INTRODUCTION
Lower respiratory tract infections (LRTI) are an important cause of morbidity and mortality worldwide [Reference McIntosh1]. There are two main clinical manifestations of severe LRTI in young children, which require hospital treatment: bronchiolitis, which is mainly caused by viral infections, most notably the respiratory syncytial virus (RSV) and pneumonia, which is associated with a large variety of different viral and bacterial pathogens [Reference Moore, Dagan and Madhi2]. Streptococcus pneumoniae remains an important cause of community-acquired pneumonia [Reference McIntosh1, Reference Toivonen3]. Immunisation programmes for children using pneumococcal conjugate vaccines (PCV) have been implemented in almost all countries to reduce the burden of severe pneumococcal infections [Reference Greenwood4, Reference Loharikar5]. Canada licensed the 7-valent PCV (PCV-7) in May 2001 and it was soon made available on the private market [Reference Poirier6]. Quebec started vaccinating high-risk children in October 2002 on a four-dose (3 + 1) schedule. A routine vaccination programme targeting all newborns (with a catch-up offered to all other children under 60 months) was started in December 2004 using a three-dose (2 + 1) schedule, keeping the four-dose schedule for high-risk children [Reference Crisinel7, Reference De Wals8]. The 10-valent PCV (PCV-10) replaced PCV-7 in 2009 and soon after, in 2011, the 13-valent vaccine (PCV-13) replaced PCV-10 with no catch-up in either instance [Reference Crisinel7, Reference De Wals8]. Since the beginning of the universal programme in December 2004, vaccine uptake has been high and stable over time, with >90% infants receiving the recommended number of doses [Reference Boulianne9].
The efficacy of PCV-7 and PCV-10 in preventing pneumonia was assessed in randomised clinical trials [Reference Black10–Reference Tregnaghi12]. In these studies, however, hospitalisation rates for pneumonia were not presented. Also, herd effect and serotype replacement which manifest in a population years after vaccine introduction cannot be observed in clinical trials [Reference Hausdorff and Hanage13]. Up to now, the evaluation of the effectiveness of PCV programmes has been mainly assessed in before-after comparisons focusing on the frequency of hospitalisations for all-cause of pneumonia and using administrative databases [Reference Grijalva and Griffin14–Reference Sigurdsson17].
The objective of the present study was to describe the epidemiology and burden of LRTI among children aged 6–59 months in Quebec from April 2000 to May 2015 using the provincial hospital discharge database, a period which covers the introduction of the routine PCV vaccination programme and changes in the type of vaccine used.
METHODS
Cases were retrospectively identified in Med-Echo, the hospital discharge database of the Quebec health insurance board (RAMQ). Med-Echo covers all admissions into acute care facilities in the province of Quebec. All hospitalisations for children from 6 to 59 months old with a date of admission between 1 April 2000 and 31 December 2014 with a main diagnosis of pneumonia, bronchiolitis, bronchitis, empyema, or pleurisy were retrieved (diagnostic codes are shown in online Supplementary Table S1). Hospitalisations in children less than 6 months of age were excluded because infections associated with perinatal causes are overwhelmingly present and no impact of pneumococcal vaccination would be expected in this age group. The immunisation status of patients is not recorded in the database. Years of observations start on 1 April and end on 31 March, as is done in Med-Echo. Yearly population estimates from the Quebec Statistics Institute were used to compute age-specific hospitalisation rates. The population of children from 6 to 59 months old in Quebec was 359 003 in 2000 and 401 574 in 2015.
All transfers and readmissions with an interval of 7 days or less after a previous discharge date were considered as one hospitalisation episode. Because of transfers 258 cases (0·4%) had two different relevant diagnoses (i.e. pneumonia and bronchiolitis). For this reason totals may equal slightly more than 100%. Cases without a personal identifier were removed. These patients did not have a medical insurance card at the time of hospitalisation, most likely because they were not residents of Quebec at the time, so it was impossible to identify any potential readmissions or transfers among these patients. Cases were considered to be severe if they were admitted to a paediatric intensive care unit (PICU). All LRTI hospitalisation episodes longer than 90 days were considered to be likely caused by errors in coding and were excluded from analyses.
