Stroke is the second main cause of mortality(Reference Johnson, Nguyen and Roth1) and the leading cause of adult disability worldwide(Reference Rajsic, Gothe and Borba2). The prevalence and burden of stroke remain high globally(Reference Johnson, Nguyen and Roth1), with the economic costs for post-stroke care keeping increasing due to the rapid rise of the population older than 65 years(Reference Ovbiagele, Goldstein and Higashida3). Primary prevention strategies are, therefore, needed to reduce the burden of stroke.
Fruits are rich in vitamins, minerals and polyphenols. Fruit consumption has been widely considered essential to prevent diseases and to promote health. A number of observational studies have shown that higher fruit intakes are associated with a lower risk of many chronic diseases, including hypertension(Reference Schwingshackl, Schwedhelm and Hoffmann4), diabetes(Reference Schwingshackl, Hoffmann and Lampousi5), CHD, stroke, cancer and all-cause mortality(Reference Aune, Giovannucci and Boffetta6). Among various nutrients in fruits, flavonoids have received increasing interest for their potential effects on human health. Flavonoids are proposed to possess cardio-protective mechanisms, including having antioxidant and anti-inflammatory effects, modulating lipid metabolism and platelet function and improving hypertension(Reference Weseler and Bast7). Such health effects indicate that flavonoid-rich fruits (FRF) may contribute to the prevention of stroke.
Although many prospective cohort studies have been carried out and shown that fruit consumptions may be protective against stroke(Reference Aune, Giovannucci and Boffetta6), the relationships of specific types of fruits with stroke risk were uncertain due to a limited number of available studies. For example, only one cohort study examined strawberries(Reference Sesso, Gaziano and Jenkins8), and two cohort studies examined grapes(Reference Hjartaker, Knudsen and Tretli9,Reference Lai, Threapleton and Day10) , which are popular fruits rich in flavonoids. Furthermore, evidence from Asian populations linking specific fruits consumption and stroke risk has been limited and controversial. For example, a Japanese cohort study showed a strong inverse relationship between the frequency of citrus fruit intake and total stroke and cerebral infarction risk(Reference Yamada, Hayasaka and Shibata11). In contrast, a Chinese cohort study found no association between intakes of total fruit, citrus fruit and stroke mortality(Reference Wang, Fan and Dawsey12).
Considering the limited and conflicting reports on specific fruits in Asian populations, we, therefore, aimed to examine the association of specific fruit consumption, in particular FRF consumption, with stroke risk in Japanese men and women.
Methods
Study design and population
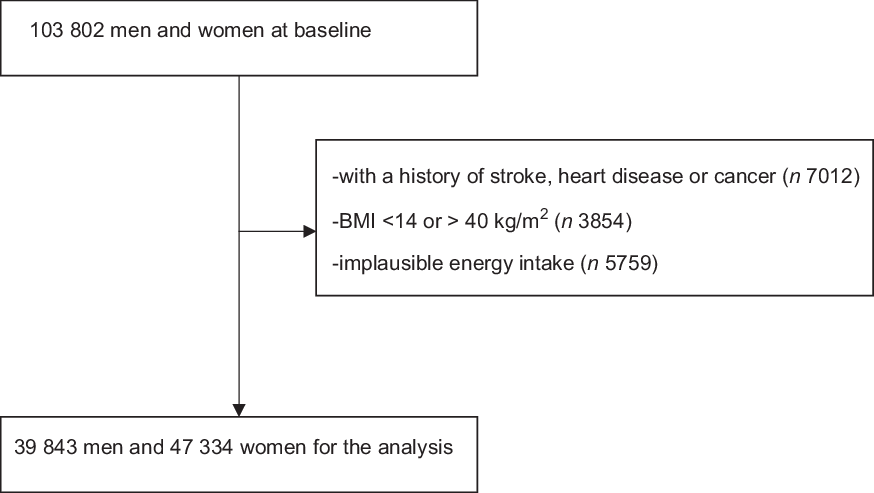
The Japan Public Health Center-based prospective study (JPHC study) is an ongoing prospective study with the primary aim to provide evidence for the prevention of CVD, cancer and other non-communicable diseases. The detailed study design has been reported previously(Reference Tsugane and Sawada13). The JPHC study was initiated in 1990 (cohort I) and 1993 (cohort II). In the cohort I, we recruited men and women aged 40–59 years from five public health centres, while in the cohort II, men and women aged 40–69 years were enrolled from the other six public health centres. We obtained socio-demographic information, self-rated physical health and mental health, disease history, smoking status, drinking status, physical activities and dietary habits through self-administered questionnaires at baseline and updated at follow-up surveys 5 and 10 years after the baseline survey. Dietary intake was assessed with a validated FFQ(Reference Ishihara, Sobue and Yamamoto14,Reference Sasaki, Matsumura and Ishihara15) . The FFQ was extended to 138 items at the 5-year follow-up survey. This extension made it possible to assess various food consumptions, and we treated 103 802 men and women responding to the 5-year follow-up survey as the baseline population for this analysis (response rate 76·2 %). We excluded men and women reporting a history of stroke, CVD or cancer at the baseline (n 7012), those having an extreme BMI (<14 or >40 kg/m2) (n 3854) and those reporting implausible energy intake (<800 or >3600 kcal/d) (n 5759). Ultimately, 87 177 men and women were eligible for the present analysis.
