


Autism spectrum disorders are a heterogeneous group of pervasive developmental disorders characterised by qualitative impairments in social interaction, communication and restricted and stereotyped patterns of interests and behaviours. Recent studies estimate that about 1% of the child population Reference Levy, Mandell and Schultz1–3 may have an autism spectrum disorder, representing almost a 20-fold rise in prevalence compared with reports before the 1980s. Reference Fombonne4 Although much of this sharp rise in prevalence may be explained by widening of diagnostic criteria and increased recognition, a true increase in incidence of autism cannot be ruled out Reference Fombonne4,Reference Rutter5 and constitutes an ‘urgent public health concern’. 3 Although heritable, the aetiology of autism spectrum disorder is not well understood. In the context of rising prevalence, the search for environmental risk factors is increasingly important.
Migration is one such factor that has attracted research interest, with vitamin D deficiency and ethnicity suggested as possible explanatory mechanisms. Reference Dealberto6,Reference Keen, Reid and Arnone7 However, previous studies on the topic of migration and risk of autism spectrum disorder vary markedly in quality, sample sizes and definitions of autism. They have also produced inconsistent findings, including reports of an increased, Reference Keen, Reid and Arnone7–Reference Barnevik-Olsson, Gillberg and Fernell12 similar Reference Hultman, Sparen and Cnattingius8,Reference Lauritsen, Pedersen and Mortensen9,Reference Croen, Grether and Selvin13,Reference Gillberg, Steffenburg, Börjesson and Andersson14 and even decreased Reference Croen, Grether and Selvin13,Reference Kamer, Zohar, Youngmann, Diamond, Inbar and Senecky15 risk of autism in children of migrants. There is some evidence that any positive association between parental migration and autism may be confined to autism with comorbid intellectual disability, Reference Dealberto6 with at least one study reporting a lowered risk for autism with normal or high intelligence. Reference Haglund and Kallen16
Clarification of the role of migration in the development and detection of autism spectrum disorder may provide aetiological insights and help reveal preventable health inequalities. A focus on the possibility of such health inequalities is particularly important in countries like Sweden where, since the 1970s, migration from outside of Europe has principally consisted of the provision of asylum to people fleeing armed conflict or other extreme adversities. Migration in this context may entail exceptionally stressful circumstances and be linked to social disadvantages both in the home country and during resettlement. Reference Bourque, van der Ven and Malla17 We therefore studied the association between migration and autism spectrum disorder in a large, Swedish total-population-based sample, concentrating on four important aspects that remain unexplored: (a) characteristics of parental region of origin (both geographical region and an index of human development), (b) the importance of timing of migration in relation to the birth of the index child, (c) discrepancies in observed associations between low- and high-functioning autism, and (d) the potentially explanatory role of obstetric and socioeconomic factors.
Method
Study design and study population
We conducted a matched case–control study nested within the Stockholm Youth Cohort, a register-based cohort of all children aged 0–17 years living in Stockholm County between 2001 to 2007 (n = 589 114). Individuals with autism spectrum disorder (the case group) were ascertained using an exhaustive multisource case ascertainment method through data linkage with official registries covering all pathways of assessment or care of individuals with autism spectrum disorder in Stockholm County (see Method in the online supplement). All Swedish citizens, including migrants with a residence permit, have unique national identification numbers that allowed record linkage with relevant registers for our study.
In the present study, we excluded children who were adopted, were resident in Stockholm County for less than 4 years, had one parent born abroad or had missing data (online Fig. DS1). Asylum seekers without a residence permit were by default excluded. Ethical approval was given by the research ethics committee at Karolinska Institutet, Stockholm, Sweden.
Case ascertainment
Sweden's child public services system is provided free of charge and used by the overwhelming majority of the population. All infants and pre-school children are offered structured health and developmental assessments to screen for developmental and medical problems in well-baby clinics. Such an assessment with evaluation of social, motor, language and cognitive development is carried out at age 4, in order to ensure timely referral of children with suspected autism to specialist services. Referrals can also be requested by parents, schools and other health or social care agencies. Diagnoses of autism spectrum disorder in Stockholm County are made by specialist multiprofessional teams at paediatric or child and adolescent mental health services. Guidelines require the use of structured diagnostic assessments covering the child's social, medical and developmental history, observation of the child in naturalistic settings and a structured neuropsychiatric assessment including cognitive testing using standardised and internationally recognised tools (such as Wechsler Intelligence Scale for Children, Wechsler Preschool and Primary Scale of Intelligence, Snijders-Oomen Non-Verbal Intelligence Test (Revised), and Leiter). Reference Axén18 The County Council offers follow-up care to children with diagnosed autism, which includes special education, occupational therapy, social care or other services through its habilitation services. The habilitation services for children with autism spectrum disorder in Stockholm County are organised and provide care according to the presence of comorbid intellectual disability (defined as an IQ of 70 or less). We identified children with autism spectrum disorder via registers covering the above healthcare pathways: that is, child and adolescent mental health, habilitation, paediatric out-patient or in-patient services (see Method in the online supplement).
