

Eating disorders – anorexia nervosa, bulimia nervosa and eating disorder not otherwise specified – comprise a group of syndromes encompassing physical, psychological and social features. About 1 in 250 females and 1 in 2000 males will experience anorexia nervosa at some point in their lives (National Collaborating Centre for Mental Health 2004). About five times that number will suffer from bulimia nervosa. Eating disorder not otherwise specified is more common still, although many individuals will not receive treatment. Eating disorders can cause significant psychiatric morbidity and the adverse physical consequences of dieting, weight loss and purging behaviour are notable and sometimes prove fatal. Indeed, anorexia nervosa has one of the highest mortality rates of any psychiatric disorder, with a reported sixfold increase in mortality compared with the general population (Reference Papadopoulos, Ekbom and BrandtPapadopoulos 2009).
This article summarises the clinical features of eating disorders and explores the unique role of the general psychiatrist in identifying individuals with these conditions, supporting patients and directing them into evidence-based treatments.
Classification and diagnosis
The DSM-IV-TR (American Psychiatric Association 2000) delineates three broad categories of eating disorders:
-
• anorexia nervosa
-
• bulimia nervosa
-
• eating disorder not otherwise specified (EDNOS), less poorly defined in ICD-10 as atypical eating disorder (World Health Organization 1992). This category also includes binge eating disorder.
Note, however, that diagnostic criteria for eating disorders are currently under revision for DSM-5 and ICD-11.
Clinicians should also be aware of the various organic and psychiatric disorders that can mimic eating disorders (Box 1).
BOX 1 Differential diagnosis for eating disorders
Organic disorders
-
• Hyperthyroidism
-
• Diabetes mellitus
-
• Chronic infection (tuberculosis, AIDS, fungal infection)
-
• Inflammatory bowel disease (Crohn’s disease, ulcerative colitis)
-
• Malignancy (lymphoma, stomach cancer)
-
• Hypothalamic lesion or tumour
-
• Chronic respiratory disease (cystic fibrosis, bronchiectasis)
-
• Chronic pancreatitis
Psychiatric disorders
-
• Depression
-
• Somatoform disorders
-
• Obsessive–compulsive disorder
-
• Schizophrenia
Clinical features
Anorexia nervosa
Core psychopathology
Anorexia nervosa is characterised by the following core features.
A fear of normal body weight
Several near-synonyms have been used to describe this specific attitude, including ‘fear of fatness’ (Reference Russell and Harding PriceRussell 1970), ‘weight phobia’ (Reference CrispCrisp 1970) and ‘the pursuit of thinness’ (Reference BruchBruch 1965). Indeed, the fear of normal body weight is so common in anorexia nervosa that it is seen as pathognomonic of the condition. Although this distorted attitude has been variously described, it is perhaps best conceptualised as an overvalued idea representing a marked exaggeration of ideas that are widespread in our society. However, it can occasionally take on a delusional quality, especially in cases of severe and enduring eating disorder where the illness becomes embedded after many years of being underweight.
A lack of concern about low weight
Weight loss is viewed as an accomplishment rather than an affliction, with a lack of concern for the physical and psychosocial consequences of being underweight. There is often denial of symptoms such as hunger and fatigue, and the ambivalence about low weight often contrasts with the high levels of concern expressed by family and health professionals. Indeed, symptoms are largely egosyntonic, i.e. they are in harmony with or acceptable to the needs and goals of the ego and consistent with the concept of one’s own image.
Self-evaluation solely in terms of weight and shape
Most people evaluate themselves in terms of perceived performance in various domains (e.g. relationships, work, parenting), but in anorexia nervosa self-evaluation is judged largely, or even exclusively, in terms of shape and weight and the ability to control them.
Body image disturbance
This is an unusual and poorly understood symptom. There are at least two components. First, there is a perceptual distortion of body size and shape so that either the whole body or specific body parts appear larger or ‘fatter’ to the individual. This overestimation is not unique to anorexia nervosa, so the diagnosing clinician should look for significant associated negative affect. The second component is that of body image disparagement, where the body is viewed as repulsive or loathsome. Body image disparagement can also be generalised or focused on specific parts of the body and is often accompanied by body shape avoidance (i.e. the avoidance of situations that place a focus on shape and weight, such as looking in a mirror).
