



Dietary habits have changed in recent decades. One of the most important changes is the increase in the ultra-processed foods (UPF) consumption around the world(1–Reference Monteiro, Moubarac and Cannon5). UPF are industrial formulations made from substances derived from food or synthesised in laboratories (dyes, flavourings and other additives) usually containing little or no whole food(Reference Monteiro, Cannon and Levy6). These are characterised by being food products with a low nutritional quality(Reference Moubarac, Batal and Louzada7–Reference Parra, da Costa-Louzada and Moubarac12). It has been estimated that UPF intake is currently increasing, contributing from values below 20 % to above 60 % of total energy intake depending on the country and age range(Reference Elizabeth, Machado and Zinöcker13,Reference Kelly and Jacoby14) . Available evidence suggests that it is the high availability, low cost and extensive marketing of ready-to-consume food items that result in an excessive intake(Reference Swinburn, Sacks and Hall15). These changes in dietary habits have been paralleled to an increase in non-communicable diseases (NCD)(Reference Mendis, Davis and Norrving16). The low nutritional content of these foods, coupled with excessive consumption patterns, is known to lead to these chronic NCD(Reference Canella, Levy and Martins17,Reference Tavares, Fonseca and Garcia Rosa18) .
As the global incidence of NCD continues to grow, it is crucial to study the impact of UPF in health. The WHO has, therefore, developed the European Action Plans for Food and Nutrition Policy with the aim of improving upon existing national policies. Specifically, they have developed a Global Action Plan on NCD(19,20) to achieve a reduction in global mortality from the four major NCD (CVD, cancer, chronic respiratory disease and diabetes) by 2025. Global modelling of the impact of risk factors on mortality, such as UPF, could provide important information to achieve goals like this. The beneficial effects of fresh or minimally processed foods consumption on mortality are known(Reference Wang, Ouyang and Liu21), but few studies have examined the harmful effects of consumption of UPF. NutriNet-Santé cohort in France(Reference Schnabel, Kesse-Guyot and Allès22), the National Health and Nutrition Examination Survey (NHANES) cohort in the USA(Reference Kim, Hu and Rebholz23) and the Moli-Sani study in Italy(Reference Bonaccio, Di Castelnuovo and Costanzo24) found a positive association between consumption of UPF and all-cause mortality. SUN cohort(Reference Rico-Campà, Martínez-González and Alvarez-Alvarez25) and a cohort selected from the ENRICA study(Reference Blanco-Rojo, Sandoval-Insausti and López-Garcia26) in Spain also report similar findings, but participants were highly selected (only university graduates) and had a relatively short follow-up period ( approximately 8 years), respectively.
This study, carried out on a representative sample of the Spanish population after 27 years of follow-up, aimed to determine the association of UPF consumption with all-cause mortality.
Methods
Design and study population
The multicentre study Diet and Risk of Cardiovascular Diseases (CVD) in Spain (DRECE) was used as a substrate for analysis. DRECE was designed in 1991 to know the real situation of the Spanish population upon the risk of developing CVD, based on the prevalence of risk factors and their relationship with dietary habits. The details of the study (background, study population and methods of the survey) are reported elsewhere(Reference Gómez Gerique, Herrera and Gómez de la Cámara27,Reference Gómez Gerique, Rubio Herrera and Gómez de la Cámara28) . Briefly, a cohort of 4787 people between 5 and 59 years of age was included, stratified by sex and age, randomly selected throughout the national territory, both rural and urban. At baseline, in 1991, a FFQ was carried out, designed and validated for epidemiological studies in the Spanish population(Reference Martin-Moreno, Boyle and Gorgojo29,Reference Rodríguez, Ballart and Pastor30) .
Dietary assessment and classification of ultra-processed food
The estimation of UPF consumption was carried out through the data collected in the FFQ. The first step was to classify all foods into four groups according to the NOVA classification, developed in Brazil and used internationally in research(Reference Monteiro, Cannon and Levy31). These four groups were: Group 1 describes unprocessed/minimally processed foods; Group 2 comprises processed culinary ingredients; Group 3 includes processed products and Group 4 collects all UPF. The full list of the recorded foods in the FFQ and their NOVA classification is shown in Supplemental Table 1. Subsequently, the kcal/d consumed from each of the four NOVA groups and the percentage they represented with respect to the total intake were determined for better interpretation. As some foods do not provide energy, the calculation was also considered in relation to the weight of the product and not only to the energy intake(Reference Schnabel, Kesse-Guyot and Allès22). As grams can be easily interpreted and measured, they were determined as an absolute value (g/d). Responses with extreme total energy intakes (<200 kcal and >5000 kcal) were excluded from the analysis. The consumption of the different nutrients in the diet (carbohydrates, proteins, fats and fibre) was also calculated (in g/d). All the information for the calculation of these data was obtained from the Spanish Food Composition Database (BEDCA)(32).
