


Until well into the 1980s, public health research focused on an individual's lifestyle when attempting to explain his/her state of health(Reference Diez Roux1). However, this individualistic approach to explaining the state of a person's health, which is limited to the micro level, has repeatedly demonstrated its limitations(Reference Mohnen2, Reference Diez Roux and Mair3): although a broad range of biopsychosocial determinants have been taken into consideration in the past, many individual-based risk factor studies have only been partially able to explain health behaviour and health outcomes. It is therefore not surprising that numerous intervention studies which have focused on individuals’ behaviour have not resulted in long-term behavioural changes(Reference Morland, Wing and Diez Roux4).
Pickett and Pearl pointed out in a critical review that this limitation is essentially due to the fact that the individual-based approach does not include factors on an aggregated level, the meso level (especially the geographical context(Reference Pickett and Pearl5)). Taking the meso level into account by considering the influences of the complex social and physical contexts in which individual behavioural decisions are made has proved to be one way of escaping from this cul-de-sac in contemporary research(Reference Cummins and Macintyre6). Recently an increasing number of interdisciplinary research groups have been focusing on investigating to what extent an individual's immediate residential surroundings – his/her social and physical neighbourhood contexts – play a role in determining health behaviour and outcomes(Reference Patterson, Eberly and Ding7). In order to do this, direct and indirect influences of neighbourhood contexts on the behaviour and the health of those individuals living there are identified(Reference Diez Roux and Mair3, Reference van Lenthe8). Examples of such direct effects include immediate exposure to noise and toxic substances. The ‘opportunity structure’(Reference Macintyre, Ellaway and Cummins9) of a residential area – meaning, for example, the availability of medical and other facilities (e.g. doctors, ambulant or clinical care facilities) and the built environment (e.g. play grounds and sports fields) – is an example of a factor which has an indirect effect on the behaviour and health of inhabitants(Reference Mohnen2). A central finding of the research is also that the neighbourhood context accounts for about 10 % of the variation in health outcomes and contributes to the emergence and stabilization of health inequalities(Reference Sellström and Bremberg10).
Tobacco consumption, alcohol consumption and an unhealthy diet rank among the major health risk factors in developed countries(Reference Ezzati, Hoorn and Rodgers11). The local availability of tobacco, alcohol and food is especially relevant and worth assessing in the investigation of place effects on health(Reference van Lenthe and Mackenbach12). In fact, some studies have previously shown a positive correlation between neighbourhood deprivation and the availability of tobacco(Reference Hyland, Travers and Cummings13–Reference Chuang, Cubbin and Ahn18), alcohol(Reference Morland, Wing and Diez Roux4, Reference Duncan, Duncan and Strycker19, Reference Berke, Tanski and Demidenko20) as well as convenience and fast foods(Reference Chuang, Cubbin and Ahn18, Reference Moore, Diez Roux and Nettleton21–Reference Pearce, Blakely and Witten24).
A recent study examined tobacco and alcohol simultaneously and also found a significantly positive correlation with deprivation indicators for both products(Reference Ogneva-Himmelberger, Ross and Burdick25). Pearce et al. found a positive correlation with deprivation indicators in their joint analysis of alcohol and fast-food outlets(Reference Pearce, Day and Witten26). However, in the process of our research we could not find any other study which included and mapped tobacco, alcohol and fast-food outlets simultaneously.
The current study takes this approach and addresses the following question using the example of a German megacity: are socially deprived residential areas more likely than affluent areas to provide access to addictive substances and food which can be detrimental to inhabitants’ health? In the study, we comply with relevant authors’ stipulations regarding both content and methods. These not only call for the consideration of characteristics of the physical environment with regard to such issues, but also for the methodological use of an advanced geographic information system (GIS)(Reference van Lenthe8, Reference Macintyre, Ellaway and Cummins9).
Experimental methods
In the present ecological study(Reference Morgenstern27), the total number of all tobacco, alcohol and fast-food outlets within a predefined investigation area was recorded and visualized using a GIS.
