


Law Schools are now required to provide education to law students on bias, cross-cultural competency, and racism under ABA Standard 303(c).1 Law clinics, with their social justice orientation, have long taught about structural causes of bias and oppression and ways to intervene at system levels to prevent problems. Medical legal partnership clinics, benefiting from interdisciplinary curriculum, have done so by employing concepts from social work and health science programs on structural competency.Reference Connolly and Lackey2 Due to the need to sift and winnow through multiple disciplines, creating interdisciplinary curriculum can have an added layer of complexity. Charity Scott was a champion for interdisciplinary approaches and health justice teaching. She was a mentor for law teachers pushing the boundaries to incorporate learnings from other disciplines into law teaching, despite (or maybe because) of pushback from law school administration.Reference Scott3 Opportunities like the Public Health Law Faculty Fellowship conceived of and led by Charity Scott, create space, and offer essential resources to support such valuable curriculum development. That experience a decade ago was eye-opening, affirming, revitalizing, and substantively rigorous.
As a teacher in an interdisciplinary field — health justice — and director of a medical legal partnership (MLP) Charity’s vision and mentorship has been an essential elixir. Due to my positioning, I have benefited from the bounty of material available from disciplines outside of law. So, when the requirement to provide education to law students on bias, cross-cultural competency, and racism under ABA Standard 303(c) was implemented, I used it as an opportunity to take a hard look at our current MLP curriculum, what I thought we were doing well, what needed much more work. I then surveyed available interdisciplinary materials to make it better. This article describes that journey, a journey that feels reminiscent of my time a decade ago in the fellowship developing curriculum in public health law. Requiring deep reflection, I described that experience as both “unpleasant” and “emboldening.”Reference Davis4
Indeed, the ABA standards serve as a catalyst for most law faculty to continue to explore how to best teach on politicized topics that are essential to effective lawyering and being a human in our complex and divisive world. While the requirement does not prescribe the form or content of the education, it does require that students participate in a substantial activity to reinforce both the skill of cultural competency and their obligation to work to eliminate racism in the legal profession. It ties part of this requirement to clinical courses.5 The mandate is part of a wider anti-racism movement in legal education and formalizes the inclusion, justice, and belonging teaching already done in many clinics.6 In particular, medical-legal partnerships (MLP) & health justice clinics can serve as a model for teaching cultural competency and bias through a structural competency lens. In this article I will use MLP to refer to all interdisciplinary service-learning opportunities teaching health justice substantive knowledge and approaches at the individual, community, and policy levels.
Charity Scott was a champion for interdisciplinary approaches and health justice teaching. She was a mentor for law teachers pushing the boundaries to incorporate learnings from other disciplines into law teaching, despite (or maybe because) of pushback from law school administration. Opportunities like the Public Health Law Faculty Fellowship conceived of and led by Charity Scott, create space, and offer essential resources to support such valuable curriculum development. That experience a decade ago was eye-opening, affirming, revitalizing, and substantively rigorous.
Part one will explore the new ABA requirement, the context of this mandate, and the value of focusing on structural competency in pedagogical approaches. Part two will describe the benefits and limitations of MLP and health justice interdisciplinary curriculum to address this call. Drawing on my own teaching and recent exploration, part three will offer an introduction to key concepts relevant to structural competency from the MLP, public health and health sciences literature. Further, it will describe some adaptable class exercises and available resources for teaching and further investigation. The conclusion will offer a reflection on responding to this call to action through an interdisciplinary-influenced structural lens as a fitting way to honor Charity Scott’s legacy.