Mortality ascertainment
Mortality in this cohort was monitored from 1991 to December 2017 through an annual agreement with the National Institute of Statistics (INE). The vital status and cause of mortality were provided by the INE, according to the registered death certificates. In this way, all-cause mortality was obtained.
Statistical analysis
All statistical analyses were performed using SAS© software, Version 9.4 of the SAS System for Windows. Descriptive data were presented as mean and standard deviation for continuous variables and categorical variables were expressed as absolute or relative frequencies.
Correlations between nutritional characteristics (carbohydrates, proteins, fats and fibre), age and UPF consumption were analysed using Pearson’s correlation coefficient (ρ).
To assess the association between all-cause mortality and UPF consumption at baseline, Cox regression models were fitted with the time variable covering from baseline in 1991 to the date of death (provided by the INE) or to the end of follow-up on 31 December 2017, whichever occurred first. Hazard ratios were estimated along with Wald’s 95 % CI. The models were adjusted for potential confounders defined a priori. Potential confounders were identified based on previous existing literature rather than on statistical criteria(Reference Hernán, Hernández-Díaz and Werler33). The following potential confounders were included as covariates in the multivariate models: age; sex; baseline BMI (continuous); total energy intake (kcal/d, continuous); alcohol consumption (servings/d, continuous); smoking status (yes/no); physical activity (yes/no); family history of CVD (yes/no); history of diabetes, hypertension or CVD at baseline (yes/no).
Cox models were built with three successive levels of additional adjustments for potential confounders: model 1 was adjusted for age and sex; model 2 was additionally adjusted for lifestyle and model 3 was additionally adjusted for clinical factors (history of chronic conditions). The likelihood of the three models was compared using the Akaike information criterion. This criterion penalises the likelihood of the model, and the one with the lowest value is the most likely model. Also, Harrell’s C index was used to evaluate the performance of the models. The proportionality of hazards was verified with the Schoenfeld residuals test. In addition, smoothing by penalised splines was used to calculate the possible non-linear association between UPF consumption and all-cause mortality. All analyses were carried out using UPF consumption measured as percentage of total energy intake and g/d. Additionally, we performed subgroup analyses separated by sex in model 3.
Sensitivity analyses were also performed by rerunning the best model (model 3) under five different a priori assumptions: (1) excluding participants with prevalent diabetes at baseline; (2) excluding participants with prevalent hypertension at baseline; (3) excluding participants aged less than 18 years; (4) excluding the first 2 years of follow-up for all participants to reduce the possibility of attribution of deaths to health conditions at baseline and (5) excluding deaths from cancer, deaths from CVD and deaths from injuries.
Isoenergetic substitution models were constructed with the aim of comparing the effects of substituting UPF by different NOVA groups (either processed foods and processed culinary ingredients or unprocessed or minimally processed foods) in vital status(Reference Willett34). In these models, the total energy intake, the percentages of energy or grams derived from processed foods and processed culinary ingredients or unprocessed/minimally processed foods, as appropriate, were simultaneously included, in addition to the confounding variables studied in model 3. The coefficients obtained in these models can be interpreted as the estimated effect of substituting a certain percentage of energy or absolute values of grams from UPF with the equivalent processed foods or unprocessed or minimally processed foods, while holding constant the intake of total energy and the energy or grams from the corresponding non-replaced NOVA group.
