



Twin research has been a cornerstone of modern science, contributing significantly to the nature versus nurture debate (Boomsma et al., Reference Boomsma, Busjahn and Peltonen2002; Galton, Reference Galton1876; Montag et al., Reference Montag, Hahn, Reuter, Spinath, Davis and Panksepp2016; Tistarelli et al., Reference Tistarelli, Fagnani, Troianiello, Stazi and Adriani2020). Twins offer a unique opportunity for researchers, as they share both genetic material and environmental factors, allowing for more controlled studies compared to broader population-based research. However, the fascination with twinning is not a recent phenomenon; it has captivated scientists for centuries (Bhalotra & Clarke, Reference Bhalotra and Clarke2019; Chauhan et al., Reference Chauhan, Scardo, Hayes, Abuhamad and Berghella2010; Duncan, Reference Duncan1865; Newman, Reference Newman1941; Parisi, Reference Parisi2004; Polderman et al., Reference Polderman, Benyamin, De Leeuw, Sullivan, Van Bochoven, Visscher and Posthuma2015; Shipley et al., Reference Shipley, Wray, Hechter, Arellano and Borhani1967; Zeleny, Reference Zeleny1921).
Historically, the birth of twins imposed unexpected challenges on families, as there was no way to predict multiple pregnancies before childbirth. If both twins survived, parents faced the daunting task of caring for two new infants on limited resources — an especially difficult situation in less developed regions outside Northwestern Europe (Clark et al., Reference Clark, Cummins and Curtis2020). In contrast, twinning has become increasingly common in developed countries, particularly with the rise of medically assisted reproduction (Blondel & Kaminski, Reference Blondel and Kaminski2002; Fell & Joseph, Reference Fell and Joseph2012; Monden et al., Reference Monden, Pison and Smits2021).
As Hossain and Hasan (Reference Hossain and Hasan2024) note, twins can be either monozygotic (MZ; from a single zygote) or dizygotic (DZ; from separate zygotes; Hall, Reference Hall2003). The rate of MZ twinning is relatively stable, ranging from 3.5 to 4 twin pairs per 1000 births (Bulmer, Reference Bulmer1970). In contrast, the rate of DZ twinning varies depending on factors such as maternal age, health, parity, education, social class, ethnicity and season (Bortolus et al., Reference Bortolus, Parazzini, Chatenoud, Benzi, Bianchi and Marini1999; Nylander, Reference Nylander1981; Pison & d’Addato, Reference Pison and d’Addato2006; Shipley et al., Reference Shipley, Wray, Hechter, Arellano and Borhani1967). These variables contribute to the wide geographical and demographic differences in twinning rates observed globally (Bulmer, Reference Bulmer1959, Reference Bulmer1970).
For instance, during the 1980s, Africa had the highest twinning rate at 16 per 1000 births, followed by North America (9.9), Europe (9.1), South America (8.7), and Asia (7.0) (Monden et al., Reference Monden, Pison and Smits2021). By 2010–2015, twinning rates in Western countries had nearly doubled (Hossain & Hasan, Reference Hossain and Hasan2024). The Spanish case does not show significant differences compared to other Western countries (Luna & Alonso, Reference Luna and Alonso2016; Pison et al., Reference Pison, Monden and Smits2015).
In addition to the changes over time of twinning rates, the mortality of twins has been a significant area of interest. Historically, twins have faced higher neonatal, infant and child mortality rates compared to singletons (Gebremedhin, Reference Gebremedhin2015; Hong, Reference Hong2006; Suder et al., Reference Suder, Gniadek, Micek and Pawlik2021). This increased mortality is linked to shared resources in utero, leading to higher rates of fetal defects, prematurity, low birth weight, respiratory issues and weaker immune systems. Consequently, twin health and survival remain critical public health concerns in both developing and developed countries (Alam et al., Reference Alam, Van Ginneken and Bosch2007; Bdolah et al., Reference Bdolah, Lam, Rajakumar, Shivalingappa, Mutter, Sachs, Lim, Bdolah-Abram, Epstein and Karumanchi2008; Choi et al., Reference Choi, Bishai and Minkovitz2009; Guo & Grummer-Strawn, Reference Guo and Grummer-Strawn1993; Katz et al., Reference Katz, West, Khatry, LeClerq, Christian, Pradhan and Shrestha2001; Pison et al., Reference Pison, Monden and Smits2015; Rauh-Hain et al., Reference Rauh-Hain, Rana, Tamez, Wang, Cohen, Cohen, Brown, Ecker, Karumanchi and Thadhani2009).