Definition of outcomes and data collection
As the locations of the outlets of interest are not officially registered, all streets and squares within the defined study area were covered during usual opening hours on foot or by bicycle. The inspection was carried out between October and December 2009 by a geographer (J.G.). All retail locations (e.g. supermarkets, shops, kiosks and gas stations) and catering venues (restaurants, bars and other venues) were checked for tobacco, alcohol and fast-food products. We identified classic providers such as service stations, drugstore chains, owner-managed shops and kiosks, as well as exterior (e.g. wall-mounted) cigarette vending machines and those located inside service establishments (e.g. bars, pubs or restaurants) as tobacco outlets. Every shop, kiosk or restaurant with a product range which included alcohol was defined as an alcohol outlet. Only outlets offering warm takeaway food were classified as fast-food outlets (e.g. hamburger, doner kebab, gyros pita, takeaway pizza, French fries, hot dogs). Outlets which also offered seating without service in addition to takeaway items were also classified as fast-food outlets. Full-service restaurants and venues without a takeaway counter – meaning those that predominantly offered table service – were not included.
Method of geocoding
Digitalization and geocoding were carried out using the GIS software ESRI®ArcMap™ (ArcGIS™ 9·3; ESRI, Redlands, CA, USA). As a basis for transferring the mapped evaluation data to GIS, we used digital details taken from the ‘German National Map’ (‘Deutsche Grundkarte’ DGK5, scale 1:5000) as raster data.
Definition of the investigation area
Data were collected in Cologne. Located in the Western part of Germany, Cologne is Germany's fourth largest city, with a population of 1 020 000 inhabitants(Reference Stadt28). Cologne is considered to be a ‘typical German city’ with a historical city centre surrounded by suburbs alongside radial and ring roads. Cologne was chosen for the present study because it is one of the few German cities in which so-called ‘social areas’ have already been delineated by the Statistical Department of Cologne. ‘Social area’ is an established (although still heterogeneously used) geographical term defined generally as conjoined clusters of homogeneous streets and houses within a city which share certain characteristics and attributes(Reference Shevky and Bell29). The complex factor analysis procedure used to define these social areas has been described in detail elsewhere(Reference Heymann30). The city of Cologne contains a total of 269 of these social areas.
A visual inspection of the entire city of Cologne would have taken over a year. For our study, eighteen social areas in four districts of Cologne (from west to east: two out of two social areas of Cologne-Junkersdorf, six out of six social areas of Cologne-Lindenthal, eight out of eight social areas of Cologne-Muelheim and two out of two social areas of Cologne-Neubrueck) were chosen. We selected these four districts after having taken into consideration their comparable distance from the city centre as well as their geographical structure: two of these districts are located 7 km away from the city centre (Cologne-Junkersdorf, Cologne-Neubrueck), while the other two districts are in close proximity to the historical city centre (2 km; Cologne-Lindenthal, Cologne-Muelheim). Furthermore, two of these districts (Cologne-Junkersdorf, Cologne-Lindenthal) are located to the west and two (Cologne-Muelheim and Cologne-Neubrueck) to the east of the Rhine River, which runs through the city. Additionally, a representative reflection of Cologne's segregation structures was sought. In short, Cologne-Junkersdorf and Cologne-Neubrueck are typical suburban areas with mixed geographical development and heterogeneous population structures. Around 10 000 inhabitants live in these two districts. In contrast, the districts of Cologne-Lindenthal and Cologne-Muelheim both exhibit an urban structure typical of city centre outskirts and are home to 30 000 and 40 000 inhabitants, respectively.