Results
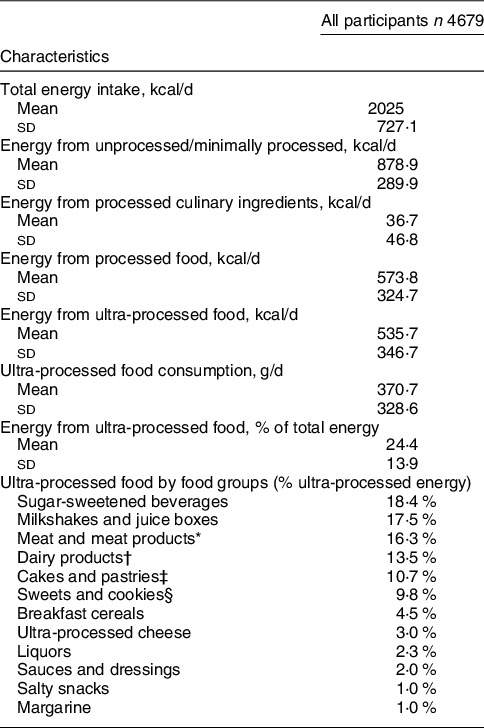
Of the 4787 study participants, 108 were excluded due to inconsistent dietary data (total daily energy intake outside the range of 200–5000 kcal/d). The final sample size was 4679. A total of 2288 (48·9 %) males and 2391 (51·1 %) females were included in this analysis. Mean age at baseline was 30·5 (sd 15·6) years. Table 1 shows the baseline characteristics of participants. After a median of 27 years and 122 134 person-years followed up, 450 deaths due to any cause occurred. An average consumption of UPF of 370·8 g/d was found, corresponding to 24·4 % of the total energy intake (Fig. 1). A total of 1·9 % of the sample did not consumed any UPF on a daily basis.
Table 1 Baseline characteristics of the cohort participants


Fig. 1 UPF consumption in Spain according to the NOVA classification. Error bars denote standard error of the mean. UPF, ultra-processed food
The main food groups contributing to the intake of UPF were sugar-sweetened beverages (i.e. soft drinks) (18·4 %), milkshakes and juice boxes (17·5 %), meat and meat products (16·3 %), dairy products (13·5 %), cakes and pastries (10·7 %) and sweets and cookies (9·8 %) (Table 2). Participants who consumed the highest amount of UPF had significantly higher intakes of total energy (ρ = 0·40, P-value <0·0001), carbohydrates (ρ = 0·34, P-value <0·0001), total fat (ρ = 0·30, P-value <0·0001), saturated fat (ρ = 0·39, P-value <0·0001), and dietary cholesterol (ρ = 0·27, P-value <0·001), and lower protein (ρ = -0·13, P-value <0·0001) and fibre (ρ = -0·06, P-value <0·0001) intake. In addition, the individuals who consumed more UPF were younger (ρ = -0·53, P-value <0·0001).
Table 2 Relative contribution of the dietary intake of food groups to UPF (NOVA group 4)
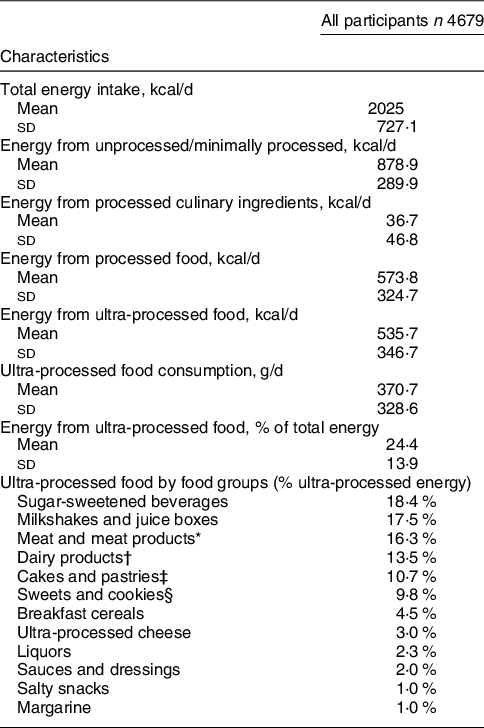
* Includes ham, cold cuts, sausages and hamburgers.
† Includes yogurts and fermented milk, ice cream, and petit suisse.
‡ Includes doughnuts, muffins or other non-hand-made pastries.
§ Includes biscuits, chocolate cookies, candies and chocolates.