We studied autism spectrum disorder as a group and dichotomised into high-functioning autism (defined by the absence of a recorded comorbid intellectual disability, IQ<70 by international and Swedish convention) and low-functioning autism (defined by the presence of a recorded comorbid intellectual disability). This strategy of subcategorisation was based on literature highlighting these as two key categories for future classification Reference Szatmari, White and Merikangas19 and since the information on DSM-IV 20 subcategories was not readily available in all registers.
Previous studies have validated the diagnostic accuracy of mental health and autism diagnoses recorded in Swedish healthcare registers and have found them to have good validity. Reference Hultman, Sandin, Levine, Lichtenstein and Reichenberg21 Similar findings have also been found in neighbouring Denmark, which has a similar system of healthcare and official registries. Reference Lauritsen, Jorgensen, Madsen, Lemcke, Toft and Grove22 We furthermore conducted a validation study, including 200 randomly selected individuals (100 with high- and 100 with low-functioning autism) from the Stockholm Youth Cohort. Case notes were scrutinised by a child and adolescent psychiatrist (S.I.) and a neuropaediatric registrar. An autism spectrum disorder diagnosis was confirmed in 170 (96%) of these individuals in whom complete records were retrieved (n = 177), and clear evidence in support of the high- and low-functioning autism dichotomy based on cognitive assessments was available in 88% and 76% of instances respectively (details available from the author on request). Finally, we cross-validated our case group against information from a national population-based study of twins (the Child and Adolescent Twin study in Sweden (CATSS)). Reference Lichtenstein, Carlstrom, Rastam, Gillberg and Anckarsater23 We identified 27 individuals with autism spectrum disorder among the twins in the Stockholm Youth Cohort and 23 (85%, 95% CI 66–96%) of these had an autism spectrum disorder confirmed in CATSS (according to parental reports and A-TAC, a screening interview targeting neurodevelopmental disorders). Reference Larson, Anckarsater, Gillberg, Stahlberg, Carlstrom and Kadesjo24 Virtually none (1%) of the non-case twins in our study (n = 2721) received an autism spectrum disorder diagnosis in CATSS.
Exposure and other variables
Prospectively recorded information on children and their parents were retrieved by linkage with registers that contain data based on mandatory reporting. This information included: country of birth; date of immigration to Sweden; family income at birth or (for children born abroad) at the earliest measured point in childhood; and pregnancy outcomes, including birth weight for gestational age, gestational age and Apgar score at 5 min (see Method in the online supplement).
Using mother's country of birth, migration status was first studied by geographical region of birth (United Nations definitions, available at http://unstats.un.org/unsd/methods/m49/m49regin.htm) and then by level of human development (using the UNDP Human Development Index, a composite indicator of development derived using indicators of life expectancy, education and income, available at http://hdr.undp.org/en/statistics/hdi/). These two groupings were employed to capture different dimensions of the parental countries of origin that may be of importance for the development or detection of offspring autism. These dimensions include, for example, ethnicity or environmental factors related to geographical region, as opposed to level of civil unrest or aspects of deprivation related to poor human development. The mother's country of origins was used to characterise parental background, since the paternal and maternal countries of birth were largely identical in children with both parents born abroad.
Data analysis
Ten randomly selected individuals in the control group (that were alive and free of autism) were matched to each individual in the case group by birth date and gender. We conducted conditional logistic regression analyses to estimate crude and adjusted odds ratios (ORs) as estimates of relative risks and their 95% confidence intervals for autism spectrum disorder according to parental region of birth and the timing of the mother's immigration in relation to the child's birth. We also studied the mutual effect of maternal region of birth and maternal timing of migration in the same model among migrant children only. We tested for trends using the Cochrane-Armitage method.
