


In recent decades, intakes of dietary protein have been associated with treating chronic diseases such as obesity (OB) and CVD besides improving health outcomes(Reference Foreyt, Salas-Salvado and Caballero1, Reference Wolfe, Miller and Miller2). Evidence indicates that a high dietary protein intake decreases the risk of non-communicable diseases via the regulation of energy intake, increment of satiety, lowering of systolic and diastolic blood pressure, decrement of total cholesterol levels and presence of LDL-cholesterol and TAG(Reference Abete, Parra and Martinez3–Reference Bortolotti, Kreis and Debard5). In addition, high protein intakes are associated with the prevention of the development of chronic diseases, including OB, the metabolic syndrome, CVD, type 2 diabetes, osteoporosis, and breast and prostate cancer(Reference Abete, Parra and Martinez3, Reference Dewell, Weidner and Sumner6–Reference Westerterp-Plantenga10).
Findings from recent randomised controlled trials relate plant proteins to health benefits more than animal proteins(Reference Allison, Gadbury and Schwartz11–Reference Wu, Stanczyk and Martinez19), mainly due to factors affecting the level of hypercholesterolaemic amino acids present in plant proteins(Reference Krajcovicova-Kudlackova, Babinska and Valachovicova20). However, the debate on the potential health effects of animal protein- and plant protein-rich diets is still ongoing. For instance, some studies have reported a positive association between animal protein intakes and the risk of chronic diseases(Reference Allen, Key and Appleby21–Reference Sieri, Krogh and Muti24), whereas others have indicated an inverse relationship(Reference Aoe, Koyama and Toba25–Reference Ouellet, Marois and Weisnagel27). One of these trials, involving healthy menopausal women, has suggested that milk whey protein can prevent bone loss(Reference Aoe, Koyama and Toba25), while two others trials with overweight (OW) or insulin-resistant subjects have indicated that proteins from meat, poultry, fish and dairy foods had beneficial metabolic effects(Reference Farnsworth, Luscombe and Noakes26, Reference Ouellet, Marois and Weisnagel27) and improved insulin sensitivity(Reference Farnsworth, Luscombe and Noakes26, Reference Ouellet, Marois and Weisnagel27).
In Belgium, information on plant and animal protein intakes of the population is still lacking until now. Therefore, the present study aims (1) to estimate the intake levels of animal and plant proteins in a representative sample of the Belgian population and (2) to examine their associations with OW and OB measured by BMI and waist circumference (WC).
Methodology
Study design and data collection
The Belgian National Food Consumption Survey(Reference De Vriese, De Backer and De Henauw28) was performed in 2004 following largely the recommendations of the European Food Consumption Survey Method project(Reference Brussaard, Johansson and Kearney29). More details on the survey can be found elsewhere(Reference De Vriese, De Backer and De Henauw28). Belgian national citizens aged 15 years or older, residing in private households in Belgium, were eligible to participate in the national survey. The population was stratified by sex and in four age groups (15–18, 19–59, 60–74 and ≥ 75 years). Approximately 400 individuals were allocated in each sex–age group. Participants were selected from the national register using a multi-stage stratified sampling procedure. Institutionalised individuals, not able to speak one of the national languages or physically or mentally unable to be interviewed, were excluded from the survey. In total, 7543 individuals were invited to participate.
The present study was conducted according to the guidelines laid down in the Declaration of Helsinki and approved by the medical ethical committee of the Scientific Institute of Public Health, Brussels. Written or verbal informed consent was obtained from all subjects. Verbal consent was witnessed and formally recorded.
Dietary intake assessment
Two repeated, non-consecutive 24 h dietary recall interviews were used to collect information on each participant's food consumption. The first 24 h recall was obtained through a computer-assisted personal interview during a home visit by a trained dietitian. The second 24 h recall was performed 2–8 weeks later during a second home visit (median 3 weeks). Interviews were randomly allocated to different days of the week and over a 12-month period in an effort to reduce within-person variation and to avoid seasonality effects. The 24 h recalls collected information on the types and quantities of foods and beverages consumed over the preceding day to the interview.