Definition of status indicators
Income is considered to be a suitable and widely used indicator of objective deprivation(Reference Townsend31). As is usually the case in Germany, no epidemiological data regarding the income of the 91 634 inhabitants of the social areas were available due to privacy protection laws. However, for each social area we were able to obtain information regarding the percentage of parents who were exempt from paying kindergarten or full-time school fees for their children. The threshold for exemption from paying such fees is set at a joint annual taxable income of €12 272. At the time of submission of the present paper, this corresponded to $US 16 013. The Department for Children, Youth and Family/Youth Assistance Planning responsible for the City of Cologne emphasizes that ‘it is possible to reach representative conclusions regarding the income situation in social areas by assessing data concerning parents paying [such] fees’(Reference Stadt32). Because the income of parents within one district in Germany is therefore likely to correlate strongly with the income of the other inhabitants, we used that income indicator for the entire district. Two measures of income were calculated for each district: (i) the percentage of parents with a joint annual taxable income of <€12 272, which was used for a correlation analysis; and (ii) whether the district percentage of low-income parents was greater or less than 32 % (the mean for the 269 social areas of Cologne), which was used in a comparison of low- and high-income areas. To back up the findings, we took three additional indicators of objective social deprivation into consideration. We had access to data from 2007 regarding youth unemployment rates, the proportion of the population receiving social welfare and the percentage of pupils attending low-qualifying schools in each social area.
Statistical methods
In the first part of the analysis we examined how accessible the outlets were to the residents. First, all residential buildings within the eighteen social areas were localized (n buildings 11 339). For this purpose the Base DLM (Digital Landscape Model 1:25 000, created by the German Federal Agency for Cartography and Geodesy) was used. In the next step the resident population was evenly distributed among the buildings identified within each social area. A separate calculation was necessary because the building structure within the social areas was homogeneous, but varied among the different social areas. As a result, the Euclidean distances from each residential building to the nearest outlet were calculated. To proceed in the most realistic manner, outlets from the neighbouring social areas were also taken into consideration. The accessibility of the outlets investigated consequently equates to the average and weighted Euclidean distance between residential building and outlet.
In the second part of the analysis we examined associations and correlations between deprivation indicators and the number of outlets in social areas. In order to present the outlet density in comparable units for all social areas, the number of identified points of sale was also set in relation to the corresponding number of inhabitants in accordance with usual standards(Reference Duncan, Duncan and Strycker19). Within bivariate analyses (t tests for association analyses and Kendall's tau β (τ β) for correlation analyses), the data were normally distributed according to the Kolmogorov–Smirnov test. Due to very few outlets in the districts of Neubrueck and Muehlheim, we used Kendall's τ β correlation analysis to examine the relationship between deprivation indicators and the number of outlets in social areas. Kendall's τ β correlation coefficients are based on ranks of observations and therefore less vulnerable to outliers than other correlation coefficients(Reference Sommer and Sommer33).
Next, we used Moran's I statistic to test for spatial autocorrelation between the number of tobacco, alcohol and fast-food outlets (which occurs when nearby spatial units are related to each other(Reference Anselin and Rey34)). A recent study showed systematic patterns in the spatial distribution of tobacco outlets in 1938 census tracts in the state of New Jersey (USA) that violated the assumption of independence of each observation and caused overestimated coefficients and standard errors(Reference Yu, Peterson and Sheffer17). Our study was limited to eighteen social areas within four districts of Cologne, and Moran's I statistic indicated no significant spatial autocorrelation. Furthermore, we employed multilevel modelling to test whether the P values and the correlation coefficients might be inflated by the hierarchical data structure. We did not find any variance on the district level and assume that our results are not biased by the clustering of the social areas within districts.
In all cases, we used two-sided tests with P < 0·05 to indicate statistical significance. All analyses were done using the statistical software package SPSS-PASW Statistics for Windows, version 18·0 (SPSS Inc.), except for the calculation of Moran's I test statistic, which was conducted using GeoDa095-i(Reference Anselin, Syabri and Kho35).