Dietary assessment
Dietary intakes were assessed using a semi-quantitative FFQ with 138 items. Participants were asked their intake frequencies of individual food items during the past 12 months. The FFQ included nine categories ranging from never to 7 or more times/d for major food items. Fruits in the FFQ included apples, oranges, other citruses, pears, strawberries, grapes, watermelons, melons, papayas, peaches, kiwifruits, pineapples, bananas and Japanese persimmons. Their flavonoid contents are listed in online Supplemental Table 1. Portion sizes of fruits ranged from 50 to 130 g. Apples, oranges, other citruses, pears, strawberries and grapes were defined as FRF according to their flavonoind contents(Reference McCullough, Peterson and Patel16). The remaining fruits were grouped as other fruits. Nutrient intakes were computed based on the Standard Table of Food Composition in Japan(17). A validity study examining the correlations between the FFQ and dietary records showed that the Spearman correlation coefficients of citrus fruits and other fruits were 0·48 and 0·51 for men and 0·36 and 0·41 for women(Reference Nanri, Shimazu and Ishihara18), respectively.
Covariate assessment
Data on age, sex, occupations, personal history of diseases, medication use, smoking status, drinking status and physical activities were obtained from a self-administrated questionnaire. BMI was calculated based on self-reported height and weight.
Identification of stroke incidence
The outcome of interest was the first incidence of stroke. The administrative districts of the JPHC cohort registered a total of seventy-eight major hospitals with the capability of treating patients from stroke. Medical records were reviewed to identify stroke cases by physicians, hospital workers or investigators who were blinded to participant’s responses to the baseline and follow-up surveys. Stroke cases were diagnosed based on the criteria of the National Survey of Stroke(Reference Robins and Baum19), specifically, a sudden or rapid occurrence of a focal, non-convulsive neurological deficit lasting for at least 24 h or until death. Information obtained from computed tomography scanning, MRI and autopsy was used to determine stroke subtypes (i.e. cerebral infarctions and haemorrhagic stroke).
