


Children placed in foster or adoptive families often have had adverse experiences (e.g., abuse and/or neglect) before their placement. Even though these experiences may differ from child to child, what these children have in common is a separation from their biological parents (Van den Dries, Juffer, van IJzendoorn, & Bakermans-Kranenburg, Reference Van den Dries, Juffer, van IJzendoorn and Bakermans-Kranenburg2009). Foster or adoptive placements generally signify an improvement, in which children are usually moved from unfavorable caregiving circumstances to nurturing families. Children's adverse experiences can, however, result in difficulties with trusting new adults, which in turn may contribute to difficulties in forming a secure attachment relationship with the (new) parent and to the development or persistence of behavior problems. Taking care of foster or adopted children is therefore frequently a demanding and difficult task. While foster care and adoptive placements can be considered as interventions themselves (Nelson, Fox, & Zeanah, Reference Nelson, Fox and Zeanah2014; van IJzendoorn & Juffer, Reference van IJzendoorn and Juffer2006), several intervention programs have been developed to help and support foster and adoptive parents and children to form a secure attachment relationship and to help these parents deal with child behavior problems and parenting challenges after placement. Parenting interventions may eventually decrease or even prevent the risk of developmental problems as a result of adverse early life experiences and increase resilience of foster and adopted children. The current meta-analysis is the first to examine the combined effect of these intervention programs in both foster and adoptive families. The focus is on parenting constructs (sensitivity, discipline, knowledge and attitudes, and parenting stress) that have been associated with child outcomes such as attachment security, problem behavior, and stress regulation. In addition, we tested effects on placement disruptions.
Developmental Challenges of Foster and Adopted Children
Adverse early life experiences may influence children's development and result in behavioral and emotional problems. One important underlying mechanism is the formation of attachment relationships. Children can use different behavioral strategies in response to the parent or caregiver (attachment figures) in stressful situations, and these strategies are an indication of the quality of the attachment relationship. Children with a secure attachment relationship seek contact with and comfort from their attachment figure when they are upset. There are different patterns that are considered as an insecure attachment: children who show avoidant attachment behaviors in times of need do not seek contact and comfort from their attachment figures, whereas children who show resistant attachment behaviors do seek contact and comfort from their attachment figure, but they stay upset because they cannot regulate their emotions properly (Ainsworth, Blehar, Waters, & Wall, Reference Ainsworth, Blehar, Waters and Wall1978). When children show a temporary breakdown of secure or insecure attachment behavior strategies, they are classified as insecurely disorganized attached, which is often seen as the most insecure attachment classification (Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990). An insecure and/or disorganized attachment relationship increases the risk of developing behavior problems and psychopathology later in life (Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley, & Roisman, Reference Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley and Roisman2010; Groh, Roisman, van IJzendoorn, Bakermans-Kranenburg, & Fearon, Reference Groh, Roisman, van IJzendoorn, Bakermans-Kranenburg and Fearon2012; Sroufe, Egeland, Carlson, & Collins, Reference Sroufe, Egeland, Carlson, Collins, Grossman, Grossman and Waters2005; van IJzendoorn, Schuengel, & Bakermans-Kranenburg, Reference van IJzendoorn, Schuengel and Bakermans-Kranenburg1999), whereas a secure attachment relationship promotes a more optimal social development, as well as adaptability and resilience in children (Groh et al., Reference Groh, Fearon, Bakermans-Kranenburg, van IJzendoorn, Steele and Roisman2014; Sroufe et al., Reference Sroufe, Egeland, Carlson, Collins, Grossman, Grossman and Waters2005). Meta-analytic results show that foster and adopted children are more likely to develop an insecure disorganized attachment relationship with their new parents than children living with and being raised by their biological parents (Van den Dries et al., Reference Van den Dries, Juffer, van IJzendoorn and Bakermans-Kranenburg2009; Vasileva & Petermann, Reference Vasileva and Petermann2018), and they are more likely to develop emotional and behavioral problems (Juffer & van IJzendoorn, Reference Juffer and van IJzendoorn2005).
Early adverse experiences and behavior problems of foster and adopted children additionally increase the risk of disruptions in foster care and adoption (Coakley & Berrick, Reference Coakley and Berrick2008; McDonald, Propp, & Murphy, Reference McDonald, Propp and Murphy2001; Oosterman, Schuengel, Slot, Bullens, & Doreleijers, Reference Oosterman, Schuengel, Slot, Bullens and Doreleijers2007), and the more previous placements and/or transitions, the higher the risk for children to develop emotional and behavioral problems later in life (Newton, Litrownik, & Landsverk, Reference Newton, Litrownik and Landsverk2000). Prevention of placement disruption is important to prevent children from having to experience another separation of an attachment figure.
Finally, adverse experiences early in life are often stressful for children. Low quality of care and separations from attachment figures can result in chronic stress in children, and this early life stress may result in dysregulation of the hypothalamic–pituitary–adrenocortical (HPA) axis (Bunea, Szentágotai-Tătar, & Miu, Reference Bunea, Szentágotai-Tătar and Miu2017; Koss & Gunnar, Reference Koss and Gunnar2018). The cortisol production (the end product of the HPA axis) of foster and adopted children seems to show an atypical, more blunted pattern during the day than that of non-foster and non-adopted children indicating that their stress-response system is atypically activated during the day (Bernard, Butzin-Dozier, Rittenhouse, & Dozier, Reference Bernard, Butzin-Dozier, Rittenhouse and Dozier2010; Bunea et al., Reference Bunea, Szentágotai-Tătar and Miu2017; Koss & Gunnar, Reference Koss and Gunnar2018). Previous research has additionally shown that dysregulation of the HPA axis is related to internalizing (e.g., depression, anxiety, or posttraumatic stress disorder) or externalizing behavior problems (e.g., conduct problems, aggression, or rule breaking) later in life (Alink et al., Reference Alink, van IJzendoorn, Bakermans-Kranenburg, Mesman, Juffer and Koot2008; Koss & Gunnar, Reference Koss and Gunnar2018). Dysregulation of the HPA axis and the probable behavioral consequences may thus also increase the risk of placement disruption in foster and adopted children.
Intervention Programs for Foster and Adoptive Parents
Foster and adoptive parents often experience challenges with and have concerns about their children's attachment security, behavior problems, and (previously or currently) experienced stress. They often experience elevated levels of stress, because the placement, the caregiving of, and the interacting with children who (due to their adverse experiences) show behavior problems can be stressful (Goemans, Van Geel, & Vedder, Reference Goemans, Van Geel and Vedder2018). Such elevated stress levels can inhibit parents’ sensitive (disciplining) behavior while interacting with the child (Feldman, Weller, Zagoory-Sharon, & Levine, Reference Feldman, Weller, Zagoory-Sharon and Levine2007). It is thus important that parenting interventions aim to reduce parenting stress in foster and adoptive parents. In addition, intervention studies have shown that children's attachment security can be improved with intervention programs focusing on increasing parental sensitivity of parents in general (Bakermans-Kranenburg, van IJzendoorn, & Juffer, Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003). Research also shows that children with early life stress and a dysregulated HPA axis benefit from intervention programs that increase parental sensitivity (Bernard, Hostinar, & Dozier, Reference Bernard, Hostinar and Dozier2015; Fisher, Gunnar, Dozier, Bruce, & Pears, Reference Fisher, Gunnar, Dozier, Bruce and Pears2006; Fisher, Stoolmiller, Gunnar, & Burraston, Reference Fisher, Stoolmiller, Gunnar and Burraston2007). However, sensitive parenting alone may not suffice to decrease the often tenacious behavior problems of foster and adoptive children. Consistent parental disciplining and positive reinforcement of desired child behavior may additionally be necessary to reduce child behavior problems (Patterson, Reference Patterson1982). Dysfunctional disciplining strategies can be reduced with parenting interventions (Ciff, Rus, Butterfield, & Parris, Reference Ciff, Rus, Butterfield and Parris2015; N'zi, Stevens, & Eyberg, Reference N'zi, Stevens and Eyberg2016; Van Zeijl et al., Reference Van Zeijl, Mesman, van IJzendoorn, Bakermans-Kranenburg, Juffer, Stolk and Alink2006). In addition, for foster and adoptive parents, it may be relevant to understand where the children's problems regarding (attachment) behavior and stress regulation come from. A previous systematic review shows that effective intervention programs that aim to improve the parent–child relationship and to reduce children's behavior problems include a psychoeducational component that teaches foster parents about the impact of the adverse early life experiences on the children's developmental problems regarding (attachment) behavior and stress regulation (Kemmis-Riggs, Dickes, & McAloon, Reference Kemmis-Riggs, Dickes and McAloon2018). A qualitative study among adoptive parents also recommends that intervention programs should educate adoptive parents about the relation between preplacement adverse experiences and attachment security, and how they can sensitively respond to the children's needs (Dunkelberg, Reference Dunkelberg2008).
Several intervention programs have been developed for foster and adoptive parents. Sensitive parenting, dysfunctional disciplining, and parenting stress of foster and adoptive parents can, for example, be improved respectively reduced with the Parent–Child Interaction Therapy (PCIT; Mersky, Topitzes, Janezewski, & McNeil, Reference Mersky, Topitzes, Janczewski and McNeil2015) or the Child Parent Relationship Therapy (Opiola, Reference Opiola2016), respectively. Promoting First Relationships (Spieker, Oxford, Kelly, Nelson, & Fleming, Reference Spieker, Oxford, Kelly, Nelson and Fleming2012) is an example of a parenting intervention that can increase foster parents’ knowledge about the children's problems with (attachment) behavior and stress regulation.
Previous Meta-Analytic Studies
Two meta-analyses examining the effectiveness of foster care intervention programs have previously been conducted. In the first meta-analysis Van Andel, Grietens, Strijker, Van der Gaag, and Knorth (Reference Van Andel, Grietens, Strijker, Van der Gaag and Knorth2012) included intervention programs that may be helpful for foster parents and children to cope with problem behavior and stress, but that were not necessarily tested in a foster care sample. Their literature search resulted in 19 studies, and results showed significant medium combined effect sizes for improved parenting skills and decreased behavior problems. However, most of the studies included in this meta-analysis did not report results specifically for foster parents or children (i.e., Becker-Weidman & Hughes, Reference Becker-Weidman and Hughes2008; Evans et al., Reference Evans, Boothroyd, Armstrong, Greenbaum, Brown and Kuppinger2003; Henggeler et al., Reference Henggeler, Rowland, Randall, Ward, Pickrel, Cunningham and Santos1999; Marvin, Cooper, Hoffman, & Powell, Reference Marvin, Cooper, Hoffman and Powell2002; Mesman et al., Reference Mesman, Stolk, Van Zeijl, Alink, Juffer, Bakermans-Kranenburg, Koot, Juffer, Bakermans-Kranenburg and van IJzendoorn2008; Moretti & Obsuth, Reference Moretti and Obsuth2009; Nabors, Proescher, & DeSilva, Reference Nabors, Proescher and DeSilva2001; Ogden & Hagen, Reference Ogden and Hagen2008; Webster-Stratton, Reference Webster-Stratton1998; Webster-Stratton & Reid, Reference Webster-Stratton and Reid2003). Other studies did not examine the effectiveness of parenting interventions (i.e., Clark & Prange, Reference Clark and Prange1994; Myeroff, Mertlich, & Gross, Reference Myeroff, Mertlich and Gross1999) or used foster care (or a comparable kind of care) as an intervention itself (i.e., Chamberlain, Leve, & DeGarmo, Reference Chamberlain, Leve and DeGarmo2007; Cowen & Reed, Reference Cowen and Reed2002; Whitemore, Ford, & Sack, Reference Whitemore, Ford and Sack2003). Finally, 3 studies did not include a (randomized) control group to test the effectiveness of the intervention programs (i.e., Marvin et al., Reference Marvin, Cooper, Hoffman and Powell2002; Nabors et al., Reference Nabors, Proescher and DeSilva2001; Whitemore et al., Reference Whitemore, Ford and Sack2003), which makes it difficult to draw conclusions based on the results.