Twin survival has historically been hampered by limited medical knowledge, with this disadvantage often exacerbated by social factors, especially for female twins. In traditional societies where son preference is prevalent, boys were often prioritized, potentially affecting the health and survival of female twins (Das Gupta et al., Reference Das Gupta, Zhenghua, Bohua, Zhenming, Chung and Hwa-Ok2003; Sen, Reference Sen1990; Williamson, Reference Williamson1976). This preference has been documented in regions of Southern and Eastern Europe and Asia (Beltrán Tapia & Gallego-Martínez, Reference Beltrán Tapia and Gallego-Martínez2017; Beltrán Tapia & Raftakis, Reference Beltrán Tapia and Raftakis2022; Marco-Gracia & Beltrán Tapia, Reference Marco-Gracia and Beltrán Tapia2021).
Therefore, the study of twins extends beyond the analysis of twinning rates and their determinants. The excess mortality among twins, gender disparities and associated social factors are equally important. The historical perspective also allows us to understand our origins, establishing a historical benchmark. Furthermore, it helps us understand how the behavior of family members has impacted the wellbeing and survival of infants based on their sex and characteristics.
Drawing on longitudinal microdata from a rural region in northeastern Spain between 1750 and 1950 (1840 twin individuals out of 70,148 births), this article traces the changes over time of twinning rates, along with their gender and period distributions, across two centuries of economic and social change. It also investigates the patterns of neonatal, infant and child mortality during this period, with a focus on gender differences among twins. The findings reveal that in the study area, twins had very high sex ratios at baptism and experienced high mortality rates during early childhood, particularly in the first days of life. Moreover, female twins were found to have higher mortality rates than their male counterparts both at birth and during early childhood. Overall, the likelihood of both female twins surviving to their 10th birthday was about half that of male twins. This provides us with a view of the historical reality of twins in rural Spain up until the mid 20th century.
Materials and Methods
To carry out a historical study over several centuries, access to individual-level data from population records is crucial. This research centers on a rural region in northeastern Spain, situated 6 to 40 kilometers from Zaragoza, the regional capital (see Figure 1). The area, a combination of plains and foothills along the Huerva River, includes 17 municipalities. The population in this region was approximately 7050 in 1750, 11,097 in 1857, 10,908 in 1900, and 12,162 in 1950. The study relies on comprehensive church registers from these villages, which provide detailed and high-quality records of all births, marriages, and deaths between 1750 and 1950, allowing for the reconstruction of complete life histories. The dataset covers 70,148 individuals, with twins comprising 1.3% of the births: 342 pairs of mixed-sex twins, 313 pairs of male twins, and 265 pairs of female twins.

Figure 1. Study area (Middle Huerva, Aragón, Spain).
Source: Own rendering.
The study area, covering roughly 500 square kilometers, is predominantly rural, with residents living mainly in nuclear households and primarily engaged in agriculture, particularly wheat cultivation, viticulture and sheep grazing. Historical records reveal that around 85% of the male workforce was involved in agriculture between 1800 and 1900. Marital fertility rates were high and stable during this period, averaging 6−7 children per couple until the late 19th and early 20th centuries. However, the high rates of infant and child mortality meant that only about half of these children survived to their 10th birthday. A notable decline in mortality rates began in the last decades of the 19th century, likely driven by improved living standards and advancements in public health, which, although primarily benefiting urban areas, also had a positive impact on rural communities (Harris & Helgertz, Reference Harris and Helgertz2019; Szreter, Reference Szreter1988). Initially, this decline was more evident among older children and later extended to younger cohorts.
Anthropometric data also suggest that the standard of living was relatively low, with the average male height in the mid 19th century being around 160 centimeters, which was lower than that of their European and other Spanish counterparts (Hatton & Bray, Reference Hatton and Bray2010; Marco-Gracia & Puche, Reference Marco-Gracia and Puche2021; Martínez-Carrión et al., Reference Martínez-Carrión, Cámara and Pérez-Castroviejo2016).