Statistical analysis
The main exposure of interest was FRF consumption in this study. Because FRF intakes were considerably higher in women than that in men, all the analyses were stratified by sex. We calculated age-adjusted means and proportions of the population characteristics at the study baseline according to total FRF intake (quintiles). P for trend across groups use generalised linear models (linear regression). Person-years of follow-up were calculated from the date at enrolment until the date of stroke incidence, death, moving out from the study area or end of follow-up (31 December 2009 for cohort I and 31 December 2012 for cohort II), whichever came first. Cox proportional hazards regression model was used to compute hazard ratios for stroke incidence according to FRF consumption. The group of lowest consumption was treated as the reference group. All hazard ratios were adjusted for age at study enrolment. In multivariable model 2, we further adjusted for the following variables: study area, BMI (<18·5, 18·5–20·9, 21–22·9, 23–24·9, 25–29·9, ≥30 kg/m2 or missing), medication use for hypertension and hypercholesterolaemia (yes or no), history of diabetes (yes or no), alcohol use (never, 0–22·9, 23–45·9, 46–68·9, ≥69 g/d or missing), smoking status (never, past, current <1 or ≥1 pack/d or missing), sports level (never, 1–3 times/month, 1–2, 3–4, ≥5 times/week or missing) and occupation (unemployed, white-collar worker, blue-collar worker or other). In multivariable model 3, we further adjusted for dietary factors including coffee intake (never, 1–2, 3–6 cups/week, 1 or ≥2 cups/d), green tea intake (never, 1–2, 3–6 cups/week, 1, 2–3 or ≥4 cups/d) and quintile intakes of total energy, red meat, processed meat, seafood, soya foods and vegetables. Interaction analyses testing whether sex could modify the association between FRF consumption and stroke risk were performed by adding a product term of FRF consumption and sex in Cox regression models. Similar interaction analyses were conducted for age, BMI and smoking status. Trend tests were carried out by modelling FRF consumption as a continuous variable and assigning the median intake value of each group. The associations between specific FRF, including apples/pears, citrus fruits, strawberries and grapes, and stroke risk were also performed. Consumptions of strawberries and grapes were divided into quartiles because of relatively lower consumptions. In addition, we examined the association between flavonoid intakes from fruits and risk of stroke. Sensitivity analysis was performed by excluding cases diagnosed in the first 2 years of the follow-up, by excluding those with history of diabetes and by excluding adults those medication use for hypertension and hypercholesterolaemia. All analyses were performed using SAS software (version 9.4; SAS Institute Inc.). All P values were two-sided, and P value < 0·05 was considered as statistically significant.
Results
Table 1 shows the baseline characteristics of the study population according to FRF stratified by sex. Median FRF intakes were 9·1, 27·5, 57·4, 105·4 and 215·1 g/d for quintiles in men and were 19·0, 61·2, 108·2, 173·1 and 329·7 g/d for quintiles in women. Compared with men with lower FRF consumption, those with higher consumption were slightly older and more likely to be never smokers and never drinkers. Also, higher consumption of FRF was related to higher intakes of green tea, seafood, vegetables, soya food, other fruits and total energy. Similar results were found in women.
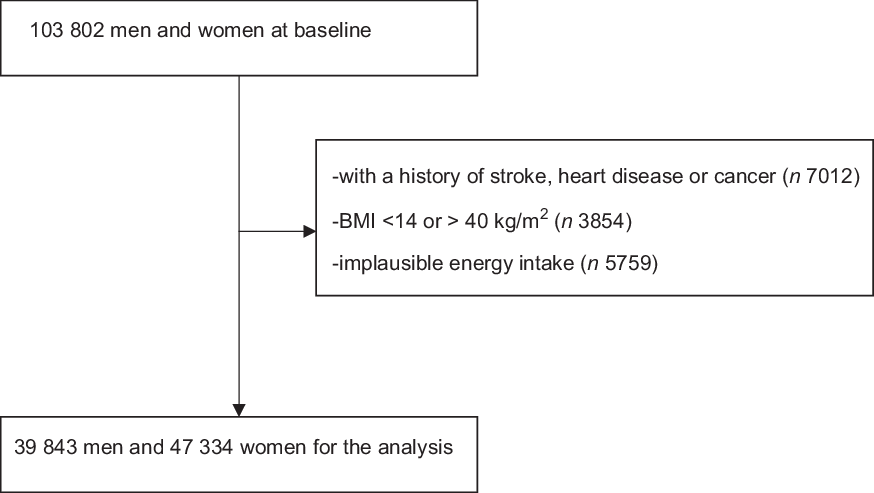
Fig. 1 Flow chart for participant selection.