General (non-core) psychopathology
When assessing patients with anorexia nervosa it is important to appreciate just how many of the psychological symptoms are a result of the starvation state and not a cause of it. This was perhaps best demonstrated in the infamous Minnesota experiments (Reference Keys, Brozek and HenschelKeys 1950), where otherwise fit and healthy young men were effectively starved to weights typical of anorexia nervosa. The men became increasingly preoccupied with food, being plagued by incessant thoughts of food and eating. Mood swings and irritability were common and a quarter of men had significant depression.
Indeed, depressive and anxiety symptoms are common in anorexia nervosa and many patients will meet criteria for one or more mood or anxiety disorders. Many patients develop symptoms of social phobia and may not be able to eat in public at all. Outside interests are often reduced and there is usually marked social withdrawal. Obsessional features may be present and frequently cause food preparation and eating to become slow and ritualistic. There may be a decline in work or school performance, although performance is often maintained despite increasing impairments of concentration and marked emaciation. Furthermore, hopelessness and thoughts of suicide may be present. Many of these features improve on re-feeding but some may persist for many months despite a return to normal body weight.
Behavioural features
By far the most common method of weight control is extreme calorific restriction. The intense dietary restraint is characterised by a narrowing of the range of foods eaten and complete avoidance of certain foods which are seen as ‘fattening’. There is often a predetermined daily calorie limit of well under 1000 calories. Patients may fast for several days at a time. Other behaviours include excessive exercising, vomiting after meals, and the misuse of laxatives, appetite suppressants or diuretics. Avoidance of treatment is common and individuals are usually persuaded to seek help by concerned family members, teaching staff or general practitioners with whom they consult about physical symptoms.
Physical complications
The physical abnormalities seen in anorexia nervosa are largely secondary to disturbed eating habits and a compromised nutritional state. Hence most are reversed by restoration of healthy eating habits and sound nutrition, with the possible exception of reduced bone density. The range of medical complications is extensive (Table 1) and knowledge of them is essential in assessing physical risk.
TABLE 1 Physical consequences of anorexia nervosa and bulimia nervosa
Two specific physical complications are worthy of further discussion.
Reproductive functioning
As a consequence of poor nutrition, a widespread endocrine disorder involving the hypothalamic–pituitary–gonadal axis develops. This is manifest in women by amenorrhoea and in men by a lack of sexual interest or potency, and forms part of the operational diagnostic criteria (American Psychiatric Association 2000). An exception is when women take the contraceptive pill which replaces the hormonal deficit and may result in ongoing menstruation. Occasionally, patients may seek treatment at an infertility clinic (Reference Freizinger, Franko and DaceyFreizinger 2010). Although pregnancy can occur, it carries a risk of poor maternal and fetal outcome with higher rates of miscarriage and birth defects. Advising patients on the impact of their low weight on fertility can often be a crucial motivating factor in recovery treatment.
Osteopenia and osteoporosis
Malnutrition and hormonal factors such as oestrogen deficiency are thought to be important mechanisms which lead to the development of osteoporosis and osteopenia in a high proportion of patients with anorexia nervosa. However, the precise aetiology of bone demineralisation remains unclear. Osteoporotic-related fractures are common in chronic cases (Reference Herzog, Minne and DeterHerzog 1993) and can contribute to long-term suffering. Conventional treatments are often unsuccessful, with weight restoration being the treatment of choice.
Bulimia nervosa
Core psychopathology
The core psychopathology in bulimia nervosa mirrors that found in anorexia nervosa, with overvalued ideas concerning weight and shape and similar preoccupations with food and eating. However, important differences do exist. In contrast to anorexia nervosa, symptoms in bulimia nervosa are largely egodystonic, i.e. they are in conflict or dissonant with the needs and goals of the ego. Profound feelings of dysphoria, guilt and self-loathing are present. Moreover, people with bulimia nervosa describe an overwhelming ‘loss of control’ during binge episodes, while a central feature in anorexia nervosa is an increased sense of control achieved by strict dieting and the ability to control one’s own weight and shape.