All models were adjusted for maternal age (<20, 20–29, 30–39, 40+ years) and paternal age (<20, 20–29, 30–39, 40–49, 50+ years) at the child's birth, and for family disposable income (in quartiles) at birth or in childhood. To study whether any observed associations between maternal region of birth and low-functioning autism were mediated by birth outcomes, we repeated our analyses with additional adjustment for birth weight for gestational age (being small for gestational age or not), gestational age (<32, 32–36, 37+ weeks) and Apgar score at 5 min after birth (<7, ≥7). Since these obstetric data were not available for children born outside Sweden, this analysis was restricted to the subsample of children born in Sweden. All analyses were conducted overall, and according to the gender of child, using SAS 9.2 for Windows.
Results
We identified 4952 individuals with autism spectrum disorder comprising 2855 children with high-functioning and 2097 with low-functioning autism. Our study population for this paper was restricted to the 3918 children with autism spectrum disorder meeting our inclusion criteria, comprising 2269 children with high-functioning and 1649 children with low-functioning autism (online Fig. DS1).
A total of 21% of our total study population had both parents born outside of Sweden. The mean duration of residence of the children to migrant parents in Stockholm County varied somewhat with region of origins, but was by definition always over 4 years, and in all age groups exceeded the age and period typically required for detection and diagnosis of autism spectrum disorder (online Table DS1).
Table 1 depicts the odds ratios for autism spectrum disorder in relation to maternal geographical region of birth among
TABLE 1 Relative risk of autism spectrum disorder in relation to maternal geographical region of birth
| Migration status | Case group/control group, n | OR (95% CI) | Adjusted OR a (95% CI) |
|---|---|---|---|
| Both parents born in Sweden | 31 22/31 445 | 1.0 | 1.0 |
| Both parents born abroad | 796/8 600 | 0.9 (0.9–1.0) | 0.9 (0.9–1.0) |
| Maternal country of birth, by geographical subregion b | |||
| Northern Africa | 31/317 | 1.0 (0.7–1.4) | 1.0 (0.7–1.4) |
| Eastern Africa | 122/933 | 1.3 (1.1–1.6) | 1.1 (0.9–1.4) |
| Other African | 30/168 | 1.8 (1.2–2.6) | 1.5 (1.0–2.2) |
| Northern America | 1/32 | N/A | N/A |
| Latin America/Caribbean | 94/759 | 1.3 (1.0–1.6) | 1.1 (0.9–1.4) |
| Southern Asia | 85/988 | 0.9 (0.7–1.1) | 0.8 (0.6–1.0) |
| Western Asia | 181/2848 | 0.6 (0.5–0.7) | 0.6 (0.5–0.7) |
| Other Asian | 26/269 | 1.0 (0.7–1.5) | 0.9 (0.6–1.3) |
| Northern Europe | 114/996 | 1.1 (0.9–1.4) | 1.1 (0.9–1.3) |
| Eastern Europe | 57/531 | 1.1 (0.8–1.4) | 0.9 (0.7–1.3) |
| Southern Europe | 41/612 | 0.7 (0.5–0.9) | 0.6 (0.4–0.9) |
| Western Europe | 14/136 | 1.1 (0.6–1.8) | 1.0 (0.6–1.7) |
N/A, not applicable.
a Adjusted for maternal and paternal age at child's birth and family disposable income at child's birth or in early life, as applicable.
b Among children with both parents born abroad. Countries contributing the largest number to the case group in each subregion being (when applicable): Northern Africa - Morocco; Eastern Africa - Somalia and Ethiopia; Latin America and the Caribbean - Chile; Southern Asia - Iran; Western Asia - Iraq and Turkey; Northern Europe - Finland; Eastern Europe - Poland; Southern Europe - Former Yugoslavia.