In the second meta-analysis, Solomon, Niec, and Schoonover (Reference Solomon, Niec and Schoonover2017) examined the effectiveness of intervention programs aimed at improving foster parents’ parenting skills, behavior, and knowledge and at reducing child behavior problems. The small to medium combined effect size based on 16 studies showed that the intervention programs effectively improved parenting skills and knowledge, and reduced child behavior problems, compared to a (randomized) control group. Because of the specific aim of this meta-analysis, effectiveness studies of intervention programs with another outcome than parenting skills, knowledge, and/or child problem behavior were excluded (e.g., parenting stress and child attachment security). Studies including kinship foster care were also excluded, resulting in a selection of available foster care intervention studies. Examples of intervention programs that were excluded due to these inclusion and exclusion criteria are Fostering Attachments (Wassall, Reference Wassall2011), Multidimensional Treatment Foster Care for Preschoolers (Fisher & Kim, Reference Fisher and Kim2007; Fisher & Stoolmiller, Reference Fisher and Stoolmiller2008), and Promoting First Relationships (Spieker et al., Reference Spieker, Oxford, Kelly, Nelson and Fleming2012).
To our knowledge, no meta-analyses regarding parenting interventions for adoptive families have been conducted. However, a systematic review by Drozd, Bergsund, Hammerstrom, Hansen, and Jacobsen (Reference Drozd, Bergsund, Hammerstrom, Hansen and Jacobsen2018) included 21 studies with a pre-/posttest design with at least one control group that examined parent outcomes in adoptive families. Some studies found improvements of interpersonal functioning and parenting, but the majority did not. Finally, a meta-analysis examining the effectiveness of interventions to prevent disorganized attachment did find that interventions focusing on increasing parental sensitivity resulted in a small but significant decrease of the prevalence of disorganized attachment and more so in children at risk, for example, adopted children (Bakermans-Kranenburg, van IJzendoorn, & Juffer, Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2005).
According to Dickes, Kemmis-Riggs, and McAloon (Reference Dickes, Kemmis-Riggs and McAloon2018), methodological differences between individual intervention programs and/or individual studies make it difficult to draw definite conclusions from the results of meta-analyses. Effectiveness studies of intervention programs depend on the internal validity within a study (e.g., program fidelity) but also the external validity in terms of generalizability to the foster care population (Dickes et al., Reference Dickes, Kemmis-Riggs and McAloon2018). Dickes et al. (Reference Dickes, Kemmis-Riggs and McAloon2018) systematically reviewed the quality of methods regarding participant (e.g., kinship vs. non-kinship, mean age, and placement history), intervention (e.g., setting, format, and aims), and outcome (i.e., measurement instruments) characteristics of 17 intervention studies, and results showed that due to heterogeneity within these methodological characteristics, it remains difficult to compare individual studies and calculate an overall effect size. It is therefore important to take possible moderators into account when conducting a meta-analysis to control for this heterogeneity.
Current Study
In the current study a series of eight meta-analyses have been performed to examine the effectiveness of parenting interventions in foster and/or adoptive families on sensitive parenting, dysfunctional discipline, knowledge and attitudes, and stress, and on child attachment security, child behavior problems, child diurnal cortisol levels, and placement disruption. Contrary to the meta-analysis of Van Andel et al. (Reference Van Andel, Grietens, Strijker, Van der Gaag and Knorth2012), the current study included studies with (at least) one intervention and one (randomized) control group that did not consider foster care as type of intervention, and that specifically reported results for foster and/or adoptive parents. In addition, compared to the meta-analysis of Solomon et al. (Reference Solomon, Niec and Schoonover2017), effectiveness studies of interventions working with foster and/or adoptive families were also included if they reported outcomes on parenting stress, child attachment security, children's diurnal cortisol levels, and placement disruption. In addition, studies with both kinship and non-kinship foster families were included. The current meta-analysis aims to provide insight in whether parenting interventions for foster and adoptive parents are effective in improving parenting, and whether parenting interventions can indirectly enhance child outcomes and placement disruptions.
Method
Literature search
A systematic search in three digital databases (ERIC, PsycINFO, and Web of Science) was done to identify eligible studies published before January 2018. The databases were searched using the following terms: interven* and/or preven*, combined with foster* and/or adopt*, and parent* and/or mother* and/or father*. The initial search resulted in 9,632 records. Fifteen papers were additionally included based on other sources, for example, previously written meta-analyses and systematic reviews (Benjamin, Reference Benjamin2010; Chamberlain, Moreland, & Reid, Reference Chamberlain, Moreland and Reid1992; Fisher & Kim, Reference Fisher and Kim2007; Jonkman et al., Reference Jonkman, Schuengel, Oosterman, Lindeboom, Boer and Lindauer2017; Leathers, Spielfogel, Gleeson, & Rolock, Reference Leathers, Spielfogel, Gleeson and Rolock2012; Lee & Holland, Reference Lee and Holland1991; Linares, Li, & Shrout, Reference Linares, Li and Shrout2012; Linares, Montalto, Li, & Oza, Reference Linares, Montalto, Li and Oza2006; Macdonald & Turner, Reference Macdonald and Turner2005; Price et al., Reference Price, Chamberlain, Landsverk, Reid, Leve and Laurent2008; Selwyn, Del Tufo, & Frazer, Reference Selwyn, Del Tufo and Frazer2009; Sprang, Reference Sprang2009; Triantafillou, Reference Triantafillou2002; Vranjin, Reference Vranjin2012; Wassall, Reference Wassall2011). After deletion of duplicates (n = 1,652) the retrieved titles, abstracts, and full texts were subsequently screened for their eligibility. Papers, dissertations, and (sections of) books were included when they were written in English and if they compared an intervention group of foster and/or adoptive parents with a control group. This resulted in a total of 63 records, of which two papers were not found with the initial search but are a result from screening reference lists during the coding phase. A flow chart of the search process is presented in Figure 1. Interrater agreement of three coders for the selection of eligible records was good for both the screening of titles and abstracts (κ = .95) and the screening of full text records (κ = 1.00).

Figure 1. Flow diagram of literature search.
Coding system
To identify possible constructs for separate meta-analyses and moderators, the outcome, sample, study design, and intervention characteristics of each study were coded using a standardized coding system. Outcome characteristics were name of construct, instrument used to measure this construct, number of subscales used, and type of instrument (independent observation, independent assessment, self-report questionnaire parent, self-report questionnaire teacher/case worker, self-report questionnaire child, physiological assessment, or other). Sample characteristics were country of study, child age (M, SD, and range), and whether the children displayed problem behavior at time of inclusion (risk sample yes/no). The target group of the intervention program was coded as foster care, adoption, or combination of both. We subsequently coded if the foster care target groups consisted of non-kinship, kinship, or a combination of non-kinship and kinship foster parents. For the adoption target groups, we coded if the study included domestic, international, or a combination of domestic and international adoptions. Study design characteristics were use of intent-to-treat analyses (yes or no), and level of randomization (random or nonrandom control group). Parent and child outcome variables and the sample and study design characteristics are presented in Table 1.
Table 1. Sample and study design characteristics
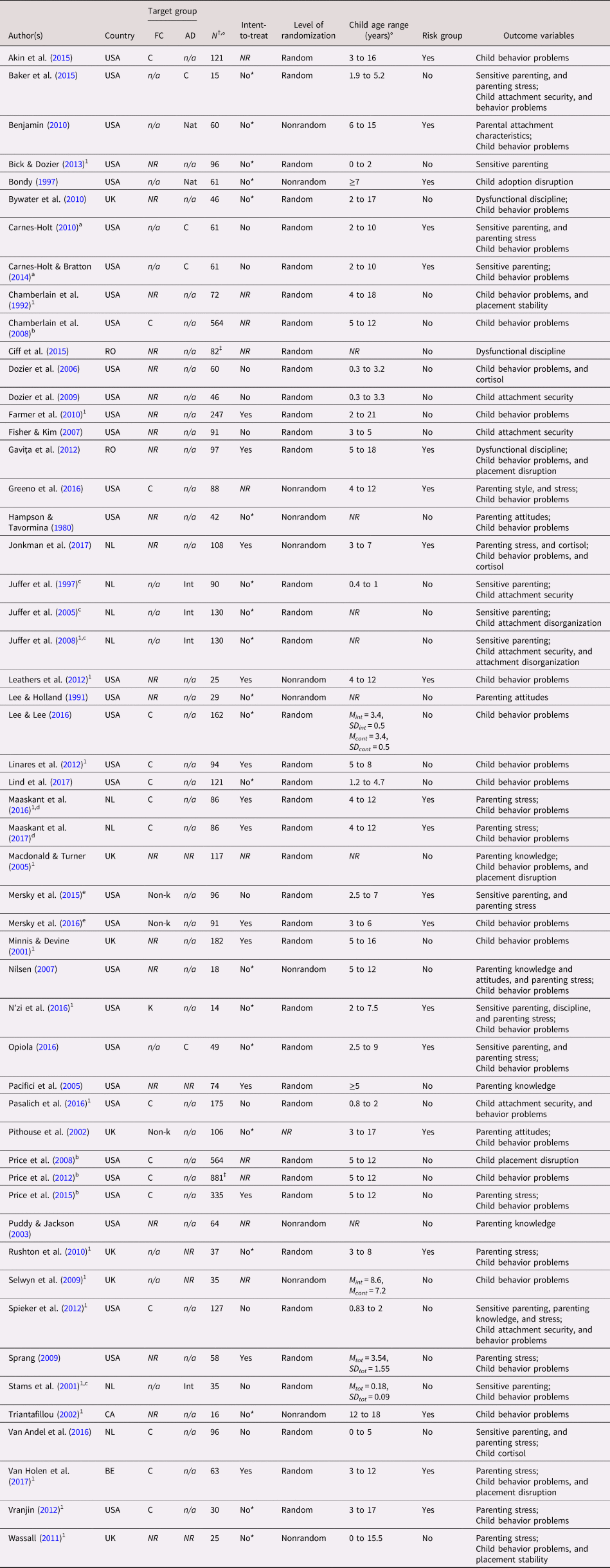
Note: BE, Belgium. CA, Canada. IL, Israel. NL, The Netherlands. RO, Romania. USA, United States of America. UK, United Kingdom. Non-k, non-kinship foster care. K, kinship foster care. Nat, national adoption. Int, international adoption. C, combination. NR, not reported. n/a, not applicable.1Study with at least one follow-up measurement, a,b,c,d,e(Partially) same study sample. †At posttest. ‡At pretest. °Unless other indicated. *Not needed because no attrition.
Intervention characteristics included name of the intervention program, delivery format (group and/or individual), setting of delivery (home, community center, or other), number of sessions, duration of intervention program (in months), focus of intervention program (psycho-education, video feedback, video modeling, in the moment feedback, or other), and control group treatment (dummy intervention, waitlist, or care as usual). An overview of the most relevant intervention characteristics is presented in Table 2.
