


Breakfast consumption is an important part of a healthy lifestyle( Reference Rampersaud, Pereira and Girard 1 ). Regular breakfast consumption among adolescents has been associated with better diet quality( Reference Ruxton and Kirk 2 – Reference Sjöberg, Hallberg and Höglund 4 ), better cognitive performance( Reference Hoyland, Dye and Lawton 5 ) and reduced risk of becoming overweight or obese( Reference Szajewska and Ruszczynski 6 ). Nevertheless, breakfast skipping is a common behaviour among European adolescents, with a prevalence ranging from 3 %( Reference Dialektakou and Vranas 7 ) to 34 %( Reference Rampersaud, Pereira and Girard 1 ).
A ‘good-quality’ breakfast can impact favourably on adolescent mental health( Reference O'Sullivan, Robinson and Kendall 8 ) and cognitive performance( Reference Wesnes, Pincock and Richardson 9 ) and improve the overall diet quality( Reference Matthys, De Henauw and Bellemans 3 , Reference Raaijmakers, Bessems and Kremers 10 ). Preferably, breakfast should include products from each of the dairy, cereal and fruit groups( Reference Giovannini, Verduci and Scaglioni 11 ). However, these three food groups were found to be consumed for breakfast by only 10 % of adolescents in studies from Belgium( Reference Matthys, De Henauw and Bellemans 3 ) and The Netherlands( Reference Raaijmakers, Bessems and Kremers 10 ) and by 5 % of adolescents in a study from Spain( Reference Aranceta, Serra-Majem and Ribas 12 ). Milk and cereal are commonly consumed at breakfast in many child and adolescent populations in Western countries( Reference Rampersaud, Pereira and Girard 1 ), while fruit is less common( Reference Raaijmakers, Bessems and Kremers 10 , Reference Aranceta, Serra-Majem and Ribas 12 ).
Previous studies in European adolescents have focused mainly on breakfast consumption v. skipping( Reference Szajewska and Ruszczynski 6 , Reference Vereecken, Dupuy and Rasmussen 13 ). These studies have shown that daily breakfast consumption decreases with age( Reference Raaijmakers, Bessems and Kremers 10 , Reference Vereecken, Dupuy and Rasmussen 13 , Reference Croezen, Visscher and Ter Bogt 14 ), and is associated with sex – girls were less likely to be daily breakfast consumers than boys( Reference Raaijmakers, Bessems and Kremers 10 , Reference Vereecken, Dupuy and Rasmussen 13 – Reference Johansen, Rasmussen and Madsen 16 ) – and socio-economic factors( Reference Vereecken, Dupuy and Rasmussen 13 , Reference Lien 15 , Reference Johansen, Rasmussen and Madsen 16 ). Studies on breakfast quality and sociodemographic factors at European level among adolescents are, however, scarce. Low levels of breakfast consumption can be considered a public health issue but in order to be able to promote breakfast consumption it is first crucial to understand potential differences in breakfast habits among European adolescents, by sex, socio-economic factors and geographical factors.
The aim of the present study was therefore to describe the breakfast habits (in terms of both frequency and quality) at food group level in European adolescents. Additionally we wanted to investigate associations between these habits and sociodemographic factors such as sex, age, region in Europe, parental education, family structure and family affluence.
Methods
Study design and sampling
The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study is a school-based multi-centre study, designed to obtain reliable and valid data on nutrition and health-related factors from a sample of 3528 adolescents (52 % girls) aged 12·50–17·49 years in ten European cities( Reference Moreno, De Henauw and Gonzalez-Gross 17 ). The selected cities are Athens (Greece), Dortmund (Germany), Ghent (Belgium), Heraklion (Greece), Lille (France), Pecs (Hungary), Rome (Italy), Vienna (Austria), Stockholm/Västerås (Sweden) and Zaragoza (Spain).
The selection of the European cities was primarily a practical one. As it was not realistic to include a random sample of all European adolescents, it was decided to study a city-based sample, striving for representativeness of adolescents living in European cities. Within these cities, schools were randomly selected, but stratified for geographical location. Within the participating schools, classes were randomly selected, stratified by grade. In all countries it was compulsory to go to school at these ages and our aim was to reach a sub-sample from the whole population in these ages.