All statistical analyses were realised with SAS 9·4 (SAS Institute, 2013). Cochran-Armitage tests were performed to assess trends in proportions. Poisson regressions were used to test for trends in yearly frequency rates. Secular trends in mean duration of hospitalisation were investigated by linear regression. Regression coefficients represent the absolute magnitude of change in the frequency rate by unit of time (1 year). Statistical significance was defined as probabilities <0·05 (bilateral tests). The study protocol was approved by the Research Ethics Board of the ‘Centre hospitalier universitaire de Québec’.
RESULTS
As seen in Table 1, 63 108 LRTI hospitalisation episodes were retained in the analysis: 37 156 (58·9%) diagnosed as pneumonia, 23 293 (36·9%) as bronchiolitis, 2741 (4·3%) as bronchitis and 176 (0·3%) as empyema and pleurisy combined. In children 6–23 months old, bronchiolitis was the most frequent diagnosis (n = 21979, 50·3%) followed by pneumonia (n = 19878, 45·9%). In children 24–59 months old, pneumonia (n = 17278, 87·3%) was more frequent than bronchiolitis (n = 1496, 7·6%). LRTI hospitalisations were more frequent among children aged 6–23 months (11·2/1000 person-years (p-y)) than among those aged 24–59 months (4·9/1000 p-y). Overall, 1226 (1·9%) of LRTI cases were admitted to PICU and the proportion was not influenced by age or diagnostic category with the exception of empyema or pleurisy. The mean duration of hospital stays was 3·6 days and was longest for empyema or pleurisy (12·8 days).
Table 1. Burden of LRTI hospitalisations among Quebec children 6–59 months of age hospitalised between 1 April 2000 and 31 December 2014

In total 704 (1·9%) of pneumonia cases were admitted to a PICU. Overall, this increased from 32 (1·3%) in 2000–01 to 40 (1·8%) in 2013–14 (P < 0·001). The mean duration of hospital stays for pneumonia was 3·8 days. In total 32641 (87·8%) of stays were less than 6 days. The mean stay for children admitted to a PICU with a primary diagnosis of pneumonia was 10·0 days, whereas those only admitted to a regular care unit stayed on average 3·6 days. Over the study period, the percentage of cases admitted to PICU for all LRTI, pneumonia and bronchiolitis increased non-significantly for those under 24 months of age and significantly for those aged 24–59 months (P < 0·04 for all).
Of the 23 293 cases of bronchiolitis, 21 797 (93·6%) occurred in infants 6–23 months old. For bronchiolitis, the incidence for children aged 6–59 months was 4·4/1000 p-y, while it was 12·2/1000 p-y for 6–23 month olds. The average hospital stay for bronchiolitis was 3·5 days and 435 (1·9%) patients hospitalised for bronchiolitis were admitted to a PICU. There were 2741 cases of bronchitis and 1777 (64·8%) of these were among 6–23 month olds. The incidence was 0·51/1000 p-y for all ages combined and 1·00/1000 p-y for 6–23 month olds.
The overall incidence of hospitalisation for empyema and pleurisy combined was 0·03/1000 p-y. It was also 0·03/1000 p-y for both age groups. A total of 33 (18·8%) of these cases were admitted into PICUs and the mean duration of stay was 12·8 days, 20·3 days for those admitted to a PICU; 11·1 days for those not. No significant trends in the incidence over time were observed for this group of patients with empyema/pleurisy (P = 0·4).