Given the reliance on local records, there are certain limitations in the study, particularly regarding individuals who migrated into or out of the area. For example, children who moved away with their families and died elsewhere are not accounted for in the age-at-death data. Similarly, individuals who moved into the area may be recorded for their deaths but not their births. Consequently, the analysis of infant and child mortality is confined to those with complete information, including those with known birth and death dates and those who married, indicating survival through infancy and childhood.
Descriptive statistics were employed to explore sex ratios at birth and at various ages for twins compared to singletons, with special attention to the temporal changes over time of these patterns. Survival and hazard estimates were used to examine statistical differences in survival and mortality between twins and singletons, boys and girls, and mixed-sex and same-sex twins. This comprehensive analysis offers new insights into the birth and mortality patterns of twins and the effects of gender discrimination on this vulnerable population.
We have also included, by subperiod, neonatal mortality rates (first 28 days of life), post-neonatal mortality rates (between 29 and 365 days of life) infant mortality rates (first year of life), and child mortality rates (first 5 years of life), as well as maternal mortality (measured in our case as the period between birth and the first 42 days of life). Additionally, in Table 1, we have conducted logistic regression analyses (Maalouf, Reference Maalouf2011), where the dependent variable is dichotomous (taking the value 1 if the individual is a twin), and the independent variables include parity, mother’s age, mother’s education level, family socioeconomic status (measured through the father’s occupation) and season of birth.
Table 1. Impact of at-birth demographic variables on twinning, 1750–1950

Note: FE, fixed effect. Robust standard errors in parentheses (clustered at the household level).
***p < .01, **p < .05, *p < .1
Source: Parish registers.
The twinning rate for each decade was defined as the number of twin births per 1000 live births within that decade. While the database lacks specific information on DZ and MZ twins, Weinberg’s differential method was utilized to estimate DZ and MZ twinning rates. This method classifies all mixed-sex twins and an equal number of same-sex twins as DZ, with the remaining same-sex twins classified as MZ (Weinberg, Reference Weinberg1901). Additionally, these rates were cross-checked with Hellin’s law, which posits that if the frequency of twin births is 1 per X births, the frequency of triplet births will be 1 per X2 births (Sel, Reference Sel2020).
Results
Trends and Patterns in Twin Births
Historically and in contemporary contexts, twins have represented a relatively small proportion of all live births, typically ranging from 1% to 1.5% in Western Europe according to various studies (Jacobsen et al., Reference Jacobsen, Møller and Mouritsen1999; Pison & Couvert, Reference Pison and Couvert2004; Pison & D’Addato, Reference Pison and d’Addato2006). In our sample, as detailed in Table 2, twins constitute 1.31% of deliveries, consistent with Hellin’s law. From the mid 18th century to the mid 20th century, the percentage of twin births gradually increased from 1.26% to 1.38%, reflecting an approximate 10% rise in twin deliveries. Among these births, 37.2% were mixed-sex (DZ) twins, while 62.8% were same-sex twins. This increase over the centuries was observed in both MZ and DZ twins, with both categories experiencing a slight upward trend.
Table 2. Number of observations of twins, and percentage over the total of birth in the study area (last column), 1750–1950

Note: The percentage of same-sex twins versus mixed-sex twins is calculated exclusively from twin births, rather than from the total births in the previous categories.
Source: Parish registers.
Studies utilizing large sample sizes have consistently shown that the sex ratio at birth for twins is slightly lower than that for the general population, indicating a higher in utero vulnerability, particularly for male fetuses (Dipietro & Voegtline, Reference Dipietro and Voegtline2017; Di Renzo et al., Reference Di Renzo, Rosati, Sarti, Cruciani and Cutuli2007; Jacobsen et al., Reference Jacobsen, Møller and Mouritsen1999). In our dataset, which includes 1840 twins born between 1750 and 1950 (968 males and 872 females), the sex ratio at baptism was 111.0 boys per 100 girls. This figure does not fully account for the skewed ratio, as mixed-sex twins, comprising 37.2% of our sample, do not affect the sex ratio. When focusing exclusively on same-sex twins, the sex ratio rises to 118.1, which is statistically distinct from the benchmark of 105 (Chao et al., Reference Chao, Gerland, Cook and Alkema2019). This observation is notable given the increased likelihood of miscarriage under the high mortality conditions characteristic of pre-industrial Europe (Woods, Reference Woods2009).