All pupils of the selected classes were invited to participate. A class was considered eligible if the participation rate was at least 70 %. The final database included only those participants who met the following criteria: they were between 12·50 and 17·49 years of age, they and their parents had provided written informed consent, and their weight and height had been measured. Participants were excluded if they were participating simultaneously in another clinical trial or had had an acute infection less than one week before the study. The adolescents completed in-class surveys, two non-consecutive computer-based 24 h dietary recalls and physical tests during the 2006–2007 academic year. A more detailed description of the study design, sampling and procedure has previously been published( Reference Moreno, De Henauw and Gonzalez-Gross 17 ). Both parents and adolescents gave written informed consent, and the HELENA study protocol was approved by the national or local independent ethical committee from the relevant European city( Reference Beghin, Castera and Manios 18 ).
The present paper includes data of 2672 adolescents from nine cities (53 % girls), with a mean age of 14·8 (sd 1·2) years. Data from Heraklion (Greece) are not used in the present analysis because only one 24 h dietary recall was collected in the majority of adolescents.
Sociodemographic measurements
Socio-economic factors were assessed, during the in-class surveys, via the questionnaire ‘Your Living Environment’( Reference Iliescu, Beghin and Maes 19 ). This questionnaire gathered general information about the education level of parents, family structure and family affluence. This latter variable was measured using a modified version of the family affluence scale (FAS), a scale developed by the WHO collaborative Health Behaviour in School-aged Children (HBSC) Study( Reference Boyce, Torsheim and Currie 20 ). A sum score of the following items was used: whether the adolescent had his/her own bedroom, the number of cars in the family, the number of computers and the presence of an Internet connection at home. The FAS was dichotomized to ‘low family affluence’ (FAS score ≤3) v. ‘high family affluence’ (FAS score ≥4).
Maternal and paternal education level was dichotomized into ‘low/medium education’ (elementary, lower secondary, higher secondary education) and ‘high education’ (university education). The family structure variable was derived from the question ‘With whom do you principally stay?’. Adolescents who chose ‘with both of your parents’, ‘with your mother and her partner’ or ‘with your father and his partner’ were considered to have a ‘traditional’ family structure. Adolescents who chose ‘with your mother’, ‘with your father’, ‘with your mother half of the time and your father half of the time’, ‘with your grandparents or other relatives’, ‘with your foster or adoptive parents’ or ‘in an orphanage or somewhere else’ were considered to have a ‘single-parent/shared-care’ family structure.
Data on sex, age and study centre were collected by a physician. Age was dichotomized to younger or older than 15 years of age. The variable ‘study centre’ was dichotomized into northern/central (Dortmund, Ghent, Lille, Pecs, Vienna and Stockholm/Västerås) and southern (Athens, Rome and Zaragoza).
All of the questionnaires included in the study were discussed and approved by the HELENA partners. After consensus was reached, the questionnaires were translated and back-translated into the native language of the participants( Reference Iliescu, Beghin and Maes 19 ).
Dietary survey
Dietary intake data were obtained using a dietary assessment tool named HELENA-DIAT, which was based on a self-administered, computerized 24 h dietary recall program called Young Adolescents’ Nutrition Assessment on Computer (YANA-C)( Reference Vereecken, Covents and Sichert-Hellert 21 , Reference Vereecken, Covents and Matthys 22 ). The program contains questions related to six meal occasions (i.e. breakfast, morning snacks, lunch, afternoon snacks, evening meal, evening snacks) with questions designed to prompt the adolescents to remember what they ate. The first two questions asked about the time they got up the previous day and if they had breakfast. If they responded no, they were prompted with an additional question ‘You didn't have anything, however small, to eat or drink for breakfast?’. If the adolescents had breakfast, a drink or something small, they were asked ‘Where and with whom did you have breakfast, yesterday?’ and ‘Around what time was that?’. Then, adolescents selected the food items consumed from a culturally adapted list and further described the quantity consumed. Pictures and measurement units helped the adolescents to give quantitatively detailed information( Reference Vereecken, Covents and Sichert-Hellert 21 , Reference Vereecken, Covents and Matthys 22 ). Two computerized 24 h recalls were performed on two non-consecutive days within the space of two weeks. The HELENA-DIAT was filled in by the adolescents at school, and it took about 10–30 min to complete.