I. ABA Requirement 303(c), Contextual Considerations, and Structural Competency as a Unifying Paradigm
In February 2022, the American Bar Association adopted Standard 303(c) requiring law schools to provide law students with education on “bias, cross-cultural competency, and racism.”7 By design the requirement did not offer a definitive definition of these concepts, nor a directive of how to implement the mandate beyond the expectation to introduce concepts in orientation and include subsequent teaching connected to law clinics or field placements.8
Teaching on these topics, especially racism, can cause high anxiety.Reference Greenberg9 Students understandably have high expectations for these conversations. Both consciously and unconsciously, some faculty (especially in public law schools) feel external pressures on curriculum despite academic freedom and first amendment protections as state legislatures cut, or threaten to cut, funding to Diversity, Equity, and Inclusion initiatives. An external environment with politicization, censoring, and even job loss, can serve to effectively extinguish vital conversations.Reference Taite and Boothe10 Internal (personal) barriers to teaching about racism has been thoughtfully covered by others.Reference Samuel-Siegel11
Bias, cross-cultural competency, and racism are independently significant issues to teach effectively. Teaching them collectively well requires at minimum sufficient knowledge, training, and experience. Learning from disciplines with existing expectations to teach these topics provides a head start. In this way, the benefit of interdisciplinary teaching is the bounty of frameworks and materials available. Having spent my entire academic career in interdisciplinary spaces, I have reaped this richness at the same time I have participated in parallel conversations using distinct concepts. Teaching and learning effectively with interdisciplinary concepts in interdisciplinary spaces requires a shared language. As will be explored in Part III, systems thinking offers a guide to do this well. A main tenet of systems thinking is that the frameworks make mental models explicit to facilitate problem-solving.Reference Stroh12 Fulsomely understanding concepts that have taken root in extra-law disciplines increases both collaboration effectiveness and problem-solving. The bounty of interdisciplinary concepts thus requires learning communities to pause to confirm shared language and core concepts. This practice of pausing and confirming understanding also supports community-building and a virtuous cycle reinforcing inclusive, intentional learning communities.
The ABA’s silence on what is meant by bias, cross-cultural competency and racism means that these topics may be taught as individual traits or systemic matters to be handled at institutional, community, and policy/law levels. With an emphasis on skills, it is possible that some clinics or field placement seminars will focus primarily on individual lawyer and client relationships. Yet, the 2020 catalytic cultural reckoning regarding the U.S. history and present of racial injustice spurred by multiple killings by police of unarmed black people and the corresponding Black Lives Matter social movement, amplified racist structures and systems. This mainstreaming of long-standing racial inequities led many law faculty to engage in critical reflection on how to address structural racism in their courses.Reference Bliss, Brooks and Huq13 Many clinical faculty have been teaching through a structural lens for decades prior to the cultural reckoning and ABA mandate.Reference Ogilvy14 For example, clinics were already employing a law in action approach which examines the role of law itself as a structural driver. It encourages learners to inquire: “how does the law impact people experiencing oppression?” Is it perpetuating power imbalances? Mediating discrimination? Acting neutrally with a biased effect? What is the history and the status quo of how people and communities experience the legal issue they are facing? Reference Noonan and Davis15 Such an approach, however, was not usually sufficiently naming racist structures, as is addressed in Part II below.
In response to the ABA mandate, my law school’s DEI committee offered guidance on teaching cultural competency through a structural framework and invited colleagues to “address the compounding effects of multiple systems of oppression.” They reframed cultural competency as structural competency with their definition: “Understanding your own place in the existing legal/sociopolitical structure and being able to respond to others differently situated in the existing legal/sociopolitical structure.”Reference Tai16 This reframing accomplishes multiple objectives. First, it introduces structural competency as an expectation for UW-Madison Law School curriculum. Second, it addresses the critique that cultural competency, as an approach, “others folks in non-dominant cultures”17 and “reinforces reductive understanding of identity markers without a consideration of context.”Reference Donald, DasGupta, Metzl and Eckstrand18 In other words, it addresses the critique that cultural competency merely requires people to understand the basics about various cultural traditions. Structural competency as a replacement for cultural competency decenters the person performing the cultural competency skill and focuses the skill on broader societal structures and context. Lastly, a structural competency lens instead of cultural competency introduces the importance of situational awareness, and the corresponding necessity of structural humility. (See Table 1 for definitions of terms).