General (non-core) psychopathology
As in anorexia nervosa, general psychiatric symptoms are prominent in bulimia nervosa. Depressive symptoms are often of a level equivalent to that seen in major depressive disorder. Anxiety and obsessive–compulsive features can also be present, although they are less common than in anorexia nervosa.
A significant minority of patients with bulimia nervosa regularly engage in a repertoire of mal-adaptive behaviours, including self-harm, alcohol and drug misuse, sexual disinhibition and shoplifting. When three or more such behaviours are consistently active, the term ‘multi-impulsive’ is sometimes used (Reference LaceyLacey 1993), most likely representing comorbid borderline personality disorder.
Behavioural features
Binge eating
In addition to a normal body weight, bulimia nervosa is distinguished from anorexia nervosa by the occurrence of repeated objective binge episodes followed by compensatory purging. Objective binge episodes are characterised by the consumption of a large amount of food in a brief period accompanied by a subjective loss of control and subsequent remorse. They should be distinguished from subjective binge episodes where patients report loss of control but do not consume an objectively large amount as judged by the interviewer (e.g. eating two pieces of pizza and feeling ‘out of control’ because only one piece was planned). Binge foods are usually high-energy, high-fat, sweet foods and may be chosen as they are ‘easy’ to binge on. Likewise, binge episodes are frequently planned, with food purchased or prepared in order to be consumed without interruption.
Purging behaviour
In most instances, binge eating is followed by compensatory purging behaviours. Self-induced vomiting is the most common form and usually occurs shortly after a binge. In severe cases the binge–purge cycle occurs daily and can go on for many hours at a time. The misuse of laxatives or diuretics and excessive exercising are also common but are not nearly as prominent as in anorexia nervosa.
Avoidance behaviour
Many patients will be secretive about their bulimic episodes, although some leave obvious signs of their disorder, such as empty food packaging or bags of vomit for other family members to discover. Individuals may also avoid situations in which they are likely to be exposed to food or will find it difficult to control their eating, such as eating out with others. Likewise, patients may avoid seeking treatment due to the fear that they will be forced to stop purging, leaving them to face the consequences of their binge eating (i.e. excessive weight gain). Such avoidance behaviour tends to add to any social or relationship difficulties that may already be present.
Physical complications
Many individuals often have no physical complaints, although bulimia nervosa can be associated with significant adverse medical consequences, especially when bingeing and purging behaviours are frequent (Table 1). However, there are some physical complications worthy of further discussion.
Hypokalaemia
Repeated vomiting can cause hypokalaemia and metabolic alkalosis, and many individuals with bulimia nervosa have electrolyte abnormalities on routine screening (Reference Wolfe, Metzger and LevineWolfe 2001). Hypokalaemia can lead to cardiac arrhythmias and cardiac arrest, and patients may require potassium supplementation or, in severe cases, medical admission for intravenous replacement and cardiac monitoring.
Reproductive and sexual functioning
At least 50% of patients with bulimia nervosa at normal weight have amenorrhoea or oligomenorrhoea (Reference Pirke, Fichter and ChloudPirke 1987) and high rates of infertility have been reported. However, women with bulimia nervosa are generally more sexually active than women in the general population, with greater lifetime numbers of sexual partners and higher rates of induced abortion and sexually transmitted diseases (Reference Abraham, Bendit and MasonAbraham 1985). Moreover, oral contraception is inappropriate and unreliable in the presence of regular self-induced vomiting.
Likewise, the interactions between pregnancy and bulimia nervosa are complex (Reference Morgan, Lacey and SedgwickMorgan 1999a, Reference Morgan, Chung and Lacey2006). On one hand, pregnancy can be a motivating factor for seeking treatment and bulimic symptoms may improve during pregnancy. On the other, symptoms may worsen postpartum, with higher rates of postnatal depression, miscarriage and preterm birth, making the fast-track of such patients into treatment paramount.
Dental erosion
Repeated vomiting can lead to erosion of dental enamel (perimylolysis) and patients often complain of dental pain and sensitivity. Vigorous tooth-brushing is common after self-induced vomiting and it may increase dental enamel wear. Using a fluoride mouthwash and then waiting several hours before brushing or eating acidic foods will reduce, but not prevent problems.