The dietitians used European Prospective Investigation into Cancer and Nutrition software (EPIC-SOFT; International Agency for Research on Cancer (IARC), Lyon, France) to obtain standardised 24 h recall interviews. EPIC-SOFT was designed to obtain a detailed description and quantification of all foods and beverages consumed in a standardised way(Reference Slimani and Valsta30). Quantification was facilitated using a picture book with coloured photographs describing foods of different portion sizes(Reference De Vriese, De Backer and De Henauw28).
Animal and plant protein contents were estimated using the Belgian food composition table NUBEL(31), the Dutch food composition database NEVO(32) and the USDA food composition guidelines(33). In the present study, consumption of soya products was analysed separately from the legumes food group because of their potential health effects. The US Food and Drug Administration(34) approved that a daily consumption of soya protein can prevent chronic diseases.
In the present study, four and six main food groups, respectively, contributed most to the animal and plant protein intakes. The four main food groups contributing to the levels of animal protein intake were dairy products, meat and meat products, fish and shellfish, and eggs and egg products. Dairy products included milk, milk beverages (including cream desserts and puddings (milk-based), dairy and non-dairy creams, milk for coffee, and creamers), yogurt, fromage blanc and petits suisses and cheeses (including fresh cheeses). The group of meat and meat products included fresh meat (beef, veal, pork and lamb), poultry and game (chicken, turkey, duck and rabbit), and processed meat, whereas the group of fish and shellfish represented all fish, crustaceans, molluscs, fish products and fish in crumbs. Eggs were the most important item in the egg and egg products group.
Plant proteins were derived mainly from potatoes and other tubers, vegetables, legumes, fruits, nuts and seeds, cereal and cereal products, and soya products. The group of potatoes and other tubers consisted mainly of potatoes. Vegetables included leafy vegetables, fruiting vegetables such as tomato and pumpkin, root vegetables, cabbages, mushrooms, grain and pod vegetables, onions, garlic, stalk vegetables and sprouts, mixed salad and mixed vegetables. Soyabeans and derived products were excluded from the legumes group and were classified as a separate group. Fruits referred to all fruits, including fresh fruits (fruits, mixed fruits and olives) and nuts and seeds. Cereals and cereal products included mainly flour, flakes, starches, semolina, pasta, rice, other grains, breakfast cereals, bread, crisp bread, rusks, salty biscuits, aperitif biscuits and dough and pastry.
Anthropometric measurements
Weight (kg) and height (m) were self-reported. WC was measured by a trained dietitian at home while participants were standing upright (upper clothes were raised to enable measurement of WC on the skin or underwear). Pregnant women reported pre-gestational weights. BMI was calculated as weight (kg)/height (m2). Adult participants were allocated to four BMI categories according to the cut-off criteria of the WHO(35) for adult BMI: underweight ( < 18·5 kg/m2); normal weight (18·5–24·9 kg/m2); OW (25·0–29·9 kg/m2); obese ( ≥ 30·0 kg/m2). Adolescent participants were classified into four similar BMI categories based on the Flemish cut-off values(36) for underweight. Cut-off points for normal weight, OW and obese were based on the criteria proposed by Cole et al. (Reference Cole, Bellizzi and Flegal37). For adult WC, sex-specific cut-off criteria were used(Reference Lean, Han and Morrison38). For males, < 94 cm was defined as normal, 94–102 cm as normal to borderline, ≥ 102 cm as high risk of OW and obese (referred to as ‘too large’ in Table 1). For females, < 80 cm was defined as normal, 80–88 cm as normal to borderline, ≥ 88 cm as high risk of OW and obese. The cut-off criteria of adolescent WC were based on Taylor et al. (Reference Taylor, Jones and Williams39).
Table 1 BMI and waist circumference (WC) measurements of subjects participating in the Belgian National Food Consumption Survey
(Mean values with their standard errors, n 3083)
* Weighted mean of BMI and WC.