TABLE 2 Relative risk of high- and low-functioning autism in relation to maternal geographical region of birth
| High-functioning autism | Low-functioning autism | |||||
|---|---|---|---|---|---|---|
| Migration status | Case group/control group, n | OR (95% CI) | Adjusted OR a (95% CI) | Case group/control group, n | OR (95% CI) | Adjusted OR a (95% CI) |
| Both parents born in Sweden | 1963/18116 | 1.0 | 1.0 | 1159/13357 | 1.0 | 1.0 |
| Both parents born abroad | 306/4925 | 0.5 (0.5–0.6) | 0.5 (0.4–0.6) | 490/3646 | 1.5 (1.3–1.7) | 1.2 (1.0–1.4) |
| Maternal country of birth, by geographical subregion b | ||||||
| Northern Africa | 8/175 | 0.4 (0.2–0.8) | 0.3 (0.2–0.7) | 23/123 | 2.0 (1.3–3.1) | 1.5 (0.9–2.4) |
| Eastern Africa | 26/521 | 0.4 (0.3–0.6) | 0.3 (0.2–0.5) | 96/414 | 2.5 (2.0–3.1) | 1.9 (1.5–2.5) |
| Other African | 2/82 | 0.2 (0.1–0.6) | 0.2 (0.0–0.7) | 28/66 | 3.6 (2.4–5.3) | 3.5 (2.5–5.6) |
| Northern America | 1/20 | N/A | N/A | 0/11 | N/A | N/A |
| Latin America/Caribbean | 35/456 | 0.7 (0.5–0.9) | 0.5 (0.4–0.8) | 59/334 | 1.9 (1.4–2.4) | 1.6 (1.2–2.2) |
| Southern Asia | 26/556 | 0.5 (0.3–0.6) | 0.3 (0.2–0.5) | 59/415 | 1.6 (1.2–2.1) | 1.3 (0.9–1.7) |
| Western Asia | 64/1627 | 0.4 (0.3–0.5) | 0.3 (0.2–0.4) | 117/1165 | 1.1 (0.9–1.3) | 0.9 (0.7–1.2) |
| Other Asian | 13/160 | 0.6 (0.4–1.1) | 0.6 (0.4–1.1) | 13/117 | 1.1 (0.7–1.9) | 1.1 (0.6–2.0) |
| Northern Europe | 74/572 | 1.2 (0.9–1.5) | 1.1 (0.8–1.4) | 40/445 | 1.1 (0.8–1.6) | 0.9 (0.6–1.2) |
| Eastern Europe | 35/308 | 1.0 (0.7–1.3) | 0.8 (0.6–1.2) | 22/232 | 1.0 (0.7–1.5) | 0.8 (0.5–1.3) |
| Southern Europe | 14/355 | 0.3 (0.2–0.6) | 0.3 (0.2–0.5) | 27/251 | 1.3 (0.9–1.8) | 1.1 (0.8–1.7) |
| Western Europe | 8/85 | 0.9 (0.5–1.8) | 0.8 (0.4–1.7) | 6/66 | 1.1 (0.5–2.3) | 1.0 (0.4–2.2) |
N/A, not applicable.
a Adjusted for maternal and paternal age at child's birth and family disposable income at child's birth or in early life, as applicable.
b Among children with both parents born abroad. Countries contributing the largest numbers to the case group in each subregion being (when applicable): Northern Africa - Morocco; Eastern Africa - Somalia and Ethiopia; Latin America and the Caribbean - Chile; Southern Asia - Iran; Western Asia - Iraq and Turkey; Northern Europe - Finland; Eastern Europe - Poland; Southern Europe - Former Yugoslavia.
children with both parents born abroad as compared with children with both parents born in Sweden. As a combined group, autism spectrum disorder did not appear to have any clear association with migration status. Yet, when this association was examined separately for high- and low-functioning autism, clearly divergent relationships were observed (Table 2). The odds of low-functioning autism was increased in children of migrant parents (crude OR = 1.5, 95% CI 1.3–1.7), and this relationship varied with region of maternal birth. Children of parents born in SubSaharan Africa had especially elevated odds, but also those with parental origins in Northern Africa, Latin America, the Caribbean and Southern Asia were more often diagnosed with low-functioning autism than children of Swedish-born parents. In strong contrast, children of migrant parents appeared to have a reduced odds of high-functioning autism (crude OR = 0.5, 95% CI 0.5–0.6) (Table 2). Notably, this inverse association was observed in almost all groups of migrant children, including those in which increased associations with low-functioning autism were not observed.
The odds of low-functioning autism increased with a decreasing human development index in the country of parental origin (P for trend <0.0001, Table 3). For high-functioning autism, the odds in migrant children were instead almost half that of children with parents born in Sweden, except when parents originated from countries with a very high human development index (Table 3).
There was a non-linear association between time since maternal immigration and odds of low-functioning autism (Fig. 1, online Table DS2). Children of mothers who migrated during pregnancy had the highest odds (crude OR = 2.3, 95% CI 1.7–3.0), whereas children born abroad and arriving in Sweden after the age of 4 had an odds ratio below unity. When both the maternal timing of migration and region of birth were considered simultaneously in a mutually adjusted model, both characteristics were independently associated with low-functioning autism (Table 4). No pattern in odds ratios with timing of migration was, however, evident for high-functioning autism.