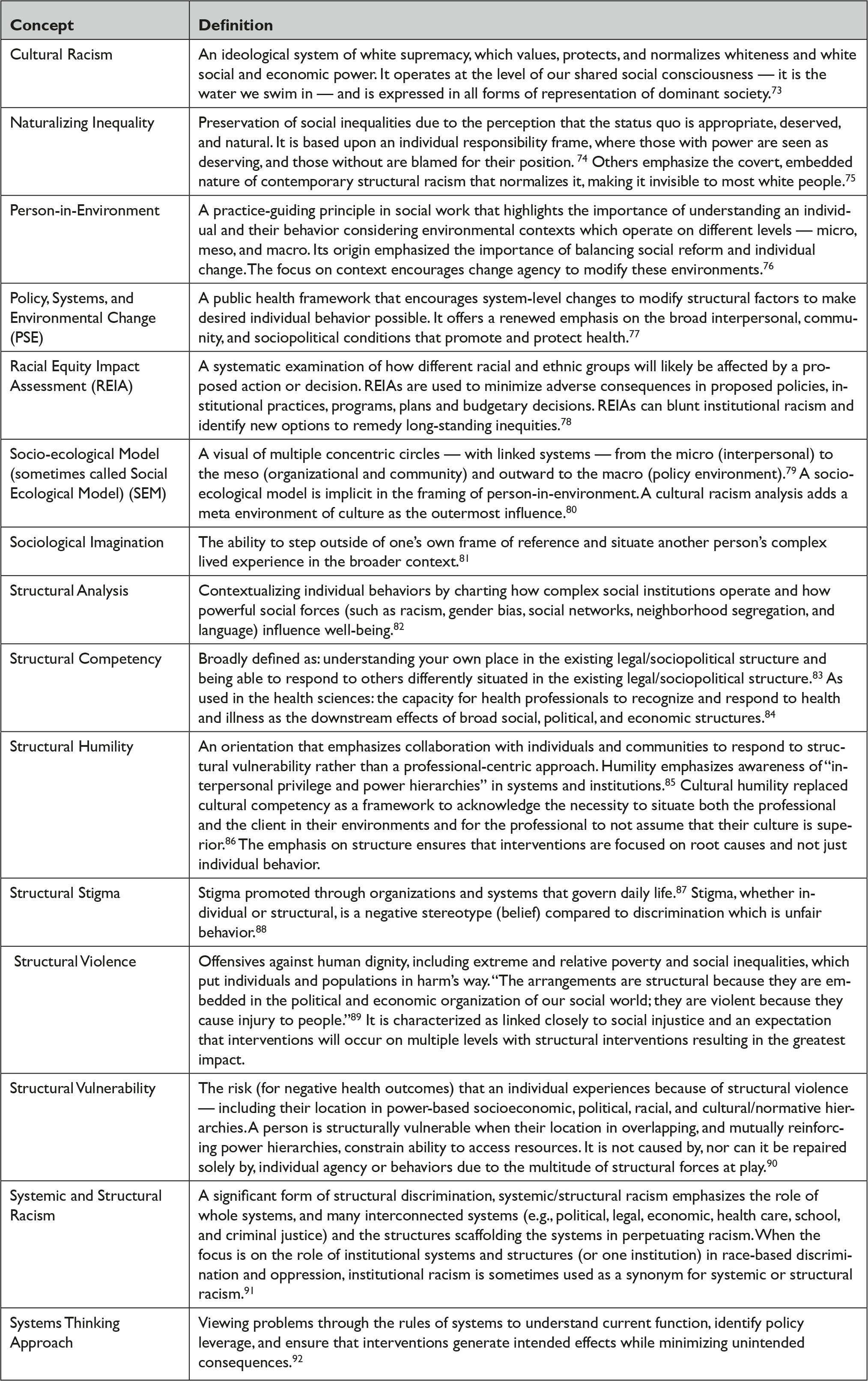
Table 1 Definitions of Key Concepts Explored in This ArticleReference Braveman, Arkin, Proctor, Kauh and Holm72
As someone who has relied on concepts from the health sciences literature, I needed to evaluate their definition in context of my understanding of structural competency from the medical-legal partnership perspective. Used there it was originally defined in 2014 as: “the trained ability to discern how a host of issues defined clinically as symptoms, attitudes, or diseases…also represent the downstream implications of a number of upstream decisions about such matters as health care and food delivery systems, zoning laws, urban and rural infrastructures, medicalization, or even about the very definitions of illness and health.”Reference Metzl and Hansen19 This original definition sees structural competency as the skill to connect social determinants of health (e.g. upstream drivers) to individual health experiences. The original authors declare that structural competency includes five components: recognizing the influence of structures on 1) individual health and 2) healthcare (including existing implicit bias frameworks); 3) understanding culture in structural terms; 4) responding to structures both in and outside of healthcare environments; and 5) structural humility.20 In the definition, structural humility is more implicit than explicit in the concept of having “the trained ability to discern.” The importance of action — responding — is emphasized in a follow-up article that notes that structural competency calls upon providers to “mobilize medical expertise and authority for the betterment of clinical and extraclinical systems.”Reference Metzl and Petty21 Other scholars streamlined this definition in 2020 to: “the capacity for health professionals to recognize and respond to health and illness as the downstream effects of broad social, political, and economic structures.”Reference Neff, Holmes, Knight, Strong, Thompson-Lastad, McGuinness, Duncan, Saxena, Harvey, Langford, Carey-Simms, Minahan, Satterwhite, Ruppel, Lee, Walkover, De Avila, Lewis, Matthews and Nelson22 In medical-legal partnership parlance, structural competency recognizes how policy interventions addressing structural barriers can prevent or resolve health issues for the patient.Reference Tobin-Tyler23
As will be described in section III below, my colleagues’ definition of structural competency has challenged me to amplify the inclusion of cultural positioning into my teaching about systems and structures. It has reinforced my use of sociology, social work and public health frameworks that situate people in these systems and to have students deeply reflect on their own positioning.