Table 1. Sex-specific baseline characteristics according to flavonoid-rich fruit (FRF) intake*
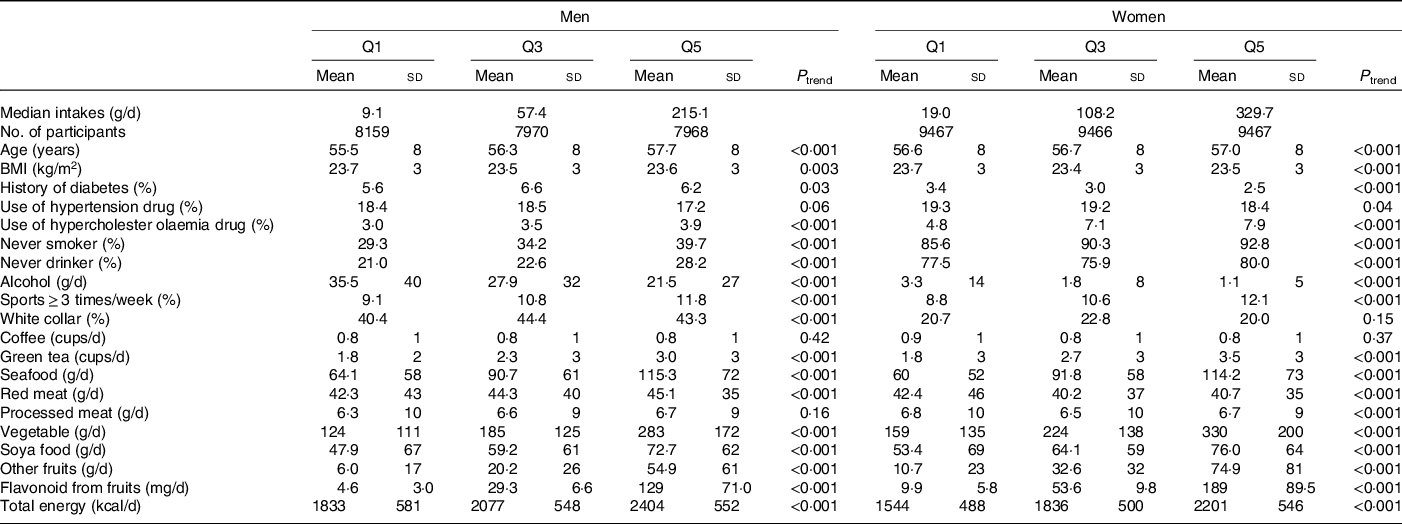
* Values are age-adjusted. Continuous variables are expressed as mean and sd and categorical variables are expressed as percentages.
During a mean of 13·1 years of follow-up, a total of 4091 incident strokes were documented, including 2557 cerebral infarctions, 1516 haemorrhagic strokes and eighteen unknown subtypes. In the age-adjusted model, men in the highest group of FRF consumption, compared with those in the lowest group, experienced a lower risk of developing stroke (Table 2). The association was attenuated but remained significant after further adjustment for sex, study area, BMI, medication use for hypertension and hypercholesterolaemia, diabetes history, occupation, drinking status, smoking status and sports level (model 2). Further adjustment for dietary factors including seafood, red meat, processed meat, soya food, green tea, coffee, vegetables and total energy led to a non-significant association (model 3). Table 3 shows the associations of FRF consumption with stroke risk in women. Women in the highest group of FRF consumption, compared with those in the lowest group, had a significantly lower risk of stroke in all three models. Furthermore, the association in women tended to be dose-dependent. However, sex did not significantly modify the association as indicated by the interaction analysis (P for interaction > 0·34 in all models). Similarly, age, BMI and smoking status did not modify the association (all P for interaction > 0·13 in all models).
Table 2. Intakes of flavonoid-rich fruits (FRF) and other fruits in relation to stroke risk in men
(Hazard ratios and 95 % confidence intervals)
* Model 1: adjusted for age.
† Model 2: adjusted further for study area, BMI, occupation, medication use for hypertension and hypercholesterolaemia, diabetes history, drinking status, smoking status and sports.
‡ Model 3: adjusted further for dietary intakes of seafood, red meat, processed meat, soya food, green tea, coffee, vegetables and total energy.