Table 2. Characteristics of intervention studies included in the meta-analysis
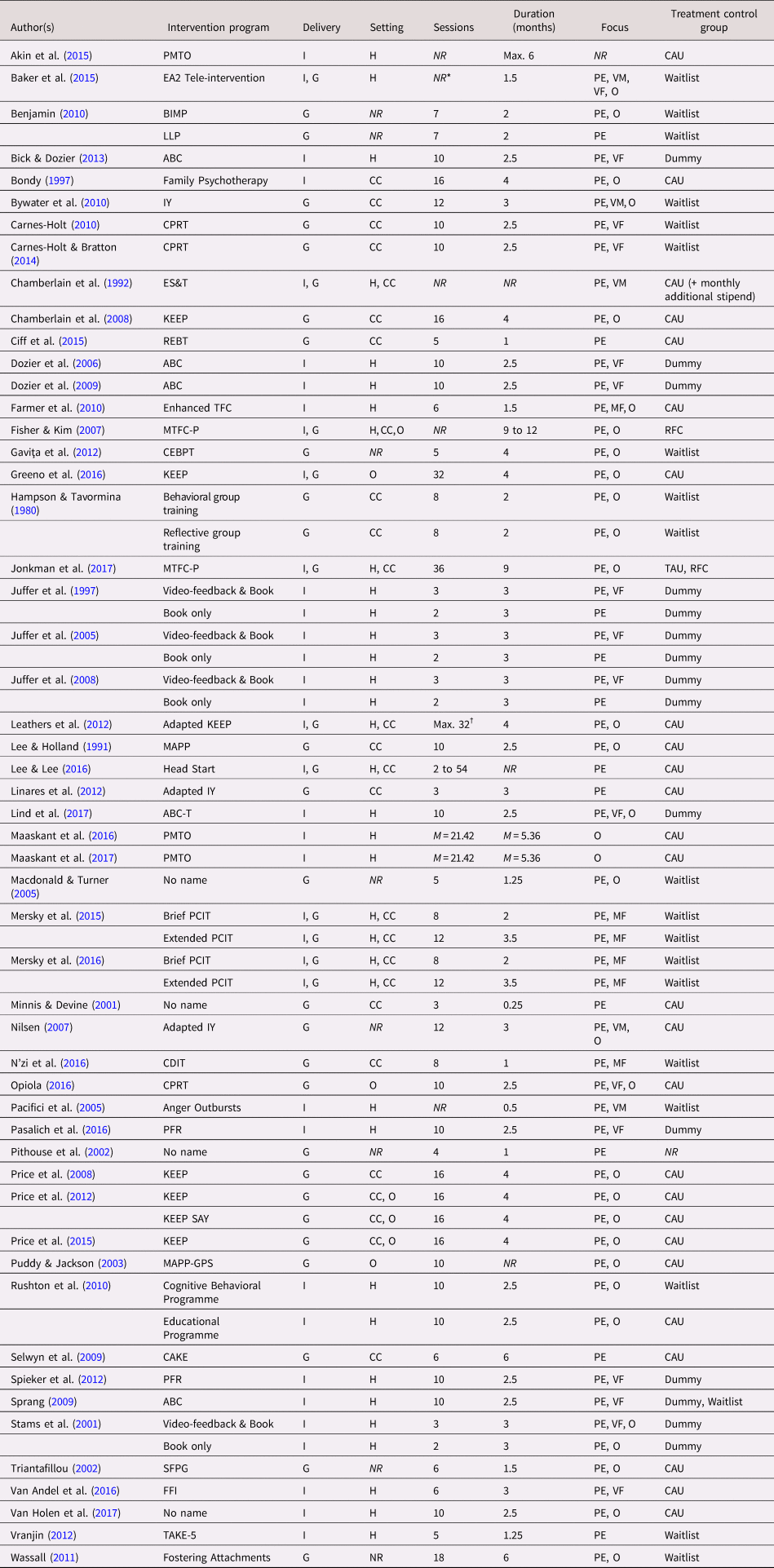
Note: ABC(-T), Attachment and Biobehavioral Catch-up(-Toddlers). BIMP, Benjamin Interactive Parenting. CAKE, It's a Piece of Cake? CDIT, Child Direction Interaction Training. CEBPT, Short Enhanced Cognitive-Behavioral Parent Training. CPRT, Child Parent Relationship Therapy. EA2, Emotional Attachment and Emotional Availability. EIFC, Early Intervention Foster Care. Enhanced TFC, enhanced treatment foster care. ES&T, enhanced support and training. FFI, Foster Family Intervention. IY, Incredible Years. KEEP (SAY), Keeping Foster Parents Trained and Supported (Social Advocates for Youth). LLP, Love and Logic Parenting. MAPP(-GPS), Model Approach to Partnerships in Parenting(/Group Selection and Participation of Foster and/or Adoptive Families). MTFC-P, Multidimensional Treatment Foster Care for Preschoolers. PCIT, Parent-Child Interaction Therapy. PFR, Promoting First Relationships. PMTO, Parent Management Training—Oregon model. REBT, Reactional Emotive Behavior Therapy. SFPG, Solution-Focused Parent Groups. TAKE-5, Trauma Affects Kids Everywhere—5 ways to resilience. G, group. I, individual. H, home. CC, community center. PE, psycho-education. VM, video modeling. VF, video feedback. MF, in the moment feedback. CAU, care as usual. RFC, regular foster care. O, other. NR, not reported. *Number of group sessions not reported, one individual session via Skype, †Number of individual sessions max. 16.
Interrater reliability between three coders was good; intraclass correlations for continuous characteristics ranged from .96 to 1.00 (k = 10) and the percentages of agreements between coders for categorical characteristics ranged from 70% to 100% (M = 88.5, SD = 10.3, k = 10). All studies were coded by the first author, and more than half of the studies (k = 39, including the 10 studies coded by all coders and used to calculate interrater reliability and coder agreements) were independently double coded by at least one other coder. Disagreements were discussed and consensus scores were made and used in the meta-analyses.
Outcome constructs
To perform a meta-analysis on a certain outcome, at least three studies reporting results on the same outcome were needed. Eight relevant constructs with sufficient effect sizes were identified: four regarding parent outcomes (sensitive parenting, dysfunctional discipline, parenting knowledge and attitudes, and parenting stress) and three regarding child outcomes (attachment security, behavior problems, and diurnal cortisol levels), and (temporary) placement disruptions. To assess the construct(s) relevant for each study, the measurement instruments used in each study were critically reviewed. Three studies reported intervention (non)effects on empathy using the Measurement of Empathy in Adult–Child Interaction (Carnes-Holt, Reference Carnes-Holt2010; Carnes-Holt & Bratton, Reference Carnes-Holt and Bratton2014; Opiola, Reference Opiola2016), but after in depth review of this measure, it was decided that this instrument fitted the sensitive parenting construct. Other studies labeled their outcome “parenting” or “parent–child interaction,” which were coded as sensitive parenting (i.e., Mersky et al., Reference Mersky, Topitzes, Janczewski and McNeil2015; N'zi et al., Reference N'zi, Stevens and Eyberg2016), dysfunctional discipline (i.e., Bywater et al., Reference Bywater, Hutchings, Linck, Whitaker, Daley, Yeo and Edwards2010; Ciff et al., Reference Ciff, Rus, Butterfield and Parris2015), or knowledge and attitudes (i.e., Lee & Holland, Reference Lee and Holland1991; Pithouse, Hill-Tout, & Lowe, Reference Pithouse, Hill-Tout and Lowe2002; Puddy & Jackson, Reference Puddy and Jackson2003; Spieker et al., Reference Spieker, Oxford, Kelly, Nelson and Fleming2012). Two meta-analyses were performed for child behavior problems: one including studies with results on behavior problems reported only by parents, and one including studies with results on parent and teacher/professional-reported behavior problems.
Unfortunately, not all instruments used in the studies could be coded as at least one of the eight constructs. Seven studies were excluded because they had outcomes that did not match the constructs (Bammens, Adkins, & Badger, Reference Bammens, Adkins and Badger2015; Bernard, Lee, & Dozier, Reference Bernard, Lee and Dozier2017; Dollberg & Keren, Reference Dollberg and Keren2013; Dozier, Peloso, Lewis, Laurenceau, & Levine, Reference Dozier, Peloso, Lewis, Laurenceau and Levine2008; Linares et al., Reference Linares, Jimenez, Nesci, Pearson, Beller, Edwards and Levin-Rector2015; Nelson & Spieker, Reference Nelson and Spieker2013; Spieker, Oxford, & Fleming, Reference Spieker, Oxford and Fleming2014). Thus, 56 studies were eligible for data extraction (Figure 1).
Effect size extraction
Of the included studies, only one study reported posttest data only (i.e., Dozier et al., Reference Dozier, Lindhiem, Lewis, Bick, Bernard and Peloso2009), but all other studies reported data on or a change score between at least two measurements: pretest and posttest data. If a study reported data on more than one posttest measurement, the data of the measurement closest to the completion of the intervention was used. The separate meta-analyses were as much as possible based on raw data (means, standard deviations, and sample size of the pre- and posttest). Twelve studies used data of the same sample (e.g., Carnes-Holt, Reference Carnes-Holt2010, and Carnes-Holt & Bratton, Reference Carnes-Holt and Bratton2014; Table 1). To ensure independence between samples in the meta-analyses, these studies could not be included in the same meta-analysis. The study with the most complete data (e.g., larger sample size, more outcome variables, etc.) was used in the meta-analyses, with a preference for peer-reviewed papers over dissertations or (sections of) books, and a preference of the most recently published paper over older publications (e.g., Euser, Alink, Stoltenborgh, Bakermans-Kranenburg, & van IJzendoorn, Reference Euser, Alink, Stoltenborgh, Bakermans-Kranenburg and van IJzendoorn2015; Goemans, Van Geel, & Vedder, Reference Goemans, Van Geel and Vedder2015). However, if the studies reported data of the same sample on different outcome variables, they could be included in separate meta-analyses. For example, Mersky et al. (Reference Mersky, Topitzes, Janczewski and McNeil2015) and Mersky et al. (Reference Mersky, Topitzes, Grant-Savela, Brondino and McNeil2016) used data from the same sample, but Mersky et al. (Reference Mersky, Topitzes, Janczewski and McNeil2015) was included in the meta-analyses on sensitive parenting and parenting stress, and Mersky et al. (Reference Mersky, Topitzes, Grant-Savela, Brondino and McNeil2016) in the meta-analysis on child behavior problems. In addition, some studies used multiple instruments to measure the same outcome variable within one study. For example, Juffer, Bakermans-Kranenburg, and van IJzendoorn (Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005) used the Ainsworth coding scales for sensitivity and cooperation to measure sensitive parenting. In these cases, data of the different scales/instruments were averaged in the meta-analyses. Finally, some studies examined the effectiveness of two intervention programs (see Table 2). These studies were considered as presenting two independent studies, and they were thus included twice in the meta-analyses, but with a halved sample size of the control group compared to the whole sample size of each intervention group to prevent that the participants of the control group were included twice in the meta-analysis (Werner, Linting, Vermeer, & van IJzendoorn, Reference Werner, Linting, Vermeer and van IJzendoorn2016).
To include data of all 56 records, the authors of four studies were contacted to provide data on (a number of) outcome variables. We obtained the requested data of Spieker et al. (Reference Spieker, Oxford, Kelly, Nelson and Fleming2012). Thus, 53 studies were included in the final meta-analyses (Figure 1).
Data analyses
Eight meta-analyses were conducted to examine the effectiveness of parenting interventions on the different parent and child outcomes using Comprehensive Meta-Analysis version 2 (Borenstein, Rothstein, & Cohen, Reference Borenstein, Rothstein and Cohen2005). Sample size, raw means and standard deviations of (preferably) pre- and posttest, or change scores of means and standard deviations, and aggregated test–retest correlation were used to compute Hedges's g (Morris & DeShon, Reference Morris and DeShon2002). Hedges's g is for the most part a similar effect size measure as Cohen's d, but where Cohen's d tends to overestimate the effect sizes of small samples, Hedges's g removes this bias from Cohen's d and thus represents an unbiased estimate of the overall effect size. Hedges's g can be calculated by the difference between two means divided by the pooled standard deviation (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2009). If the test–retest correlation was not reported in the included studies of any of the eight meta-analyses, a literature search was performed to make a substantiated estimate (Borenstein et al., Reference Borenstein, Hedges, Higgins and Rothstein2009). Only for the meta-analysis on parental dysfunctional discipline an estimate of .50 was used, due to lack of reports on the test–retest correlation. All included studies in this meta-analysis used a questionnaire to measure parental discipline, and a test–retest correlation of .50 is a conservative estimate considering that questionnaires usually have a moderate to high test–retest correlation.
Assuming that there is variation in effect sizes per study, a random effects models was used to analyze the data and calculate an estimated overall effect size of the distribution of effect sizes of the included studies per construct (Borenstein et al., Reference Borenstein, Hedges, Higgins and Rothstein2009). The homogeneity across studies was tested with Q-statistics, with a significant Q test indicating true homogeneity across studies. To quantify the heterogeneity between the effect sizes of the included studies, the I 2 was used. I 2 represents the percentage of total variability in a set of effect sizes due to true heterogeneity (Borenstein, Higgins, Hedges, & Rothstein, Reference Borenstein, Higgins, Hedges and Rothstein2017). If I 2 is large, the proportion of variance of observed effects is due to a high variation in true effects rather than sampling error.
