


Obesity and overweight, defined as a BMI greater than or equal to 30 kg/m2 and 25 kg/m2, respectively, are global health challenges(1). Worldwide, it is estimated 1·9 billion adults were in the overweight range(1), while 390 million women and 281 million men had obesity in 2016(2) and that the prevalence of obesity has tripled since the 1970s(3). It is one of the leading risk factors contributing to the total non-fatal and fatal disease burden in high-income countries worldwide(Reference Afshin and Forouzanfar4). A recent systematic review found that obesity is also associated with a substantial economic burden in both developed and developing countries(Reference Tremmel, Gerdtham and Nilsson5). Improving our understanding of the effect of dietary patterns (DP) on the course of obesity could lead to the development of new obesity prevention strategies and management interventions and yield substantial health and economic benefits in affected societies.
Although the origins of the obesity epidemic are not entirely clear(Reference McAllister, Dhurandhar and Keith6), the effects of globalisation resulting in ‘obesogenic’ environments since the 1970s are believed to be the most plausible explanation for the population-wide imbalance between energy intake and expenditure in most societies worldwide(Reference Bleich, Cutler and Murray7,Reference Bray, Nielsen and Popkin8) . Unhealthy DP associated with excess energy intake, especially from energy-dense and nutrient poor foods, have likely played a major role in the development of obesity(Reference Willett, Rockstrom and Loken9). A DP is broadly defined by the quantity, variety, or combination of different foods and beverage in a diet and the frequency with which they are habitually consumed(Reference Sánchez Villegas and Sánchez-Tainta10). Evidence from some systematic reviews have shown that the risk of weight gain and obesity are associated with ‘Western’ diets typically high in energy and nutrient poor(Reference Mu, Xu and Hu11), high intake of refined grains, red meat and sugar-sweetened beverages(Reference Schlesinger, Neuenschwander and Schwedhelm12). Conversely, observational research has shown that both dairy consumption(Reference Louie, Flood and Hector13) and Mediterranean diets (MD), mostly composed of olive oil, fruits, vegetables, bread and cereals, legumes or nuts(Reference Davis, Bryan and Hodgson14), may have a protective effect against developing obesity, but methodological differences between studies weaken the strength of this evidence(Reference Buckland, Bach and Serra-Majem15). Despite this uncertainty, the overall body of evidence suggests that public health strategies warning against established unhealthy DP could help reverse population levels of obesity(16).
Because of the variability in published systematic reviews on this topic regarding DP and their association with obesity(Reference Mu, Xu and Hu11–Reference Louie, Flood and Hector13,Reference Buckland, Bach and Serra-Majem15,Reference Santos, Esteves and da Costa Pereira17–Reference Franz, VanWormer and Crain20) , a summary and grading of this evidence is needed and timely. Following a thorough scoping of the published literature and electronic databases, we found no evidence of an existing or ongoing umbrella review on the above topic. Therefore, to address this knowledge gap, we aimed to summarise the evidence from existing systematic reviews on the association between different DP and overweight/obesity outcomes in adults.
Method
We reported the findings of our umbrella review according to the Preferred Reporting Items of Systematic Reviews and Meta-analyses statement (PRISMA checklist)(Reference Moher, Liberati and Tetzlaff21).
Protocol and registration
Our protocol is registered with the International Prospective Register of Systematic Reviews hosted by the Centre for Reviews and Dissemination (PROSPERO) (CRD42020165391).
Inclusion criteria
To address the broad aim of this systematic review, we developed our research question and selected our specific inclusion and exclusion criteria using the Population, Interventions, Comparators, Outcomes and Study designs (PICOS) framework (Table 1)(Reference Schardt, Adams and Owens22). Our broad research question is ‘are DP associated with obesity outcomes according to systematic reviews?’ We included systematic reviews (with or without meta-analysis) of observational (cohort, case–control or cross-sectional) studies investigating the association of DP (exposure) on obesity incidence, or weight gain (change in weight, change in BMI and change in waist circumference (WC)), as primary outcomes in adult populations. In this study, a DP can be combination of foods consumed and assessed ‘a priori’ or ‘a posteriori’ (derived from cluster analysis or factor analysis). Unhealthy DP, consisting of foods high in energy such as heavily processed and animal source foods, are associated with excessive energy intake and have undoubtedly played a major role in the development of obesity(Reference Willett, Rockstrom and Loken9). Furthermore, components in food such as refined grains and processed meats as well as an excess of sugary drinks have been classified as detrimental to health(Reference Tapsell23). Moreover, high consumption of saturated fats and low consumption of fruits and vegetables have been described as unhealthy dietary practices(24).