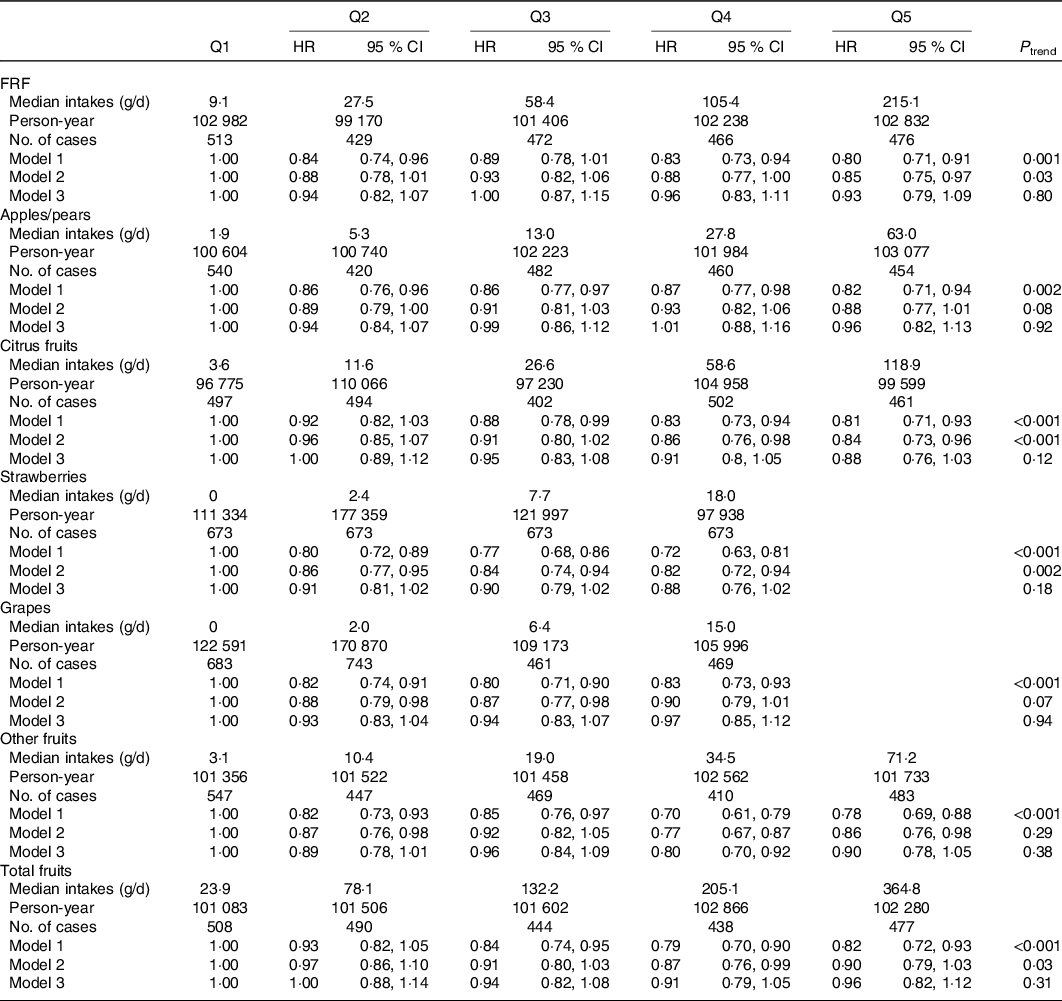
Table 3. Intakes of flavonoid-rich fruits (FRF) and other fruits in relation to stroke risk in women
(Hazard ratios and 95 % confidence intervals)
* Model 1: adjusted for age.
† Model 2: adjusted further for study area, BMI, occupation, medication use for hypertension and hypercholesterolaemia, diabetes history, drinking status, smoking status and sports.
‡ Model 3: adjusted further for dietary intakes of seafood, red meat, processed meat, soya food, green tea, coffee, vegetables and total energy.
