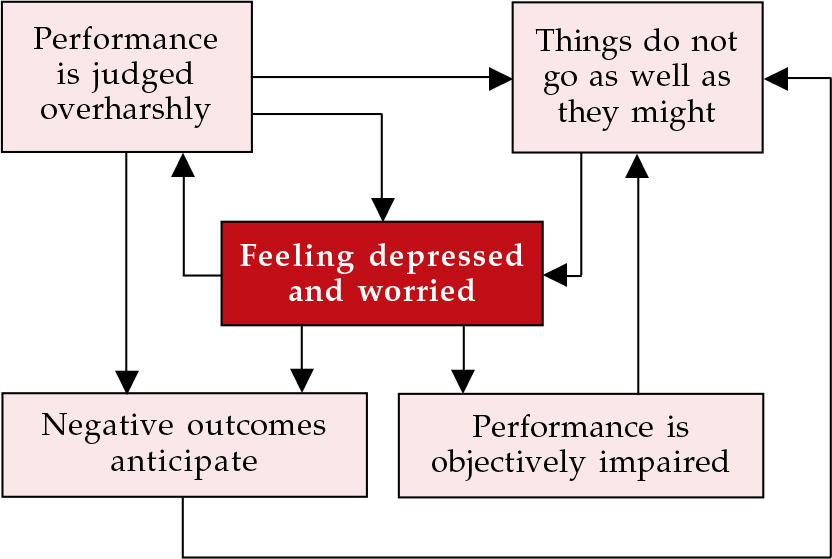
Fig. 2 The depressed-thinking trap
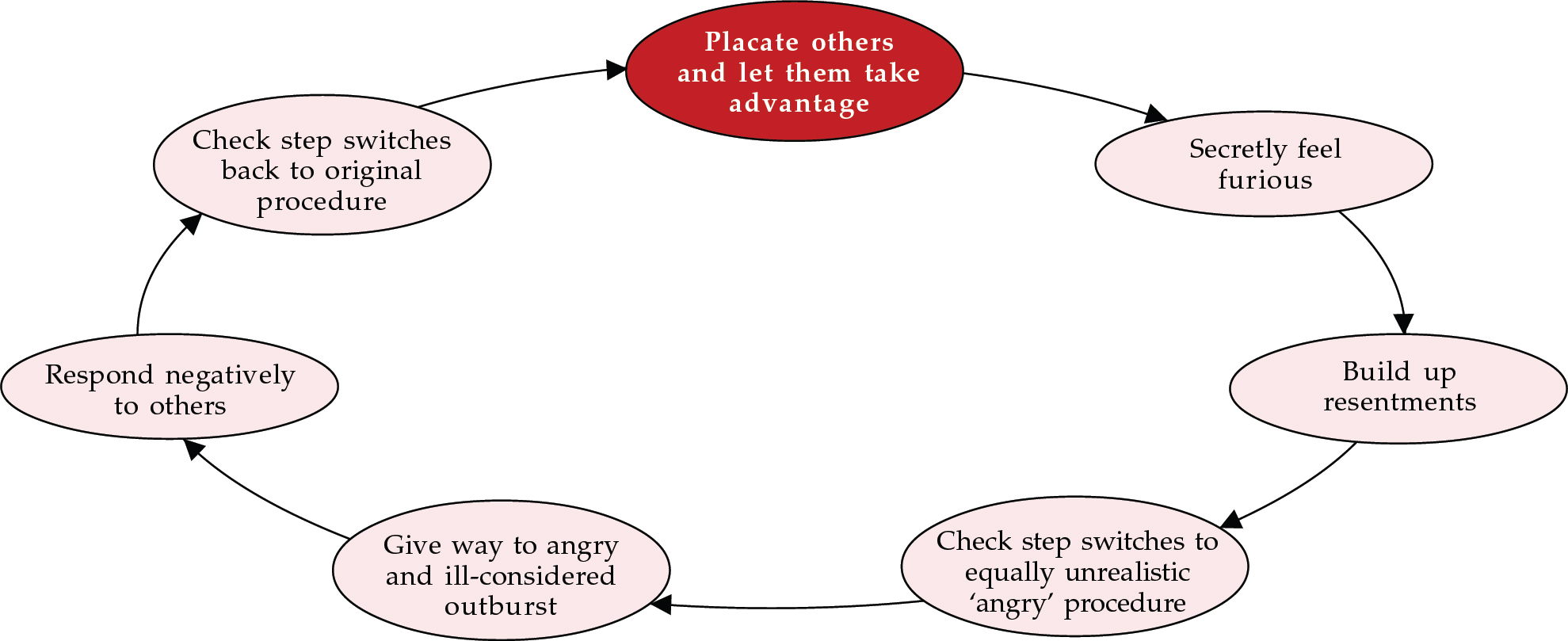
Fig. 3 A dilemma of placation
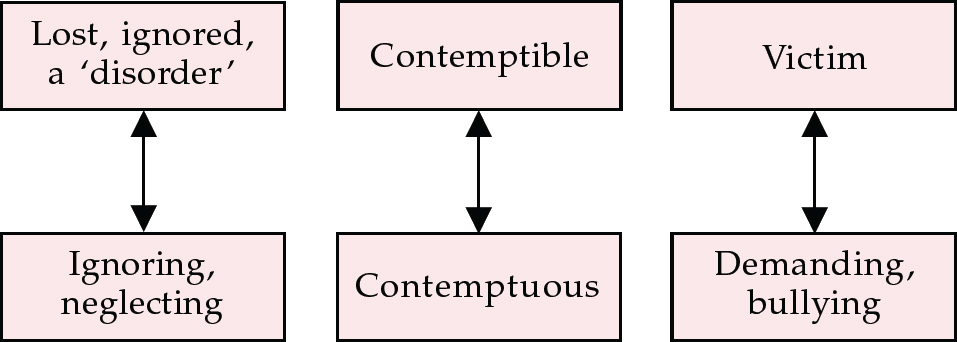
Fig. 4 Fragment of Paul's diagram, showing paired reciprocal roles





eLetters
No eLetters have been published for this article.