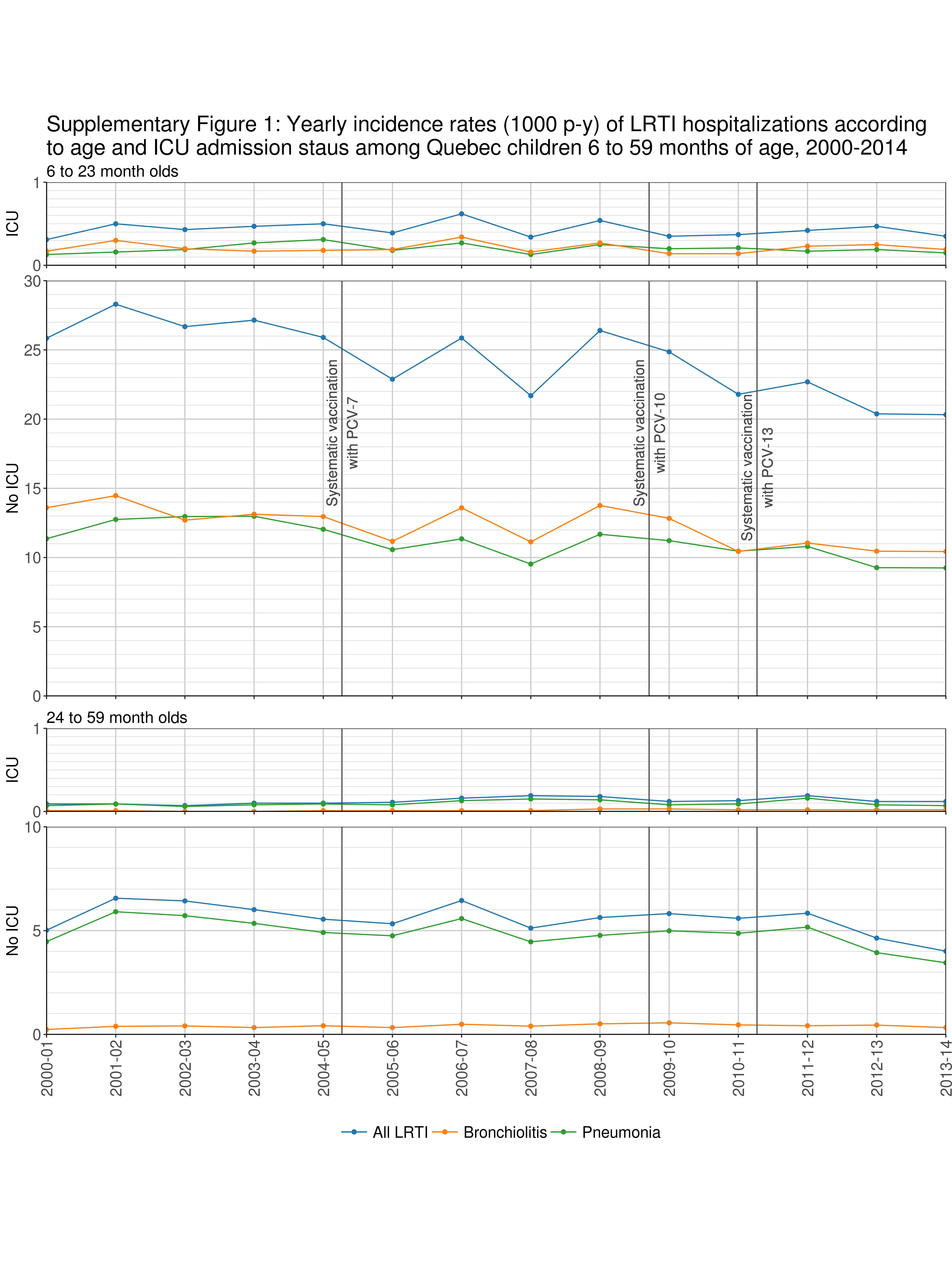
We observed a general trend of reduction in incidence of all LRTI (from 11·55/1000 p-y in 2000–2001 to 9·59/1000 in 2013–14, a 17·0% reduction). This was seen for all age groups and for all diagnostic categories (Figs 1 and 2; P < 0·001). These decreases were relatively steady over the whole study period and were initiated before PCV7 was introduced in the routine immunisation programme. This was also true of those patients admitted only to a standard paediatric unit (P < 0·001), but not for those admitted to a PICU (online Supplementary Figure S1). Diminishing trends were also found in both age groups (6–23 and 24–59 month olds) for pneumonia (minus 18·2% and 22·5%, respectively; P < 0·001) and for bronchiolitis in 6–23 month olds (minus 22·9%; P < 0·001). However, the incidence of bronchiolitis in patients 24–59 months old increased over time (P < 0·001). Between 2000 and 2014, the linear coefficient these trends were 0·9838 (95% CI: 0·9819–0·9857), 0·9818 (0·9793–0·9843) and 0·9871 (0·9840–0·9903) for all-LRTI, pneumonia and bronchiolitis, respectively, for all ages. For the 6–23 month olds, we found 0·9843 (0·9820–0·9867), 0·9846 (0·9811–0·9880) and 0·9847 (0·9814–0·9880) and for the 24–59 month olds, we found 0·9821 (0·9787–0·9855), 0·9784 (0·9748–0·9821) and 1·0206 (1·0077–1·0338), for the same categories.