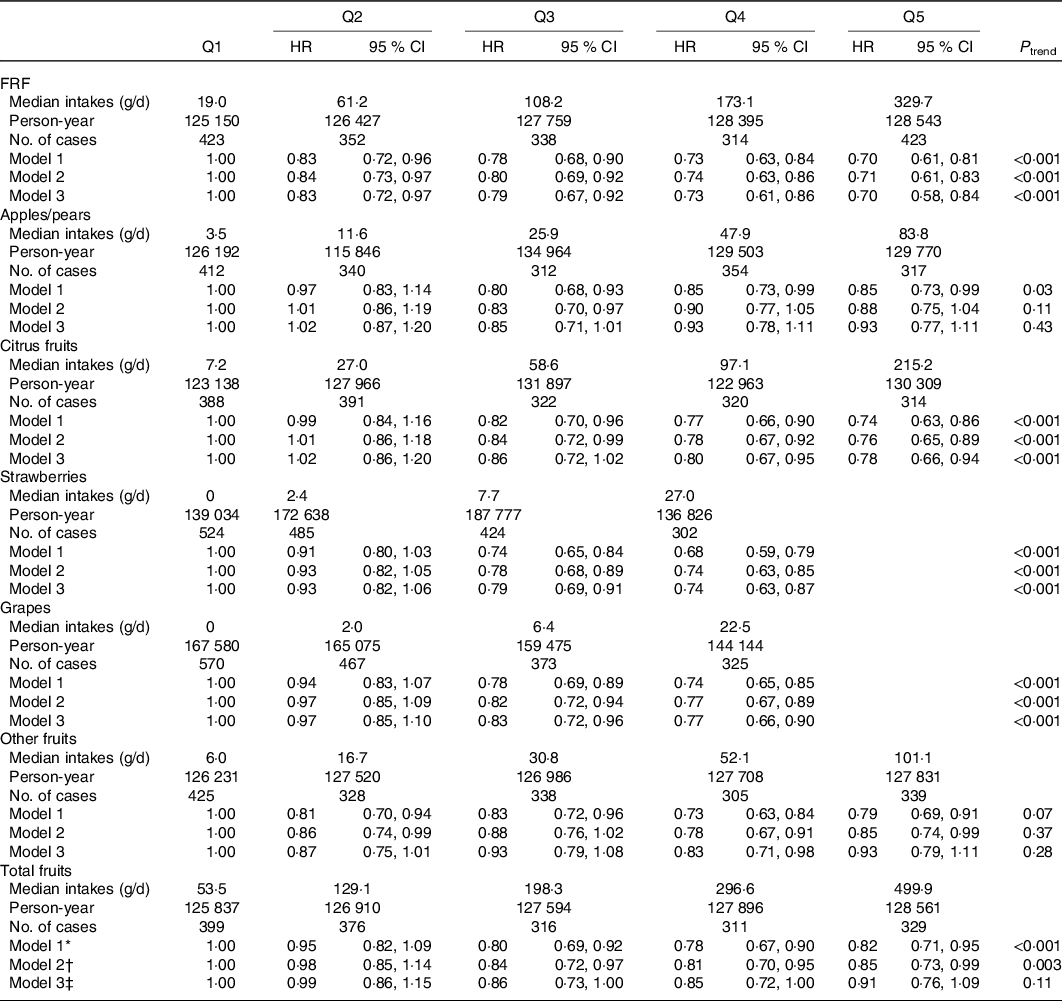
We next examined the associations for specific FRF: apples/pears, citrus fruits, strawberries and grapes. None of these fruits was associated with stroke risk in men. In women, inverse associations were found for citrus fruits, strawberries and grapes but not for apples/pears (Table 3). In addition, other fruit consumption was not related to stroke risk in either men or women. Additional analyses according to stroke subtypes yielded similar results as those for the total stroke (see online supplementary material, Supplemental Table 2).
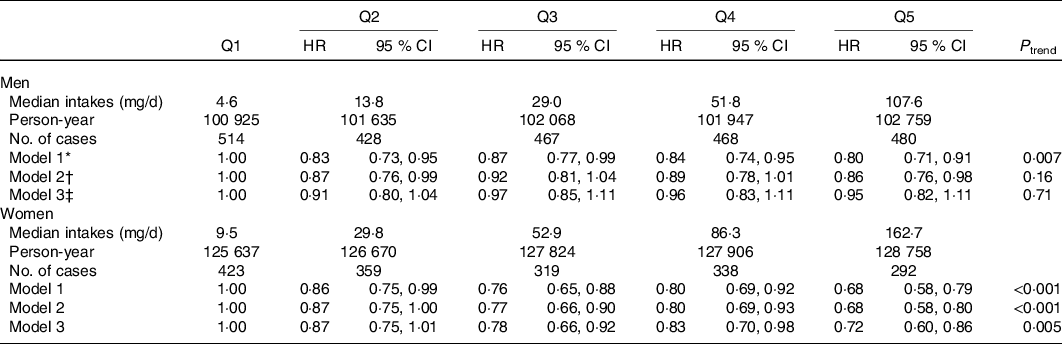
Furthermore, we examined the association between flavonoid intakes from fruits and risk of stroke among men and women (Table 4). The results were similar as our main analysis that higher flavonoid intakes from fruits were associated with a lower risk of stroke among women but not among men.