Breakfast patterns
Based on reported breakfast consumption the adolescent was classified as a ‘breakfast consumer’ (i.e. they consumed breakfast on at least one recall day) or a ‘breakfast skipper’ (i.e. they did not consume breakfast on either of the two recall days). According to one previous study( Reference Alexy, Wicher and Kersting 23 ), a breakfast meal should weigh more than 15 g to be considered a meal. In our study five breakfast meals weighed less than 15 g and were excluded. The computer program initially categorized foods into twenty-seven food groups (Table 1), but because many of the food groups were infrequently consumed for breakfast we merged similar groups and reduced this number to seventeen (Tables 2 to 4). All food items were classified as being consumed (on one or both of the recall days) or not consumed (not on either of the two recall days). For the purpose of the study, breakfast quality was related to the presence (irrespective of amount) of food items from three specific food groups: cereal products (‘bread’ and ‘breakfast cereals’), dairy products (‘milk and yoghurt’ and ‘cheese’) and fruit/vegetables (‘fruit & vegetables’ and ‘fruit juice’). Additionally, a ‘breakfast quality index’ was created in which 1 point was awarded for consuming a breakfast and an extra 1 point was awarded for each of the three food groups (hereafter called ‘target food groups’) consumed (i.e. 1 to 3 extra points), resulting in a possible score of 0 to 8 across both days. Adolescents consuming a breakfast that scored highly (≥6 points) were considered to have a ‘high quality breakfast’ while those who scored lowly (<4 points) were considered to have a ‘low quality breakfast’.
Table 1 Percentage of adolescents consuming twenty-seven food groups and the median (P25–P75) consumption on the days the food was consumed (observed sample): adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

P25, 25th percentile; P75, 75th percentile.
*Gram consumed on consumption days.
†Milk-based dessert and cream.
‡Potatoes, pulses, etc.
§Oats and rice.
Table 2 Percentage of consumers of breakfast and of seventeen food groups for breakfast by sociodemographic factors (observed sample): adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

FAS, family affluence scale.
*The proportion of adolescents who consumed the different food items (on one or both days).
†Breakfast consumption on at least one day.
‡Milk-based dessert, sugared milk and cream.
§Breakfast cereals and other cereals.
Statistical analyses
All analyses were performed using the statistical software package IBM SPSS Statistics version 19·0 for Windows (IBM SPSS Inc., Chicago, IL, USA), and the level of significance was set at 5 %. We used percentage, median and 25th and 75th percentiles for describing breakfast consumers and the total quantity of each food group consumed for breakfast (g/d).
Multiple logistic regression analyses were used to investigate the associations with breakfast consumption and food groups for breakfast (dependent variables) according to sociodemographic variables (independent variables). All multiple logistic regression models included sex (boy v. girl), age (<15 years v. ≥15 years), region (southern v. northern/central), maternal and paternal education level (low/medium v. high), family structure (traditional v. single parent/shared care) and FAS score (low v. high) as independent variables.
Multiple linear regression analyses were performed to evaluate associations between the breakfast quality index (continuous) and sex, age (in years, continuous), region, maternal and paternal education level, family structure and FAS score as independent variables. All analyses were adjusted by a weighting factor to balance the sample according to the age and sex distribution of the theoretical sample, to guarantee representation of each of the stratified groups.
Results
Population characteristics
Table 2 shows that 53 % of the population were girls, 56 % were under 15 years of age and 29 % came from the southern part of Europe. One-third of the adolescents had highly educated mothers, one-third had highly educated fathers and 80 % were living in a traditional family structure. Three-quarters (77 %) indicated that their family was affluent, as defined by the FAS.
Breakfast consumption according to sociodemographic factors
We observed that 7 % of the adolescents were ‘breakfast skippers’ (Fig. 1). Breakfast consumption, on both recall days, was reported among 77 % of the adolescents (data not shown). Younger adolescents (<15 years of age) reported more often than older adolescents that they were ‘breakfast consumers’ (OR = 1·66; 95 % CI 1·17, 2·35). Fewer adolescents with a low/medium maternal education level indicated that they were ‘breakfast consumers’ compared with adolescents with a high maternal education level (OR = 0·61; 95 % CI 0·38, 0·98). There were no significant differences in breakfast consumption (‘consumer’ v. ‘skipper’) by sex, region, paternal education, family structure and FAS (Tables 3 and 4).