Table 3 elucidates how biological and socioeconomic variables of expectant families influence the likelihood of live twin births. This table shows the percentage of deliveries that were twins. The results indicate that women who have previously given birth are 25% more likely to have twins. This increased likelihood may be attributed to the positive effects of maternal experience on the survival of twin embryos in utero, or to the correlation between maternal age at first childbirth and parity. Our findings demonstrate that the probability of delivering twins rises with maternal age, consistent with studies linking this phenomenon to a higher risk of intrauterine death in multiple births among first-time mothers (Botting et al., Reference Botting, Davies and Macfarlane1987; Pison & D’Addato, Reference Pison and d’Addato2006). For instance, a mother aged 20 to 25 is nearly half as likely to give birth to twins as a mother aged 35 to 40. Beyond age 40, the likelihood of twin births decreases, potentially due to hormonal changes associated with the end of the reproductive cycle.
Table 3. Twinning rate across different determining factors, 1750–1950
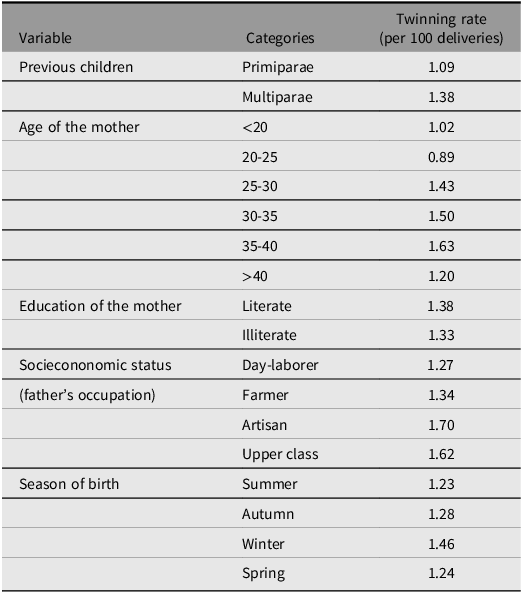
Source: Parish registers.
The result is particularly low for women aged 20 to 25, with less than 1% of their deliveries recorded as twins. This could be due to a higher percentage of primiparas and a greater rate of miscarriage resulting from increased stress and social difficulties (such as being in the early stages of marriage with fewer economic resources). It could also be a sample artifact. Therefore, further research is needed to understand the extent to which these results are typical.
Regarding socioeconomic factors, our findings suggest that better family conditions, such as higher education levels associated with improved hygienic knowledge and economic resources, correlate with a higher incidence of twin births. This correlation is likely due to reduced miscarriage rates (Woods, Reference Woods2009). Illiterate women were approximately 5% less likely to give birth to twins, while the wife of a laborer had a 25% lower chance of twin births compared to a woman from the upper class. This disparity is likely due to more favorable living and biological conditions in higher socioeconomic groups, which enhance the likelihood of successful pregnancies. Our analysis of the season of birth revealed no significant differences in the twinning rate, except for a slight increase in twin births during winter, which aligns with recent findings from Bangladesh (Hossain & Hasan, Reference Hossain and Hasan2024).
Finally, we assessed the impact of these variables on the likelihood of twin births using regression analysis, as shown in Table 1. The results clearly demonstrate that maternal age, parity, maternal education (though with lower statistical significance), and socioeconomic status significantly influence the biological wellbeing of the mother, and consequently, the twinning rate. In contrast, the season of birth did not show any significant effects, consistent with previous studies (Hossain & Hasan, Reference Hossain and Hasan2024).
Survival of Multiple Births
Table 4 presents neonatal, post-neonatal, infant, child and maternal mortality rates over 50-year subperiods, comparing singletons to twins. We observe that mortality rates are consistently much higher among twins than singletons. For neonatal mortality, twin mortality rates (always above 20% and often exceeding 30%) are consistently five to six times higher than those of singletons. The disparity lessens slightly with infant mortality, where twin mortality is two to three times higher than that of singletons (which never exceeds 20%). By the age of 5, the mortality differences have significantly narrowed, although twins still almost double the mortality rate of singletons. Notably, prior to the 20th century, nearly 60% of twins did not survive to their 5th birthday. The table also shows that in the 20th century (specifically from 1900 to 1950), mortality rates nearly halved for both twins and singletons.