Results
In the entire investigation area, 339 tobacco, 353 alcohol and sixty-seven fast-food outlets were identified, which represents approximately one point of sale per 270, 260 and 1368 inhabitants, respectively. Most tobacco points of sale were cigarette vending machines: forty-eight of them were outdoor and 138 of them were indoor vending machines. Additional tobacco sources included kiosks (n 85), supermarkets (n 25), petrol stations (n 13), drugstores (n 10), tobacco shops (n 8) and grocery stores (n 12). The spatial distribution of the commercial tobacco sources is shown in the GIS-based map (Fig. 1). It illustrates the almost ubiquitous availability of cigarettes in all areas, with the highest densities along arterial roads and district centres. Any arbitrarily chosen residential building inside the investigation area was situated within a few hundred metres of a commercial tobacco source, at most (range: 0–568 m, mean: 135 m, median: 111 m, n buildings 11 339).
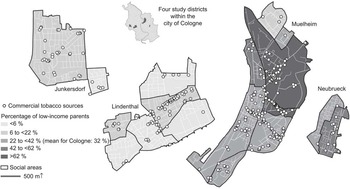
Fig. 1 True to scale, cartographic depiction of all tobacco outlets in eighteen social areas of the city of Cologne, Germany, autumn 2009
The density of outlets offering alcoholic beverages was found to be even higher (Fig. 2). More than half of the alcohol outlets identified were located inside catering venues, namely in restaurants, bars and pubs (n 194). Kiosks (n 83) and petrol stations (n 13) represented approximately a quarter of all alcohol outlets (n 353) identified. Approximately every ninth outlet identified (n 41) was a large grocery store/supermarket (n 30) or drugstore (n 11) and about 7 % were specialty stores such as wine and spirit shops, delicatessens, etc.

Fig. 2 True to scale, cartographic depiction of all alcohol outlets in eighteen social areas of the city of Cologne, Germany, autumn 2009
The Euclidean distances between the residential buildings and the nearest outlet amounted on average to between 82 and 151 m for tobacco (Fig. 1) and 92 and 175 m for alcohol, depending on the district (Fig. 2). In comparison, fast-food points of sale were found to be further away from residential buildings (194–782 m, Fig. 3). Twenty-two out of a total of sixty-seven points of sale were solely takeaway outlets. The remaining outlets also offered the possibility to eat while standing or sitting (e.g. food chains/catering industry).

Fig. 3 True to scale, cartographic depiction of all fast-food outlets in eighteen social areas of the city of Cologne, Germany, autumn 2009
Next we examined the association between neighbourhood deprivation and local supply. We compared all social areas of above-average income with all those of below-average income with respect to the density of points of sale. With 4·70 tobacco sources per 1000 inhabitants, we found significantly more commercial cigarette sources in the disadvantaged districts than in the affluent districts, where the density was 2·67 per 1000 inhabitants (t = −2·22; P = 0·041). Differences were also seen regarding alcohol and fast food: the number of outlets in the disadvantaged districts was 4·70 and 1·19 per 1000 inhabitants, respectively. In the more affluent districts, the number of commercial sources per 1000 inhabitants was 2·98 for alcohol (t = −1·58; P = 0·134) and 0·27 for fast food (t = −2·44; P = 0·042).
Neighbourhood deprivation showed a clear association with the average distance to the nearest outlet: whereas the residential population in the ten more affluent areas had an average Euclidean distance of 151 m (tobacco), 166 m (alcohol), 511 m (fast food) to the next point of sale, these distances amounted to 85 m (tobacco), 99 m (alcohol), 177 m (fast food) in the eight disadvantaged districts. Legal drugs and fast food were significantly (P < 0·05) more accessible to the residents of socially disadvantaged districts.
In more detailed analyses, significant correlations between the income indicator and outlet density were also found for all three categories of product which can be detrimental to inhabitants’ health: the lower the income in a district, the higher the availability of cigarettes, alcohol and fast food (Figs 4–6). This correlation was strongest for fast food (τ β = 0·473; P = 0·009), followed by tobacco products (τ β = 0·433; P = 0·012) and alcohol (τ β = 0·341, P = 0·049).