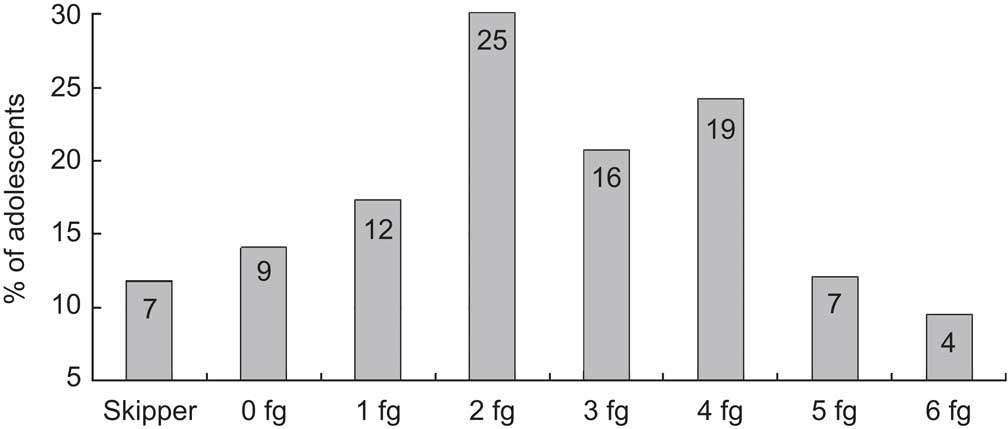
Fig. 1 Breakfast skippers and total number of target food groups (fg) consumed at breakfast over both recall days (maximum: three per day) in the study population: adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study
Table 3 Results of multivariate logistic regression analyses with consumption of breakfast and of food groups as dependent variables and sociodemographic factors as independent variables: adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

Odds ratios and 95 % confidence intervals weighted for age and sex. Reference categories: boys, ≥15 years of age and southern Europe.
*Breakfast consumed on one or both of the recall days.
†Milk-based dessert, sugared milk and cream.
‡Breakfast cereals and other cereals.
Table 4 Results of multivariate logistic regression analyses with consumption of breakfast and of food groups as dependent variables and sociodemographic factors as independent variables: adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

FAS, family affluence scale.
Odds ratios and 95 % confidence intervals weighted for age and sex. Reference categories: high maternal education, high paternal education, traditional family structure and high FAS.
*Breakfast consumed on one or both recall days.
†Milk-based dessert, sugared milk and cream.
‡Breakfast cereals and other cereals.
Breakfast quality according to sociodemographic factors
We found that 4 % of the sample consumed all three of the target food groups on both recall days (Fig. 1). Figure 1 also shows that 53 % of the adolescents consumed products from two or fewer of the target food groups.
Breakfast quality was higher in adolescents from the northern and central part of Europe (β = 0·142, P < 0·001), in those whose mothers had a high education level (β = 0·129, P < 0·001), in those reporting higher family affluence (β = 0·068, P = 0·002) and in those coming from a traditional family structure (β = 0·055, P = 0·006). Breakfast quality was lower among older adolescents than among younger (β = −0·063, P = 0·001). There was no association between breakfast quality and sex or paternal education (Table 5).
Table 5 Multiple regression analyses exploring the association between breakfast quality index* and sociodemographic factors: adolescents (n 2672) aged 12–17 years from nine European cities participating in the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

FAS, family affluence scale.
*Breakfast quality index score has nine categories from skipper (score of 0) to three target food groups consumed on both days (score of 8).
†Age is a continuous variable.
Food groups consumed at breakfast according to sociodemographic factors
Table 3 shows that girls were more likely to consume ‘tea and coffee’ and ‘butter’ but less likely to consume ‘meat, fish and eggs’ (all P < 0·05) for breakfast than boys. Younger adolescents (<15 years of age) were more likely to consume ‘other milk products’ (P < 0·001) and less likely to consume ‘tea and coffee’, ‘water’ and ‘added sugar’ (all P < 0·05) than older adolescents. Adolescents from northern/central parts of Europe were more likely to consume a drink (tea, coffee, fruit juice and soft drink; all P < 0·0 0 1) for breakfast compared with those from the southern part of Europe. They were also more likely to consume ‘cheese’, ‘other milk products’, ‘meat, fish and eggs’, ‘fruit and vegetables’, ‘bread’, ‘cereals’ and ‘added fat or oil’ and less likely to consume ‘milk and yoghurt’, ‘cakes’, ‘sweets’ and ‘added sugar’ (all P < 0·001) for breakfast compared with their counterparts from southern Europe.
Adolescents whose mothers had a low/medium education level were less likely to consume ‘fruit juice’ and ‘milk and yoghurt’ and more likely to consume ‘soft drinks’ (all P < 0·001) and ‘fruit and vegetables’ and ‘bread’ (both P < 0·05) for breakfast compared with those whose mothers had a high education level (Table 4). Adolescents from single-parent/shared-care families were less likely to consume ‘sweets’ (P < 0·01) for breakfast compared with those from traditional families. Adolescents who reported lower family affluence were less likely to consume ‘fruit juice’ and ‘milk and yoghurt’ (both P < 0·01) and to consume ‘cereals’ and ‘sweets’ (both P < 0·001); they were also more likely to consume ‘other milk products’ (P < 0·01), ‘meat, fish and eggs’ and ‘vegetable fat’ (both P < 0·001) for breakfast compared with those who reported greater family affluence. There were no significant differences in food groups consumed for breakfast by level of paternal education (Table 4).