Statistical analyses
The Statistical Package for the Social Sciences for Windows version 15 (SPSS, Inc., Chicago, IL, USA) was used to perform descriptive and statistical analyses. Descriptive statistics are presented in the sex–age-specific groups as means with their standard errors. Total energy, total protein, animal and plant protein intake and percentage of energy intake (Table 2) were normally distributed, whereas animal and plant protein intakes from food groups (Tables 3 and 4, respectively) were skewed. Student's t test, ANOVA with Bonferroni correction and the Mann–Whitney U test were used to examine statistically significant differences, with a two-tailed significance level set at 0·05.
Table 2 Total energy, total protein, animal and plant protein intake, and percentage of energy intakes of the survey participants
(Mean values with their standard errors, n 3083)
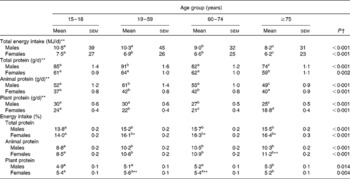
a,b,c,d Mean values within a row with unlike superscript letters were significantly different (P < 0·05; ANOVA with Bonferroni correction).
Mean values were significantly different between men and women: *P < 0·05, **P < 0·001 (Student's t test).
† P value for mean differences between the sex–age groups (ANOVA).
Table 3 Mean total animal protein intakes and intakes from main sources stratified by age (years) and sex
(Mean values with their standard errors, n 3083)

a,b,c,d Mean values within a column with unlike superscript letters were significantly different (t test, ANOVA with Bonferroni correction and Mann–Whitney U test).
* Weighted mean of animal protein intake and its percentage.
† P value for mean differences between males and females for animal protein intake (Student's t test and Mann–Whitney U test).
Table 4 Mean total plant protein intakes and intakes from main sources stratified by age (years) and sex
(Mean values with their standard errors, n 3083)

a,b,c Mean values within a column with unlike superscript letters were significantly different (t test, ANOVA with Bonferroni correction and Mann–Whitney U test).
* Weighted mean of plant protein intake and its percentage.
† P value for mean differences between males and females for plant protein intake (Student's t test and Mann–Whitney U test).
Multiple linear regression analysis (generalised linear model) by the sex–age strata was used to evaluate the association between BMI, WC and animal and plant protein intakes. Each model included BMI and WC as separate dependent variables, animal and plant protein as covariates and age as the factor variable. Interactions were tested, and the significance level was estimated by type 3 Wald χ2 test.
Results
Individuals who provided two 24 h dietary recall interviews with valid information were included in the analysis (3083 out of a total of 7543). Male (n 1546) participants had a mean of 25 kg/m2 for BMI and a mean of 88 cm for WC. In total, 34 % of the males were defined as OW, 10·1 % as obese and 29 % had a too large WC. Mean BMI for female (n 1537) participants was 24 kg/m2, and mean WC was 80 cm. In total, 25 % of the females were defined as OW, 10·5 % as obese and 42 % had a too large WC (Table 1).
Most of the participants in the older categories were categorised as OW or obese (60–75 years: 63 %; ≥ 75 years: 50 %) and with borderline or too large WC (60–75 years: 80 %; ≥ 75 years: 81 %).
Total protein, animal protein and plant protein intakes
Total protein intakes (1·2 MJ/d) contributed 15·4 % to the total energy intakes of the population. Animal protein intakes contributed most and delivered a mean energy intake of 0·795 MJ/d. Animal protein intake (47 g/d, range 0·030–222 g/d) was the main contributor (64 %) to the total protein intakes (mean 72 g/d), while plant protein intake accounted for 25 g/d (range 2·4–83 g/d). The total protein intakes of the present study population were in line with the WHO/FAO/United Nations University recommendations (i.e. 10·0–15·0 % of the total energy intake)(40) (data not shown).
Total protein, animal protein and plant protein intakes were significantly higher in males than in females (Table 2). Percentage energy contributions from the total protein and animal protein intakes were significantly lower in male and in female adolescents than in the older age groups. The contribution of plant proteins to the total energy intakes was higher in elderly males aged ≥ 75 years and lowest in females aged ≥ 75 years.