The relationships reported above were not affected by adjustment for parental age (Tables 1,2,3,4), or for obstetric complications (in an analysis restricted to children born in Sweden, see online Table DS3). Adjustment for family disposable income, a characteristic highly correlated with migration from low-income countries, partially attenuated the positive associations between parental migration and low-functioning autism (Tables 1,2,3,4). The relationships between maternal geographical region of birth and high-functioning autism as well as low-functioning autism were similar in boys and girls (data not shown).
Discussion
In this large population-based study in Stockholm County, we found children of migrant parents to be at an increased risk of autism with intellectual disability. This risk appeared greatest in children of parents who migrated to Sweden from regions with a low human development index, and peaked when migration occurred around the time of pregnancy. In contrast, the risk of autism without intellectual disability was reduced regardless of timing of migration, and for most regions of parental origin.
Comparison with previous studies
One recent study in Malmö, Sweden, presented separate associations for risks of autism with and without intellectual disability and found results strikingly similar to ours, albeit in a much smaller sample of 250 participants. Reference Haglund and Kallen16 All other population-based studies with individual-level data have only examined migration as one of several risk factors, Reference Hultman, Sparen and Cnattingius8–Reference Williams, Helmer, Duncan, Peat and Mellis11,Reference Croen, Grether and Selvin13 often
TABLE 3 Relative risk of high- and low-functioning autism in relation to maternal country of birth categorised according to human development index (HDI)
| High-functioning autism | Low-functioning autism | |||||
|---|---|---|---|---|---|---|
| Migration status | Case group/control group, n | OR | Adjusted OR a | Case group/control group, n | OR | Adjusted OR a |
| Both parents born in Sweden | 1963/18116 | 1.0 | 1.0 | 1159/13357 | 1.0 | 1.0 |
| Both parents born abroad Maternal country of birth, by HDI | ||||||
| Low | 54/1179 | 0.4 (0.3–0.5) | 0.4 (0.3–0.5) | 167/898 | 2.1 (1.8–2.6) | 1.9 (1.6–2.3) |
| Medium | 62/1276 | 0.4 (0.4–0.6) | 0.4 (0.3–0.5) | 128/933 | 1.6 (1.3–1.9) | 1.4 (1.1–1.7) |
| High | 92/1579 | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) | 137/1145 | 1.4 (1.1–1.7) | 1.3 (1.0–1.6) |
| Very high | 98/891 | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 58/670 | 1.0 (0.8–1.3) | 0.9 (0.7–1.2) |
a Adjusted for maternal and paternal age at child's birth and family disposable income at child's birth or in early life, as applicable.
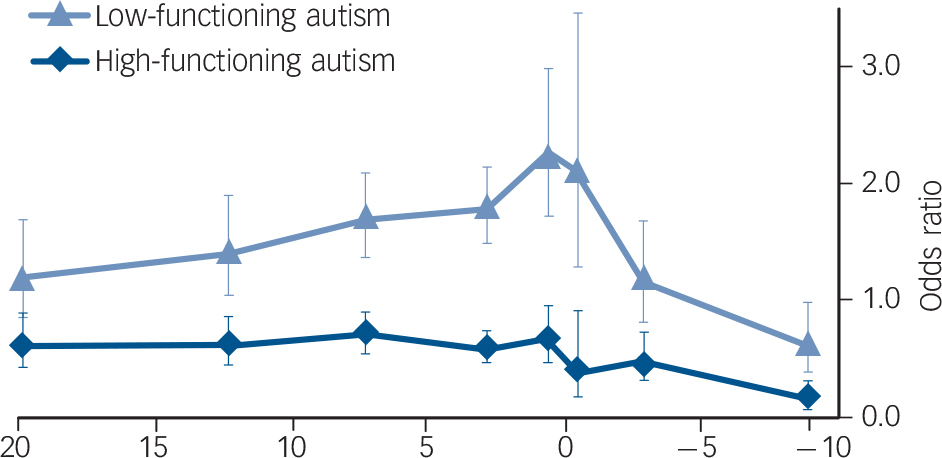
Fig. 1 Relative risk of high- and low-functioning autism in children with both parents born abroad as compared with those with both parents born in Sweden, by time since maternal immigration in relation to the child's birth.