Table 1 PICOS criteria for including reviews
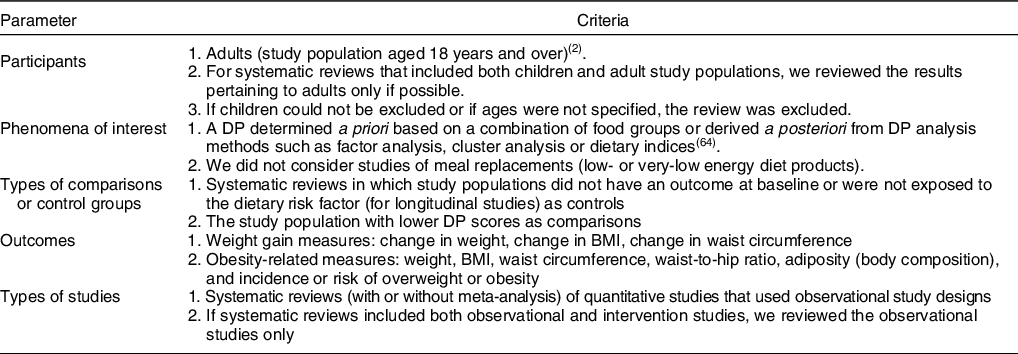
DP, dietary pattern.
The focus of the review includes the following categories: (i) unhealthy v. healthy DP associated with overweight/obesity incidence and (ii) unhealthy v. healthy DP associated with weight gain.
Exclusion criteria
We excluded studies not meeting our inclusion criteria (Fig. 1). For systematic reviews that included both children and adult study populations, we reviewed the results pertaining to adults only where possible. If children could not be excluded or if ages were not specified, the review was excluded. Also, we did not consider studies of meal replacements (low- or very-low energy diet products). If systematic reviews included both observational and intervention studies, we reviewed the observational studies only.
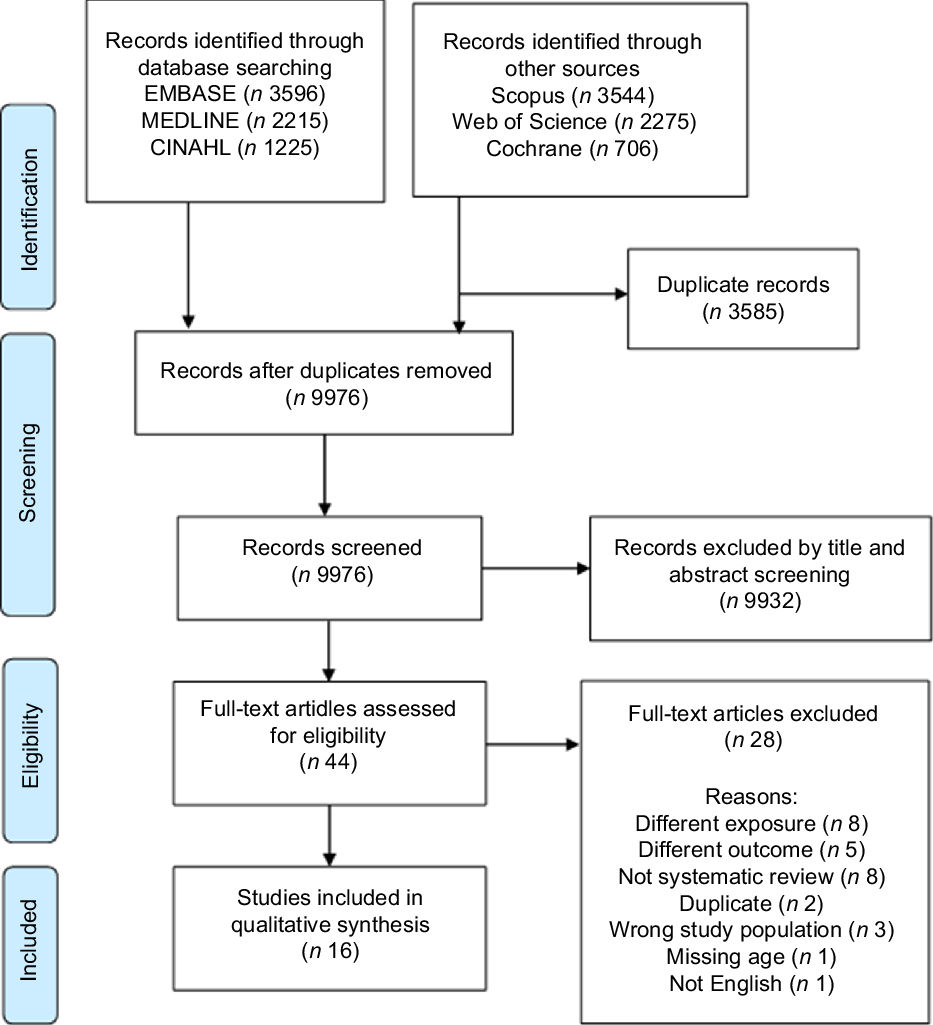
Fig. 1 Preferred reporting items for systematic review and meta-analysis flow diagram of the study selection process
Search strategy
Our search strategy was developed in consultation with a university librarian. We considered reviews written in English and published after 1990 because of limited publications before that(Reference Chalmers, Hedges and Cooper25). Also, since then, high BMI became one of the top five risk factors contributing to deaths and disability-adjusted life-years(26). We searched electronic databases up to February 2020. In the current review, a three-step search process was carried out. First, initial keywords were identified in MEDLINE, then text words included in the title and abstracts were documented followed using index terms to describe related reviews. Second, a search was undertaken in MEDLINE, EMBASE, CINHAL, Cochrane, Scopus and Web of Science using a search strategy, which used subject headings and free texts such as diet, feeding behaviour, plant-based diet, prudent diet, Western diet, overweight, obesity, BMI, and systematic review were used after an academic librarian evaluated them. Third, we searched the reference lists of selected reviews for other potentially eligible reviews. The full search strategy on MEDLINE is available (Appendix S1).