II. Benefits and Critiques of MLP Curriculum
Health justice is a multisector movement for structural change to ensure that all people can be as healthy as possible.Reference Tobin-Tyler and Teitelbaum24 As a pedagogical approach, it is strongly linked with social justice education (SJE) which is an interdisciplinary conceptual framework for analyzing oppression and a set of pedagogical principles and practices.Reference Adams, Bell, Goodman, Shlasko, Briggs and Pacheco25 With their patient-to-policy framework, medical-legal partnerships have focused on structural and system interventions to prevent and solve problems in addition to the individual client who walks in the door.26 By analyzing how the patient/client seeking advocacy/legal services is harmed by factors and forces at multiple system levels — organizational, community, and legal structures — preventive interventions to benefit populations of patients can be undertaken to slow the flow of individual clients in need of legal help.Reference Kruse27
The focus is on structural change because such factors (laws, policies, practices, and systems) are primary drivers of health.28 A strength of MLP curriculum comes from their interdisciplinary roots. They employ concepts from social work and health science programs on structural competency and related concepts such as person-in-environment, structural interventions, systems thinking and more. Several MLP professors have vocalized their concern, however, that the goal of structural change in the original MLP framing did not focus on the root causes of racism. Reference Makhlouf29 These self-critiques highlight that the historical MLP model was a poverty intervention which would impact the effects of racism as a social determinant, but that they were not framed to address structural racism or disrupt power structures. In some cases, they may have perpetuated racist institutions by upholding and legitimizing the structures that maintain them. A neutral (colorblind) stance leaves inequitable systems that drive health inequities. Future law and health professionals must acknowledge how the professions they are entering have perpetuated structural racism. Recent publications suggest that today many MLPs are answering this call to center the dismantling of structural racism.Reference Cannon and Johnson30 Productive criticism is essential to better teaching and to achieving a more just world. My teaching has benefited from these calls to explicitly name and discuss structural racism at the heart of our health care systems.