Fig. 4 Scatter plot for the correlation between an income indicator and tobacco outlet density in eighteen social areas of the city of Cologne, Germany, autumn 2009. τ β = 0·433, P = 0·012; C = mean for city of Cologne;  $$$$
, social areas with under-average income indicator;
$$$$
, social areas with under-average income indicator;  $$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)
$$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)

Fig. 5 Scatter plot for the correlation between an income indicator and alcohol outlet density in eighteen social areas of the city of Cologne, Germany, autumn 2009. τ β = 0·341, P = 0·049; C = mean for city of Cologne;  $$$$
, social areas with under-average income indicator;
$$$$
, social areas with under-average income indicator;  $$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)
$$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)

Fig. 6 Scatter plot for the correlation between an income indicator and fast-food outlet density in eighteen social areas of the city of Cologne, Germany, autumn 2009. τ β = 0·473, P = 0·009; C = mean for city of Cologne;  $$$$
, social areas with under-average income indicator;
$$$$
, social areas with under-average income indicator;  $$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)
$$$$
, social areas with above-average income indicator; income indicator = parents with a joint annual taxable income <€12 272 within the social area/all parents within the social area (in %)
Correlation coefficients for the three alternative indicators of youth unemployment (τ β(tobacco) = 0·322; τ β(alcohol) = 0·257; τ β(fast food) = 0·496), the percentage of people receiving social welfare (τ β(tobacco) = 0·289; τ β(alcohol) = 0·184; τ β(fast food) = 0·409) and the percentage of pupils attending low-qualifying schools (τ β(tobacco) = 0·268; τ β(alcohol) = 0·229; τ β(fast food) = 0·450) indicated a similar tendency, but were significant only in the case of fast food (0·006<P < 0·023).
Discussion
Principal findings and contribution to the current state of research
In residential areas with low income and high deprivation levels, the availability of unhealthy products was significantly higher than in more affluent areas. The density of outlets which provide alcohol and tobacco, as well as those offering unhealthy food, correlated significantly with the social structure of a specific residential area. Thus, the physical environment, specifically discrepancies in the availability of fast food and addictive substances, can have a contextual influence on the health of an individual and can, in the form of physical exposure, contribute to a further culmination of health risks.
Based on the term ‘obesogenic environments’(Reference Pearce, Day and Witten26, Reference Lake, Townshend and Alvanides36), we suggest that there are also ‘addictive environments’ which cluster in socially disadvantaged neighbourhoods. This is consistent with relevant literature which we summarized in the paper's introduction. (By contrast, the literature on the relationship between neighbourhood deprivation and the accessibility of healthy food (like fruit and vegetables) is inconsistent(Reference Morland, Wing and Diez Roux4, Reference Larson, Story and Nelson23, Reference Pearce, Day and Witten26, Reference Cummins, Smith and Taylor37).) That such a higher exposure is in fact correlated with a higher demand is confirmed by several studies on tobacco and alcohol(Reference Chuang, Cubbin and Ahn18, Reference Asumda and Jordan38, Reference Gibbons, Gerrard and Vande Lune39). Several authors report spatial aggregation structures in the form of so-called ‘smoking islands’(Reference Thompson, Pearce and Barnett40). According to three current reviews, the majority(Reference Larson, Story and Nelson23, Reference Jago, Baranowski and Baranowski41, Reference Holsten42) but not all(Reference Pearce, Hiscock and Blakely43, Reference Pearce, Hiscock and Blakely44) of the studies also identified a significant association between a healthy community food environment and limited access to fast-food restaurants, on the one hand, and healthy diets and lower obesity rates on the other hand.
Consequently, our results support the thesis of ‘deprivation amplification’(Reference Dunn, Frohlich and Ross45). The effects of higher availability of fast-food and legal drug outlets is further amplified because disadvantaged groups are less likely to own a car and are therefore less mobile, making them less able to obtain alternative, healthy products (e.g. organic food, fresh fruits and vegetables)(Reference Morland, Wing and Diez Roux4). It is possible that these phenomena on the meso level could help to partially explain the widening gap in social and health inequalities(Reference Moore and Diez Roux22, Reference Pearce, Day and Witten26, Reference Barnett, Pearce and Moon46). In our conclusion we take up suggestions recently made by the WHO and other research groups as to how such a deprivation amplification could be countered on the meso level(Reference Chuang, Cubbin and Ahn18, Reference Ogneva-Himmelberger, Ross and Burdick25, Reference Ashe, Jernigan and Kline47–49).