Discussion
The aim of the present study was to describe breakfast habits (in terms of both frequency and quality) at food group level in European adolescents. Additionally we wanted to investigate the associations between these habits and sociodemographic factors such as sex, age, region in Europe, parental education, family structure and family affluence.
The main findings of the study are that the majority of the adolescents studied consumed some form of breakfast, but that the quality was rather low. We also found that breakfast habits were associated with age, region in Europe, maternal education, family structure and family affluence. Breakfast skipping (not consuming breakfast on any of the two recall days) was reported by 7 % of the adolescents, a figure which is in agreement with other studies among European adolescents( Reference Rampersaud, Pereira and Girard 1 , Reference Vereecken, Dupuy and Rasmussen 13 ). With regard to breakfast quality, our study shows that the majority of the adolescents (96 %) did not consume a breakfast including foods from all three of the target food groups on both recall days. Additionally, half of the adolescents consumed products from no more than two of the target food groups together during both the recall days. Similar results were reported in a Dutch study( Reference Raaijmakers, Bessems and Kremers 10 ) and in Spanish children and adolescents( Reference Aranceta, Serra-Majem and Ribas 12 ).
Sex differences in breakfast consumption have been reported in other studies( Reference Rampersaud, Pereira and Girard 1 , Reference Vereecken, Dupuy and Rasmussen 13 ); however, we found no differences between boys and girls in either frequency of breakfast consumption or breakfast quality. We did observe that girls were more likely to drink/eat ‘tea and coffee’ and ‘butter’ and less likely to eat ‘meat, fish and eggs’ for breakfast than boys, which concurs with results from other studies( Reference Raaijmakers, Bessems and Kremers 10 , Reference Von Post-Skagegard, Samuelson and Karlstrom 24 ).
Adolescents under the age of 15 years were more likely to be breakfast consumers and to consume more of the target food groups for breakfast than older adolescents. Aranceta et al. reported similar results in Spanish adolescents( Reference Aranceta, Serra-Majem and Ribas 12 ). Other authors have also shown that younger European adolescents consume breakfast more often than their older counterparts( Reference Rampersaud, Pereira and Girard 1 , Reference Raaijmakers, Bessems and Kremers 10 , Reference Vereecken, Dupuy and Rasmussen 13 ). More autonomy and independence in regard to food choices among older adolescents could explain the age decline in breakfast consumption( Reference Story, Neumark-Sztainer and French 25 ). Younger adolescents were also more likely to drink ‘other milk products’ and less likely to consume ‘tea and coffee’, ‘water’ or ‘added sugar’ in comparison to older adolescents. This is in contrast to Raaijmakers et al. who showed that higher consumption from the liquid group was more common among older adolescents( Reference Raaijmakers, Bessems and Kremers 10 ).
Adolescents from northern and central parts of Europe were more likely to score more highly on the breakfast quality index and were more likely to consume the target food groups than those from southern Europe. Risvas et al. suggested that Greek students have learnt to categorize food as ‘healthier but less tasty’ and ‘appealing but unhealthy’( Reference Risvas, Panagiotakos and Zampelas 26 ), while Finnish adolescents perceived e.g. healthy bread as pleasant and very acceptable( Reference Pohjanheimo, Luomala and Tahvonen 27 ). These attitudinal differences to healthy food between countries might explain why we saw a higher score on the breakfast quality index among adolescents in the northern and central part of Europe.
We did not find significant differences in breakfast consumption v. skipping between the two regions in Europe. Vereecken et al. reported differences in the frequency of breakfast consumption among different countries in Europe; in the southern region daily breakfast consumption varied from 33 % (Greek girls) to 72 % (Spanish boys), while in the northern/central region the daily breakfast consumption ranged from 42 % (Hungarian girls) to 73 % (Swedish boys)( Reference Vereecken, Dupuy and Rasmussen 13 ). Differences in breakfast consumption have also been reported between Greece and Finland( Reference Veltsista, Laitinen and Sovio 28 ). It could be that many inter-country differences are even more pronounced than inter-regional differences, which may explain why we did not observe any differences in breakfast consumption between our two regions, but further studies are required to confirm this theory.