The role of the general psychiatrist
Screening
Not all patients will volunteer their symptoms or regard themselves as ill. However, early detection of an eating disorder in patients with unexplained weight loss improves prognosis. The SCOFF questionnaire (Reference Morgan, Reid and LaceyMorgan 1999b) (Box 2) is a useful screening tool which uses five simple questions, with two or more positive answers prompting the need to take a more detailed history. Although it is perhaps more commonly used in primary care, it has also been validated in secondary care (Reference Luck, Morgan and ReidLuck 2002) and can serve as a helpful aide-memoire during the assessment process.
BOX 2 SCOFF questionnaire as a screening tool for eating disorders
-
• Do you make yourself SICK because you feel uncomfortably full?
-
• Do you worry you have lost CONTROL over how much you eat?
-
• Have you recently lost OVER 14 pounds in a 3-month period?
-
• Do you believe yourself to be FAT when others say you are too thin?
-
• Would you say that FOOD dominates your life?
One point for every ‘yes’; a score of 2 or more indicates a likely case of anorexia nervosa or bulimia nervosa.
Making an accurate diagnosis
In addition to taking a full psychiatric history there should be a focus on the clinical features described earlier. The dietetic and developmental history are of particular interest, and calculating the body mass index (BMI) (weight (kg)/height (m2)) is a crucial step in making an accurate diagnosis and choosing the most appropriate care pathway.
Physical risk assessment
Eating disorders carry a heavy burden of physical morbidity and mortality but the predictors of physical risk have not been fully researched. Hence the following is only a guide to ‘usual practice’, and should be considered in the context of a full physical examination and applied only to adults. Moreover, attempts should be made to engage the general practitioner in the assessment and management of physical risk.
A screening assessment of risk should include a minimum of blood pressure, pulse, BMI, temperature and tests of proximal myopathy. An electrocardiogram (ECG) should be carried out if weight is low (BMI <16). Where a low BMI combines with abnormalities on ECG, rapid gradient of weight loss, abnormal electrolytes and muscle wasting, these can be considered ‘rough and ready’ predictors of higher physical risk.
Recommended routine tests include:
-
• BMI
-
• full blood count, urea and electrolytes, phosphate, glucose and liver function
-
• ECG if the BMI is <16, if drugs affecting QT interval are prescribed or if there are electrolyte abnormalities
-
• bone density and thyroid function may also be considered, but are not part of the immediate risk assessment
-
• tests should be repeated, and evaluation of risk should be seen as a longitudinal process.
Patients should be considered at risk and in need of close medical monitoring if they meet any of the criteria outlined in Table 2. However, some patients with chronic anorexia nervosa may show one or more of these features without necessarily indicating immediate risk. For example, most patients below a BMI of 12 should be regarded as ‘high risk’, whereas some patients can tolerate a BMI in the range of 12–14. Thus, the risk assessment should form part of a broader clinical history and physical examination, rather than replacing that examination. Rapid change such as sudden symptoms of dehydration should always be taken seriously. Cardiovascular signs and symptoms are particularly pertinent, as cardiac arrhythmia is an important cause of death.
TABLE 2 Assessment of physical risk in eating disorders
Assessment of motivation
Ambivalence about recovery is often a central feature of eating disorders. Careful assessment of motivation and readiness to change is essential to treatment planning and may reduce the likelihood of drop-out and treatment non-adherence.
Assessing motivation and readiness to change in eating disorders is based on the stages of change model (Reference Prochaska, DiClemente, Herson, Eisler and MillerProchaska 1992) (Table 3) and the framework and principles of motivational interviewing (Reference Miller and RollnickMiller 1991). In motivational interviewing, the spirit of the interview is an essential part of the interaction and combines elements of both style (e.g. warmth and empathy) and technique (e.g. key questions and reactive listening) in initiating a dialogue about the patients’ feelings about their symptoms. The interviewer adopts a curious, non-judgemental stance, shows genuine interest in the patients’ experience and seeks clarification as needed. A humble and curious presence facilitates a partnership conducive to a successful assessment.