Table 4. Intakes of flavonoids from fruits in relation to stroke risk in men and women
(Hazard ratios and 95 % confidence intervals)
* Model 1: adjusted for age.
† Model 2: adjusted further for study area, BMI, occupation, medication use for hypertension and hypercholesterolaemia, diabetes history, drinking status, smoking status and sports.
‡ Model 3: adjusted further for dietary intakes of seafood, red meat, processed meat, soya food, green tea, coffee, vegetables and total energy.
Sensitivity analyses excluding cases diagnosed in the first 2 years of the follow-up, excluding those with history of diabetes and excluding those with medication use for hypertension and hypercholesterolaemia yielded similar results. The fully adjusted hazard ratios were from 0·86 (95 % CI 0·72, 1·04) to 0·92 (95 % CI 0·79, 1·09) for men and from 0·72 (95 % CI 0·60, 0·87) to 0·75 (95 % CI 0·59, 0·94) for women.
Discussion
In this prospective cohort study of Japanese populations, we found that higher intakes of FRF were associated with a decreased risk of developing stroke in women but not in men. For specific FRF, consumptions of citrus fruits, strawberries and grapes were found associated with lower stroke risk in women. For stroke subtypes, similar results were found as that for total stroke.
Consumptions of apples/pears were found to help reduce stroke risk in epidemiological studies(Reference Aune, Giovannucci and Boffetta6). However, the absence of such an association in the present study was not surprising. Peeling is common among Japanese when they consume apples or pears, while the peels of apples have been shown to contain much greater amount of total phenolic compounds, the ingredient responsible for the antioxidant activity, than the fleshes do(Reference Escarpa and Gonzalez20). With antioxidant-rich peels frequently discarded as a waste before eating, it may explain the null association between the consumption of apples/pears and stroke risk in the Japanese population.
An inverse association between citrus fruits and stroke risk in Japanese women was consistent with previous studies conducted in Western populations. In a Finnish cohort of 10 054 men and women, the incidence of cerebrovascular disease was lower in the group taking the dietary sources rich in flavonoids, orange (0·79; 95 % CI 0·64, 0·98; P = 0·02) and grapefruit (0·63; 95 % CI 0·36, 1·09; P = 0·07)(Reference Keli, Hertog and Feskens21). A prospective study among 69 622 women during 14 years of follow-up from the Nurses’ Health Study also indicated that women’s intake of citrus fruits/juices tended to be associated with a reduced risk for ischaemic stroke (RR = 0·90 and 95 % CI 0·77, 1·05)(Reference Cassidy, Rimm and O’Reilly22). A cohort study during a 24-year follow-up based on data from the Finnish Mobile Clinic Health Examination Survey on 3932 men and women aged 40–74 years indicated that the intake of citrus fruits helped to reduce the risks of both ischaemic stroke and intracerebral haemorrhage(Reference Mizrahi, Knekt and Montonen23). Another prospective cohort study of 54 506 men and women in the Danish showed the reduced risk of ischaemic stroke was most obvious in the highest quintiles of intake of citrus fruit(Reference Johnsen, Overvad and Stripp24).
We are aware of one observational cohort study which examined the association between strawberry intake and risk of stroke. In the Women’s Health Study of 38 176 women with a mean age of 54·4 years during a mean follow-up of 10·1 years, consuming strawberry ≥2 servings/week compared with having no strawberry consumption did not appear to affect risk of stroke (hazard ratio = 1·40; 95 % CI 0·86, 2·28) [10], which was inconsistent with our finding. The authors noted that the low level of strawberry consumption in their study may be responsible for the null association. In addition, the number of incident stroke cases was limited in their study (n 339). The differences in the levels of strawberry consumption and statistical power may have contributed to the inconsistent results between that study and ours.