In all the models, the participants who consumed the highest amount of UPF had a higher risk of mortality. When covariates were added to the models, the association did not change substantially. Model 3 was the one with the best Harrell’s C index and the lowest Akaike information criterion. In model 3, every 10 % absolute increment of the energy intake from UPF had a relatively 15 % higher hazard of all-cause mortality (multivariable-adjusted hazard ratio 1·15; (95 % CI 1·03, 1·27); P-value = 0·012) (Table 3). The corresponding mortality risk when UPF consumption was expressed in g/d was (1·04 (95 % CI 1·01, 1·10); P-value = 0·018; see online Supplemental Table 2).
Table 3 Cox proportional hazard ratios (Wald’s 95 % CI) for all-cause mortality according to ultra-processed food consumption (measured as % of total energy intake) in the DRECE study
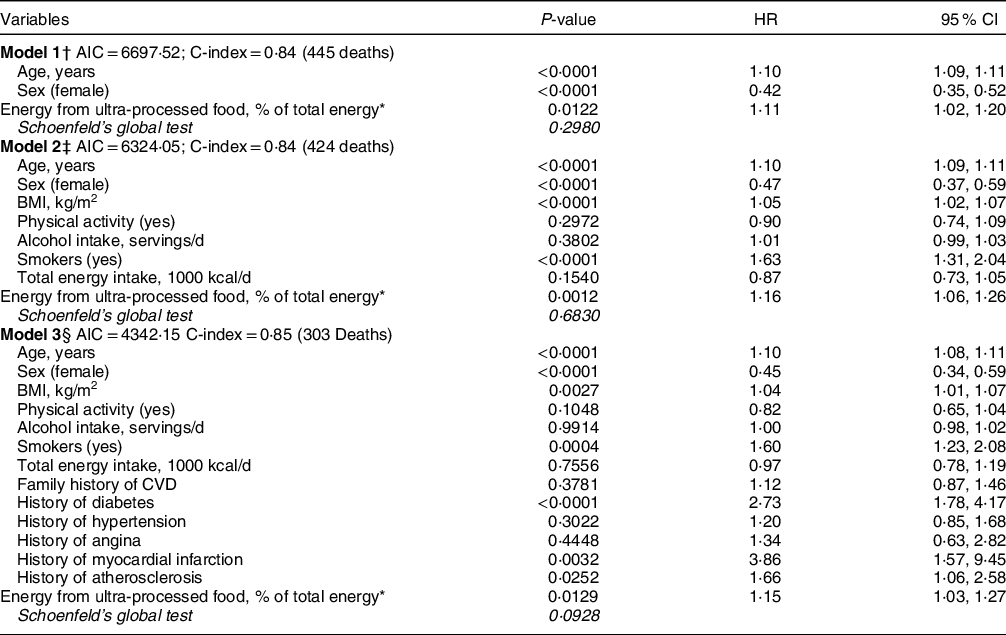
AIC, Akaike information criterion.
The names of the different models constructed are shown in bold. The Schoenfeld’s global test for each model is shown in italic.
* Calculated for every 10 %.
† Model 1 was adjusted for age and sex.
‡ Model 2 was adjusted for the variables in model 1 plus BMI, physical activity, alcohol intake, smoking status and total energy intake.
§ Model 3 was adjusted for the variables in model 2 plus family history of CVD, history of diabetes, hypertension, angina, myocardial infarction and atherosclerosis.
The proportionality of hazards was verified with a test based on Schoenfeld residuals; the non-significant result (P-value >0·05) suggested that there was no evidence against the proportionality assumption in all models (corresponding P-values in Table 3 and see online Supplemental Table 2). The linearity assumptions between UPF consumption and all-cause mortality were confirmed by the restricted cubic spline (model 3 non-linear association in percentage P-value = 0·470; in g/d P-value = 0·101).
Sensitivity analyses were performed by repeating the multivariable-adjusted Cox regression model 3 under different scenarios. All point estimates showed a direct association between consumption of UPF and higher mortality. Results did not substantially change in any of these alternative scenarios, suggesting that the direct association between consumption of UPF and mortality was robust (Fig. 2(a) and (b)). When UPF consumption was measured as percentage of total energy intake (Fig. 2(a)), the association when excluding cases of prevalent hypertension at baseline was non-significant. In contrast, the association became stronger after excluding deaths from cancer, CVD and injuries. The association remained significant after excluding cases of prevalent diabetes at baseline, excluding participants aged <18 years and excluding the first 2 years of follow-up. When UPF consumption was measured as g/d (Fig. 2(b)), some associations were no longer significant, in particular under the scenarios of excluding participants aged less than 18 years, excluding the first 2 years of follow-up and after excluding deaths from CVD and injuries. The association became slightly higher after excluding cases of prevalent hypertension and diabetes at baseline and after excluding deaths from cancer. Subgroup analysis was performed in model 3. According to Supplemental Fig. 1, the association between UPF energy contribution and all-cause mortality was stronger and only significant among males. On the other hand, associations between UPF gram intake and all-cause mortality in males and females were non-significant, probably due to lack of statistical power. The interaction between sex and UPF consumption was non-significant for both energy and gram consumption (P-value = 0·054 and P-value = 0·511, respectively).