When examined by sex, total protein intakes were higher among adults (19–59 years) and lower among the elderly population ≥ 75 years. Adult males (19–59 years) reported significantly higher animal protein intakes, while elderly males ( ≥ 75 years) had the lowest. For female participants, on the other hand, animal protein intakes in the age groups of 19–59 years and 60–74 years were significantly higher than those in the other age groups. Plant protein intakes decreased with age in both sex groups, resulting in significant differences between the youngest and the oldest age groups (P < 0·001 for both).
Main food groups
Tables 3 and 4 show, respectively, the food groups contributing 57 % to the total animal protein intakes (dairy products, meat and meat products, fish and shellfish, and egg and egg products) and 28 % to the total plant protein intakes (potatoes and other tubers, vegetables, legumes (excluding soya products), soya products, fruits, and cereal and cereal products). Meat protein was the main contributor to the total protein intakes (34 %), with a mean intake of 26 g/d, followed by cereal protein (19·3 %), with a mean intake of 13·7 g/d, and dairy protein (15·1 %), with a mean intake of 11·0 g/d (data not shown).
For both sexes, meat and meat products contributed most to the total animal protein intakes (males: 55 %, mean intake of 31 g/d; females: 50 %, mean intake of 21 g/d; P < 0·001), followed by dairy products (males: 22 %, mean intake of 11·9 g/d; females: 26 %, mean intake of 10·0 g/d; P < 0·001) (data not shown). Compared with males, females consumed less meat and dairy proteins derived from the above-mentioned food groups in general and their specific subgroups, except for yogurt. In particular, proteins from fresh and processed meat were consumed significantly less by females in all age groups (range of consumption: males and females, respectively: 14·3–18·2 and 10·2–11·6 g/d for fresh meat; 7·3–9·2 and 3·9–5·1 g/d for processed meat; P < 0·001 for both).
The elderly population (60–74 or ≥ 75 years) consumed less proteins derived from dairy and meat products compared with the other age groups. Female adolescents had significantly lower meat protein intakes than others (18·9 g/d contributing to 30 % of the total animal protein intake). The elderly population (60–74 years) reported the lowest and the highest fish and shellfish protein intakes (males: 7·9 %, mean intake of 6·4 g/d; females: 6·7 %, mean intake of 4·4 g/d). Protein intakes from eggs and egg products were not significantly different between the sex–age groups, with the exception of elderly females ( ≥ 75 years) who had the lowest consumption among the sample.
Cereals and cereal products (males: 55 %, mean intake of 15·9 g/d; females: 52 %, mean intake of 11·4 g/d) contributed most to the total plant protein intakes followed by potatoes and other tubers, vegetables and fruits. The consumption of soya proteins was very low (0·174 g/d). Intakes from potatoes and other tubers, vegetables and fresh fruits were significantly higher in the elderly population (60–74 and ≥ 75 year groups) than in the adolescent and adult groups. The latter groups consumed, however, significantly more proteins from cereals and cereal products (data not shown).
Associations between BMI and animal and plant protein intakes
The χ2 test showed significant positive linear relationships between BMI and animal protein intake in the elderly group (60–74 years) for both sexes (Table 5). On the other hand, negative associations were observed between BMI and plant protein intakes in the age group of adolescents (15–18 years) and adults (19–59 years) in males and females. Moreover, animal protein intake was not significantly associated with BMI of females and was not retained in the final model.
Table 5 Generalised linear model for the associations between BMI and animal and plant protein intakes in the sex–age-specific strata
(β Coefficients with their standard errors and 95 % confidence interval, n 3054)
* Age ( ≥ 75 years) reference category.
Associations between waist circumference and animal and plant protein intakes
Table 6 shows the associations between WC and animal and plant protein intakes, which were in line with the observations for BMI. The intake of plant proteins was inversely associated with WC in all sex–age groups, except for males aged 60–74 years. Animal protein intake was positively associated with males' WC but not with females' WC.
Table 6 Generalised linear model for the associations between waist circumference and animal and plant protein intakes in the sex–age-specific strata
(β Coefficients with their standard errors and 95 % confidence intervals, n 2874)
* Age ( ≥ 75 years) reference category.
Discussion
The present findings suggest that in a representative sample of the Belgian population, the most important contributors to animal protein intakes were fresh meat, cheese and milk products. In addition, cereals and cereal products were the most important contributor to plant protein intakes. Other food groups, including soya, contributed to a very low degree to the total plant protein intakes observed.