TABLE 3 Stages and characteristics of the stages of change model
Specific areas to cover in motivational interviewing in eating disorders include:
-
• the extent to which the individual understands the nature of their illness and how it affects their life and those around them;
-
• the extent to which each relevant symptom (e.g. binge eating) is experienced as a problem;
-
• the extent to which the individual: either does not see the symptom as a problem or does not wish the symptom to change (precontemplation); is seriously thinking about changing the symptom (contemplation); and is taking action to change the symptom (action);
-
• if action to change a symptom is taking place, the extent to which this is done for themselves or for someone or something outside of themselves (internality).
Clinically, this approach may assist in building rapport and sets the scene for planning future treatment. Patients may be able to combat feelings of shame about their eating disorder and begin to turn a curious eye on their symptoms. Likewise, it provides a clear description of those aspects of the eating disorder that patients are more interested in changing and those symptoms they may not yet be willing to relinquish. Reference Treasure, Schmidt, Arkowitz, Westra and MillerTreasure & Schmidt (2008) provide an excellent up-to-date account and a detailed description of the use of motivational interviewing for eating disorders.
Knowledge of local care pathways
Figure 1 illustrates a simple treatment algorithm for adults with eating disorders and outlines the importance of an initial comprehensive assessment, including an assessment of physical risk. Close liaison between primary care, secondary care and specialist eating disorder services is essential. Proper integrated care coordination, such as the care programme approach, may play a significant role in improving adherence to treatment and ensuring successful outcomes (Reference Schmidt, Morgan and YousafSchmidt 2008).

FIG 1 Treatment algorithm for eating disorders (18+ years): identification and referral. BMI, body mass index.
Self-help material
The National Institute for Health and Clinical Excellence (NICE) recommends that patients with bulimia nervosa and binge eating disorder should be encouraged to follow a guided self-help programme as a possible first step in treatment (National Collaborating Centre for Mental Health 2004). In fact, self-help programmes may be a good starting point in the treatment of all mild to moderate eating disorders. Self-help resources are also available for carers, who should be encouraged to access support from local and national support groups. A list of self-help material and support groups is provided in Box 3.
BOX 3 Self-help material and support groups
Self-help material
Anorexia nervosa
-
• Overcoming Anorexia Nervosa: A Self-Help Guide Using Cognitive Behavioural Techniques (Reference FreemanFreeman 2009)
-
• The Anorexia Workbook: How to Accept Yourself, Heal Your Suffering, and Reclaim Your Life (Reference Heffner and EifertHeffner 2004)
Bulimia nervosa and binge eating disorder
-
• Overcoming Bulimia Self-help Course: A Self-help Practical Manual Using Cognitive Behavioral Techniques (3-Book Set) (Reference CooperCooper 2007)
-
• Overcoming Bulimia Nervosa and Binge Eating: A Guide to Recovery (Reference CooperCooper 1993)
-
• Overcoming Binge Eating (Reference FairburnFairburn 1995)
-
• Getting Better Bit(e) by Bit(e): Survival Kit for Sufferers of Bulimia Nervosa and Binge Eating Disorders (Reference Schmidt and TreasureSchmidt 1993)
Family and carers
-
• Skills-based Learning for Caring for a Loved One with an Eating Disorder: The New Maudsley Method (Reference Treasure, Smith and CraneTreasure 2007).
Eating disorders in men
-
• The Invisible Man: A Self-help Guide for Men with Eating Disorders, Compulsive Exercise and Bigorexia (Reference MorganMorgan 2008)
Support groups
-
• Beat (www.b-eat.co.uk) – formerly the Eating Disorders Association, Beat is the UK’s leading eating disorders charity. This website includes information about eating disorders, a section specifically for young people, helpline telephone numbers and information about other help and support available.
-
• Bodywhys (www.bodywhys.ie) – Bodywhys is the Eating Disorder Association of Ireland. The website contains information and support service details.
-
• Anorexia and Bulimia Care (www.anorexiabulimiacare.org.uk) – a national Christian charity offering help and support to people with eating disorders and their carers.
-
• Student Run Self Help (www.srsh.co.uk) – a website about a project aiming to improve support available to students and young people with eating disorders by setting up a network of student-run self-help groups. The website contains information about existing self-help groups and on how to get involved.
-
• Men Get Eating Disorders Too (http://mengetedstoo.co.uk) – a website for men who have been affected by anorexia, bulimia, binge eating disorder, compulsive eating and/or compulsive exercise.