III. Structural Competency Concepts and Teaching Tools from Interdisciplinary Sources
I have become a great advocate and practitioner of promoting interdisciplinary education, especially on issues of health and law … I believe the benefits are worth our hard efforts to overcome the challenges of interdisciplinary education.31
Charity ScottThis section explores key concepts relevant to structural competency from the MLP, public health and health sciences literature. Concepts discussed are defined in Table 1. The section also describes some adaptable class exercises and available resources for teaching and further exploration. Learning in my health justice clinic and courses is richest when students see themselves, their clients, and their colleagues in the systems they are struggling to navigate. When we ask: Why do systems function the way they do? In what way do I contribute to the current functioning of the (healthcare) system? How do I benefit from its excess and how am I hurt by its deprivation? Reference Bodenheimer and Grumbach32 How can I best advocate for transformation, and how is my advocacy and wellness interconnected with my colleagues and my clients’ advocacy? Answering these questions leads to recognition of structural inequities and motivates action to make structural change.
Answering these questions requires viewing health — yours, mine, our students’ and our clients’ — as individually embodied and structurally determined. This framing turns us away from blame and shame towards productive action.Reference Downey and Thompson-Lastad33 Use of the system thinkings truism “every system is perfectly designed to get the results it does” framing in my courses offers a subtle but effective cognitive frame for my students to view as essential their role in influencing that system. When it is a dysfunctional or broken system, somehow the task seems too daunting or outside our locus of control. But when we amplify the action of those in power to design and perpetuate the system for the benefit of some, a catalytic fire is sparked, and the invitation to be a change agent is seized. Inaction is understood as the explicit act of doing nothing — in being complicit in the reproduction of white supremacy.Reference Crowley34
Shared framing is key to fruitful learning and communication. Many siloed concepts have overlapping meanings and usage. A venn diagram of these relationships offers confirmation of their validity and value, and their intersectional nature and experience. It also reinforces the need for concepts to be defined at the beginning of lessons, so participants are having the same conversation. If I am using a socio-ecological model, my public health students know the Policy, Systems, and Environmental Change framework, my social work students know Person-in-Environment, and my law students have been introduced to structural competency in other classes - our ability to apply a structural analysis is compromised unless we pause to interpret our language for each other and come to shared understand. Even a course with only one discipline requires a shared understanding to engage in rich discussion. Intentionality around this shared understanding in the classroom models deliberation and trust necessary for effective problem-solving in the real world.35
To set the table about structural competency is to evaluate relevant systems and the constrained experience of living in them. Metzel and Roberts offer six concrete steps for health care professionals to increase the skill of structural competency and apply it meaningfully. 36 I have adapted these for lawyers in Figure 1. These included cross-cutting themes of curiosity about client’s lived experiences, searching for deeper causes, collaboration and learning across disciplines, creativity, and engaging in system advocacy. Existing structural competency curriculum introduces concepts like structural violence and structural vulnerability, naturalizing inequality, and structural humility (see Table 1 for definitions). Bourgois and authors offer a checklist to evaluate a person with lived experience’s (client’s) structural vulnerability across multiple domains.Reference Bourgois, Holmes, Sue and Quesada37 A structural vulnerability framing emphasizes the structural constraint on access to resources. In my undergraduate Community Resource Navigator Program (modeled after Health Leads and Community Health Worker interventions), we use a resource screener focused on individual social determinants of health needs. In my Health Justice Clinic, we engage in wide-open listening for the client to tell us their lived experience and frame their needs and gather additional information with classic demographic questions. Prioritizing listening is one method to ensure that the client’s goals are driving problem-solving. Coupling that with demographics that highlight possible barriers to solutions (e.g. employment, income, insurance), has been used to guide our advocacy for individual clients. The benefits of also using a structural vulnerability tool include increasing empathy skills and exploring deeper structural barriers of racism and cultural discrimination. It also provides a call to action to address issues in a systemic way along with individual client services.38 The structural vulnerability tool includes a category and questions about discrimination, a category about risk environments, and a prompt for the interviewer to reflect on how others will view the client’s presumed worthiness. Will others discount this person or believe they deserve their circumstances? Will others distrust them based upon their identity or lived experience? I plan to incorporate these questions and reflections in our programs going forward to reinforce that interventions — on all levels — must consider clients’ experiences of structural discrimination, bias, and racism.