Outliers were identified by transforming the individual effect sizes of the included studies into standardized z scores with –3.29 < z > 3.29 indicating outlying effect sizes (Tabachnick & Fidell, Reference Tabachnick and Fidell2007). Only the study of Baker, Biringen, Meyer-Parsons, and Schneider (Reference Baker, Biringen, Meyer-Parsons and Schneider2015) had an outlying effect size (z > 3.29) in the meta-analysis of child behavior problems. This meta-analysis was done twice: once without and once with the outlying effect size.
To control for possible publication bias, and thus an overestimation of the effect sizes in the meta-analyses, Kendall's τ and the trim-and-fill procedure were used. Kendall's τ was used to assess the risk of publication bias. The Kendall's τ method calculates the relation between the standardized effect sizes and the variance of these effect sizes (Begg & Mazumdar, Reference Begg and Mazumdar1994; Macaskill, Walter, & Irwig, Reference Macaskill, Walter and Irwig2001). The presence of possible publication bias is indicated by a significant correlation that indicates that studies with small sample sizes and nonsignificant results were unlikely to be published. The trim-and-fill procedure constructs a funnel plot of the effect sizes of the studies against the sample size or the standard error (usually plotted as 1/SE, or precision; Duval & Tweedie, Reference Duval and Tweedie2000a, Reference Duval and Tweedie2000b). If no publication error is present, the funnel plot will look like a normality curve: increasing large variation in effect sizes is expected for studies with smaller sample sizes and larger standard errors, whereas smaller variation in effect sizes is expected in studies with larger sample sizes and smaller standard errors (Duval & Tweedie, Reference Duval and Tweedie2000b; Sutton, Duval, Tweedie, Abrams, & Jones, Reference Sutton, Duval, Tweedie, Abrams and Jones2000). However, studies with results in the unexpected direction are less likely to be published and are thus missing in the bottom left-hand corner of the plot (Sutton et al., Reference Sutton, Duval, Tweedie, Abrams and Jones2000). The trim-and-fill procedure trims the k right-most studies considered to be symmetrically unmatched, and fills (i.e., imputes) their missing counterparts as mirror images of the trimmed outcomes. An adjusted estimate of the overall effect size could subsequently be calculated, taking a potential publication bias into account (Gilbody, Song, Eastwood, & Sutton, Reference Gilbody, Song, Eastwood and Sutton2000).
Moderator analyses
The included studies varied in sample, study design, and intervention characteristics. Some studies used a randomized controlled trial, whereas others had a quasi-experimental design. Studies also varied in target group (foster care, adoption, or both), in examining a risk group or not, and in age of the included children. The investigated intervention programs varied in delivery format (group meetings, individual meetings, or both), in setting (home or community center), in number of sessions, and in using video-feedback or not. Moderator analyses were therefore performed to examine the associations of some of these characteristics with intervention program effects.
For each meta-analysis, several moderator analyses were performed if possible. The role of potential moderators related to sample, study design, or intervention characteristics were examined only if a subset consisted of at least three studies (k ≥ 3). Considering sample characteristics, it was examined whether the outcomes of intervention programs differed between foster and adoptive parents. In addition, the overall intervention effects for families with children who displayed high levels of behavior problems (risk group = yes) were compared with families with children who did not (risk group = no). Considering study design characteristics, the overall effect of studies that included a random control group were compared with studies with a nonrandom control group. Finally, considering intervention characteristics, intervention programs that used video-feedback were compared with interventions with another focus. Intervention programs working with groups, individuals, or both were also compared. Different intervention settings were compared, distinguishing between at home, at a community center, or both.
The number of sessions varied between intervention programs, and a meta-regression analysis was conducted to examine the moderator effect of this intervention characteristic. Because children's age range varied between studies, two meta-regression analyses were performed for each meta-analysis using continuous moderators for child age: one for the minimum age and one for the maximum age of the children included in the studies.
Results
Parent outcomes
Sensitive parenting
Eleven studies yielded effect sizes on sensitive parenting of a total of 684 foster and/or adoptive parents (Table 3). There was a significant and large combined effect size of Hedges's g = 2.20, p < .001. Figure 2 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates an increase in sensitive parenting. The Q statistic showed that the studies included in the meta-analysis were highly heterogeneous, Q (10) = 233.73, p < .001, and the percentage of variance was fairly high (I 2 = 95.72); thus the proportion of the variance of observed effects is due to a high variation in true effects rather than sampling error.
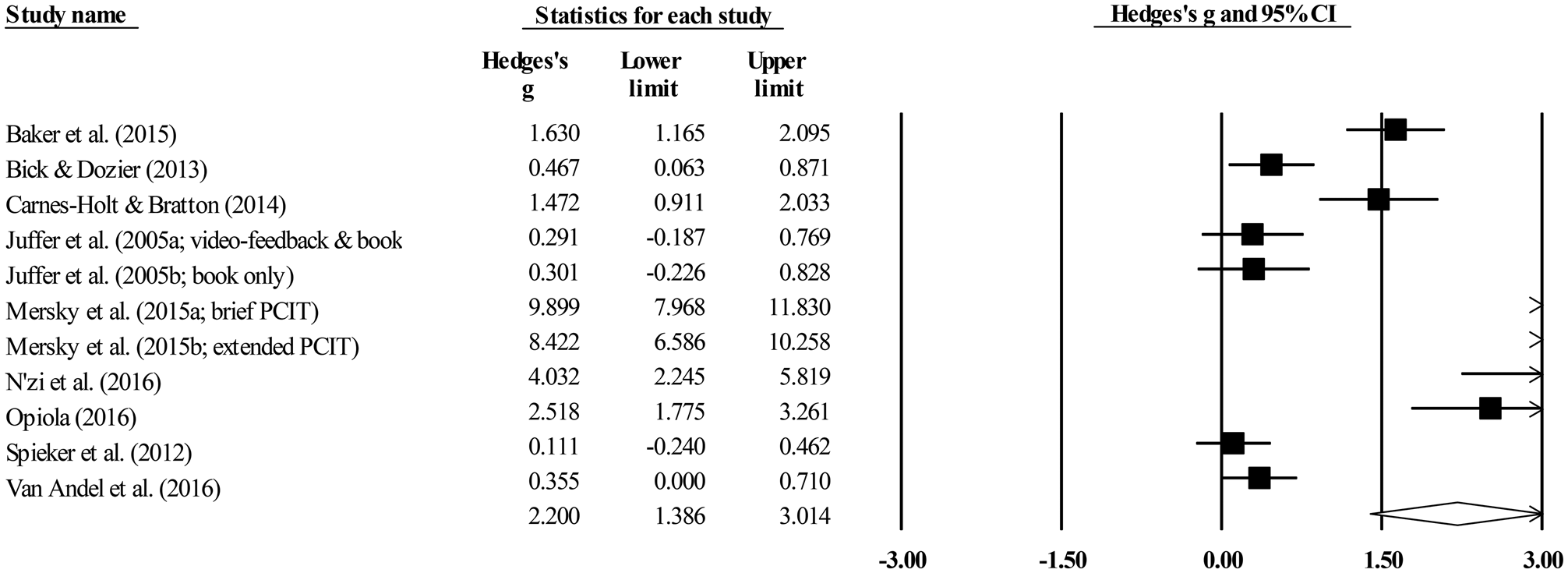
Figure 2. Forest plot for the meta-analysis on sensitive parenting.
Table 3. Results of the meta-analyses on parent and child constructs

Note: Results from the trim-and-fill procedure are only mentioned in the text; none of the trim-and-fill results yielded different results. aWithout the outlying effect size of Baker et al. (Reference Baker, Biringen, Meyer-Parsons and Schneider2015). *p < .05. **p < .001.
The results for publication bias were inconclusive. Kendall's τ was 0.73 (z = 3.11, p = .002), which suggests the presence of publication bias (Table 3), while Duvall and Tweedie's trim-and-fill procedure did not. Results indicate that foster and/or adoptive parents receiving a parenting intervention showed significantly stronger improvements in sensitive parenting between pre- and posttest compared to the control group.
Overall effect sizes of studies that examined intervention programs working with foster parents (g = 3.21, p < .001, k = 6, N = 429) were significantly higher than those of studies examining intervention programs for adoptive parents (g = 1.23, p < .05, k = 5, N = 255), Q (1) = 5.08, p = .049 (Table 4). Studies that focused on interventions with children who displayed high levels of behavior problems (g = 4.55, p < .001, k = 6, N = 220) were also significantly more effective than studies that did not (g = 0.52, p = .23, k = 5, N = 464), Q (1) = 32.57, p < .001 (Table 4). In addition, effect sizes of intervention programs working with groups (g = 2.47, p < .001, k = 3, N = 124) and intervention programs working with both groups and individual parents (g = 5.62, p < .001, k = 3, N = 111) were significantly higher than those of studies working with only individuals (g = 0.31, p = .52, k = 3, N = 449), Q (1) = 37.86, p < .001 (Table 4). The intervention programs working with both groups and individuals were most effective. Meta-regression analyses showed that intervention effects were significantly moderated by number of sessions (z = 3.28, p = .001, k = 10, N = 669, range: 2 to 12 sessions), and by minimum age (z = 10.18, p < .001, k = 11, N = 684, range: 0 to 2.5 years) and maximum age (z = 8.28, p < .001, k = 11, N = 684, range: 1 to 10 years) of the included children. Studies that examined the effectiveness of intervention programs on sensitive parenting were most effective if intervention programs had a higher number of sessions and targeted older children.
Table 4. Results of the categorical moderator analyses on parent constructs

Note: Categorical moderator analyses were only performed if a subset consisted of at least three studies (k ≥ 3); therefore, no moderator analyses were possible for the meta-analysis on dysfunctional discipline. *p < .05. **p < .001.
Dysfunctional discipline
Four studies yielded effect sizes on dysfunctional discipline of a total of 239 foster and/or adoptive parents (Table 3). There was a significant and medium combined effect size of Hedges's g = 0.58, p = .01. Figure 3 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates a decrease in dysfunctional discipline. The Q statistic showed that the studies included in the meta-analysis were homogeneous, Q (3) = 7.23, p = .07, and the percentage of variance was mediocre (I 2 = 58.50); thus proportion of the variance of observed effects is due to some variation in true effects rather than sampling error.

Figure 3. Forest plot for the meta-analysis on dysfunctional discipline.
Kendall's τ was –0.17 (z = 0.34, p = .73), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure showed that one study to the left of the mean was likely to be missing. If this study was trimmed and filled the point estimate would shift from 0.58 (95% confidence interval; CI [0.14, 1.02]) to 0.53 (95% CI [0.13, 0.93]), which still indicates a significant overall effect. Based on the results of these two measurements, it was assumed that there were no strong indications for the presence and effect of publication bias. Thus, results indicate that dysfunctional discipline of foster and/or adoptive parents receiving a parenting intervention decreased significantly more between pre- and posttest compared to the control group.
Categorical moderator analyses were not possible, because the subsets consisted of fewer than three studies. Meta-regression analyses showed that intervention effects were significantly moderated by number of sessions (z = –2.41, p = .02, k = 4, N = 239, range: 5 to 12 sessions), and by minimum age (z = 2.07, p = .04, k = 3, N = 157, range: 2 to 5 years). The effect size was highest for intervention programs with a lower number of sessions and for studies including children with a higher minimum age. No moderator effect was found for studies with maximum child age (z = –0.34, p = .74, k = 3, N = 157, range: 7.5 to 8 years).
Parenting knowledge and attitudes
Seven studies yielded effect sizes on knowledge and attitudes of a total of 535 foster and/or adoptive parents (Table 3). There was a significant and small to medium combined effect size of Hedges's g = 0.35, p = .01. Figure 4 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates an increase in parenting knowledge and attitudes. The Q statistic showed that the studies included in the meta-analysis were homogeneous, Q (6) = 12.50, p = .05, and the percentage of variance was mediocre (I 2 = 51.99); thus proportion of the variance of observed effects is due to some variation in true effects rather than sampling error.
