


A 59-year-old shipyard worker presented to the emergency department (ED) with the complaints of mid-thoracic back pain and fever, both of 1-day duration. He was seen by a general practitioner 3 days prior for epigastric pain (now resolved) and vomiting. In the ED, he was found to be tachycardic at 104 beats per minute and normotensive. Examination found only tenderness in the left iliac fossa and decreased left-sided breath sounds. He had a total white blood cell count of 5.32×109/L with 87% neutrophils. His procalcitonin was raised at 11.2 and lactate at 10.7. A chest radiograph was obtained (Figure 1).
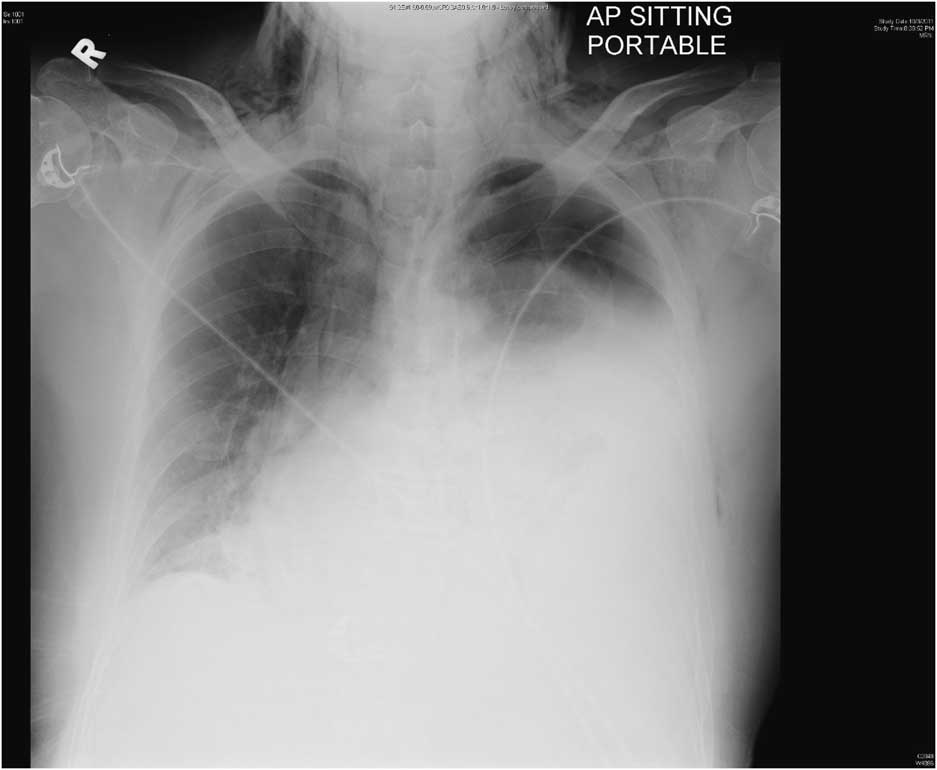
Figure 1 Chest radiograph showing left pleural effusion, left pneumothorax and subcutaneous emphysema involving the base of the neck and chest wall bilaterally.
DIAGNOSIS
Effort rupture of the esophagus (Boerhaave syndrome) is spontaneous perforation resulting from sudden increase in intraesophageal pressure such as from retching. It is rarely encountered in the ED, yet early diagnosis is crucial because survival decreases to 50% after 24 hours of delay in treatment and 10% after 48 hours.Reference Brinster, Singhal and Lee 1 Clinical presentation can be nonspecific with 50% present atypically. Retrosternal chest pain is the commonest symptom (85%);Reference Pate, Walker and Cole 2 25% to 45% may have no history of vomiting.Reference Brinster, Singhal and Lee 1 The diagnosis is suggested by chest radiograph and confirmed by computed tomogram.Reference de Lutio di Castelguidone, Merola and Pinto 3
This patient underwent a contrast-enhanced computed tomogram of the thorax and abdomen, which showed evidence of extensive subcutaneous emphysema and pneumomediastinum, a large left hydropneumothorax with passive collapse of the left lung, a mild right pleural effusion, intact tracheal walls, and a sliding hiatal hernia. He was brought to the operating room for emergency thoracotomy. Operative findings were of a perforation in the lower third of the esophagus marked by extensive necrosis along with the nearby pleura and pericardium. He underwent debridement and insertion of chest drains, an open gastrostomy, and a feeding jejunostomy. He was transferred out of the intensive care unit on Day 8.
Competing interests: None declared.