Positive values indicate time since maternal migration to Sweden before the child's birth (in second-generation immigrant children), negative values indicate age of child when the mother migrated to Sweden (in first-generation immigrant children). Bars represent 95% confidence interval.
simply defining migration status as ‘mother born abroad’. These studies generated inconsistent findings, with parental migration either not related to autism spectrum disorder Reference Hultman, Sparen and Cnattingius8,Reference Lauritsen, Pedersen and Mortensen9,Reference Croen, Grether and Selvin13 or associated with a higher Reference Hultman, Sparen and Cnattingius8–Reference Williams, Helmer, Duncan, Peat and Mellis11 or lower Reference Croen, Grether and Selvin13 risk. This inconsistency may be partly explained by differences between studies in their definitions of autism and the proportion of children with associated intellectual disability (online Table DS4). Other studies on this topic lacked individual-level control data Reference Keen, Reid and Arnone7,Reference Barnevik-Olsson, Gillberg and Fernell12,Reference Gillberg, Steffenburg, Börjesson and Andersson14,Reference Kamer, Zohar, Youngmann, Diamond, Inbar and Senecky15,Reference Gillberg and Gillberg25–Reference Wing27 and reported similar or increased risks of autism in children of migrant mothers, except one study from Israel Reference Kamer, Zohar, Youngmann, Diamond, Inbar and Senecky15 that found a reduced risk in Ethiopian migrants (online Table DS4).
Increased risk of low-functioning autism in children of migrant parents
One possible explanation for the observed association between mother's (employed as a proxy for both parents') country of birth and risk of low-functioning autism is that the underlying autism-spectrum disorder rates vary in different countries of origin. It is difficult to examine this possibility, because very little is known about indigenous prevalence of autism spectrum disorder in low- and middle-income countries. Reference Fombonne28 Difference in risk by ethnicity or skin colour is another possible explanation (for example, reflecting darker skin pigmentation increasing the risk of maternal vitamin D insufficiency during pregnancy Reference Dealberto6 ), although a British study found little evidence of an independent ethnic
TABLE 4 Relative risk of high- and low-functioning autism in relation to mother's region of birth and time since immigration, among children with both parents born abroad only
| High-functioning autism | Low-functioning autism | |||||
|---|---|---|---|---|---|---|
| Migration status | Case group/control group, n | Adjusted OR a | Adjusted OR b | Case group/control group, n | Adjusted OR a | Adjusted OR b |
| Mother's geographical subregion of birth c | ||||||
| Northern Africa | 8/175 | 0.3 (0.1–0.6) | 0.3 (0.1–0.6) | 23/123 | 1.9 (1.0–3.5) | 1.7 (0.9–3.2) |
| Eastern Africa | 26/518 | 0.3 (0.2–0.5) | 0.3 (0.2–0.5) | 96/412 | 2.0 (1.2–3.1) | 1.9 (1.2–3.0) |
| Other African | 2/81 | 0.1 (0.0–0.6) | 0.1 (0.0–0.5) | 28/66 | 3.7 (2.0–6.9) | 3.6 (1.9–6.9) |
| Northern America | 1/20 | N/A | N/A | 0/11 | N/A | N/A |
| Latin America/Caribbean | 34/451 | 0.6 (0.4–0.9) | 0.6 (0.3–0.9) | 59/330 | 2.0 (1.2–3.1) | 2.0 (1.2–3.3) |
| Southern Asia | 26/551 | 0.3 (0.2–0.5) | 0.3 (0.2–0.5) | 59/412 | 1.3 (0.8–2.2) | 1.3 (0.8–2.1) |
| Western Asia | 64/1617 | 0.3 (0.2–0.4) | 0.3 (0.2–0.4) | 116/1159 | 1.0 (0.7–1.5) | 1.0 (0.6–1.5) |
| Other Asian | 13/158 | 0.6 (0.3–1.1) | 0.5 (0.3–1.1) | 13/116 | 1.0 (0.5–2.1) | 1.1 (0.5–2.2) |
| Northern Europe | 67/527 | 1.0 | 1.0 | 37/410 | 1.0 | 1.0 |
| Eastern Europe | 35/305 | 0.7 (0.4–1.2) | 0.7 (0.4–1.2) | 22/230 | 0.9 (0.5–1.6) | 0.8 (0.4–1.5) |
| Southern Europe | 13/349 | 0.3 (0.1–0.5) | 0.2 (0.1–0.5) | 27/249 | 1.1 (0.6–1.9) | 1.2 (0.7–2.1) |
| Western Europe | 7/81 | 0.6 (0.2–1.4) | 0.6 (0.2–1.5) | 5/63 | 0.7 (0.3–2.0) | 0.8 (0.3–2.1) |
| Time since mother's immigration to Sweden in relation to the child's birth | ||||||
| ≥15 years before birth | 30/457 | 1.0 | 1.0 | 38/356 | 1.0 | 1.0 |
| 10–14 years before birth | 39/579 | 1.1 (0.6–1.9) | 1.1 (0.6–1.8) | 51/413 | 1.2 (0.7–1.9) | 1.2 (0.7–1.9) |
| 5–9 years before birth | 74/970 | 1.5 (0.9–2.5) | 1.5 (0.9–2.5) | 108/733 | 1.2 (0.8–1.8) | 1.1 (0.7–1.8) |