Limitations and strengths
Methodical limitations of the present study mainly concern the selection of the study area, the clustering of social areas and the inability to assess causality. Strengths of the study include the simultaneous consideration of the availability of tobacco, alcohol and fast-food products, the use of innovative GIS methods to visualize the number and distribution of outlets, and the comprehensive and valid data collection process which included every outlet in an extensive geographic investigation area.
Selectivity of the area of investigation
Although we have termed Cologne a ‘typical German city’, it cannot be considered to be representative of all German cities. Nevertheless, the proportion of persons aged 0–25 years amounted to 24·3 % (compared with the Germany-wide average of 25·8 %) and the unemployment rate was 13·1 % (compared with the Germany-wide average of 11·7 %), and therefore the city can be said to be typical of the nationwide urban situation.
Clustering of social areas
We used a stratified sample design to identify eighteen social areas clustered within four different districts. In this way we were able to economize field time and field costs. We intentionally incorporated districts with different social and geographical structures into the study, which provided a key basis for comparison. However, this design can produce spatial autocorrelation because social areas within the same district are likely to have similar numbers of outlets and a similar social structure(Reference Morland, Wing and Diez Roux4, Reference Hyland, Travers and Cummings13). If spatial autocorrelation occurs and spatial units in close proximity are related to each other, the assumption of independence in classical statistical models is violated and the type I error is inflated(Reference Ward and Gleditsch50). We therefore carefully checked the dependent variables by social area for spatial autocorrelation using Moran's I test statistic and did not observe any significant spatial clustering. Furthermore, we used multilevel modelling to test whether the reported coefficients and P values were biased by the hierarchical data structure and socio-economic differences between the four districts. We did not find any variance on the district level (results not shown) and therefore applied classic statistical non-parametric models.
Inability to assess causality
An ecological study such as this one can naturally not come to conclusions regarding the causal direction of the correlations observed(Reference Schulz and Northridge48). First, it is possible that investors follow demand and open and run their stores in areas where they expect the highest buyer density (‘supply follows demand’(Reference Morland, Wing and Diez Roux4)). Correspondingly, over-proportionally high tobacco advertisement density has been observed in socially deprived areas(Reference Laws, Whitman and Bowser14, Reference Feighery, Schleicher and Boley Cruz51, Reference Meyer and Schneider52). Second, it is possible that tenants and home owners move to areas where they have access to their preferred products (according to their preference, either healthy or unhealthy products; ‘demand follows supply’(Reference Chuang, Cubbin and Ahn18)). Both explanatory directions are concordant with economic theory, which posits that the net price faced by consumers is a function of search costs. Search costs include time necessary and distance travelled by individuals to the point of sale. Thus, the higher the outlet density, the lower the subjective costs(Reference Schneider, Reid and Peterson53). As individuals with a lower social status are particularly price sensitive, lowering access costs (e.g. reduced travelling time) is likely to increase their consumption(Reference Schneider, Reid and Peterson53). Suppliers (the tobacco, alcohol and fast-food industries, as well as vending machine distributors) are just as likely to take these points into consideration when planning the location of their outlets as consumers are when deciding where they want to live. However, the cause of this pivotal correlation is not as important for the public health message of our study as the resulting consequences regarding neighbourhood environment and health. In addition to the supply of unhealthy foods, future studies on neighbourhood context and health should simultaneously take the supply of healthy foods (e.g. fresh fruit and vegetables) into account.