Study selection
Two reviewers (CNS and TGH) assessed the titles and abstracts of systematic reviews against the inclusion criteria and completed the data extraction and quality assessments. First, titles and abstracts were screened and then full-text articles were screened (Fig. 1). We resolved any discrepancies through discussion with a third author (EA) to achieve a consensus.
Data extraction
Two reviewers (CNS and EA) reached a consensus on items such as search databases, source of funding, number of studies, types of studies, exposure and outcome to extract from eligible studies. We created a data extraction template on Microsoft Excel based on items from the Joanna Briggs Institute (JBI) data extraction tool and other items from a literature search.
Quality assessment
We used the JBI critical appraisal checklist for systematic reviews and research syntheses(Reference Aromataris, Fernandez and Godfrey27) (Appendix S2) to assess the quality of included systematic reviews. We assessed the overall quality score of the included reviews using eleven items (Appendix S3), including the clarity of research question, inclusion criteria, search strategy, critical appraisal of individual studies and ways to minimise error and publication bias. Responses were ‘yes’, ‘no’, ‘unclear’or ‘not applicable’; a score of 1 was given for a ‘yes’ response while 0 was given for a ‘no’ response. The overall quality score was sum of score for each item.
Data synthesis
Because of the diverse types of systematic reviews selected, we present the findings in narrative form only with summary tables to aid in data presentation, where appropriate. We defined ‘overlapping studies’ for primary studies reviewed in more than one of the included systematic reviews.
Results
Identification of relevant systematic reviews
A flow diagram of the study selection process appears below (Fig. 1). Our search strategy identified 9976 records after 3585 duplicates were removed. Of these, 9932 records were excluded after the first screening, leaving 44 full-text articles for the second screening. After further assessment, sixteen articles(Reference Buckland, Bach and Serra-Majem15,Reference Aljadani, Patterson and Sibbritt28–Reference Asghari, Mirmiran and Yuzbashian42) met our eligibility criteria for inclusion and narrative synthesis. We summarised the reasons for excluding the twenty-eight full-text articles below (Fig. 1) and in detail in supporting information (Appendix S4). The reasons included not meeting the inclusion criteria such as different exposure, not a systematic review or, missing age. The review of the reference lists added no further eligible articles. The overlapping studies ranged from one to eight in thirteen systematic reviews (Appendix S5)(Reference Buckland, Bach and Serra-Majem15,Reference Aljadani, Patterson and Sibbritt28–Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Hsiao, Jensen and Hartman33,Reference Kastorini, Milionis and Goudevenos36–Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41–Reference Kastorini, Milionis and Esposito43) .
Characteristics of included systematic reviews
The characteristics of the review papers included are presented below (Table 2). In total, there were sixteen systematic reviews published between 2001 and 2019. They reviewed a total of 201 studies published between 1975 and 2015, of which 143 were unique while 58 were duplicates. The studies were conducted in Europe 85 (42·3 %), North America 61 (30·3 %), Asia 21 (10·4 %), Middle East 14 (7·0 %), South America 10 (5·0 %), Africa 6 (3·0 %) and Oceania 4 (2·0 %) in study participants aged 18 years and beyond. The number of individual studies who met the eligibility criteria ranged from 1(Reference Ledoux, Hingle and Baranowski40) to 32(Reference Asghari, Mirmiran and Yuzbashian42), and sample sizes ranged from 11 040(Reference Green, Milner and Joy31) to 946 977(Reference Grosso, Mistretta and Frigiola32). Six reviews assessed the relationship between adherence to MD or Mediterranean diet score (MDS) and overweight/obesity outcomes(Reference Buckland, Bach and Serra-Majem15,Reference Choi, Kim and Joung29,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Esposito35,Reference Kastorini, Milionis and Goudevenos36) . Of these, five reported obesity(Reference Buckland, Bach and Serra-Majem15,Reference Choi, Kim and Joung29,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Esposito35) , four reported abdominal obesity(Reference Choi, Kim and Joung29,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Esposito35) and one reported WC(Reference Kastorini, Milionis and Goudevenos36). Four reviews focused on different diet quality measures and overweight/obesity outcomes(Reference Aljadani, Patterson and Sibbritt28,Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) . Of these, three reported overweight/obesity outcomes(Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) and two reported abdominal obesity(Reference Vadiveloo, Dixon and Parekh39,Reference Asghari, Mirmiran and Yuzbashian42) . Two reviews assessed if fruit and vegetable (FV) consumption was associated with risk of obesity or weight gain(Reference Hutfless, Gudzune and Maruthur34,Reference Ledoux, Hingle and Baranowski40) ; they reported effect estimates of obesity or weight gain. Five reviews assessed other DP and obesity or weight gain(Reference Choi, Kim and Joung29,Reference Green, Milner and Joy31,Reference Hsiao, Jensen and Hartman33,Reference Rezagholizadeh, Djafarian and Khosravi37,Reference Togo, Osler and Sorensen38) . They reported outcomes such as BMI, obesity, abdominal obesity or WC(Reference Choi, Kim and Joung29,Reference Green, Milner and Joy31,Reference Hsiao, Jensen and Hartman33,Reference Rezagholizadeh, Djafarian and Khosravi37,Reference Togo, Osler and Sorensen38) . As presented in Table 2, the overall quality score ranged from 4 to 10. The most frequent quality items lacking in the systematic reviews were for item 6: critical appraisal done in duplicate (n 14); item 5: appropriateness of criteria for critical appraisal (n 11); and item 7: methods to minimise errors in data extraction (n 9) (Appendix S3).