| 1–4 years before birth | 82/1284 | 1.5 (0.9–2.4) | 1.4 (0.9–2.4) | 149/966 | 1.4 (0.9–2.1) | 1.4 (0.9–2.1) |
| Migrated in the year before birth | 33/454 | 1.7 (0.9–3.0) | 1.7 (0.9–3.0) | 65/333 | 1.8 (1.1–2.9) | 1.9 (1.1–3.1) |
| Migrated within 1 year after birth | 6/138 | 1.0 (0.4–2.6) | 1.0 (0.4–2.6) | 19/102 | 1.2 (0.6–2.4) | 1.3 (0.7–2.5) |
| 1–4 years after birth | 23/437 | 1.3 (0.7–2.4) | 1.3 (0.7–2.5) | 34/334 | 0.9 (0.5–1.6) | 1 (0.6–1.7) |
| ≥5 years after birth | 9/514 | 0.5 (0.2–1.2) | 0.5 (0.2–1.2) | 19/344 | 0.6 (0.3–1.2) | 0.7 (0.4–1.3) |
N/A, not applicable.
a Mother's region of birth and time since immigration in relation to child birth mutually adjusted.
b Additionally adjusted for maternal and paternal age and family disposable income at child's birth or in early life, as applicable.
c Countries contributing the largest number of cases in each subregion being (when applicable): Northern Africa - Morocco; Eastern Africa - Somalia and Ethiopia; Latin America and the Caribbean - Chile; Southern Asia - Iran; Western Asia - Iraq and Turkey; Northern Europe - Finland; Eastern Europe - Poland; Southern Europe - Former Yugoslavia.
effect on the risk of autism in the absence of maternal migration. Reference Keen, Reid and Arnone7 Studies from the USA have reported both elevated Reference Croen, Grether and Selvin13 and reduced 3 risks of autism in non-Hispanic Black and Hispanic children compared with White children, and provided some evidence that Black ethnicity may be linked to autism with, but not without, comorbid intellectual disability. Reference Bhasin and Schendel29 Further research is required, but the above evidence suggests that factors beyond ethnicity may be important in the relationship between migration and low-functioning autism.
In recent decades, many non-European migrants to Sweden have been asylum seekers, often migrating under exceptionally stressful circumstances and often facing social disadvantages both in the home country and during resettlement. To try to capture this dimension of the migration experience we studied whether the association between migration and autism spectrum disorder varied according to the human development index of the maternal country of birth, and found increasing risks of low-functioning autism with decreasing levels on the human development index.
One key and entirely novel finding of this study was that the risk of low-functioning autism varied with the timing of maternal migration. The risk of low-functioning autism appeared to be highest when migration occurred in the year before birth. This result is important, since it provides further evidence against ethnicity or case ascertainment differences being the main explanations of the parental migration–low-functioning autism association. Furthermore, it indicates that environmental, and hence possibly preventable, factors associated with a stressful parental migration process and acting in utero may be implicated in the aetiology of low-functioning autism.
Although we were unable to study many potential causal mechanisms directly, we investigated whether the increased risk of low-functioning autism in migrant children was explained by obstetric complications, parental age or family disposable income. Since we did not have access to obstetric data on children born abroad, these analyses were conducted in the sample of children born in Sweden. Apart from income, consideration of which may have comprised an over-adjustment since low income was almost always a feature of families originating from regions with a low human development index, these factors explained little of the observed associations. Instead, our results are compatible with the ‘maternal stress theory’. Reference Kinney, Munir, Crowley and Miller30
Maternal stress during pregnancy is a proposed risk factor for neuropsychiatric disorders in offspring, Reference Khashan, Abel, McNamee, Pedersen, Webb and Baker31,Reference Beydoun and Saftlas32 perhaps via impairments in foetal neurodevelopment due to dysregulation of the hypothalamic–pituitary–adrenal axis or epigenetic mechanisms. There is emerging evidence this may be applicable to autism, Reference Kinney, Munir, Crowley and Miller30 but further confirmatory research is needed.