Table 4. Neonatal, infant, and child (under 5years) mortality rate (per 1000 individuals) by type of birth

Source: Parish registers.
Our study underscores the severe survival challenges faced by twins in preindustrial rural Spain. Figure 2 presents survival and hazard estimates for twins and singletons up to their 10th birthday between 1750 and 1900. The 1900−1950 subperiod is not considered due to the fertility transition and improvements in healthcare, which reduced mortality differences. Our aim is to highlight the significant historical disparities between singletons and twins. Historically, twins experienced markedly higher mortality rates compared to singletons, with a significant portion of this disparity evident within the first weeks of life. Mortality rates for twins were 10 times higher than those for singletons during the initial hours post-birth (during the first approximately 24 hours of life) followed by a slight convergence afterward), and over 40% of twins had died by the end of the first month. This mortality rate increased to approximately 50% before their first birthday. Ultimately, fewer than 30% of twins survived to age 10, indicating an extremely low probability — around 10% — of both twins surviving childhood.
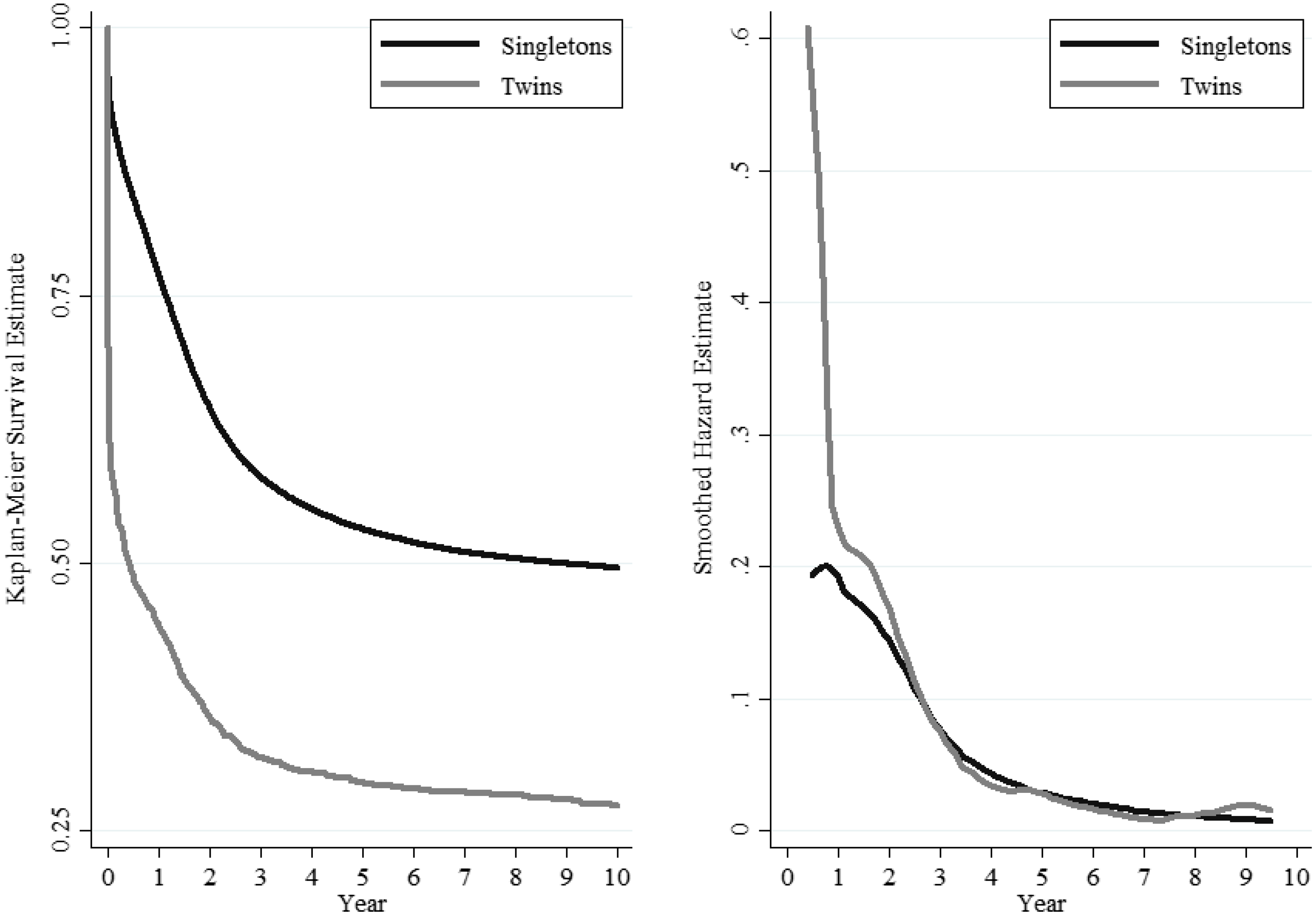
Figure 2. Survival and hazard estimates for twins and singletons, 1750–1900.