Fig. 1. Yearly incidence (/1000 p-y) of LTRI hospitalisations according to age among Quebec children, 2000–2014.

Fig. 2. Yearly incidence (1000 p-y) of LTRI hospitalisations according to diagnostic category among Quebec children 6–59 months of age, 2000–2014.
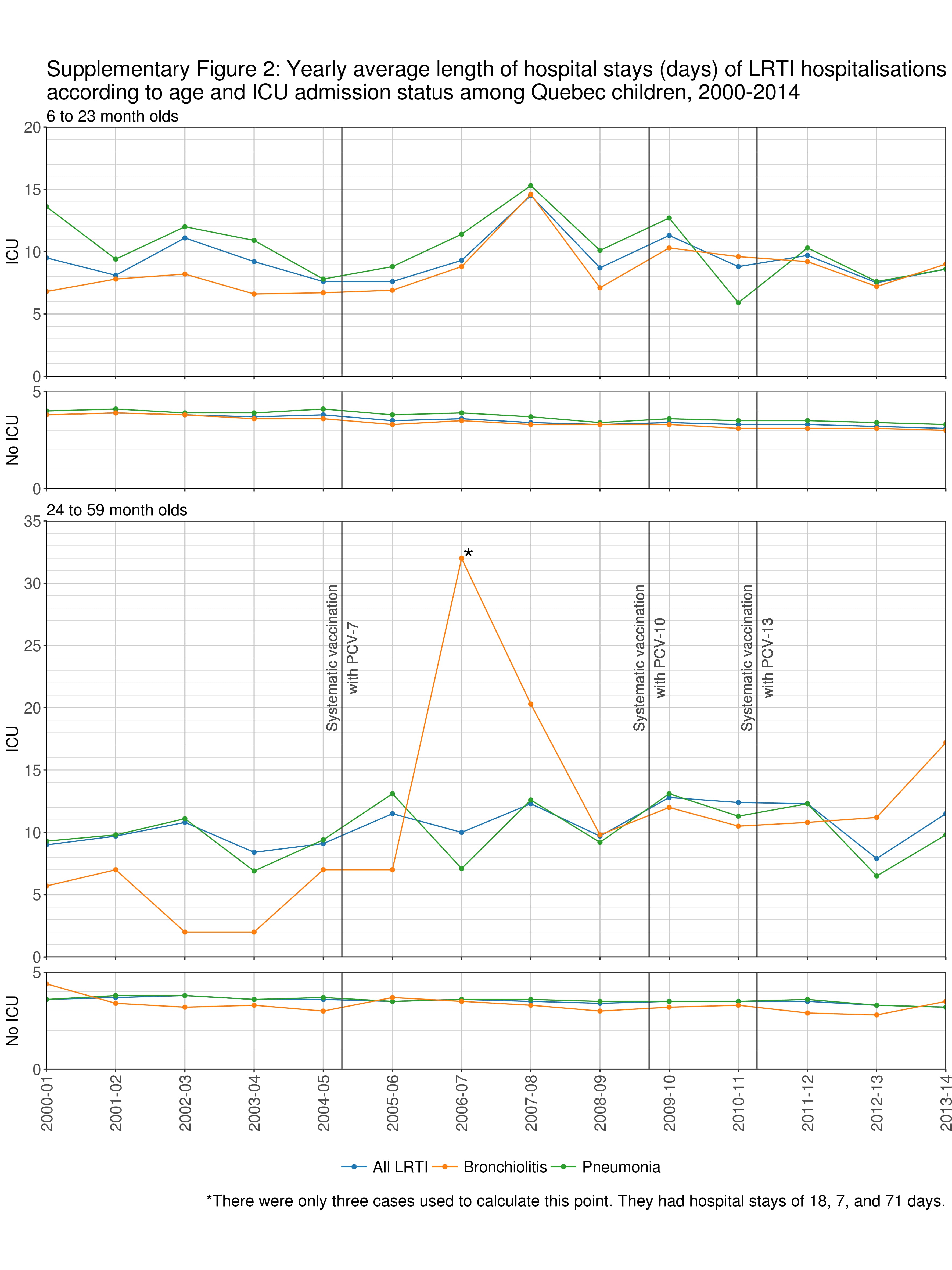
The mean duration of hospital stays for pneumonia decreased over the study period (P < 0·001). The mean duration of hospitalisation decreased for LRTI, pneumonia and bronchiolitis for both age groups for those not admitted to a PICU (P < 0·001 for all except children 24–59 months old with bronchiolitis where P = 0·06; online Supplementary Figure S2), but not for those admitted to a PICU.