Several other hypotheses have also been conceptualised for the role of migration in impaired neurodevelopment and may underlie our findings, but have yet to be rigorously tested. These include maternal vitamin D deficiency, Reference Keen, Reid and Arnone7 poor maternal nutrition, Reference Barak, Ring, Sulkes, Gabbay and Elizur33 and early life infections. Reference Morgan, Charalambides, Hutchinson and Murray34 These theories have also been posited for the effect of migration on psychotic disorders such as schizophrenia, but despite several lines of enquiry for over 40 years, the mechanisms behind these observed associations are unclear. Reference Bourque, van der Ven and Malla17,Reference Morgan, Charalambides, Hutchinson and Murray34
Reduced risk of high-functioning autism in children of migrant parents
Overall, the increased risk of low-functioning autism among migrants was balanced out by a decreased risk of high-functioning autism, such that migration status was not associated with autism spectrum disorder as a combined category. One intuitive explanation of this finding is misclassification of high-functioning individuals as low-functioning, due to inter-ethnic bias in diagnostic procedures related to language barriers, cultural misunderstanding, prejudice or differential properties of diagnostic instruments. This explanation is not, however, supported by closer examination of the association between migration status and low-functioning/high-functioning autism status as (a) high-functioning autism was also less common in children to migrants from regions that had no elevated risk of low-functioning autism and (b) the risk of low-functioning autism peaked in children of mothers who migrated during pregnancy, whereas no similar trend with timing of migration was evident for high-functioning autism.
It is impossible to rule out discrete aetiological mechanisms leading to a true protective effect of migration on high-functioning autism, but we consider underdiagnosis of high-functioning autism in migrant children a more plausible explanation of our findings. Unlike intellectual disabilities associated with low-functioning autism, which may be easily recognised, the nuanced social deficits related to high-functioning autism in migrant populations may be missed or attributed to cultural differences. Also, a low perceived need for mental healthcare, stigma and lower awareness of service availability in migrant populations, Reference Fassaert, de Wit, Tuinebreijer, Verhoeff, Beekman and Dekker35,Reference Bradby, Varyani, Oglethorpe, Raine, White and Helen36 may lead to reduced help-seeking in the absence of overt developmental delays. Reference Begeer, Bouk, Boussaid, Terwogt and Koot37 The cross-cultural validity of assessment tools for autism is another area of future research, but whatever the reason for our results, they mirrored those of a smaller study in a different region of Sweden Reference Haglund and Kallen16 and provide enough evidence to suggest autism-spectrum disorder with and without intellectual disability should be studied separately.
Strengths and limitations
Our results must be interpreted in light of some limitations. In common with previous studies on this topic, our case ascertainment was based on service use; therefore it is impossible to tease out whether our findings are specific to development or detection of autism spectrum disorder. We were also unable to study whether the increased risk of low-functioning autism in migrants is unique to autism or reflects risk factors for intellectual disability in general. We also did not have information on current autism spectrum disorder diagnostic subtypes, although it should be noted that our strategy of treating autism spectrum disorder as a single group stratified by comorbid intellectual disability is supported by epidemiological evidence and reflects and an approach proposed by the DSM-5 work group for future autism spectrum disorder classification. Reference Szatmari, White and Merikangas19,Reference Witwer and Lecavalier38
The strengths of our study include its large sample and population-based design ensuring high external validity. The universal and free system of mandatory child development assessments in Stockholm County makes it likely that a large proportion of individuals with at least severe autism in the community would have been identified and diagnosed. Furthermore, our multisource case ascertainment, using registries covering all pathways of autism care, warrants that we captured the majority of diagnosed individuals. Furthermore, our validation studies indicated that the case ascertainment had high sensitivity as well as specificity. This is an advantage as few studies use multisource case ascertainment approaches, and often rely on hospital discharge or healthcare records. A majority of children with autism may not have special healthcare needs that require hospital admission (instead more often requiring educational or social interventions).
Implications
In conclusion, our findings suggest that environmental factors associated with migration and acting in utero may contribute substantially to the risk of autism with comorbid intellectual disability. They also indicate that high-functioning autism may be underdiagnosed in children of migrant parents. Risk factors for low- and high-functioning autism may be markedly different, implying that these diagnostic subgroups should be studied separately. Migration during pregnancy could entail fetal risks, and policy measures to ensure comprehensive antenatal care for immigrant families from low- and middle-income countries should be a priority.
Funding
The Stockholm County Council, the Swedish Council for Working Life and Social Research (grant no. 2007-2064). D.R. is supported by a clinical lecturer award funded by the Severn Deanery, Bristol, UK.







eLetters
No eLetters have been published for this article.