To our knowledge the present study is the first to map tobacco, alcohol and fast-food outlets simultaneously using a GIS, which provides information not only about the number, but also about the spatial distribution and density of sources. The comparatively extensive area of investigation and the topicality, thoroughness and validity of the data collection are further strengths of this study. In this way we have fulfilled the stipulations of several authors who had previously questioned the validity of the data (such as selected outlets, register data or participant reports(Reference Chuang, Cubbin and Ahn18, Reference Moore, Diez Roux and Nettleton21, Reference Schneider, Reid and Peterson53–Reference Pearce, Hiscock and Moon55)) and criticized the lack of cartographic GIS mapping in similar studies(Reference Duncan, Duncan and Strycker19).
Conclusions
Our study demonstrates the link between social and physical contextual factors on the meso level. It can be said that those individuals who are already socially disadvantaged experience a further contextual disadvantage due to their place of residence.
Possible intervention measures to prevent deprivation amplification on the meso level can be initiated on the supply side or on the demand side. On the supply side, the WHO and the aforementioned research groups recommend – among other things – legal age barriers, licensing laws and restrictions on advertising and on local outlet density. In our opinion this should also include the strict prohibition of publicly accessible cigarette vending machines. In Germany, Austria, Italy and Japan such machines are freely accessible on the walls of buildings and in front of tobacconists. In Germany the high-risk group, which includes children and adolescents, is supposed to be protected via non-regulative (and barely effective) commitments made by the cigarette industry and vending machine operators according to which they are not allowed to install poster advertising (within 100 m) or cigarette vending machines (within 50 m) within a certain distance of schools or youth facilities. Local disparities in the supply of alternative foods could be balanced, at least to a small degree, by enabling higher permeability between neighbourhoods. This could be done, for example, by improving the public transportation system or the network of cycling paths and sidewalks. An adequate settlement policy (retail mix, health-promoting urban planning of new residential areas and industrial settlements) could counteract negative social differentiation due, for example, to the non-regulated gentrification, segregation or deprivation of whole neighbourhoods. In Germany, for example, each municipal district is responsible for its own retail planning. This type of retail planning employs very detailed product lists to ensure that all residents (also those who are not mobile) have access to a wide range of products. It would therefore be very possible to take health-related issues into consideration in such retail planning processes, allowing targeted intervention on the supply side.
On the demand side, besides better communication about health risks and public health empowerment, promoting diverse shopping facilities (e.g. organic markets) and therapy options in socially disadvantaged areas (e.g. local advertising), the prevention of the onset and the promotion of cessation of tobacco, alcohol or fast-food consumption are central intervention strategies on the meso level. Lifestyle-specific prevention campaigns in schools, youth and old-age facilities, poster campaigns as well as outreach work should be offered, especially in socially disadvantaged districts. Additionally, incentive and support systems (bonification, deductions, quit lines and help lines) could motivate decision makers and disseminators (physicians, pharmacies and teachers) in critical social neighbourhoods to offer tobacco and alcohol cessation courses and to provide nutrition counselling. Furthermore, all of these measures should consider the specific social structure (including migrants) of the respective districts through multilingual and a low-threshold implementation.
Acknowledgements
Source of funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. According to German law an ethical approval was not required as no personal data were used. Conflicts of interest: The authors had no conflict of interest. Authors’ contribution: S.S. was the principal investigator. J.G. conducted the field work of the study, including geocoding. Both authors prepared data management, statistical analyses and figures and wrote the manuscript. Acknowledgements: Without the wealth of statistical information provided by the personnel of the Office for Youth Support in the Department of Youth, Children and Family Welfare, namely Mr Heymann, Mrs Langenbach and Mr Gringmuth-Held, this study would not have been possible. Moreover, the authors would like to thank Professor Thomas Kistemann (Institute for Hygiene and Public Health, University of Bonn) for methodological ideas; Shelby Yamamoto, PhD, and Silke Roehrig, BA, for their helpful comments and support in the preparation of the manuscript; as well as Christian Weidmann, MA, for his statistical programming support.