The enforcement of stricter rules regarding the obligation of Quebec residents to produce a valid health insurance card in the emergency room may explain why 645 (2·0%) of the cases were missing a health insurance number by 1 April 2006, but only 431 (1·0%) after this date. This factor would have inflated hospitalisation rates as they were excluded from analysis, but not to the contrary. We nonetheless performed sensitivity analyses in order to gauge the importance of these cases without a health insurance card. When we included them, we found the incidence for all-LRTI, pneumonia and bronchiolitis to be only marginally affected: 12·01/1000 p-y vs. 11·83, 7·05 vs. 6·96 and 4·45 vs. 4·37, respectively. The slopes of the Poisson regressions for the rate by year remained statistically significant (P < 0·001): 0·9824 (CI 95% 0·9805–0·9843), 0·9807 (0·9782–0·9832), and 0·9851 (0·9819–0·9882), respectively.
DISCUSSION
Although we observed a global reduction in the incidence of LRTI, particularly in pneumonia, over the period of the study, it is not obvious that this is mainly due to the universal PCV vaccination programme in Quebec. There already existed a decreasing trend in the incidence before the introduction of the PCV7 programme and the steady rate of the observed decline is not congruent with the introduction of a vaccine or a change in vaccine type. This implies that there could be other factors apart from PCV vaccination to account for the reduction in the hospitalisation rates in LRTI in these children.
A potential environmental factor is the general decreasing trend in smoking rates in Quebec. Ried and collaborators estimated that the percentage of the total Quebec population who smoked declined from 28·2% to 17·1% between 2000 and 2013 [Reference Reid18]. Another factor could be air pollution. Tests done by Statistics Canada on data from the National Air Pollution Surveillance programme show decreases in the annual average concentration of sulphur dioxide, nitrogen dioxide and volatile organic compounds from 1999 to 2013 in Southern Quebec. However, they found no change in annual average concentrations of ozone and an increasing trend in the annual average concentrations of fine particulate matter during the same period [19].
Another important factor is a potential decrease in the circulation of respiratory viruses. Although, in the winter of 2008–09 Quebec was affected by the H1N1 pandemic, unpublished data from the Quebec Provincial Public Health Laboratory Surveillance Network has shown global decreases in the number of positive tests for influenza A and B and RSV over our study period (written communication, September 2016). The interpretation of this trend is difficult as there have been changes in the assay methodology and frequency of respiratory viral testing done in the province, with an increasing use of genome-amplification-based assays both in children and adults. A decrease in the circulation of RSV, however, would be congruent with the observed reduction in hospital admissions for bronchiolitis among 6–23 months old children in our study.
Other changes in clinical and coding practices may also play a role. On 1 April 2006, Med-Echo switched from using ICD-9 to ICD-10. However, as seen in the online Supplementary Table S1, the large diagnostic categories used in our study were not affected by this change.