Figure 1 Six Concrete Ways for Future Lawyers to Become More Structurally Competent93
For those of us seeking more material on structural competency, Neff and co-authors offer a comprehensive training including modules, slides, a workbook, facilitator guidelines, and supplemental reading.39 One module specifically focuses on how to respond to health-harming structures. Learners reported appreciating the curriculum’s focus on real-world application, its success in helping them “reframe” how they thought about patients, and reconnecting with their original reasons for pursuing medicine. These three motivations are shared by my law students debriefing their experience in the Health Justice Clinic, as it related to the legal profession. The Berkeley Collective offers handouts that include a case, exercises, key concept definitions, and adaptation of the Bourgois structural vulnerability checklist and a reading list.Reference Neff, Knight, Satterwhite, Nelson, Matthews and Holmes40 Paul and authors offer a case study of a patient facing an eviction who receives advocacy from a MLP and offer insights and analysis from a structural competency framework for each level of intervention — patient, institution, and population.Reference Paul, Curran and Tyler41
A main goal of structural competency is to understand how systems operate to impact clients and other stakeholders, including ourselves. A core skill of this competency is structural analysis. Structural analysis contextualizes patient’s individual health-related behaviors by charting how complex social institutions (such as hospitals, insurance plans, prisons, regulatory agencies, and religious organizations) operate and how powerful social forces (such as racism, gender bias, social networks, neighborhood segregation, and language) influence health.Reference Stonington, Holmes, Hansen, Greene, Wailoo, Malina, Morrissey, armer and Marmot42 Applying these skills requires a modern interpretation of sociological imagination, the ability to step outside of one’s own frame of reference and situate other person’s complex lived experience in the broader context; to build and exercise empathy. Engaging in sociological imagination is essential to avoid apathy and burnout, and to direct actions effectively.Reference Hirshfield43 Ghidina offers a class activity that invites sociology students to deconstruct two lived experience scenarios — the bullying of a transgender youth and the un/under employment of a working-class man. Students start by examining common explanations for these situations, watch videos of individuals discussing their experiences, and then have group discussions about structural causes and present on the discussion of these larger forces at play.Reference Ghidina44 I plan to use Ghidina’s class activity about the transgender youth in our new LGBTQ+ Health Justice Clinic section. We have been representing transgender and non-binary adults in insurance appeals of denials for medically recommended treatment for several years. Our students are zoomed in with clients supporting them as they face insurance denials and the corresponding delays in care. During the program’s pilot phase, we listened to students describe the learning they deem necessary to fully support their clients. It includes deeply understanding all the forces that make being transgender/non-binary in the United Stated today so taxing and dangerous. Students asked that we situate the barriers to care in the context of daily systemic barriers in multiple systems, institutions, and culture at large
A structural analysis can also be achieved by engaging in systems thinking. A systems thinking approach views problems through the rules of systems to understand current function, identify policy leverage, and ensure that interventions generate intended effects while minimizing unintended consequences.45 Systems thinking is a set of tools and strategies used for transformational change, including three cross-cutting themes: collaboration across disciplines, sectors and organizations; ongoing, iterative learning; and leadership focused on constant improvement.Reference Swanson, Cattaneo, Bradley, Chunharas, Atun, Abbas, Katsaliaki, Mustafee, Meier and Best46
I started teaching systems thinking in my core MPH course,Reference Davis, Park, Morgen, Khan, Donovan, Kaur and Hackett47 and then expanded to include introductions to these skills in my seperate macro advocacy skills classes for medical and law students. In my teaching I use videos and key concepts from the CDC’s Polaris Project. I particularly like the stock and flow diagrams about diabetes that first zoom in on treatment options and then zoom out to explore opportunities to prevent diabetes in the first place. In addition to introducing key tools like stock and flow diagrams, it also offers three, one hour-long webinars.48 I also use Systems Thinking for Social Change, an accessible practical guide to applying the skill of systems thinking and the Waters of Systems Change, systems change framework that emphasizes structural and implicit changes necessary for long-term transformation.49