Given the lack of information on the total protein intakes from previous Belgian national nutrition surveys, we relate the present study findings to those available in other countries including the USA, Europe, Spain and China(Reference Keinan-Boker, Peeters and Mulligan41–Reference Zhang, Chen and Huang44). Differences in study design, food consumption assessment methods and food group classifications used in the various surveys should be taken into consideration when interpreting the relationships. The total energy intakes in Belgian males and females (9·5 and 6·6 MJ/d, respectively) were slightly lower than those in the UK population (males: 9·7 MJ/d; females: 6·9 MJ/d) and were considerably lower than in the Dutch population (Third Dutch National Food Consumption Survey – 1997/98) (males: 10·8–11·0 MJ/d; females: 7·8–8·4 MJ/d)(Reference Hulshof, Brussaard and Kruizinga45, Reference Swan46). In addition, the total protein intakes expressed as percentage of energy intake were slightly lower in the Belgian population (males: 15·0 %; females: 15·7 %) than in the UK population (males: 16·5 %; females: 16·6 %). On the other hand, Belgians had similar intakes to the Dutch population (males: 14·7–15·2 %; females: 15·6–16·6 %), with the exception of the adolescent age group.
We have also compared the present findings with the results of the Third US National Health and Nutrition Examination Survey (1988–91)(Reference Smit, Nieto and Crespo43) and the Spanish Catalan Nutritional Survey (2002–3)(Reference Serra-Majem, Ribas-Barba and Salvador42), which used the same dietary assessment methods. It was observed that the total energy intakes of the Belgian population were lower than those of the US population (males: 10·8 MJ/d; females: 7·3 MJ/d). Belgian males and elderly females (60–75 years), however, had higher total energy intakes than the Spanish (males: 9·0 MJ/d; females: 5·7 MJ/d).
Total protein, animal protein and plant protein intakes
According to the present study, total protein intakes were lower in the Belgian population, especially in males, when compared with US males and females (97 and 65 g/d, respectively)(Reference Smit, Nieto and Crespo43) and with Spanish males and females (97 and 79 g/d, respectively)(Reference Serra-Majem, Ribas-Barba and Salvador42) presumably due to lower intakes of animal protein. Protein intakes expressed as percentage of energy intake among Belgian sex–age-specific groups were rather similar to US adults and the elderly population (males: 15·0–16·0 %; females: 15·0–17·0 %), but lower than those observed in Spanish sex–age groups (males: 18·9 %; females: 19·4 %). The Belgian population, with the exception of participants in the ≥ 75 years age category, however, had higher total protein, animal protein and plant protein intakes than average intakes of the European Prospective Investigation into Cancer and Nutrition Potsdam Study participants (total protein: 70 g/d; animal protein: 44 g/d; plant protein: 24 g/d)(Reference Weikert, Walter and Hoffmann47).
Compared with the US survey, the Belgian population had lower protein intakes from milk, yogurt, and eggs and egg products than the US population (milk and yogurt: 11·3 % in males and 13·4 % in females; eggs and egg products: 4·1 % in males and 4·3 % in females). The present results showed that fish and shellfish, and cheese contributed more to the total protein intakes in the Belgian population than in the US population. More specifically, participants in the age groups of 60–74 years and ≥ 75 years consumed approximately twice as much fish-derived proteins than their US counterparts (males: 5·3 %; females: 5·6 %). On the other hand, fish proteins contributed more to total protein intakes in Spain (14·7 %) than in Belgium (males: 3·6–7·9 %; females: 4·4–6·7 %). In contrast, meat and meat products contributed less to animal intakes in the Belgian population (males: 36–37 %; females: 30–36 %) than in the Spanish (39·4 %).
It was also observed that the consumption of meat proteins from subgroups including fresh meat, poultry and processed meat was lower among the Belgian than the Spanish population; females, in particular, had lower intakes of the above-mentioned meat subgroups. For example, protein intakes from poultry were much lower among Belgians (males: 7·0–8·1 %; females: 7·5–8·9 %) than among Spanish (14·0 %). In addition, dairy and egg protein intakes were slightly higher among the Spanish population (12·5 and 3·1 %, respectively).