-
• Carers UK (www.carersuk.org) – an organisation of carers: this website provides forums and information.
Education
Patients with eating disorders commonly read articles, books and websites about nutrition and dieting and may acquire an idiosyncratic body of knowledge that is not well founded. Typically, they are not well informed about the effects of vomiting and laxative misuse on calorific absorption. Likewise, patients may be unaware of the physical and psychological consequences of starvation and bingeing and purging behaviours. The clinician should give the patient information on the principles of healthy eating and portion sizes to read and consider for the next appointment. The Royal College of Psychiatrists (www.rcpsych.ac.uk) and British Nutrition Foundation (www.nutrition.org.uk) provide a number of good public information leaflets on such topics. Cognitive techniques can then be used to challenge the dietary rules that lead to unhelpful assumptions about food and eating. Useful resources for health professionals are listed in Box 4.
BOX 4 Online resources for psychiatrists
-
• The Royal College of Psychiatrists (www.rcpsych.ac.uk)
-
• The Institute of Psychiatry (www.kcl.ac.uk/iop)
-
• Centre for Research on Eating Disorders at Oxford (CREDO-1) (www.psychiatry.ox.ac.uk/psychiatry/research/researchunits/credo)
-
• Yorkshire Centre for Eating Disorders (www.leedspft.nhs.uk/our_services/yced)
Self-monitoring
Self-monitoring is achieved by the patient completing a therapeutic diary. To ensure ‘real-time’ monitoring, the patient is asked to carry the diary with them at all times, noting down their eating patterns and any associated thoughts, feelings or behaviours. Diaries are reviewed at each appointment. Honesty in completing the diary is emphasised and the practitioner adopts a non-judgemental approach when reviewing it. Diaries are useful in identifying baseline information and monitoring the progress of:
-
• eating patterns;
-
• trigger factors for dietary restriction, bingeing or purging behaviours; these may include unhelpful thoughts, specific situations, negative feelings, hunger, alcohol, relationship problems or boredom;
-
• barriers to recovery such as avoidance of certain situations and/or foods, and limited self-management skills (e.g. assertiveness).
A blank monitoring record and instructions on how to complete this are available online at www.psych.ox.ac.uk/research/researchunits/credo/cbt-and-eating-disorders-fairburn-2008.
Psychological interventions for eating disorders
The delivery of any psychological intervention should be accompanied by regular monitoring of a patient’s physical state, including weight and specific indicators of increased physical risk.
The National Institute for Health and Clinical Excellence (National Collaborating Centre for Mental Health 2004) recommends that cognitive analytic therapy (CAT), cognitive–behavioural therapy (CBT), interpersonal psychotherapy (IPT), focal psychodynamic therapy or family interventions be considered as psychological treatments of anorexia nervosa. Most individuals should be managed on an out-patient basis for at least 6 months. Cognitive–behavioural therapy for bulimia nervosa (CBT-BN) should be offered to adults with bulimia nervosa. The course of CBT-BN should normally be of 16–20 sessions provided on an out-patient basis over 4–5 months. Interpersonal psychotherapy should be considered as an alternative to CBT-BN, but patients should be informed that it takes 8–12 months to achieve comparable results.
There is little evidence to guide the treatment of patients with EDNOS, although NICE recommends that clinicians choose the specific treatment that most closely resembles the patient’s eating disorder (National Collaborating Centre for Mental Health 2004). However, it is recommended that CBT for binge eating disorder (CBT-BED) be offered to adults with binge eating disorder.
CBT for eating disorders
The theory that underpins CBT for eating disorders is concerned with the processes that maintain eating disorder psychopathology rather than those responsible for its initial development, although the two may overlap. Most other features seen in eating disorders can be understood as stemming directly from the underlying core psychopathology, including dietary restraint, other forms of weight-control behaviour, the various forms of body-checking and avoidance, and the preoccupation with thoughts about shape, weight and eating. Figures 2 and 3 demonstrate the cognitive–behavioural theory of anorexia nervosa and bulimia nervosa respectively.