My exploration uncovered other law faculty teaching about systems thinking. Pierson-Brown offers guidance and examples of process and mind mapping in a health law clinic addressing such issues as social safety nets, social security disability eligibility, and clients’ legal issues in context. These activities enable students to empathize with clients due to the totality of their experience and to distinguish between positive and normative outcomes of systems.Reference Pierson-Brown50 Sulentic offers an introduction to systems analysis as valuable to expand legal analysis beyond doctrine to include non-doctrinal factors essential to the application of law, showing how to helps to unpack the federal health insurance continuation law which operates in two independent, interlocking systems.Reference Sulentic51 Notably Stanford Law School faculty have also developed a free training on systems thinking, designed for policymakers and social entrepreneurs and offered through the business school.52
A key motivator for the structural analysis is to uncover embedded discrimination — especially system and structural racism, and all the forces that hold it in place. In orientation for my Health Justice Clinic, I facilitate self-reflection and a discussion using audio excerpts of the 1619 project’s episode on foundational racial health disparities and the Medicaid/Medicare at 50 video about the history of racism in healthcare coverage and facilities.53 Throughout the course we explore contemporary health-related racial disparities in access, treatment, and legal protections such as rates of Power of Attorney for Health Care completion. My research resurfaced old and uncovered new sources of applied materials from the health sciences field that could be adapted for law courses.54 The role of cultural racism as an amplifier of all forms of racism is also an essential concept for students to understand.Reference Michaels, Lan Hine, Nguyen, Gee and Allen55 For that reason, going forward, I plan to be more explicit about this concept when I introduce the socio-ecological model as a framing concept at the beginning of my courses.
I teach using a socio-ecological model to visually demonstrate, explore, and interrogate the multiple system factors and corresponding health advocacy opportunities related to our clients in the Health Justice Clinic. In my Advocacy for Populations course for medical students, students engage in a self-assessment of both the level(s) of advocacy they envision themselves engaged in and the corresponding skills they will need to cultivate to be effective.Reference Gilkey, Earp, French, Earp, French and Gilkey56 To address cultural racism, I will label the environment outside the socio-ecological model as culture to explore the impact of cultural racism and discrimination on clients and the possibilities for system changes that impact this transformational level. To further teach about cultural racism, I plan to use the excellent figures and tables from Micheals and co-authors article. One offers a visual representation of how cultural, structural, institutional racism reinforce each other, a second breaks down the constructs of cultural racism, and a third offers definitions and examples of racism in all its forms and the relationship to cultural racism.57
Oftentimes the best teaching is done by inviting guest experts into the classroom — for solo facilitation, or to serve as a co-facilitator, especially if the guest complements one’s own identities. Since the implicit (or hidden) curriculum — the context in which learning happens —can be more important than the explicit curriculum, inviting diverse voices into the classroom may be the most impactful lesson.
Another key concept related to the ABA 303(c) requirement is structural stigma. Stigma, whether individual or structural, is a negative stereotype — belief — compared to discrimination which is unfair behavior.58 Structural stigma has been linked to poor mental and physical health, social well-being and reduced educational achievement and income.Reference Hatzenbuehler and Link59 Laws can both be stigmatizing — due to their influence on societal operations and cultural norms — and be a powerful mediator of stigma if they are used to combat stigma. Because laws are infrequently amended or removed, their language is enduring, codifying stigma into day-to-day life.60 Examples relevant to my teaching include social security disability and legal experiences for non-binary and transgender individuals. The Social Security Administration defines and evaluates disability by standards that do not account for the complexity of illness experiences, and the bureaucratic experience at the application and recertification stages.Reference Whittle, Palar, Ranadive, Janet, Kushel and Weiser61 In the LGBTQ+ space, public and private insurance contracts, regulations, and law, regarding gender affirming care require one path of treatment, for example taking hormones prior to surgery, which may be medically contraindicated or simply personally inappropriate for non-binary individuals. Also problematic for LGBTQ+ clients are name change laws that require surgical transition, which relies on a bygone notion of the gender binary and what constitutes transition.