Source: Parish registers.
Figure 2 specifically examines the period prior to the onset of the fertility transition in the study area to mitigate the effects of changing fertility patterns (Marco-Gracia, Reference Marco-Gracia2018). Despite an overall decline in mortality rates during the demographic transition, differences in mortality between twins and singletons persisted and even slightly widened in the early stages. A trend towards convergence in survival rates began only in the last decades of the 20th century, aligning with Spain’s significant improvements in living standards and, particularly after the 1980s, advancements in healthcare for rural populations.
Moreover, the timing of a twin’s birth and the number of surviving siblings significantly impacted their likelihood of surviving the first year of life in our study area (Marco-Gracia & Beltrán Tapia, Reference Marco-Gracia and Beltrán Tapia2022). The highest mortality rates were observed among twins who had no living siblings and were likely born early in their parents’ marriage. For twins without surviving siblings, over 50% did not survive their first year, whereas the mortality rate for singletons in similar circumstances was approximately 17%.
In summary, twins experienced extremely high mortality rates, with their chances of surviving to adulthood being notably low. In the study area, only 10.2% of twin pairs reached the age of 10. These outcomes are closely associated with the inherent frailty of twins at birth and the lack of medical advancements. The impact of twin births was comparable to that of a single healthy child, as in most cases where one twin survived, the other typically died within the first few weeks of life. Among twins who lived beyond 5 years, 46% had lost their sibling within the first week, and 72% within the first month. Consequently, the development and potentially the investment in the surviving twin were similar to those of a singleton.
Gender Discrimination?
Gender-discriminatory practices likely influenced the survival rates of male and female twins during this period. In contexts with near subsistence living standards and high infant mortality, a preference for boys — stemming from the unequal allocation of family resources — may have favored the health of boys while disadvantaging girls (Marco-Gracia & Beltrán Tapia, Reference Marco-Gracia and Beltrán Tapia2021). However, the inherent biological advantage typically held by females could obscure the detection of such disparities in mortality rates. Boys are generally more vulnerable during the first year of life, particularly in the high-mortality environment of pre-industrial Europe (Drevenstedt et al., Reference Drevenstedt, Crimmins, Vasunilashorn and Finch2008; Knodel, Reference Knodel2002; Waldron, Reference Waldron and Waldron1998; Zarulli et al., Reference Zarulli, Barthold Jones, Oksuzyan, Lindahl-Jacobsen, Christensen and Vaupel2018). Consistent with findings related to singletons, most studies report higher mortality rates among male twins (Botting et al., Reference Botting, Davies and Macfarlane1987; Imaizumi, Reference Imaizumi2001; Rydhstrom, Reference Rydhström1990).
However, Figure 3, which presents survival and hazard estimates for male and female twins based on historical data from pre-industrial rural Spain, reveals that female twins had lower survival rates. Despite their biological advantages, female twins were particularly vulnerable during the first few months of life and again between their second and fourth years. Mortality rates began to converge only after the age of 5, by which time over 50% of all twins had died, with very few twin pairs having both members survive. The excess mortality among female twins was most pronounced during infancy and early childhood. Notably, even during the first year of life — when the biological advantage for females should be most evident — female twin mortality rates surpassed those of male twins. This is especially significant given that, unlike singletons, twin infants must share their mother’s milk during breastfeeding. Similar patterns of female disadvantage have been documented in countries with a strong preference for boys (Jayachandran, Reference Jayachandran2017; Kashyap & Behrman, Reference Kashyap and Behrman2020).