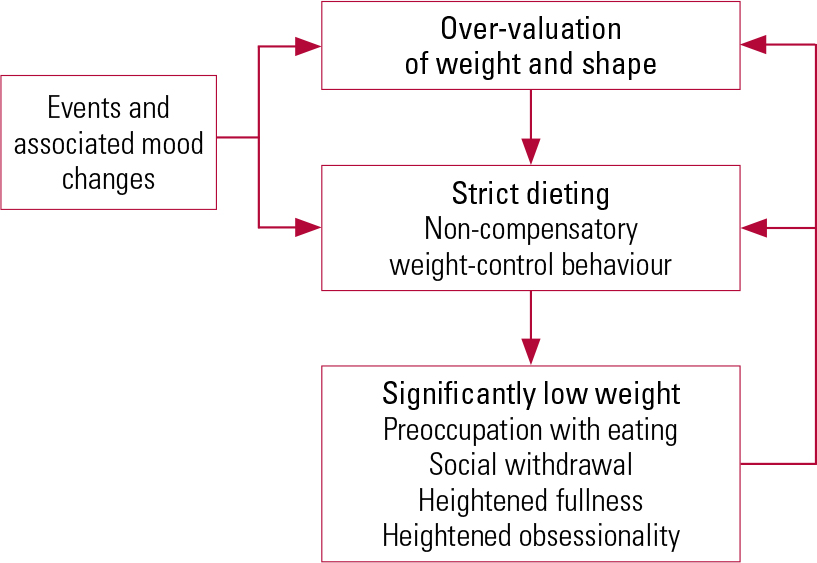
FIG 2 The cognitive–behavioural theory of anorexia nervosa.
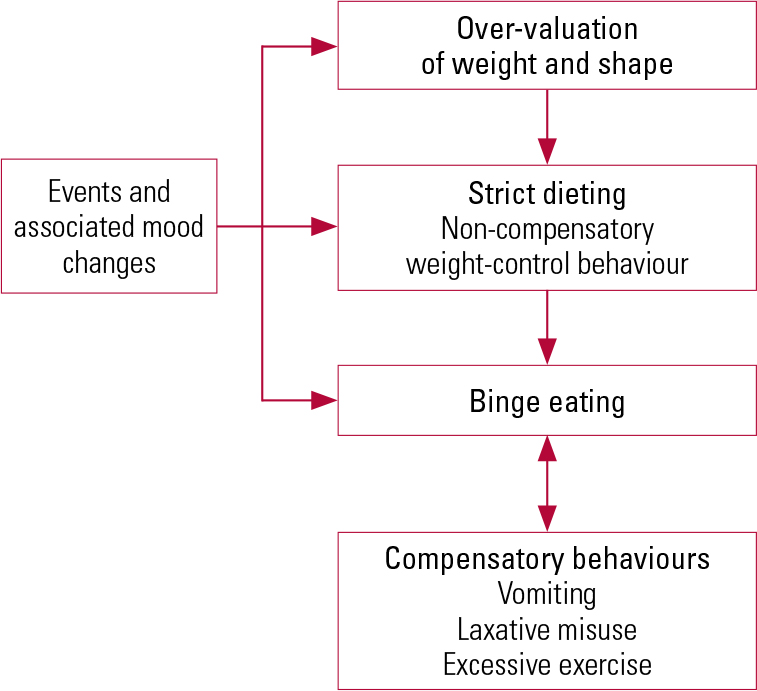
FIG 3 The cognitive–behavioural theory of bulimia nervosa.
Provision of psychological interventions
Psychological interventions are largely provided by specialist eating disorder services and training in their provision is essential for the eating disorder psychiatrist. Some psychology departments are also able to provide such treatment. However, access to these services varies greatly around the UK and the general psychiatrist may choose to provide a brief psychological intervention independently for motivated individuals with mild to moderate eating disorders. A brief psychological intervention can take two forms.
The first is integration of the principles and techniques described earlier (e.g. CBT, motivational interviewing, self-help, self-monitoring) into normal practice.
The second is the use of a more structured intervention such as the manualised workbook by Reference SaeidiSaeidi (2008); this intervention can be delivered in 6–12 weekly sessions, depending on the patient’s presenting problems and readiness to change. Patients are asked to complete various questionnaires in the manual, covering areas such as readiness and motivation to change, nutrition, healthy eating and changing thoughts and beliefs about food and eating.