Fresh fruits contributed less to the total protein intakes in the Belgian population (males: 0·533–1·4 %; females: 1·2–1·9 %) than in the US population (males: 1·4 %; females: 1·8 %) and in the Spanish population (2·0 %). Protein intakes from legumes in the Belgian population were also lower than both the US (males: 2·3 %; females: 2·1 %) and the Spanish population (2·1 %). Plant protein intake from vegetables in the present study population (males: 2·1–2·9 %; females: 2·5–3·7 %) was much lower than in the US population (males: 7·7 %, females: 8·7 %), but higher than in the Spanish population (2·3 %). On the other hand, higher amounts of plant proteins from cereals and cereal products were consumed by the Belgian population in all sex–age-specific groups in comparison with the US (males: 18·0 %; females: 18·1 %) and the Spanish populations (13·0 %).
Soya protein intakes were separately analysed in the present study, as soyabeans are rich sources of protein (35–49 %) and of essential amino acids(Reference Torres, Torre-Villalvazo and Tovar48, Reference Velasquez and Bhathena49). The analysis suggested that the consumption of the Belgian population was very low and lower than those of the Chinese Guangzhou populations (males: 0·111–0·228 and 3·6 g/d; females: 0·085–0·271 and 4·1 g/d, respectively)(Reference Zhang, Chen and Huang44) and of other East Asian populations (2·0–9·6 g/d, soya protein:total protein ratio: 3·5–15·3 %)(Reference Messina, Nagata and Wu50). This finding is supported by the European Prospective Investigation into Cancer and Nutrition study, which found that soya product intakes were low across all ten participating European countries(Reference Keinan-Boker, Peeters and Mulligan41).
BMI and animal and plant protein intake
The present results showed that animal protein intakes were positively associated with BMI of males, whereas plant protein intakes were inversely associated with the BMI of both sexes. After adjustment for potential confounders, these associations remained statistically significant. Others have reported similar results(Reference Mahon, Flynn and Stewart7, Reference Hermanussen51). Hermanussen(Reference Hermanussen51) concluded that the BMI of German male and female adolescents showed significant positive associations with total protein (r 0·143; P < 0·0001) and animal protein intakes (r 0·151; P < 0·0001). Plant protein intakes in the study of Mahon et al. (Reference Mahon, Flynn and Stewart7) were inversely associated with the BMI of the US OW post-menopausal women.
Other studies have, however, suggested an inverse relationship between both plant and animal protein intakes and BMI(Reference Liao, Shieh and Yang52, Reference Yamashita, Sasahara and Pomeroy53), which are supported by some separate studies on animal protein intake(Reference Hermanussen51, Reference Benito-Garcia, Feskanich and Hu54, Reference Xu, Yin and Tong55) and plant protein intake(Reference Allison, Gadbury and Schwartz11, Reference Alewaeters, Clarys and Hebbelinck56–Reference Perez-Guisado, Munoz-Serrano and Alonso-Moraga59). In relation to animal protein intake, some studies have reported different results(Reference Mahon, Flynn and Stewart7, Reference Umesawa, Sato and Imano60). Umesawa et al. (Reference Umesawa, Sato and Imano60), for instance, found no association between BMI and animal protein intake, while BMI decreased slightly when females increased their animal protein consumption. Two(Reference Umesawa, Sato and Imano60, Reference Sites, Cooper and Toth61) similar studies have reported that plant protein-based diets had no significant effect on the BMI of East Asian and Western populations.
Waist circumference and animal and plant protein intake
The WHO guidelines state that risks for metabolic complications increase in men with a WC ≥ 102 cm and in women with a WC ≥ 88 cm(62). Although the Belgian population had WC values below these cut-offs, the results of the present study indicate that Belgian females and the elderly in particular are at higher risk of being OW and obese.