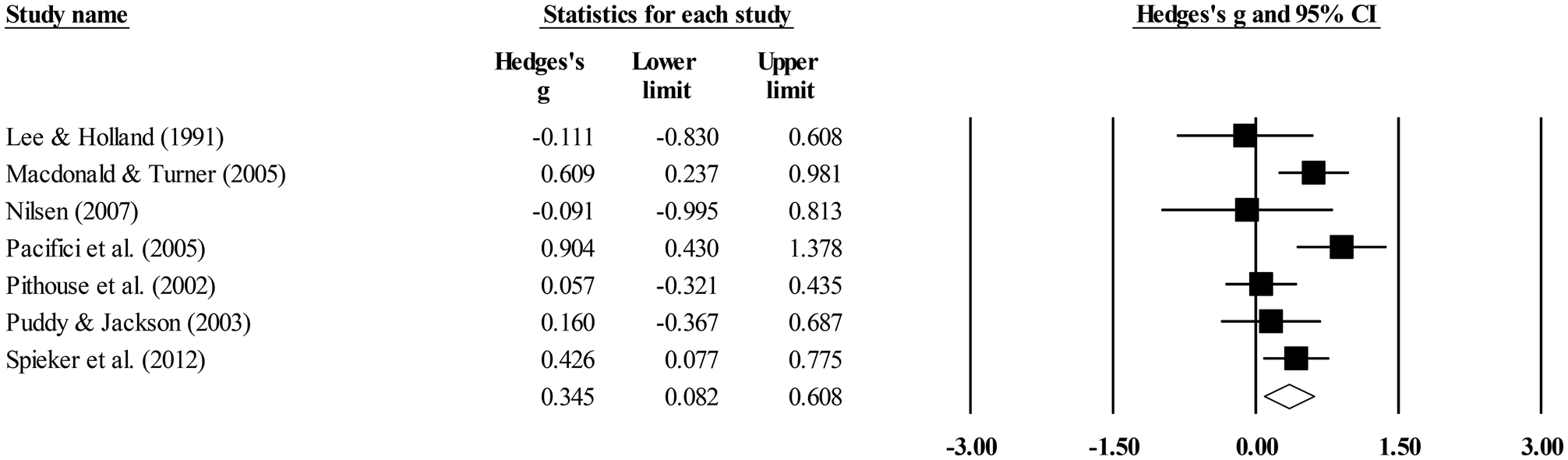
Figure 4. Forest plot for the meta-analysis on parenting knowledge and attitudes.
Kendall's τ was –0.19 (z = 0.60, p = .55), which suggests absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure showed that one study to the right of the mean was likely to be missing. If this study was trimmed and filled, the point estimate would shift from 0.35 (95% CI [0.08, 0.62]) to 0.40 (95% CI [0.23, 0.60]), which still indicates a significant overall effect. Based on the results of these two measurements, it was assumed that there were no strong indications for the presence and the effect of publication bias. Thus, results show that foster and/or adoptive parents receiving a parenting intervention improved significantly more between pre- and posttest in parenting knowledge and attitudes compared to the control group.
Overall effect sizes of studies with a random control group (g = 0.60, p < .001, k = 3, N = 318) were significantly higher than those of studies with a nonrandom control group (g = 0.04, p = .85, k = 3, N = 111), Q (1) = 6.12, p < .05 (Table 4). Meta-regression analysis showed no significant effect for number of sessions (z = –0.31, p = .74, k = 6, N = 461, range: 4 to 12 sessions). Regarding child age, only a meta-regression for minimum child age was possible and this analysis showed that intervention effects were not moderated by minimum age (z = 0.66, p = .51, k = 3, N = 325, range: 0.8 to 5 years).
Parenting stress
Eighteen studies yielded effect sizes on parenting stress of a total of 1,306 foster and/or adoptive parents (Table 3). There was a significant and medium combined effect size of Hedges's g = 0.60, p = .002. Figure 5 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates a decrease in parenting stress. The Q statistic showed that the studies included in the meta-analysis were highly heterogeneous, Q (17) = 171.71, p < .001, and the percentage of variance was fairly high (I 2 = 90.10); thus proportion of the variance of observed effects is due to a high variation in true effects rather than sampling error.
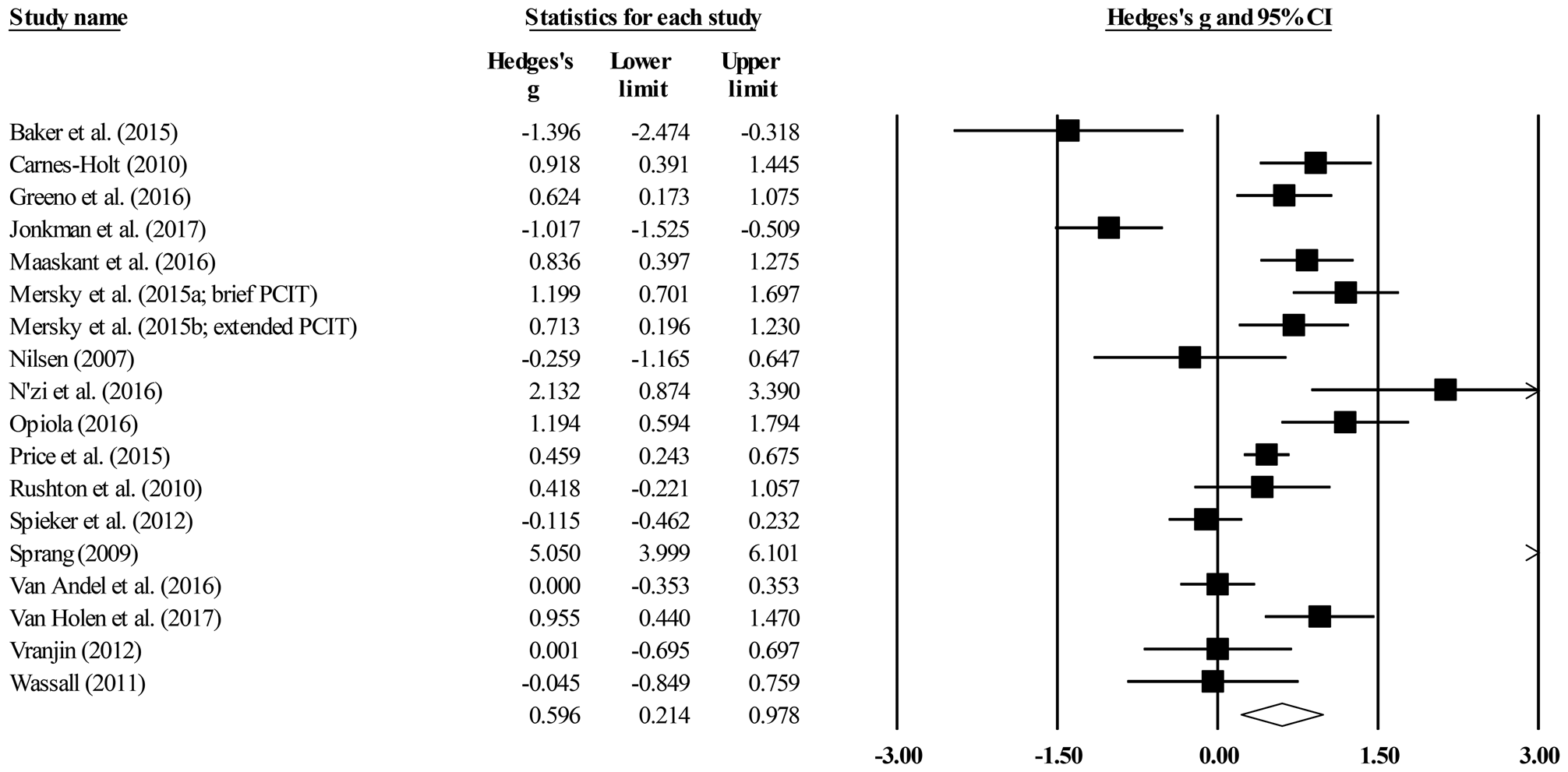
Figure 5. Forest plot for the meta-analysis on parenting stress.
Kendall's τ was 0.07 (z = 0.38, p = .70), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure also indicated no publication bias. Thus, results indicate that parenting stress of foster and/or adoptive parents receiving a parenting intervention decreased significantly more between pre- and posttest compared to the control group.
Of six categorical moderator analyses, only the moderator analysis that compared studies with a random control group and studies with a nonrandom control group yielded a significant difference, Q (1) = 4.44, p < .05 (Table 4). The overall effect size of studies with a random control group (g = 0.81, p < .001, k = 14, N = 1,067) was significantly higher than the overall effect size of studies with a nonrandom control group (g = –0.17, p = .68, k = 4, N = 239). In addition, meta-regression analyses showed that intervention effects were significantly moderated by number of sessions (z = –3.39, p = .001, k = 16, N = 1,205, range: 5 to 36 sessions), by minimum age (z = 2.68, p = .01, k = 17, N = 1,248, range: 0 to 5 years) and maximum age (z = 3.39, p < .001, k = 17, N = 1,248, range: 2 to 17 years) of the included children. Intervention programs on parenting stress were most effective if intervention programs had a lower number of sessions and for older children.
Child outcomes
Attachment security
Six studies yielded effect sizes on children's attachment security of a total of 369 foster and/or adopted children (Table 3). There was a nonsignificant combined effect size of Hedges's g = 0.22, p = .14. Figure 6 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates an increase in attachment security. The Q statistic showed that the studies included in the meta-analysis were homogeneous, Q (5) = 8.77, p = .12, and the percentage of variance was mediocre (I 2 = 43.02); thus proportion of the variance of observed effects is due to some variation in true effects rather than sampling error.
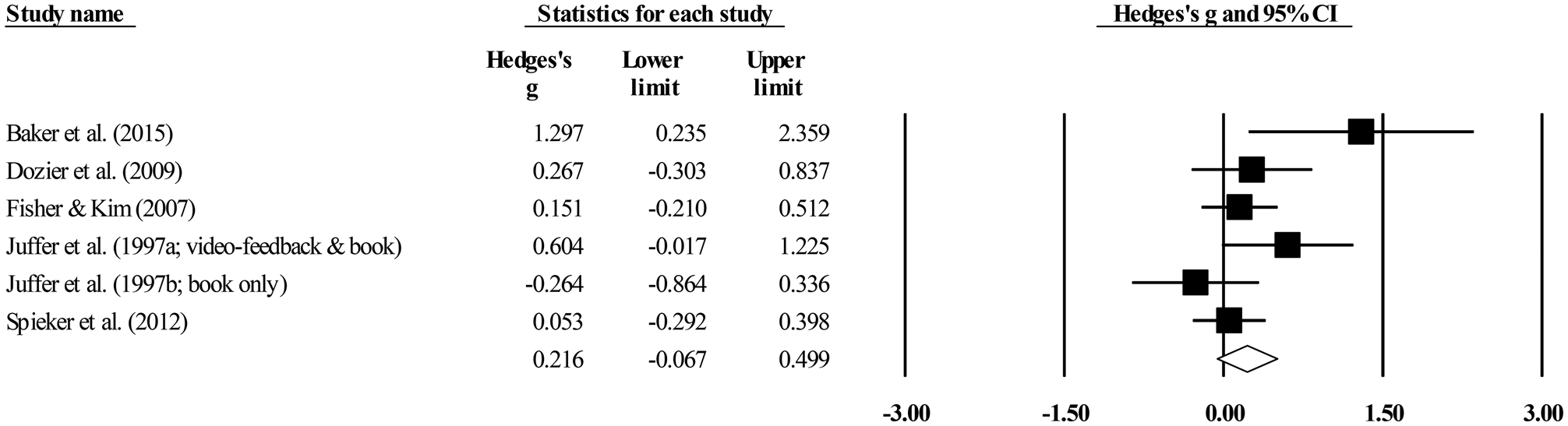
Figure 6. Forest plot for the meta-analysis on attachment security.