Medication
All medication should be regularly reviewed, as many patients will be prescribed unnecessary and often harmful medication such as laxatives, appetite suppressants and psychotropic medication.
Anorexia nervosa
There is a very limited evidence base for the pharmacological treatment of anorexia nervosa. A range of drugs may be used in the treatment of comorbid conditions but caution should be exercised in their use as there may be improvement with weight restoration alone. If the prescription of medication that may compromise cardiac functioning is essential, ECG monitoring should be undertaken. Likewise, all patients should have an alert placed in their prescribing record concerning the risk of side-effects.
Bulimia nervosa and binge-eating disorder
The National Institute for Health and Clinical Excellence (National Collaborating Centre for Mental Health 2004) recommends that adults with bulimia nervosa and binge eating disorder may be offered a trial of antidepressant medication as an alternative or additional first step to using a self-help programme. Patients should be informed that antidepressants can reduce the frequency of bingeing and purging but these behaviours are likely to return on stopping the medication. Best results are achieved when medication is used in conjunction with psychological therapy. Selective serotonin reuptake inhibitors (specifically fluoxetine) are recommended and should be used at higher doses than for depression (e.g. fluoxetine 60mg/day).
Compulsory treatment
In general, compulsory treatment should be a last resort for patients with eating disorders. However, compulsory admission is justified in cases of serious threat to health, where compulsory feeding may be necessary to combat both the physical complications and the underlying mental disorder. In such cases the use of the Mental Health Act 1983, as opposed to the Mental Capacity Act 2005, needs to be considered in order to facilitate treatment in an attempt to prevent death. Nasogastric feeding has been accepted as a ‘medical treatment’, forming an integral part of the treatment of anorexia nervosa and as such is directly permitted under the Mental Health Act, rather than requiring justification under the Mental Capacity Act.
Conclusions
Most people with severe eating disorders are treated in specialist eating disorder services, but the general psychiatrist is often responsible for the care of many individuals with mild to moderate disorder. Likewise, the general psychiatrist will be familiar with many of the clinical features of eating disorders but they may lack confidence in treating and supporting patients in a non-specialist setting. Making an accurate diagnosis, assessing motivation and ensuring regular physical risk assessment are essential steps in choosing the most appropriate care pathway. Providing self-help and educational material is often a good starting point in treatment, and integrating various psychological principles and techniques (e.g. CBT, motivational interviewing, self-monitoring) into normal practice can be beneficial to patients.
MCQs
Select the single best option for each question stem
-
1 The criteria required for a diagnosis of anorexia nervosa (DSM-IV-TR) include:
-
a amenorrhoea for 2 months
-
b weight loss leading to maintenance of body weight less than 90% of that expected
-
c low self-esteem
-
d intense fear of gaining weight or becoming fat, even though underweight
-
e lanugo hair.
-
-
2 The criteria are required for a diagnosis of bulimia nervosa (DSM-IV-TR) include:
-
a weight loss leading to maintenance of body weight less than 85% of that expected
-
b binge eating and inappropriate compensatory behaviour both occur, on average, at least twice a week for 3 months
-
c binge eating and inappropriate compensatory behaviour both occur, on average, at least once a week for 3 months
-
d amenorrhoea
-
e low self-esteem.
-
-
3 A core feature of anorexia nervosa is:
-
a avoiding carbohydrate-rich foods
-
b body image disturbance
-
c anxiety around meal times
-
d calorie counting
-
e low mood.
-
-
4 Physical complications commonly found in bulimia nervosa include:
-
a hyperkalaemia
-
b hypokalaemia
-
c hypernatraemia
-
d hyperchloraemia
-
e lanugo hair.
-
-
5 Patients with eating disorders should be considered at risk and in need of close medical monitoring if:
-
a QTc interval is 445 ms
-
b potassium is 3.5 mmol/l
-
c pulse rate is 51 bpm
-
d rate of weight loss is 1.8 kg per week
-
e there is evidence of dental erosion.
-
MCQ answers

| 1 | d | 2 | b | 3 | b | 4 | b | 5 | d |







eLetters
No eLetters have been published for this article.