Excellent cases studies exist to facilitate classroom discussions about structural stigma. Whittle and authors’ results from their in-depth qualitative interviews with people living with HIV receiving public benefits offer rich first person accounts of lived experiences that punctuate the stigma experiences by beneficiaries interacting with these institutions.62 Metzel and Roberts offer three case studies that highlight the impact of structural sigma, socioeconomic factors, and politics on health disparities — including on the overdiagnosis of schizophrenia in African American men, the framing of nutritional insecurity as “noncompliant” unhealthy eating, and the criminalization of drug addiction in pregnant persons.63
Resources on cross-cutting issues relevant to ABA 303(c) are bountiful. Teaching for Diversity and Social Justice, now in its 4th edition, addresses racism and other structures of oppression, intersectionality, and offers design and facilitation guidance. The book’s companion website offers numerous activities and handouts.64 The Health Equity Curricular Toolkit, championed by the Health Equity Team of Family Medicine for America’s Health, provides a structured curricular tool to facilitate exploration of pressing questions around social determinants of health, vulnerable populations, and economics and policy. The toolkit covers structural competency, racism, oppression, power, bias, and intersectionality. It offers guidance on facilitation, definitions, and additional readings and audio-visual resources. Action-oriented, it provides activities and resources to promote skill-building to confront drivers of persistent and pervasive inequities.65
Many of these teaching tools are easily adaptable for medical legal partnerships in law school clinics and health-related courses. For those teaching in other experiential subject areas with a social justice focus, material can serve as a catalyst for finding more appropriate material or to adapt it as necessary. Within higher education, materials have been adapted for student affairs,Reference Whitman and Jayakumar66 and outside of academia for: government, non-profit organizations, and elected officials;Reference Scott, Andazola, Smith, Smith, de la Rosa and Michael67 and community-based activism (for migrants).Reference Piñones-Rivera, Liberona, Jiménez, Corona and García68 Oftentimes the best teaching is done by inviting guest experts into the classroom — for solo facilitation, or to serve as a co-facilitator, especially if the guest complements one’s own identities.69 Since the implicit (or hidden) curriculum — the context in which learning happens — can be more important than the explicit curriculum, inviting diverse voices into the classroom may be the most impactful lesson.70
Conclusion
The rich interdisciplinary materials available to teach about structural competency and the expectations to do so are major pieces of the puzzle to teach skills essential to lawyers in our times. Communities of learning, like the Public Health Law Faculty Fellowship championed by Charity Scott, which provide support, encouragement, and productive criticism, are also valuable pieces due to the structural forces dissuading innovative approaches. Those of us teaching in interdisciplinary clinics have often faced pressures to conform — to not innovate so much, to focus on what is best for our home discipline.Reference Connolly71 It is within this constraining environment, positioned in universities under a magnifying glass, nested in a hostile world that we are trying to do right by our students, communities, and society.
I hope others pick up Charity’s cause of championing interdisciplinary teaching.
No doubt, the approaches and teaching tools described within will not fit some circumstances and will become dated and replaced as our thinking and teaching continues to evolve. Let us not let perfection be the enemy of the good when the world, and our students, need us to lean in. Let us channel Charity Scott and celebrate the bounty of interdisciplinarity to teach fulsomely on bias, cross-cultural competency, and racism through a structural lens.
Acknowledgments
Thanks to Sylvia Caley, Lisa Radtke Bliss, and Sarah Orr for excellent edits and comments that made this a better piece. Thanks also to Steph Tai and the UW-Madison Law School DEI Committee for the inspiration to explore ways to teach about structural competency. Despite significant barriers, I continue to be the interdisciplinary teaching champion I am today in large part due to Charity Scott.
Note
The author has no conflicts of interest to disclose.



 Open access
Open access