During the study period, there have been major changes in microbiological investigations in hospitalised children in Quebec with an increasing use of antigen detection tests and PCR for respiratory viruses [Reference Zhou20]. Tests for bacterial infections (i.e. blood culture) have a poor sensitivity in children [Reference Wallihan and Ramilo21]. The hospital discharge database does not contain results of microbiology investigations and medical archivists use discharge summaries but not the results from laboratory or radiological investigations to code the main diagnosis. It was thus impossible in our study to assess the proportion of hospitalisations that were attributable to infections caused by S. pneumoniae. Serotyping has been performed in cases of invasive pneumococcal disease reported from sentinel laboratories since 1995. As observed in other countries [Reference Feikin22] vaccine-serotypes decreased and non-vaccine serotypes increased in all age groups following PCV7 use in children. The overall IPD rate decreased from 16·4/100 000 in 2005 to 10·8/100 000 in 2014. There was a substantial decrease (minus 41%) in the IPD rate in children less than 5 years of age but not in adults [Reference Lefebvre and Côté23].
As viral testing has increased and pneumococcal vaccine uptake has remained high, practitioners may have shifted from diagnosing patients with ambiguous cases with pneumonia to diagnosing them with bronchiolitis. This may potentially explain the reduction in the incidence rate of pneumonia as clinical and radiologic manifestations of the two diseases can be difficult to differentiate from each other in young children [Reference Klig and Chen24]. If this is the case, we may expect to see a shift in the ratio of the hospitalisation rate from pneumonia to bronchiolitis over time. However, although the ratio of the incidence of pneumonia and bronchiolitis in children 24–59 months old decreased throughout the study period, among children less than 24 months old it increased. The decrease in hospitalisations for pneumonia was more marked than the decrease in hospitalisations for bronchiolitis in children under 60 months old, whereas the hospitalisation rate for bronchiolitis increased slightly in those aged 24–59 months while it decreased in pneumonia hospitalisations.
Generally, the large majority of children seen in emergency rooms with a LRTI are not hospitalised. In a study in Washington State, the proportion of patients with suspected pneumonia that were hospitalised ranged from 12% in children less than 12 months of age to 4% in children 48–59 months age [Reference Nelson25]. One limitation of our study is that, in Quebec, valid population-based data on patients receiving ambulatory care were not available for the whole study period. The fact that hospitalisation rates and mean duration of hospital stays decreased for almost all diagnostic categories, but not for the most severe cases requiring intensive care is a clear indication of changes in the criteria for hospital admission, which may be associated with the decreasing use of parenteral antibiotics, the development of home intravenous therapy in children and the development of short-stay observation units in many hospitals [Reference Moore and Bortolussi26].
CONCLUSION
-
• Downward trends in hospitalisation rates for respiratory infection were more pronounced for all-cause pneumonia than for bronchiolitis and started before the introduction of PCV vaccination in Quebec.
-
• The reductions in the hospitalisation rate of all-cause pneumonia and bronchiolitis as well as in the duration of stay may be related to changes in clinical practice.
-
• There is little evidence that all-cause pneumonia, especially the most severe cases, decreased over the study period due to the introduction of PCVs.
There is little evidence that all-cause pneumonia decreased over the study period has been mainly caused by the introduction of PCVs, especially the most severe cases requiring intensive care. Reductions in the hospitalisation rate of all-cause pneumonia and bronchiolitis as well as in the duration of stays may be related to changes in clinical practice and possibly by other environmental factors. One cannot, however, exclude the hypothesis that PCVs contributed to the decrease in hospitalisations for pneumonia in Quebec, but the magnitude of this contribution is impossible to assess in a context of changes in practices. This study casts doubt on the over-simplistic interpretation of many ecological analyses of the implementation of PCV vaccination programmes as discussed in a recent analysis in Brazil [Reference Schuck-Paim27]. It implies that it is necessary to take into account other contextual factors, which are often not easy account for due to a lack of valid quantitative information. The limitations of administrative databases when analysing the effectiveness of PCV vaccination programmes should be more fully recognised.
SUPPLEMENTARY MATERIAL
The supplementary material for this article can be found at https://doi.org/10.1017/S0950268817001510
ACKNOWLEDGEMENTS
The authors thank Manale Ouakki for statistical advice. This work was supported by the Quebec Minister of Health and Social Services (le Ministère de la santé et des services sociaux du Québec).
DECLARATION OF INTEREST
Philippe De Wals has received research grants and reimbursement for travel expenses from GlaxoSmithKline, Pfizer and Novartis. Rodica Gilca has received research grants from Pfizer and Sanofi-Pasteur. The other authors do not have any commercial or other association that might pose a conflict of interest.