Table 2 Characteristics of included reviews
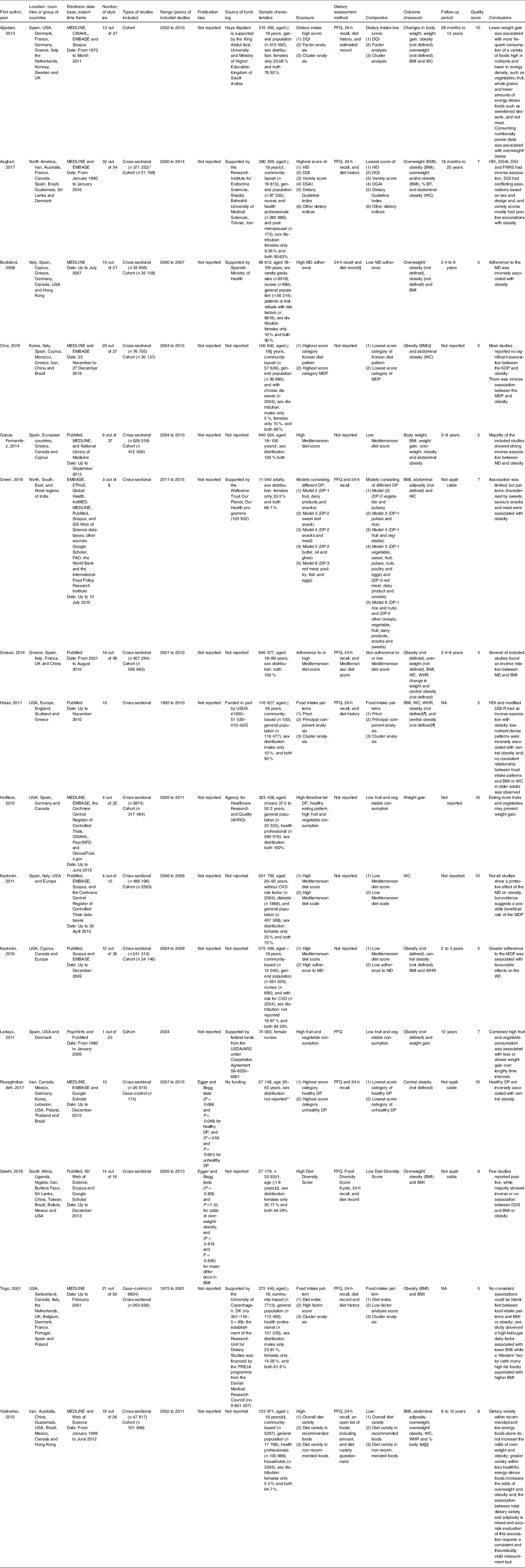
DQI, Diet Quality Index; WC, waist circumference; WHR, waist to hip ratio; BF, body fat; HEI, Healthy Eating Index; DGAI, Dietary Guidelines for Americans Index; DGI, Dietary Guideline Index; FNRS, Framingham nutritional risk score; MD, Mediterranean diet; KDP, Korean dietary pattern; MDP, Mediterranean diet pattern; DP,dietary pattern; NA, not applicable; HDI, Healthy Diet Indicator; DQI-R, Diet Quality Index-International; DDS, Dietary Diversity Score; USDA, United States Department of Agriculture.
* There was double counting of study participants because two studies had both cross-sectional and cohort designs.
† One study had only a population of ≥ 65 years.
‡ Only two studies reported their diet assessment method.
§ Three studies had only participant who are ≥ 55 years of age.
‖ Different BMI cut-offs were used to define obesity.
¶ A cut-off of BMI > 30 kg/m2 for obesity and WC of > 102 cm in men and > 88 cm in women for abdominal obesity was used for one study.
** Sex distribution was reported for both pattern; healthy DP four studies on women and twelve studies on both; unhealthy DP five studies on women and eighteen studies on both.
†† Primary sampling units were households, and analysis is based on that.
‡‡ Two studies included only participants who are above 60 years of age.
§§ WHO cut-offs were used to define obesity.
Findings of systematic reviews
We summarised the findings of all systematic reviews included in our umbrella review (Table 3). The findings are presented first by DP and then by study design.