Kendall's τ was 0.53 (z = 1.50, p = .13), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure also indicated no publication bias. Thus, results show that foster and/or adopted children of foster and adoptive parents attending an intervention program did not improve significantly more between pre- and posttest in attachment security compared to the control group.
Neither intervention programs working with adoptive (g = 0.37, p = .15, k = 3, N = 105) nor with foster parents (g = 0.14, p = .47, k = 3, N = 264) were found to improve scores of attachment security, Q (1) = 0.50, p = .48 (Table 5). Meta-regression analyses showed that intervention effects were not moderated by number of sessions (z = 0.00, p = 1.00, k = 4, N = 263, range: 2 to 10 sessions), minimum age (z = 0.21, p = .83, k = 6, N = 264, range: 0.3 to 3 years), nor maximum age (z = 0.76, p = .45, k = 6, N = 264, range: 1 to 5 years) of the included children.
Table 5. Results of the categorical moderator analyses on child constructs and placement disruption
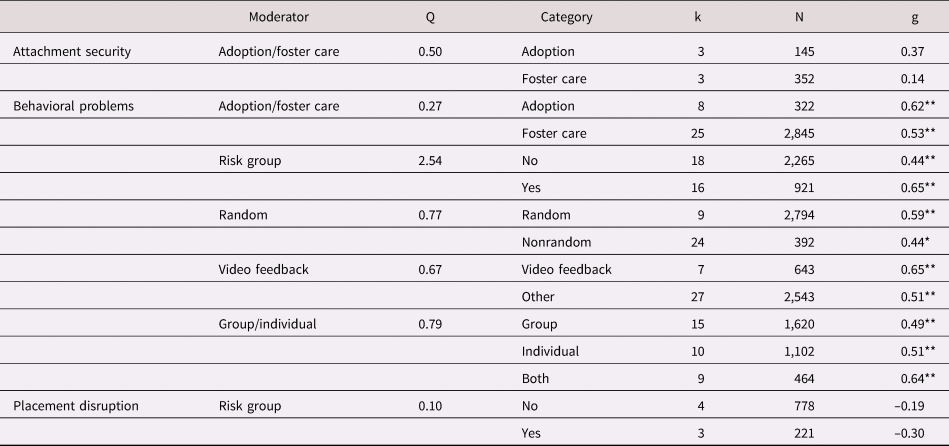
Note. Categorical moderator analyses were only performed if a subset consisted of at least three studies (k ≥ 3); therefore, no moderator analyses were possible for the meta-analysis on diurnal cortisol levels. *p < .05. **p < .001.
Behavior problems
Thirty-three studies yielded effect sizes on children's behavior problems of a total of 3,001 foster and/or adopted children (Table 3). There was a significant and medium combined effect size of Hedges's g = 0.53, p < .001 (without the outlying effect size of Baker et al., Reference Baker, Biringen, Meyer-Parsons and Schneider2015). Figure 7 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates a decrease in behavior problems. The Q statistic showed that the studies included in the meta-analysis were highly heterogeneous, Q (32) = 87.28, p < .001, and the percentage of variance was fairly high (I 2 = 63.34); thus proportion of the variance of observed effects is due to a somewhat high variation in true effects rather than sampling error.
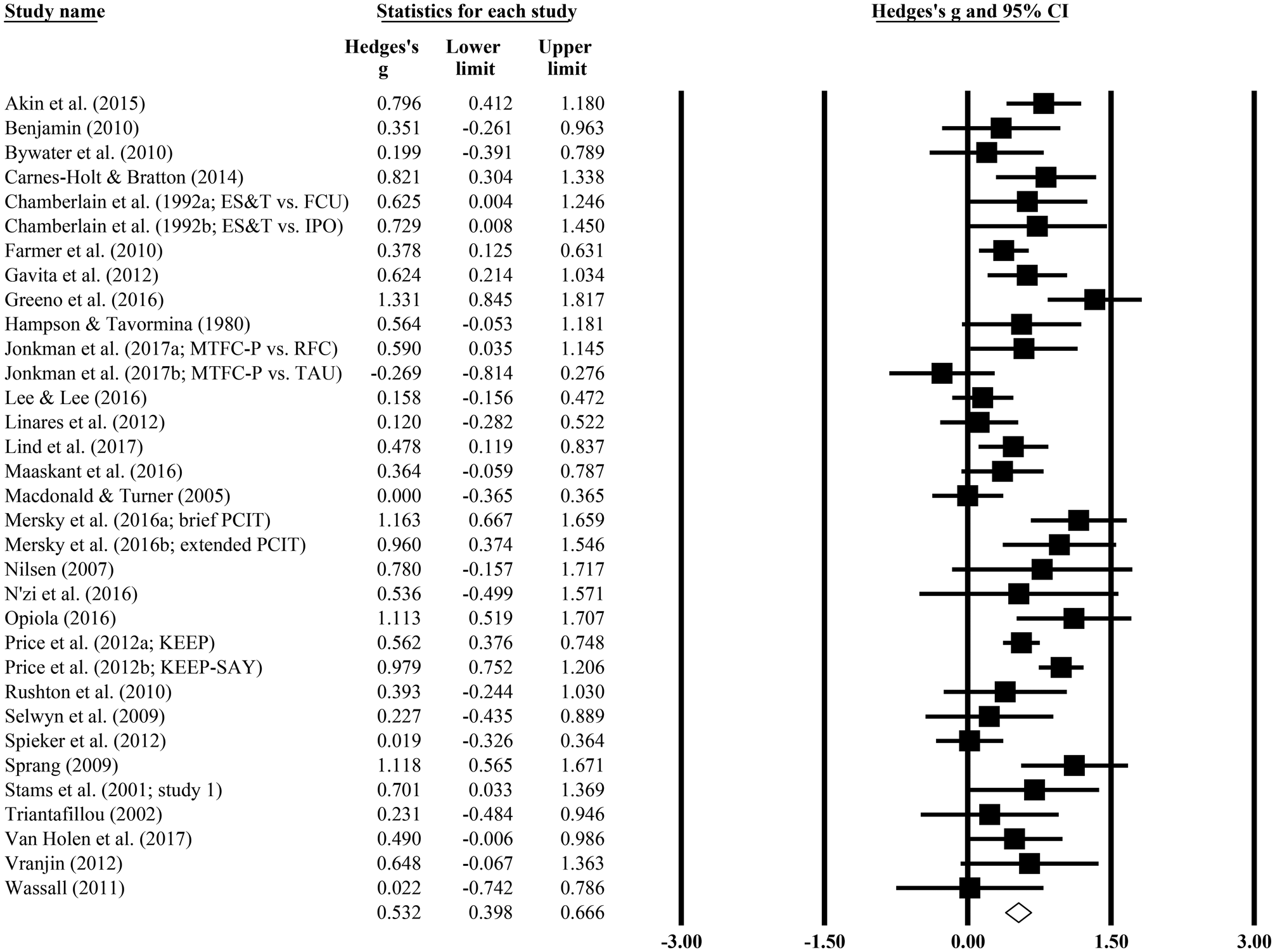
Figure 7. Forest plot for the meta-analysis on behavior problems.
Kendall's τ was 0.05 (z = 0.42, p = .68), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure also indicated no publication bias. Thus, results indicate that children of foster and adoptive parents attending an intervention program showed significantly fewer behavior problems between pre- and posttest compared to the control group. The results were similar if the outlying effect size of Baker et al. (Reference Baker, Biringen, Meyer-Parsons and Schneider2015) was included: Hedges's g = 0.56, 95% CI [0.42, 0.69], p < .001, k = 34, N = 3,016. The studies were also still highly heterogeneous, Q (33) = 96.92, p < .001, I 2 = 65.95, and Kendall's τ and the trim-and-fill procedure still suggested the absence of publication bias.
None of the categorical moderator analyses showed significant differences (Table 5). Meta-regression analyses showed that intervention effects were moderated by number of sessions (z = 2.02, p = .04, k = 28, N = 2,560, range: 3 to 36 sessions). Intervention programs on child behavior problems were most effective if intervention programs had a higher number of sessions. No moderator effects were found for minimum age (z = 1.96, p = .05, k = 27, N = 2,552, range: 0 to 12 years) and maximum age (z = 0.64, p = .52, k = 27, N = 2,552, range: 2 to 21 years) of the included children.
The 33 studies included in this meta-analysis included data on behavior problems from parent and teacher/professional reports. The majority of these studies used parent reports only (k = 29), some studies used a combination of parent and teacher/professional reports (k = 4), and only 2 studies solely used teacher/professional reports. To test whether results would be different when only parent report was used, a separate meta-analysis was conducted of effect sizes based on parent reports of children's behavior problems, and the overall effect size was compared with the combined effect size for the total set of studies in which parent and teacher/professional reports were used. The meta-analysis on parent reports showed that the overall effect size remained significant (g = 0.55, 95% CI [0.41, 0.69], p < .001, k = 31, N = 2,804) and was not different from the overall effect size based on parent and teacher/professional reports. No differences were found regarding homogeneity, Q (30) = 79.44, p < .001, I 2 = 62.24, or publication bias compared to results for parent and teacher/professional reports.
Diurnal cortisol levels
Three studies yielded effect sizes on children's diurnal cortisol levels of a total of 264 foster and/or adopted children (Table 3). There was a nonsignificant combined effect size of Hedges's g = –0.08, p = .82. Figure 8 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates a decrease in diurnal cortisol levels from pre- to posttest. The Q statistic showed that the studies included in the meta-analysis were highly heterogeneous, Q (2) = 13.38, p = .001, and the percentage of variance was fairly high (I 2 = 85.06); thus proportion of the variance of observed effects is due to a high variation in true effects rather than sampling error.

Figure 8. Forest plot for the meta-analysis on diurnal cortisol levels.
Kendall's τ was 0.00 (z = 0.00, p = 1.00), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure also indicated no publication bias. Thus, results indicate that diurnal cortisol levels of children whose foster and adoptive parents attended an intervention program did not differ significantly between pre- and posttest compared to the control group.
Categorical moderator analyses were not possible, because the subsets consisted of fewer than three studies. Meta-regression analyses were also not performed because of the small subset of studies.
Placement disruption
Seven studies yielded effect sizes on (temporary) placement disruptions of a total of 999 foster and/or adopted children (Table 3). There was a nonsignificant combined effect size of Hedges's g = 0.20, p = .05. Figure 9 presents the effect sizes of the included studies in a forest plot, in which a positive effect size indicates a decrease in placement disruptions. The Q statistic showed that the studies included in the meta-analysis were homogeneous, Q (6) = 3.99, p = .68, and there was no variance (I 2 = 0.00); thus the effect sizes of the studies included in this meta-analysis tend to be consistent.

Figure 9. Forest plot for the meta-analysis on placement disruption.
Kendall's τ was –0.10 (z = 0.30, p = .76), which suggests the absence of publication bias (Table 3). Duvall and Tweedie's trim-and-fill procedure showed that four studies to the right of the mean needed to be imputed for the meta-analysis to result in a significant overall effect size. If this study was trimmed and filled, the point estimate would shift from –0.20 (95% CI [–0.41, 0.00]) to –0.11 (95% CI [–0.30, 0.08]), which still indicates a nonsignificant overall effect. Thus, results show that foster and/or adoptive children whose caregivers received a parenting intervention did not experience fewer (temporary) placement disruptions between pre- and posttest compared to the control group based on the effect sizes of the included studies of this meta-analysis.
Overall effect sizes of studies that examined children who displayed high levels of problem behavior (g = 0.30, p = .36, k = 3, N = 221) were similar to those of studies that did not (g = 0.19, p = .08, k = 4, N = 778), Q (1) = 0.10, p = .75 (Table 5). Meta-regression analyses showed that intervention effects were not moderated by number of sessions (z = 0.99, p = .32, k = 6, N = 927, range: 5 to 18 sessions), minimum age (z = 1.05, p = .29, k = 6, N = 882, range: 0 to 7 years), nor maximum age (z = –1.09, p = .27, k = 5, N = 821, range: 12 to 18 years) of the included children.