Fig. 2 Sensitivity analyses for association between consumption of ultra-processed foods and all-cause mortality performed in model 3. a) Cox proportional hazard ratios (Wald’s 95% CI) for all-cause mortality of UPF consumption measured as percentage of total energy intake and b) Cox proportional hazard ratios (Wald’s 95% CI) for all-cause mortality of UPF consumption measured as grams/day. UPF, ultra-processed food
After performing the isoenergetic substitution in model 3, the hazard ratio when UPF were substituted by processed foods was less than 1 but did not achieve statistical significance (neither in percentage of energy nor in grams). However, when UPF were replaced by unprocessed or minimally processed foods, an inverse pattern was observed. A reduction of 14 % (in percentage of energy) and 6 % (in g) in all-cause mortality was estimated (P-value = 0·018 and P-value = 0·002, respectively) (see Table 4).
Table 4 Isoenergetic substitution. Hazard ratios derived from Cox multiple regression model 3 in which processed foods or unprocessed/minimally processed foods replaced UPF

UPF, ultra-processed food.
Discussion
In this longitudinal cohort study of a representative Spanish population, a significant association between higher consumption of UPF and an increased risk of all-cause mortality over a median follow-up of 27 years was found. This association remained significant after adjusting for socio-demographic factors, lifestyle and clinical factors.
The average consumption of UPF in Spain was 24·4 % of the total energy intake. These data are in line with those provided by the ENRICA cohort study(Reference Blanco-Rojo, Sandoval-Insausti and López-Garcia26). Spain is a country with low UPF consumption when compared with other countries, such as Canada (48 %)(Reference Moubarac, Batal and Louzada7), the USA (57·9 %)(Reference Martínez Steele, Baraldi and Louzada35), the UK (56·8 %)(Reference Rauber, da Costa Louzada and Steele10), Belgium (about 30 %)(Reference Vandevijvere, De Ridder and Fiolet36), France (35·9 %)(Reference Julia, Martinez and Allès37) and even in developing countries like Brazil (21·5 %)(Reference Costa Louzada, Martins and Canella38). One of the possible causes for these differences may be the period of time in which these data were collected; our data are based on the diet assessed in 1991, where there was probably a lower intake of UPF. This also could be due to the Mediterranean diet, which is characterised by a high consumption of plant-based foods, a low consumption of red meat and other processed foods, the use of olive oil as the main source of fat, and a moderate intake of wine during meals(Reference Willett, Sacks and Trichopoulou39). In addition, the Mediterranean diet is mainly based on cooking at home, so the consumption of ready-to consume UPF is smaller compared to other countries. However, it is also known that in recent decades. the Spanish population has been moving away from this traditional diet pattern to adopt a less healthy diet(Reference León-Muñoz, Guallar-Castillón and Graciani40), especially the younger population(Reference García-Meseguer, Burriel and García41). These dietary changes support estimates that the consumption of UPF will continue to increase as will their sales in Spain(Reference Kelly and Jacoby14,Reference Latasa, Louzada and Martinez Steele42) .
The present study builds on previous longitudinal studies that examined the association between consumption of UPF (using the NOVA classification) and NCD. These studies found associations between UPF consumption and different adverse health outcomes such as obesity, dyslipidemia, hypertension and cancer at mid-life (≥40 years)(Reference Rauber, Campagnolo and Hoffman43–Reference Fiolet, Srour and Sellem46). Our results appear to be consistent with those studies and reflect the adverse effects associated with UPF consumption.