Figure 3. Survival and hazard estimates for male and female twins, 1750–1900.
Source: Parish registers.
Considering that parents might treat their twins differently based on whether they were mixed-sex or same-sex pairs, the analysis has been conducted separately for each group. While the penalty for female twins during the first months of life appears similar in both groups, early childhood was especially lethal for pairs of female twins (Figure 4). In mixed-sex twins, however, male twins were at a slightly higher risk. This difference is expected due to male frailty, but complex selection effects may also be influencing these results. The probability that both twins survived to their first birthday was low, meaning these findings might be shaped by which twin died first and the timing of that death.

Figure 4. Smoothed hazard estimates for mixed-sex and same-sex twins (ages 0–10), 1750–1900.
Source: Parish registers.
Discussion
Historical data on twins provide a longitudinal perspective on the changes over time of twinning rates and the factors influencing these rates. This study examines data from 17 rural villages in Spain over a 200-year period (1750−1950), during an era when Spain was a developing country with low living standards for most of its rural population. Consequently, our findings offer valuable historical insights into pre-industrial Western societies, with implications for both contemporary Western societies and developing nations.
The results reveal that the incidence of live twin births increased by nearly 10% from the mid 18th to the mid 20th century. This increase is likely attributable to improvements in socioeconomic conditions, hygiene, and medical care. The biological wellbeing of the population appears to have improved, as evidenced by a reduction in miscarriage rates and a higher success rate of twin pregnancies reaching full term (Marco-Gracia, Reference Marco-Gracia2020; Marco-Gracia & Beltrán Tapia, Reference Marco-Gracia and Beltrán Tapia2022).
Several factors are associated with a higher incidence of twin births, including maternal age. Older mothers are more likely to give birth to twins, although this tendency diminishes after the age of 40. Additionally, the likelihood of twin births was higher among mothers with previous childbirth experience. Historically, socioeconomic factors have played a significant role in the probability of twin births. Literate women — often indicative of higher living standards due to educational investment — and women from higher socioeconomic backgrounds had a 5% to 25% greater probability of delivering twins. Conversely, the season of birth (and thus the season of conception) did not exhibit a statistically significant effect.
Twins generally experience higher neonatal, infant and child mortality rates. In subsistence-level living conditions, twins are often born with lower average birth weights and face elevated mortality risks. To address the high mortality rates associated with low birth weight and associated weaknesses, urban maternity homes implemented breastfeeding support systems (Sánchez Lecha, Reference Sánchez Lecha2020). However, such resources were unavailable in the rural settings examined in this study. Mortality rates for singletons and twins were reduced by approximately half during the first half of the 20th century. This was a result of the epidemiological transition, as well as the introduction of new hygiene practices and medical advancements (Marco-Gracia & González-Esteban, Reference Marco-Gracia and González-Esteban2021).
Despite their biological advantages, female twins faced even higher mortality risks. Historically, 13.0% of male twin pairs survived, whereas only 6.1% of female twins survived. Among mixed-sex twins, if one child survived to the age of 10, the surviving child was male in nearly 55% of cases. These findings contrast with the well-documented greater male vulnerability, particularly in early life. The distribution of resources and family care evidently affected the sex-specific survival chances of twins in the study area. With the decline in childhood mortality rates in the late 19th and early 20th centuries, survival rates for all children, including twins, improved. The probability of both twins surviving increased from less than 10% throughout the 19th century to over 20% in the early 20th century.
Our findings indicate that social factors within the context of generally low living standards significantly influenced twin survival, including the presence of additional family members who could assist with the increased care demands of twins. Historically, fewer than 50% of live-born twins reached the age of five, with even lower survival rates for females.
Data availability statement
Data are available on request from the corresponding author.
Financial support
This research has been financially supported by the Ministry of Science and Innovation of Spain (PID2022-138886NB-I00) and the Government of Aragon (S55_23R).
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guides on the care and use of laboratory animals.









 Open access
Open access