Table 3 Summary of findings

DI, Diet Index; DQI, Diet Quality Index; MDS, Mediterranean diet score; MD, Mediterranean diet; FA, factor analysis; WC, waist circumference; CA, cluster analysis; CHO, carbohydrate; EI, energy intake; HEI, Healthy Eating Index; DDS, Dietary Diversity Score; FVS, food variety score; DGAI, Dietary Guidelines for Americans Index; DGI, Dietary Guideline Index; PNNS-GS, Program National Nutrition Sante´-Guideline Score; ARFS, Australian Recommended Food Score; RFS, Recommended Food Score; EDI, Elderly Dietary Index; DQS, dietary quality score; NRFS, Not Recommended Food Score; MDP, Mediterranean diet pattern; KDP, Korean dietary pattern; RR, relative risk; DP, dietary pattern; HDI, Healthy Diet Indicator; FS-MDS, Framingham-SENECA Mediterranean Diet Score; HDS, Healthy Diet Score; DQI-R, Diet Quality Index, Revised; PCA, principal component analysis; FV, fruit and vegetable; DMGFV, combination of dairy, meat, grain, fruit and vegetables; DDS-R, Dietary Diversity Score-Revised; FVR, Food Variety Ratio.
Note. Studies may be counted more than once where they have reported more than one outcome. DP in bold show their corresponding results in the right.
Mediterranean diet pattern
Six out of sixteen systematic reviews included eleven cohort and nineteen cross-sectional studies that reported associations between the MD and overweight/obesity-related outcomes or weight gain (Table 3)(Reference Buckland, Bach and Serra-Majem15,Reference Choi, Kim and Joung29,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Esposito35,Reference Kastorini, Milionis and Goudevenos36) . The reviewers generally concluded that the MD was associated with a decreased risk of overweight/obesity outcomes.
Cohort studies
Out of the eleven cohort studies, two reported a decreased incidence of obesity (OR ranging from 0·53 to 0·73) associated with adherence to the MD or higher MDS. One out of the six reviews reported a lower risk of weight gain in two cohort studies with higher MDS (β = –20·16 kg and OR = 0·76)(Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30). No significant association between MD and overweight/obesity-related outcomes was reported in seven out of eleven studies included in three reviews(Reference Buckland, Bach and Serra-Majem15,Reference Choi, Kim and Joung29,Reference Grosso, Mistretta and Frigiola32) .
Cross-sectional studies
Out of the nineteen cross-sectional studies, six reported a decreased prevalence of obesity (OR ranging from 0·12 to 0·88) associated with adherence to the MD or higher MDS. Three out of the six systematic reviews reported a decreased prevalence of central obesity in two cross-sectional studies with adherence to the MD or highest tertile of MDS (OR ranging from 0·41 to 0·72)(Reference Choi, Kim and Joung29,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Goudevenos36) . Two out of the six reviews reported lower BMI in three cross-sectional studies with adherence to the MD or higher MDS (β ranging from –4 to –0·186)(Reference Buckland, Bach and Serra-Majem15,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30) . One out of the six reviews reported a decreased prevalence of overweight in one cross-sectional study with adherence to the MD (OR = 0·33)(Reference Choi, Kim and Joung29). No significant association between MD and overweight/obesity-related outcomes was reported in four out of nineteen studies included in three reviews(Reference Buckland, Bach and Serra-Majem15,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Esposito43) .
Diet quality
Five out of sixteen systematic reviews included fifteen cohort, forty-five cross-sectional or one case–control studies reported associations between diet quality measures such as Diet Quality Index (DQI), Diet Diversity Score (DDS), Food Variety Ratio (FVR), Elderly Dietary Index, Diet Guideline Index, Healthy Eating Index (HEI), and Recommended Food Score and overweight/obesity-related outcomes or weight gain(Reference Aljadani, Patterson and Sibbritt28,Reference Togo, Osler and Sorensen38,Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) . The reviewers generally concluded that there is a mixed association between various diet quality measures and overweight/obesity outcomes.
Cohort studies
Two of three reviews reported an inverse association between weight gain and DQI (mean = –0·059 kg/year, 95 % CI –0·111, –0·008); (mean ± sd = 3·3 ± 17·4 lb v. 8·0 ± 13·0 lb in females and 2·7 ± 10·1 lb v. 5·1 ± 13·3 lb in males); (OR = 0·9); and (mean = –0·061 (–0·116, –0·006)) in four studies(Reference Aljadani, Patterson and Sibbritt28,Reference Asghari, Mirmiran and Yuzbashian42) . One of the three reviews reported decreased incidence of obesity (OR = 0·69, 95 % CI 0·54, 0·89 in females and OR = 0·68, 95 % CI 0·53, 0·89 in males) in one study(Reference Aljadani, Patterson and Sibbritt28). In contrast, two of the three reviews reported increased incidence of obesity (with DQI) (OR = 1·32) or overweight (with FVR) (OR = 1·36, 95 % CI 1·01, 1·82) in two studies(Reference Vadiveloo, Dixon and Parekh39,Reference Asghari, Mirmiran and Yuzbashian42) . No significant association between diet quality measures and overweight/obesity-related outcomes or weight gain was reported in seven out of fifteen studies included in three reviews(Reference Aljadani, Patterson and Sibbritt28,Reference Vadiveloo, Dixon and Parekh39,Reference Asghari, Mirmiran and Yuzbashian42) .