There are also other studies under the NOVA framework that evaluate the association between UPF intake and all-cause mortality, such as the NutriNet-Santé (≥45 years) in France(Reference Schnabel, Kesse-Guyot and Allès22), the US National Health and Nutrition Examination Survey (NHANES)(Reference Kim, Hu and Rebholz23), Moli-sani study in Italy(Reference Bonaccio, Di Castelnuovo and Costanzo24), SUN cohort(Reference Rico-Campà, Martínez-González and Alvarez-Alvarez25) and a cohort selected from the ENRICA study(Reference Blanco-Rojo, Sandoval-Insausti and López-Garcia26) in Spain. NHANES, Moli-sani, SUN and ENRICA cohort(Reference Kim, Hu and Rebholz23–Reference Blanco-Rojo, Sandoval-Insausti and López-Garcia26) categorise the consumption of UPF into quartiles and study the risk associated with the fourth quartile v. the first quartile. Based on the existing literature(Reference Altman47,Reference Cumsille and Bangdiwala48) , we consider that in epidemiological studies in which it is intended to evaluate the effect of an exposure on a response, the magnitude or direction of such effect may be biased as a consequence of the categorisation of the variable. To avoid possible biases or loss of information, we decided not to categorise the variable and use it as continuous. In this sense, these previous studies report a much higher effect of UPF on all-cause mortality than our study. However, they only take into account the first and fourth quartiles of consumption adjusted for different covariates (NHANES: HR = 1·30; (95 % CI 1·08, 1·57); P-value = 0·001); (Moli-sani: HR = 1·26; (95 % CI 1·09, 1·46); P-value <0·050); (SUN: HR = 1·62; (95 % CI 1·13, 2·33); P-value = 0·005) and (ENRICA: HR = 1·44; (95 % CI 1·01, 2·07); P-value = 0·030). The information provided by the second and third quartiles is not reflected in these results. Specifically, the SUN cohort is the one that finds a greater effect of the UPF on all-cause mortality, a 62 % relatively higher hazard of mortality. This may be due to the fact that the SUN cohort is a relatively young population of university graduates, and it is known that young people have a less healthy diet(Reference García-Meseguer, Burriel and García41). As these participants were non-representative of the population, these results cannot be extrapolated to the general Spanish population. NutriNet-Santé Cohort(Reference Schnabel, Kesse-Guyot and Allès22) in France studies the consumption of UPF as a continuous variable, and their reports are very similar to ours, and the HR per 10 % increment of UPF consumed was (1·14 (95 % CI 1·04, 1·27); P-value = 0·008). However, the population of this study is older than 45 years, which reduces the generalisability of their results. Similar results in different populations, with several methods for assessing dietary exposures and different age ranges, support a robust association. Moreover, the results obtained from isoenergetic replacement are in line with different studies that estimated through national household data the contribution of dietary trends to the risk of CVD mortality. In the UK, if the consumption of processed and ultra-processed products were reduced to the levels of unprocessed and minimally processed foods, there could be a substantial 10–13 % decrease in cardiovascular deaths from CVD(Reference Moreira, Baraldi and Moubarac49). In Brazil, with a similar approach, assuming a 50 % reduction in UPF, replacing this reduction in consumption with a 50 % increase in the consumption of unprocessed or minimally processed foods, plus an additional reduction of 50 % in processed culinary ingredients, an 11 % reduction in cardiovascular mortality was estimated(Reference Moreira, Hyseni and Moubarac50). As far as we know, no previous studies have performed the isoenergetic substitution of UPF for all-cause mortality. Although the studies published so far provide results for CVD deaths, they support the results we found for all-cause mortality.