Discussion
The effectiveness of parenting interventions for foster and/or adoptive families was tested in a series of meta-analyses regarding four parent outcomes, three child outcomes, and placement disruption. Two measurements for publication bias were used, and overall no strong indications were found for the presence and effect of publication bias.
Parent outcomes
Results showed that parenting interventions are positively effective (with small to large overall effect sizes) in improving sensitive parenting, dysfunctional discipline, parenting knowledge and attitudes, and parenting stress of foster and adoptive parents. The implementation of parenting interventions thus not only improves foster and adoptive parents’ behaviors, knowledge and attitudes, but also reduces their stress. The largest overall effect size was found for sensitive parenting, indicating that the evidence base for existing parenting interventions that are aimed at improving sensitive behaviors in foster and adoptive parents is strong. The subsets of effect sizes for dysfunctional discipline, parenting knowledge, and parenting stress yielded smaller effect sizes and may thus benefit from more studies or the development of intervention programs that specifically aim to improve these constructs. Within each subset of effect sizes, not all intervention programs directly focus on yielding a positive effect on dysfunctional discipline, parenting knowledge, or parenting stress. For example, included in the meta-analysis on parenting stress are Parent Management Training—Oregon model (used by Maaskant, Van Rooij, Overbeek, Oort, & Hermanns, Reference Maaskant, Van Rooij, Overbeek, Oort and Hermanns2016) and PCIT (Mersky et al., Reference Mersky, Topitzes, Janczewski and McNeil2015), which both aim to reduce behavior problems of foster children. Child behavior problems can increase stress in the caregivers, but neither Parent Management Training—Oregon model nor PCIT intervention do purposely aim to reduce parenting stress.
Foster versus adoptive parents
Significantly larger improvements in sensitive parenting were found for intervention programs working with foster parents compared to adoptive parents. Previous research has shown that adoptive parents display more sensitive behaviors toward their children than foster parents (Bickell, Reference Bickell2012), and this may leave little room for improving adoptive parents’ sensitive skills as compared to foster parents. Especially kinship foster parents may benefit most from parenting interventions, because they often originate from the same (deprived) socioeconomic environment as birth parents, whereas adoptive parents generally have a higher economic status (Johnson, McGue, & Iacono, Reference Johnson, McGue and Iacono2007; Sakai, Lin, & Flores, Reference Sakai, Lin and Flores2011). In addition, the perspective of a foster care placement is often temporary or unknown. Foster parents may (unconsciously) not want to invest too much in their relationship with their foster children because the children may return to their birth parents or another, more permanent, solution will be found. Adoptive parents may be more committed to the children from the start of the placement, because it is less likely than in foster care that the adoption placement will be disrupted (Van den Dries et al., Reference Van den Dries, Juffer, van IJzendoorn and Bakermans-Kranenburg2009).
Risk versus no-risk group
Intervention programs also showed significantly larger improvements in sensitive parenting if parents took care of a child displaying high levels of behavior problems compared to parents who did not. Taking care of and interacting with children who show behavior problems can be very stressful for parents, and parents’ sensitive behavior can be inhibited by elevated stress levels (Feldman et al., Reference Feldman, Weller, Zagoory-Sharon and Levine2007). Parents who take care of children with high rates of behavior problems may therefore benefit most from parenting interventions, because there is more to gain in terms of sensitive parenting and parenting stress reduction as compared to parents who do not take care of children that display high levels of behavior problems. Mersky et al. (Reference Mersky, Topitzes, Janczewski and McNeil2015) and N'zi et al. (Reference N'zi, Stevens and Eyberg2016) included at-risk families and reported improvements in both sensitive parenting and parenting stress due to intervention programs. However, in the current meta-analysis, no difference in intervention effects for families with and without children with high levels of behavior problems was found for parenting stress. This suggests that families with children who display behavior problems and with children who do not both experience less parenting stress after completing an intervention program, and parents who take care of children with behavior problems benefit more from parenting interventions that increase their sensitive parenting behavior than parents who do not take care of children with behavior problems.
Video feedback versus other interventions
It was unfortunately not possible to compare the effectiveness of intervention programs that include a video-feedback component with intervention programs that do not on sensitive parenting, discipline, and parenting knowledge and attitudes in the current meta-analytic review. The effectiveness of video-feedback intervention programs in the current meta-analysis did not differ from other interventions in improving parenting stress. Video feedback is useful if parents need help to correctly recognize and interpret behavioral signals of their children and how they can adequately respond to these signals (Fukkink, Reference Fukkink2008). However, for improving parenting stress, video feedback may not be necessary because parenting stress can be easily recognized by parents without the use of video feedback.
Group versus individual approach
Improvements in sensitive parenting were larger if the intervention program was delivered in groups compared to individuals, and the overall effect was even larger if the intervention was delivered in groups with additional individual sessions. Foster and adoptive parents thus seem to benefit from other parents in comparable situations because they may serve as a source of social support. Working with an intervener on their individual situation is only effective if the group sessions are also part of the intervention program. Previous research shows that adoptive parents report less parenting stress if they experience more social support (Viana & Welsh, Reference Viana and Welsh2010), which may make them more receptive of parenting interventions. This effect was, however, only found for sensitive parenting and not for parenting stress in the current meta-analysis. Results show that parenting interventions delivered in groups, individuals, or a combination of both were equally effective in reducing parenting stress.
Number of sessions
Meta-regression analyses on number of sessions were inconsistent. For dysfunctional discipline and parenting stress, fewer sessions seem to generate stronger effects, whereas for sensitive parenting, a larger number of sessions seemed more beneficial. However, the range of number of sessions for interventions aimed at improving sensitive parenting was relatively small with a maximum of 12 sessions. According to the meta-analysis of Bakermans-Kranenburg et al. (Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003), intervention programs are most effective in increasing parental sensitivity and attachment security if the intervention consists of 16 or fewer sessions. Based on the current meta-analytic results, it is not possible to draw the same conclusion because studies examining the effectiveness of parenting intervention programs with more than 16 sessions were rare.
Child age
Finally, intervention programs were most effective for older children with regard to sensitive parenting, dysfunctional discipline (only for children up to 5 years old), and parenting stress. Thus, intervention programs are effective for both foster and adoptive parents of preschoolers and for foster and adoptive families with school-aged children or adolescents. Age seems to act as a confounding variable related to both child and parent outcomes. Of the 10 studies that included families with adolescents, only Benjamin (Reference Benjamin2010) included an adoption sample. Moreover, foster children are on average older than adopted children at time of placement and older children often show more severe behavior problems because the adverse period before placement was longer, which gives the negative experiences more time to influence the children's development (Helder, Mulder, & Gunnoe, Reference Helder, Mulder and Gunnoe2016; Leloux-Opmeer, Kuiper, Swaab, & Scholte, Reference Leloux-Opmeer, Kuiper, Swaab and Scholte2016; Tarren-Sweeney, Reference Tarren-Sweeney2008). The child behavior problems related to the adverse early life experiences may also influence parent outcomes such as sensitive parenting and parenting stress (Feldman et al., Reference Feldman, Weller, Zagoory-Sharon and Levine2007; Goemans et al., Reference Goemans, Van Geel and Vedder2018).
Child outcomes
Behavior problems
The meta-analyses for child outcomes showed that parenting interventions are only effective in decreasing child behavior problems. Thus, the implementation of parenting interventions in foster care and adoption samples reduces behavior problems in children. Moderator analyses showed no significant differences, with the exception of number of intervention sessions. Intervention programs with a higher number of sessions are most effective in decreasing behavior problems in foster and adoptive children.
Overall, the included studies of the current meta-analyses examined intervention programs specifically focusing on behavior, knowledge, attitudes, and stress in foster and/or adoptive parents. Any effects on child outcomes are thus indirect and may take some time to be revealed because they are dependent on the development and interaction of parent and child behaviors over time. The majority of the included studies had a relatively short interval of approximately 4 months between the pre- and postintervention measurements. Improvements in parenting behavior, knowledge and attitudes, and/or parenting stress may not have resulted in changes (yet) in child outcomes during these few months. Of the 19 studies with a follow-up measurement, only 1 study reported results on attachment security (Spieker et al., Reference Spieker, Oxford, Kelly, Nelson and Fleming2012; 6 months after the postintervention measurement), and no studies reported results on diurnal cortisol levels, which made it impossible to investigate the long-term follow-up effects of intervention programs on these constructs. This might explain why no significant overall effects of parenting interventions were found for attachment security and diurnal cortisol levels. However, the strongest overall effect was found for sensitive parenting, and previous research has suggested that increasing parents’ sensitive behavior may result in improvements in attachment security, stress regulation, and placement disruption of children (Bakermans-Kranenburg et al., Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003; Feldman et al., Reference Feldman, Weller, Zagoory-Sharon and Levine2007; Fisher et al., Reference Fisher, Stoolmiller, Gunnar and Burraston2007). Experiences with sensitive behavior of new caregivers may enable foster and adopted children to adjust their internal working model. In other words, sensitive parenting can help foster and adopted children adjust their expectations of how people around them will respond to them (Bakermans-Kranenburg et al., Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003; Schoemaker et al., Reference Schoemaker, Jagersma, Stoltenborgh, Maras, Vermeer, Juffer and Alink2018). Previous research additionally shows that children with sensitive parents experience less stress when this attachment figure is present during a negative experience (Dozier, Highley, Albus, & Nutter, Reference Dozier, Highley, Albus and Nutter2002) and that parenting interventions can reverse the dysregulation of the HPA axis by increasing sensitive parenting (Fisher et al., Reference Fisher, Gunnar, Dozier, Bruce and Pears2006). Parenting interventions can thus indirectly improve children's attachment security and stress regulation by changing their internal working models, but this may be a time-consuming process that seems to start by increasing parents’ sensitive behavior.
Attachment security
Results showed that parenting interventions are not effective in improving attachment security. Because of the indirect effects of parenting interventions on child outcomes, the overall effect sizes were expected to be smaller and a larger set of studies reporting on child outcomes was thus needed to find significant overall effects. Compared to 33 studies reporting results on child behavior problems, which yielded a significant meta-analytic intervention effect, only 6 studies reported results on attachment security of foster and/or adopted children. A previous meta-analysis of 29 studies did show that attachment security could be improved by increasing sensitive parenting with parenting interventions (Bakermans-Kranenburg et al., Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003). However, this previous meta-analysis did not specifically focus on foster care or adoption populations, and if more intervention studies were available for foster care and/or adoption samples, a significant overall effect of parenting interventions on attachment security may emerge. In addition, of the 6 studies included in the current meta-analysis on attachment security, only Juffer et al. (Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005) used the Strange Situation Procedure (Ainsworth et al., Reference Ainsworth, Blehar, Waters and Wall1978), which enables coding of attachment disorganization, which is more prevalent among foster and adopted children compared to children living with and being raised by their biological parents (Van den Dries et al., Reference Van den Dries, Juffer, van IJzendoorn and Bakermans-Kranenburg2009; Vasileva & Petermann, Reference Vasileva and Petermann2018). The four other studies used the Attachment Q-Sort (Baker et al., Reference Baker, Biringen, Meyer-Parsons and Schneider2015; Spieker et al., Reference Spieker, Oxford, Kelly, Nelson and Fleming2012) or the Parent Attachment Diary (Dozier et al., Reference Dozier, Lindhiem, Lewis, Bick, Bernard and Peloso2009; Fisher & Kim, Reference Fisher and Kim2007), which do not measure disorganized attachment. It was not possible to examine the moderating effect of the type of measurement (observation vs. questionnaire) because the subset of studies using an observational instrument was too small. The effectiveness of parenting interventions on attachment disorganization could also not be examined because only Juffer et al. (Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005) reported results on attachment disorganization. This study showed that a video-feedback intervention focused on increasing sensitive parenting of adoptive parents was effective in decreasing attachment disorganization. Future intervention studies for foster and adoptive families focusing on attachment should also report effects for attachment disorganization, not only because foster and/or adopted children are at higher risk of developing an insecure disorganized attachment (Van den Dries et al., Reference Van den Dries, Juffer, van IJzendoorn and Bakermans-Kranenburg2009), but also because an insecure disorganized attachment puts these children at an additional risk of developing behavior problems and psychopathology (Fearon et al., Reference Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley and Roisman2010; Groh et al., Reference Groh, Roisman, van IJzendoorn, Bakermans-Kranenburg and Fearon2012; Sroufe et al., Reference Sroufe, Egeland, Carlson, Collins, Grossman, Grossman and Waters2005; van IJzendoorn et al., Reference van IJzendoorn, Schuengel and Bakermans-Kranenburg1999).