Cross-sectional studies
Three systematic reviews reported lower BMI (with DDS, DQI, energy-weak variety, Recommended Food Score, food variety and HEI) (β ranging from –1·3 to –0·05) in ten cross-sectional studies, but effect estimates were not reported in seven(Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) . Two of the three reviews reported decreased abdominal obesity (with DDS, FVS and HEI) (OR ranging from 0·21 to 0·7) in five studies(Reference Vadiveloo, Dixon and Parekh39,Reference Asghari, Mirmiran and Yuzbashian42) . Similarly, the same reviews reported a decreased obesity (OR ranging from 0·2 to 0·97) (with DDS, Elderly Dietary Index and HEI) in five studies. In contrast, all three reviews reported a higher BMI (β = 0·118) (with DQI, DDS and FVR) in four studies, but effect estimates were unclear in three studies. No significant association between diet quality measures and overweight/obesity-related outcomes was reported in twenty-one out of forty-five studies included in all three reviews(Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) .
Case–control study
One systematic review with one case–control study reported no significant associations between a diet quality measure (diet index) and overweight/obesity-related outcomes(Reference Togo, Osler and Sorensen38).
Combined fruit and vegetable intake
Two out of sixteen systematic reviews included three cohort or two cross-sectional studies that reported associations between combined FV consumption and obesity or weight gain(Reference Hutfless, Gudzune and Maruthur34,Reference Ledoux, Hingle and Baranowski40) . The reviewers generally concluded that eating more FV may prevent weight gain.
Cohort studies
Both reviews in one of the three cohort studies reported decreased incidence of obesity (OR = 0·76, 95 % CI 0·69, 0·86), decreased risk of weight gain >25 kg (OR = 0·72, 95 % CI 0·55, 0·93) and decreased weight gain (0·76 kg less in overweight subjects and 0·52 kg less in normal-weight subjects at baseline). No significant association between combined FV consumption and weight gain was reported in two out of three studies included in both reviews(Reference Hutfless, Gudzune and Maruthur34,Reference Ledoux, Hingle and Baranowski40) .
Cross-sectional studies
One review included two cross-sectional studies that reported an association between combined FV consumption and weight gain(Reference Hutfless, Gudzune and Maruthur34). Of these two studies, one reported more than 698 g/d of fruits and vegetables was associated with decreased weight gain (OR = 0·26, 95 % CI 0·07, 0·97). No significant association between combined FV consumption and weight gain was reported in one out of two studies in this review(Reference Hutfless, Gudzune and Maruthur34).
Other DP
Five systematic reviews and one meta-analysis included forty cross-sectional, six cohort and one case–control studies that reported associations between a range of other different DP such as Korean DP, Indian DP, ‘a priori’ DP, ‘a posteriori’ DP and, healthy/unhealthy DP and overweight/obesity outcomes(Reference Aljadani, Patterson and Sibbritt28,Reference Choi, Kim and Joung29,Reference Green, Milner and Joy31,Reference Hsiao, Jensen and Hartman33,Reference Rezagholizadeh, Djafarian and Khosravi37,Reference Togo, Osler and Sorensen38) .
Cross-sectional studies
Korean diet pattern
One review reported an association between Korean diet pattern and obesity-related outcomes(Reference Choi, Kim and Joung29). Of the forty studies, one study reported a decreased prevalence of abdominal obesity (OR = 0·76, 95 % CI 0·59, 0·98). In contrast, one reported a higher prevalence of obesity (OR = 1·19, 95 % CI 1·06, 1·33) and two studies reported a higher prevalence of abdominal obesity (OR ranging from 1·07 to 1·27) in females with the highest tertile of Korean diet pattern.
Indian DP
One review, in three out of forty studies, reported an association between DP in India and overweight/obesity outcomes. Five DP enriched with fruit, dairy products, snacks; sweets, snacks; snacks, meat; butter, oil, ghee; and red meat, poultry, fish, eggs were associated with high BMI, abdominal adiposity or WC in three studies; however, effect estimates were not reported(Reference Green, Milner and Joy31).
‘A priori’ DP
Two reviews used ‘a priori’ approaches for determining DP associated with obesity outcomes(Reference Hsiao, Jensen and Hartman33,Reference Togo, Osler and Sorensen38) . Of forty studies, two reported associations between lowest quality by Healthy Diet Indicator and Framingham-SENECA MDS and higher (effect estimates not reported) WC in one review(Reference Hsiao, Jensen and Hartman33). Moreover, in the same review, two studies reported that higher Mediterranean score was associated with lower WC (β = –1·2 kg/m2 in one study, effect estimate was unclear the other study) and decreased prevalence of obesity (OR = 0·88) in another(Reference Hsiao, Jensen and Hartman33). One review, in one study, reported a DP consisting type A diet (Table 3) was associated with increased OR for prevalence of obesity (OR = 1·61) in males and (OR = 1·53) in females(Reference Togo, Osler and Sorensen38).