The present findings also suggest that animal protein intakes might result in an increased WC for males, and plant protein intakes decrease in both males and females. This is in line with the observations that plant-based protein diets, compared with animal-based protein diets, have an inverse impact on WC of obese subjects(Reference Allison, Gadbury and Schwartz11, Reference Konig, Deibert and Frey63). For example, the results of a randomised controlled clinical trial on OW and obese people suggested that soya protein-based diets resulted in bigger reductions in participants' WC than those not consuming soya protein-based diets(Reference Allison, Gadbury and Schwartz11). Other studies(Reference Ouellet, Marois and Weisnagel27, Reference Liao, Shieh and Yang52, Reference Hermansen, Sondergaard and Hoie64, Reference Nakamura, Ueno and Tamaki65) have, however, reported the opposite. For instance, a randomised trial involving obese adults reported no significant difference between the effect of animal protein and plant protein on WC, with total protein intakes significantly lowering the WC (P < 0·05)(Reference Liao, Shieh and Yang52). Hence, the results of randomised trials indicate that plant protein-based diets have a more protective effect against OB than animal protein-based diets(Reference Liao, Shieh and Yang52, Reference Hermansen, Sondergaard and Hoie64, Reference Hoie, Morgenstern and Gruenwald66). Recent studies have, however, suggested that the negative relationship between animal protein and BMI refers only to OW and obese individuals and does not affect individuals with a normal BMI(Reference Farnsworth, Luscombe and Noakes26, Reference Abete, Parra and Crujeiras67, Reference Bellissimo, Desantadina and Pencharz68).
The mechanisms that relate animal and plant protein intakes with BMI and WC are unclear. One proposed mechanism is that animal proteins from beef, pork and poultry provide an important amount of energy and are positively associated with cholesterol and SFA intakes. Therefore, animal protein intake may result in an increase in BMI and the risk of OW and OB. The intake of plant proteins, conversely, is considered an important factor to control body weight and improved body composition and blood lipid profiles because of their associations with lower intakes of energy, total fat, cholesterol and SFA, and higher PUFA:SFA ratios(Reference Jenkins, Wong and Kendall16, Reference Berkow and Barnard69, Reference Gardner, Coulston and Chatterjee70).
Strengths and limitations of the study
This nutrition survey was representative for the Belgian population. One of the limitations of the present study is the use of self-reported body composition variables including weight and height. However, WC was measured by trained dietitians. Furthermore, the present study did not consider physical activity and energy expenditure, factors that could have an effect on the observed associations. Information on food intake was collected via two non-consecutive 24 h recalls, which allows statistical adjustments for within-person variability. Yet, one of the limitations of the 24 h recall method is that it does not allow quantifying proportions of non-consumers for particular food items, a fortiori for infrequently consumed foods. Moreover, information on the food consumption relies on individuals' memory and might therefore be biased towards misreporting. Additionally, underestimation or overestimation of portion sizes could result in inaccurate associations between dietary intake and body composition.
Conclusion
The results of the present study suggest that meat protein contributed most to animal protein intakes, and cereals and cereal products contributed to plant protein intakes. Animal and plant protein intakes were significantly different between males and females, and intakes decreased with age in both sexes. It was also observed that the consumption of legume- and soya-derived protein was very low in Belgium. Furthermore, the results indicated that animal protein intake was positively associated with BMI and WC of males, while plant protein intake was found to be negatively associated with BMI and WC of the whole population. The present study findings indicate that the intakes of plant protein could offer a potential protective effect against OW and OB.
Acknowledgements
The authors would like to acknowledge Mr Paul Bahta for the English proofreading of the manuscript. This study was supported by the ALPRO Foundation. The food consumption survey was funded by the Federal Ministry of Health, Food Chain Safety and Environment. Y. L. performed and interpreted the statistical analyses and drafted the manuscript. A. P. and M. D. N., the dietitians of our team, were responsible for the data linking with the food composition databases. S. D. V., H. V. O. and I. H. were responsible for the coordination of the fieldwork of the Belgian food consumption survey, and G. D. B. and S. D. H. were involved in the conceptualisation of the national food consumption survey. All other authors helped in the evaluation of the results and in the writing of the manuscript. All authors have evaluated and approved the final version of the manuscript. The authors declare no conflicts of interest.