The increased risk of all-cause mortality associated with consumption of UPF depends on several factors. UPF cause overconsumption due to the high energy density they provide which is less satiating. This inadvertent overconsumption has been associated with mortality(Reference Nagai, Ohkubo and Miura51). Several of these UPF contain high amounts of salt, and high Na intake has been associated with mortality and cardiovascular deaths(Reference Mozaffarian, Fahimi and Singh52,Reference Graudal, Jürgens and Baslund53) . Likewise, UPF provide added sugars(Reference Martínez Steele, Baraldi and Louzada35), which contributes to the excessive consumption of added sugars that has been associated with increased CVD mortality(Reference Yang, Zhang and Gregg54). Processed meats and sugar-sweetened beverages have been consistently linked to mortality in prospective studies(Reference Abete, Romaguera and Vieira55–Reference Wang, Lin and Ouyang58) and may therefore be important factors in the association found between UPF and mortality. In contrast, UPF tend to be low in fibre and dietary fibre has been associated with a lower risk of mortality(Reference Yang, Zhao and Wu59,Reference Veronese, Solmi and Caruso60) . UPF are characterised by being food products of low nutritional quality and their high consumption is associated with unhealthy dietary patterns(Reference Moubarac, Batal and Louzada7,Reference Luiten, Steenhuis and Eyles61,Reference Poti, Mendez and Ng62) . Such unhealthy patterns could lead to develop NCD, contributing to an increased risk of mortality(Reference Micha, Peñalvo and Cudhea63,Reference Murray, Atkinson and Bhalla64) . Finally, UPF often contain additives in their composition (such as titanium dioxide, artificial sweeteners, emulsifiers,etc), and several studies have raised concerns about the health consequences of those additives(65,Reference Chang, Zhang and Tang66) . Other studies have found associations between the consumption of UPF and urinary concentrations of phthalates and bisphenol(Reference Martínez Steele, Khandpur and da Costa Louzada67). These chemicals are present in food packaging and have been associated with harmful health effects. However, more research is needed to know how and to which extent UPF could affect health(Reference Zota, Phillips and Mitro68–Reference Varshavsky, Morello-Frosch and Woodruff70).
All these findings reinforce the detrimental effects of UPF. Consistent with the evidence cited, our findings support the negative impact of UPF on the overall incidence of NCD and all-cause mortality in Spain; they also highlight the importance of implementing new nutritional policies and guidelines as soon as possible to address this impact in the population.
Strengths and limitations of this study
The strengths of this study are its prospective design, long follow-up and the large sample size, representative of Spanish population, which broadens the generalisation of the results and also the use of validated methods and the adjustment for a wide range of potential confounders in the analysis. The most important novelty is that we did not categorise the consumption of UPF and use as a continuous variable, which provides richer information and avoids biases. As well, to avoid underestimating the consumption of UPF (since some foods do not provide energy), all the analyses were considered in relation to the weight of the product and not only to the energy contribution. Lastly, the performances of several sensitivity analyses support the robustness of the results.
However, the study also has some limitations. First, dietary information was collected only at baseline, assuming no changes over time in dietary intake. Furthermore, the dietary data were collected in 1991, a time frame that was likely characterised by less UPF intake, which probably underestimates the true impact of UPF consumption on mortality nowadays. Second, although the NOVA classification has been sometimes questioned(Reference Gibney, Forde and Mullally71), it is clear and simply to apply, no better alternative has yet been proposed. Third, the FFQ was not designed to collect data on consumption of UPF according to the NOVA classification. Each food product was classified in the most likely NOVA group, but we cannot rule out misclassification of some foods. Finally, due to the observational design of this study, the hypothesis of residual confounding cannot be ruled out.
Conclusions
Our results suggest that an increased consumption of UPF is associated with a higher hazard of all-cause mortality. Furthermore, the theoretical isoenergetic substitution of UPF with unprocessed or minimally processed foods would lead to a reduction in the risk of mortality. More studies are needed to confirm these findings in different populations and to unravel the mechanisms by which UPF can affect human health. Likewise, the evidence on the harmful effects on health of the intake of UPF highlights the need for new public health policies, such as the development of nutritional guidelines, to limit the consumption of UPF and to promote the consumption of unprocessed or minimally processed foods.
Acknowledgements
Acknowledgements: The authors thank all collaborators for their involvement in the DRECE study. Financial support: This study was funded by Instituto de Salud Carlos III FIS 03/0014, FIS 08/90643; and by Fundación MMA de Investigación biomédica P-MMA2004/19, P-MMA2008/88. Conflict of interest: The authors declare that they have no conflict of interest. Authorship: All authors contributed to the study conception and design. Funding acquisition and supervision were carried out by A.G.D.L.C. and P.C.N. Material preparation, data collection and analysis were performed by C.R.F., D.L.P. and C.M.-A.A. The first draft of the manuscript was written by Carmen Romero Ferreiro and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. Ethics of human subject participation: The present study was approved by the Research Ethics Committee of the Hospital Universitario 12 de Octubre on 05 November 2010 (ref. 10/292) and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its latter amendments.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021003256







 Open access
Open access