In various animal experiments, polyphenols from grape powder, taken as a diet supplement, have been found to deter macrophage cholesterol accumulation, inhibit enhanced development of atherosclerosis(Reference Fuhrman, Volkova and Coleman25) and protect the brain against ischaemic damage(Reference Wang, Simonyi and Li26). However, previous studies in humans found no association between grape consumption and risk of stroke(Reference Lai, Threapleton and Day10,Reference Tognon, Lissner and Saebye27) . The inverse association of grape consumption with stroke risk in Japanese women warranted further research.
Flavonoids have been suggested to have potential effects on stroke prevention. The association between flavonoids intake and stroke risk has been evaluated in several epidemiological studies. The Zutphen Study, a cohort study examining 552 men aged 50–69 years for 15 years since 1970, showed that the habitual intake of flavonoids (the highest v. the lowest quartile of flavonoid intake (≥28·6 mg/d < 18·3 mg/d)) may protect against stroke (RR = 0·27; 95 % CI 0·11, 0·70)(Reference Keli, Hertog and Feskens21). The Finnish cohort on a sample of 10 054 participants showed that the flavonoid groups (flavonols, flavones and flavanones) were inversely associated with the incidence of cerebrovascular disease leading to hospitalisation or death(Reference Knekt, Kumpulainen and Jarvinen28). However, no association between total flavonoid intake and stroke mortality (P for trend = 0·83) was found in a prospective study on 34 492 postmenopausal women in Iowa over 10 years of follow-up(Reference Yochum, Kushi and Meyer29). In addition, the cohort study on 26 593 male smokers aged 50–69 years during a 6·1-year follow-up performed by the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study in Finland showed that dietary flavonols and flavones were not associated with risk for stroke in male smokers(Reference Hirvonen, Virtamo and Korhonen30). Recently, it was found that dietary flavonoid intake may be inversely associated with the risk of stroke in one meta-analysis of eleven prospective studies. In addition, it is indicated that a 100 mg/d increment in flavonoid intake led to a 9 % lower risk of stroke (RR 0·91; 95 % CI 0·77, 1·08) in a dose–response analysis(Reference Tang, Li and Zhang31).
The strengths of our study included a large sample size and a prospective population-based cohort design, which reduced the risk of selection and recall biases. However, our study also had limitations. First, the FFQ used in this cohort did not include other FRF such as blueberries and cherries. However, because the consumptions of blueberries and cherries were relatively low in Japan, a lack of data on them was not likely to change our findings materially. Second, residual confounding is always an alternative explanation for findings from observational studies. In our study, higher FRF intakes were associated with a healthier lifestyle, including less smoking, less drinking and higher intakes of seafood, vegetables, soya food, green tea and other fruits. Although we controlled many risk factors, unmeasured factors may have an influence on our findings. Moreover, we only calculated the content of flavonoids in fruits and did not include the content of flavonoids in vegetables and other foods (such as onions, chocolate or cocoa, tea and soya)(Reference Hooper, Kroon and Rimm32). A lack of validity of flavonoid estimates may also affect our findings. Third, dietary habits may change during the follow-up period. As only baseline dietary data were used for analysis, the influence of dietary changes on the associations could not be examined. Finally, our findings may be limited in generalisation to other Western populations in which dietary habits and lifestyles are different from those of the Japanese population.
In conclusion, this prospective cohort study provided evidence that higher consumptions of FRF, in particular citrus fruits, strawberries and grapes, were associated with a lower risk of developing stroke in Japanese women.
Acknowledgements
Members of the Japan Public Health Center-based prospective study (JPHC study) group are listed in https://epi.ncc.go.jp/en/jphc/781/8233.html.
J-Y. D. designed the study, analyzed the data, and edited the manuscript. Q.G. analyzed the data and drafted the manuscript. All authors conducted the technique review and edited the manuscript. The JPHC study was supported by National Cancer Center Research and Development Fund (23-A-31[toku] and 26-A-2) (since 2011) and a Grant-in-Aid for Cancer Research from the Ministry of Health, Labour and Welfare of Japan (from 1989 to 2010). This work was supported by the JSPS KAKENHI (A18H06391, T19K214700) to Dr. Dong.
The authors declare that there are no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114521000404