‘A posteriori’ DP
Three reviews assessed the association between ‘a posteriori’ DP (derived from cluster analysis, factor analysis or principal component analysis) and obesity outcomes(Reference Hsiao, Jensen and Hartman33,Reference Rezagholizadeh, Djafarian and Khosravi37,Reference Togo, Osler and Sorensen38) . Three of the forty studies in one review(Reference Togo, Osler and Sorensen38) reported DP such as ‘low culinary complexity’, ‘prudent’ and ‘satiating’ (Table 3) were associated with lower BMI in males, while ‘convenience’ was associated with lower BMI in females, but effect estimates were not reported. One study in the same review reported ‘Western’ DP was associated with higher BMI, whereas another reported ‘bush foods’ were associated with a higher prevalence of obesity. Three of the fifty-two studies in one review reported DP such as ‘meat, eggs and fat’, ‘rice, added fats (cooking oil), beans and poultry’, ‘low-nutrient-dense’ and ‘vegetable-based’ were associated with high BMI(Reference Hsiao, Jensen and Hartman33). No significant association between other DP and overweight/obesity-related outcomes was reported in fifteen out of forty studies included in three reviews(Reference Choi, Kim and Joung29,Reference Hsiao, Jensen and Hartman33,Reference Togo, Osler and Sorensen38) .
Cohort studies
‘A posteriori’ DP
One systematic review included six cohort studies that reported association between ‘a posteriori’ DP (derived from cluster analysis or factor analysis) and obesity outcomes(Reference Aljadani, Patterson and Sibbritt28). One of the six studies reported highest quintile of ‘healthy and fibre-rich diet pattern’ was associated with lower annual change in WC (β =–1·06 cm, 95 % CI –1·88, –0·24). Another study showed ‘meat and potatoes diet pattern’ was associated with greater annual increase in BMI (β = 0·26). No significant association between other DP and overweight/obesity-related outcomes was reported in three out of six studies in this review(Reference Aljadani, Patterson and Sibbritt28).
Case–control studies
‘A posteriori’ DP
One systematic review included one case–control study that reported associations between other DP and obesity outcomes. This study reported ‘high fat/sugar-dairy’ (Table 3) was associated with lower BMI in males, while ‘Drinker’ was associated with lower BMI in females, but effect estimate not reported(Reference Togo, Osler and Sorensen38). ‘Drinker’ and ‘Fruit juice’ were associated with higher BMI in males, while ‘Western’ was associated with higher BMI in the same study.
Findings from meta-analysis
Healthy and unhealthy DP
One review with twelve cross-sectional and one case–control studies reported a decreased pooled OR (0·81, 95 % CI 0·66, 0·96) for central obesity with higher healthy DP (Table 3). However, no significant association between unhealthy DP and central obesity was reported(Reference Rezagholizadeh, Djafarian and Khosravi37).
Discussion
Summary of evidence
We believe that this is the first umbrella review of observational studies on specific DP associated with overweight/obesity outcomes. Our evidence summary suggests that the most widely researched Mediterranean-type DP was consistently associated with lower overweight or obesity prevalence and incidence over 2 to 9 years of follow-up(Reference Buckland, Bach and Serra-Majem15,Reference Choi, Kim and Joung29,Reference Garcia-Fernandez, Rico-Cabanas and Rosgaard30,Reference Grosso, Mistretta and Frigiola32,Reference Kastorini, Milionis and Goudevenos36,Reference Kastorini, Milionis and Esposito43) . Similarly, a smaller body of evidence suggests that combined FV consumption was inversely associated with weight gain(Reference Hutfless, Gudzune and Maruthur34,Reference Ledoux, Hingle and Baranowski40) . Other DP, which also overlap with components of the MD, were also inversely associated with overweight/obesity outcomes(Reference Hsiao, Jensen and Hartman33,Reference Rezagholizadeh, Djafarian and Khosravi37,Reference Togo, Osler and Sorensen38) . By contrast, overweight/obesity outcomes were inconsistently associated with other diet quality predictors, namely DQI, DDS and FVR(Reference Aljadani, Patterson and Sibbritt28,Reference Vadiveloo, Dixon and Parekh39,Reference Salehi-Abargouei, Akbari and Bellissimo41,Reference Asghari, Mirmiran and Yuzbashian42) . Thus, the body of evidence provides some support for the usefulness of Mediterranean-type DP in reducing the risk of obesity between 12 % and 65 %, a range that is broadly consistent with current guidelines for overall health(16,44) .