Diurnal cortisol levels
The meta-analysis on diurnal cortisol levels of foster and/or adopted children also showed no significant overall effect. Because only three studies reported data on the effectiveness of parenting interventions on child diurnal cortisol levels, the total sample size was relatively small and categorical moderator analyses could not be performed. Of the three studies included in this meta-analysis, the study by Jonkman et al. (Reference Jonkman, Schuengel, Oosterman, Lindeboom, Boer and Lindauer2017) differed from the Dozier et al. (Reference Dozier, Peloso, Lindhiem, Gordon, Manni, Sepulveda and Levine2006) and Van Andel et al. (Reference Van Andel, Post, Jansen, Van der Gaag, Knorth and Grietens2016) studies in a number of ways. First, Jonkman et al. (Reference Jonkman, Schuengel, Oosterman, Lindeboom, Boer and Lindauer2017) was the only study that included a sample of foster children who displayed high levels of behavior problems. Second, it was the only study with a quasi-experimental design that included a nonrandom control group. Third, the intervention program investigated by Jonkman et al. (Reference Jonkman, Schuengel, Oosterman, Lindeboom, Boer and Lindauer2017) was the only one not including a video-feedback component and the only intervention program that also worked with groups of foster parents at a community center instead of only with individual parents at home. Because categorical moderator analyses were not possible, it is unclear which sample, study design, and/or intervention characteristics were associated with possible intervention effects. It is therefore important that more studies investigate the effectiveness of parenting interventions on foster and/or adopted children's stress regulation because intervention programs may help children overcome the chronic stress they often experienced early in life and to reverse the dysregulation of the stress system in order to have the children respond adequately to stressful and arousing events (Koss & Gunnar, Reference Koss and Gunnar2018).
Placement disruption
The meta-analysis on placement disruption also did not show a significant overall intervention effect. It may take more time to observe a decrease in placement disruption because parenting interventions are more likely to first improve parent outcomes (e.g., parenting behavior), which subsequently may improve child outcomes (e.g., behavior problems), and finally, reduce placement disruptions. Previous meta-analytic evidence has shown that the risk of placement disruptions is higher if foster or adopted children display behavior problems and that if the relationship between foster or adopted children and their new parents is good (e.g., a secure attachment relationship due to sensitive parenting), the likelihood of placement disruption is small (Oosterman et al., Reference Oosterman, Schuengel, Slot, Bullens and Doreleijers2007).
The effect of parenting interventions on placement disruption would thus be indirect and the overall effect size was (as with the child outcomes) expected to be smaller. A larger set of studies with longer follow-up periods may have resulted in a significant overall intervention effect for placement disruption. The majority of the studies included in the current meta-analysis reported data on placement disruption during the postintervention measurement approximately 6 months after baseline. Only Bondy (Reference Bondy1997) measured placement disruption at a 1-year follow-up measurement, and thus it was not possible to examine the moderating effect of time of measurement. In addition, only Price et al. (Reference Price, Chamberlain, Landsverk, Reid, Leve and Laurent2008), Van Holen, Vanschoonlandt, and Vanderfaeillie (Reference Van Holen, Vanschoonlandt and Vanderfaeillie2017) and Wassall (Reference Wassall2011) reported some information about placement duration at baseline. This information suggested that the variation in placement duration is large, but the possible moderating role of placement duration could not be examined. Moreover, longitudinal effectiveness studies of parenting interventions on placement disruption are needed, because (foster care) research shows that the first 18 months after placement may be critical for placement disruption (Vanderfaeillie, Goemans, Damen, Van Holen, & Pijnenburg, Reference Vanderfaeillie, Goemans, Damen, Van Holen and Pijnenburg2017). The existing intervention studies often were too short or provided incomplete data on placement duration to draw conclusions about the effects on placement disruption.
Limitations
Intervention studies are often heterogeneous, which makes it difficult to compare and combine the effects of the different studies in meta-analyses (Dickes et al., Reference Dickes, Kemmis-Riggs and McAloon2018). I 2 values were mediocre to high for most of the conducted meta-analyses, indicating that the variation in a set of individual effect sizes was large. This large variation between studies may influence the reliability of the overall effect sizes for sensitive parenting, dysfunctional discipline, parenting knowledge and attitudes, and child behavior problems. Moderator analyses were used to examine the variation. The overall effects of parenting interventions on these parent and child outcomes may not be generalizable. Moderator analyses are crucial to control for the heterogeneity between studies, but in the current meta-analytic review, performing moderator analysis was not always possible because the subset of studies was too small, or the required information was not reported frequently enough or not at all. As a result, it was not possible to perform moderator analyses to compare kinship and non-kinship foster care, domestic and international adoptions, and to examine the moderating effect of placement duration. In addition, moderator analyses that examine differences in the treatment of the control group (i.e., care as usual, waitlist, dummy intervention, or regular foster care) were not possible because it was not always clear what the different treatments entailed. Specifically, care as usual may not only differ between foster care and adoption but also between countries. In the United States and the United Kingdom it is common that foster children are adopted from foster care, whereas the Dutch foster care policy primarily aims for reunification of children with their biological parents and adoptions from foster care are rare (Goemans, Vanderfaeillie, Damen, Pijnenburg, & Van Holen, Reference Goemans, Vanderfaeillie, Damen, Pijnenburg and Van Holen2016; Wulczyn, Reference Wulczyn2004). Differences in control group treatment may (partly) explain the heterogeneity between studies.
If an out-of-home placement is needed, it is often preferred to place children with kin (Ehrle & Geen, Reference Ehrle and Geen2002; Winokur, Holtan, & Batchelder, Reference Winokur, Holtan and Batchelder2018). Research suggests that foster children in kinship and non-kinship care do not differ in terms of gender, age at placement, and reasons for out-of-home placement, but foster children in kinship foster care show fewer behavior problems, psychopathology, and have a lower risk of placement disruption than children in non-kinship care (Winokur et al., Reference Winokur, Holtan and Batchelder2018). Non-kinship foster families may thus benefit more from parenting interventions than kinship foster families. However, kinship foster parents are on average older, poorer, and less well educated. They also have less contact with their assigned family social worker and receive less support and services (Ehrle & Geen, Reference Ehrle and Geen2002; Farmer, Reference Farmer2009). These factors may imply that kinship foster parents would benefit more from interventions than non-kinship foster parents. More research is needed to meta-analytically test differences between kinship and non-kinship foster parents.
The effectiveness of parenting interventions for domestic and international adoptions could also not be compared, but could be relevant because domestic adoptees show more behavior and mental health problems than international adoptees (Juffer & van IJzendoorn, Reference Juffer and van IJzendoorn2005). This does not necessarily mean that parents of international adoptees are not in need of or will not benefit from parenting interventions, because international adoptees still show more behavior and mental health problems than non-adopted children (Juffer & van IJzendoorn, Reference Juffer and van IJzendoorn2005).
It was not possible to perform meta-regression analyses for placement duration because this information was not provided by the majority of the individual studies. Nevertheless, it can be argued that the longer the placement (in the same family), the better foster and/or adoptive parents and children are attuned to each other. The likelihood that foster and adoptive families already received extra support, for example, a parenting intervention to improve parenting skills, is also greater when the duration of the placement is longer. As stated before, there is evidence that the risk of placement disruption is smaller when caregiving quality is good and when the placement lasts longer (Oosterman et al., Reference Oosterman, Schuengel, Slot, Bullens and Doreleijers2007; Vanderfaeillie et al., Reference Vanderfaeillie, Goemans, Damen, Van Holen and Pijnenburg2017). In addition, if the duration of the placement is longer, it is more likely that the children where younger at time of placement. Previous research shows that younger children experience fewer mental health problems and they and their families are consequently in less need of extra support such as parenting interventions (Tarren-Sweeney, Reference Tarren-Sweeney2008).
Finally, the aim of the current study was to test the effectiveness of intervention programs for foster and adoptive parents on several parent and child outcomes, and placement disruption. In line with the meta-analysis of Bakermans-Kranenburg et al. (Reference Bakermans-Kranenburg, van IJzendoorn and Juffer2003), we additionally investigated the moderating effect of video feedback by comparing video-feedback interventions with interventions without a video-feedback component. Future research is needed to examine which specific program elements (other than video-feedback vs. no video-feedback component) are effective in improving parent and child outcomes, and placement disruption in participants with specific characteristics (e.g., families with children who display high levels of behavior problems), for example, with the distillation and matching model (Chorpita, Daleiden, & Weisz, Reference Chorpita, Daleiden and Weisz2005) or the common components analysis (Morgan, Davis, Richardson, & Perkins, Reference Morgan, Davis, Richardson and Perkins2018). Knowledge about the effectiveness of specific intervention program elements is valuable for the implementation and use of parenting interventions in clinical practice.
Conclusion
Foster care and adoptive placements can be challenging for both parents and children. Children with adverse early life experiences may be less likely to form a secure attachment relationship with their new caregivers, which can increase the risk of the development and persistence of behavior problems and stress dysregulation. Taking care of foster and adopted children is in turn often very stressful for foster and adoptive parents because of the children's previous adverse experiences and their behavior problems. Many foster and adoptive families need help and support to overcome these challenges. The results of the current meta-analytic review showed that parenting interventions are effective in increasing sensitive parenting and parenting knowledge and positive attitudes, and in decreasing dysfunctional discipline and parenting stress. The subset of effect sizes for sensitive parenting yielded strong evidence for the effectiveness of intervention programs. The evidence base for the effectiveness of intervention programs aimed at improving dysfunctional discipline, parenting knowledge, and parenting stress was not so strong and may therefore benefit from more studies examining the effectiveness of (newly developed) parenting interventions in foster care and adoption populations. In addition, an indirect effect on child behavior problems was found: children of foster and adoptive parents attending a parenting intervention program showed greater reductions in behavior problems than children whose parents did not receive an intervention. No significant overall effects were found for children's attachment security and diurnal cortisol levels. However, because any effect on child outcomes would be indirect, it may take more time to observe significant changes in children's attachment security and diurnal cortisol levels. Longitudinal effectiveness studies are thus needed to examine the long-term effects of intervention programs especially on child outcomes. Future studies should also report results of subgroups within the foster care and adoption populations; the effectiveness of parenting interventions for kinship versus non-kinship foster care and domestic versus international adoption is still unclear. For professionals working in the field of foster care and adoption, it is also important to know which specific program elements are effective in improving parent and child outcomes, and placement disruption in families with specific characteristics (e.g., families with children who display high levels of behavior problems). Future research is needed to examine the effectiveness of program elements in more depth. Knowledge from these future studies may lead to the development of intervention programs that are specifically designed to use in foster care and adoption populations. Results of the current series of meta-analyses, showing that parenting interventions can effectively help foster and adoptive families in the important areas of sensitive parenting, dysfunctional discipline, parenting knowledge and attitudes, parenting stress, and child behavior problems, lay an important basis for these future directions.
Acknowledgments
The authors would like to thank Chantal van Elswijk, Lisette Herrebout, and Lynn van Schie for their help with screening and coding the records.
Financial Support
Nikita Schoemaker is supported by Stichting Kinderpostzegels Nederland. The Netherlands Organization for Scientific Research supported Lenneke Alink (VIDI Grant 016.145.360) and Femmie Juffer (Meerwaarde Grant 475-11-002).















 Open access
Open access