The Mediterranean-type DP is characterised by high intake of plant foods such fruit, vegetables, legumes, nuts and whole grains; olive oil as the main source of dietary fat; a frequent but moderate intake of red wine with meals; moderate intake of fresh fish, dairy products, poultry and eggs; and a low intake of red meat and processed meat in amount and frequency(Reference Willett, Sacks and Trichopoulou45,Reference Olmedo-Requena, González-Donquiles and Dávila-Batista46) . The most important factor explaining how the Mediterranean-type DP is potentially protective against obesity is its low energy density composition(Reference Schröder, Vila and Marrugat47). A recent systematic review of cohort studies found consistent evidence of an increased risk of obesity outcomes associated with energy density(Reference Rouhani, Haghighatdoost and Surkan48). By contrast, evidence from randomised controlled trials of the MD have consistently shown a reduction in body weight and BMI(Reference Huo, Du and Xu49), as well as improvements in metabolic and inflammatory risk parameters(Reference Dinu, Pagliai and Casini50). The above-described overall health benefits of the Mediterranean DP may also be partly attributable to its high micronutrient and flavonoid content(Reference Castro-Quezada, Roman-Vinas and Serra-Majem51–Reference Davis, Bryan and Hodgson53).
In this umbrella review, we found that variably measured diet quality was inconsistently associated with overweight/obesity outcomes. For instance, HEI was inversely consistently associated(Reference Asghari, Mirmiran and Yuzbashian42), while DQI, DDS and FVR were both directly and inversely associated with obesity outcomes(Reference Vadiveloo, Dixon and Parekh39). It has been previously shown that higher diet diversity intervention may not be an effective strategy to promote healthy weight(Reference de Oliveira Otto, Anderson and Dearborn54). Moreover, the findings from other studies of diet quality are inconsistent for BMI outcomes across specific population groups(Reference Sundararajan, Campbell and Choi55,Reference López-Olmedo, Popkin and Mendez56) . Although diet quality is likely to be associated with obesity in some populations(Reference Livingstone and McNaughton57), the heterogeneity in diet quality measures may have confounded true associations among other populations.
In this study, the evidence on the positive relationship between FV consumption and decreased weight gain was limited but consistent with previous research(Reference Hutfless, Gudzune and Maruthur34). For instance, a recent systematic review reported ‘moderate quality evidence’ for an inverse association between vegetable intake and weight-related outcomes in adults(Reference Nour, Lutze and Grech58). Another study published since showed that FV intake was inversely associated with BMI and WC(Reference Yu, DeClercq and Cui59). FV consumption is often recommended by expert bodies as an effective strategy for obesity prevention(Reference Tohill60) or weight management(Reference Rolls, Ello-Martin and Beth Carlton61). In this review, healthy DP, including higher fruits and vegetables, based on ‘a posteriori’ approach (derived from principal component analysis) were also associated with decreased central obesity(Reference Rezagholizadeh, Djafarian and Khosravi37). Thus, public health policy-makers should consider strategies to increase population-wide consumption of fruits and vegetables to reduce the risk of obesity in their countries.
Limitations
The present umbrella review has several limitations that should be considered. First, since the individual studies in included reviews were observational studies, the association between MD and overweight/obesity outcomes should be interpreted with caution. For instance, none of the reviews considered or handled the possibility of unadjusted confounding (in their included studies) from other well-established risk factors such as genetic or environmental factors(Reference Choquet and Meyre62,Reference Bouchard63,Reference Hu64) . Second, diet quality was assessed by different methods which may have contributed to the mixed findings between diet quality and overweight/obesity outcomes. For instance, of all the diet quality measures, only the HEI was consistently and inversely associated with overweight/obesity outcomes(Reference Togo, Osler and Sorensen38,Reference Vadiveloo, Dixon and Parekh39,Reference Asghari, Mirmiran and Yuzbashian42) , whereas there was a mixed association between DQI and overweight/obesity outcomes(Reference Asghari, Mirmiran and Yuzbashian42). Moreover, dietary assessment was heterogeneous, and the use of FFQ without evidence of their validity(Reference Aljadani, Patterson and Sibbritt28,Reference Choi, Kim and Joung29) in individual studies may have partially biased in findings of the included systematic reviews. Third, despite using a rigorous search strategy, we may have missed potentially relevant systematic reviews (e.g. selection bias, unpublished reports and records archived in other electronic databases).
Implications
This umbrella review indicates that there is a growing body of evidence supporting the potential benefit of Mediterranean-type DP in reducing the risk of obesity in adults. Public health policy-makers should consider developing dietary guidelines that are aligned with the Mediterranean-type DP for overall health benefits, including the prevention of overweight/obesity at the population level. Strategies focusing on DP that are low in energy density such as the MD could help reverse the high rates of obesity worldwide. Population-specific evidence of effective interventions and implementation strategies are still needed.
Conclusion
Our review confirms the hypothesis that Mediterranean-type DP reduce the risk of obesity in adults. Health policy-makers, healthcare professionals and consumers should consider the importance of Mediterranean-type DP and low energy density diets more broadly in applying obesity prevention recommendations, with caution.
Acknowledgements
Acknowledgements: The reviewers would like to acknowledge the Western Sydney University’s academic librarian. Financial support: This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Conflict of interest: There are no conflicts of interest. Authorship: Conceptualisation: E.A. and C.N.S.; search, screening, data extraction and quality: C.N.S., T.G.H. and E.A.; writing: C.N.S., T.G.H., P.P.F., S.F. and E.A.. All authors read and approved the final version of this manuscript. Ethics of human subject participation: This article does not include studies conducted by the authors.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021000823