Socio-economic status seems to be associated with dietary habits among adolescents but not to the same extent as in adults( Reference Hanson and Chen 29 ). One reason for this could be that peers influence the adolescent's behaviour even more than does the family's socio-economic status. In our study, the only socio-economic variable that was associated with breakfast consumption was maternal education level; adolescents whose mothers had a high education level were more likely to be breakfast consumers compared with adolescents whose mothers had a low/medium education level. Similar results have been found in Norway( Reference Lien 15 ) and the USA( Reference Franko, Thompson and Bauserman 30 , Reference Timlin, Pereira and Story 31 ). Additionally, our study shows that adolescents whose mothers had a high education level were more likely to consume a breakfast of higher quality, to consume the target food groups and were less likely to consume ‘soft drinks’ for breakfast. Similar patterns have been shown in Norway( Reference Nilsen, Krokstad and Holmen 32 ). Mothers have a strong influence on the dietary habits of their families and influence the family food environment, and mothers who are more educated may be more likely to consider health in their choice of foods( Reference Hanson and Chen 29 , Reference Pearson, Biddle and Gorely 33 ).
Adolescents reporting higher family affluence were more likely to consume a breakfast of higher quality, to consume the target food groups and to consume ‘sweets’, but less likely to consume ‘other milk products’, ‘meat, fish and eggs’ and ‘vegetable fat’ for breakfast in comparison to those reporting low family affluence. The HBSC Study showed an association between a high score on the FAS and breakfast consumption in five of the countries included in HELENA (Belgium, France, Germany, Hungary and Sweden)( Reference Vereecken, Dupuy and Rasmussen 13 ). Higher fruit consumption among the more affluent adolescents has also been shown in the HBSC Study( Reference Vereecken, Inchley and Subramanian 34 ). Less affluent families might have less money to spend on food( Reference Roos, Prattala and Lahelma 35 ) and when cost is a barrier families might be less likely to consider health in their choice of food.
Finally, adolescents from a ‘traditional’ family structure were more likely to report a high-quality breakfast and were also more likely to eat ‘sweets’ for breakfast compared with those from single-parent/shared-care families. A similar association between breakfast consumption and this family structure were observed in the HBSC Study, among the countries included in HELENA, with the exception of Greece( Reference Vereecken, Dupuy and Rasmussen 13 ). Family cohesion has been found to be associated with breakfast consumption and decreased soda intake in a population of girls in the USA( Reference Franko, Thompson and Bauserman 30 ). One possible explanation for the higher quality of breakfast in adolescents from traditional families could be that these adolescents could be more likely to comply with their parents’ wishes regarding breakfast consumption and the family may be more likely to consume breakfast together.
Strengths and limitations
The strengths of our study include the large sample of adolescents. Our aim was to reach a sub-sample within each country that was representative of the whole population of adolescents in Europe regarding sex, age and socio-economic status. As it was compulsory in all countries for this age group to attend school and as we collected the data in large cities, we assert that the sample will be representative of large cities in Europe. The standardized and harmonized methodology is also a study strength. The computerized 24 h recall method provides both frequency and quality data about the breakfast and two non-consecutive 24 h recalls have shown to be a relatively reproducible estimate of the mean usual intake of a group( Reference Gibson 36 ).
Some limitations of the current study include the fact that there is no accepted definition of breakfast in the literature; although the issue has been discussed at length( Reference Giovannini, Verduci and Scaglioni 11 ), no consensus has been reached. For the purpose of our study we defined high and low breakfast quality based on a relatively simple index that considered both breakfast consumption and consumption of three desirable target food groups. The index does not allow for other food groups that may also be considered nutritious, nor can it take into account whether undesirable food groups were also consumed and in what quantities. The fact that the study population comes only from urban areas could mean that the sociodemographic distribution is not representative of the total population of the nine countries studied. The inability to compare the results between the different countries in Europe( Reference Moreno, De Henauw and Gonzalez-Gross 17 ) is also a limitation as heterogeneity in breakfast habits between European countries has been reported( Reference Vereecken, Dupuy and Rasmussen 13 ). The 24 h recall was collected during school time on weekdays, so there are no Fridays and Saturdays in the dietary recall database; this could influence the results as differences in dietary intakes between weekdays and weekends have been reported( Reference Gibson 36 ).
Implications for further research
The public health implications of poor breakfast consumption habits are considerable and our finding that only 4 % of European adolescents consumed a high-quality breakfast highlights the need to promote breakfast, especially a high-quality breakfast, among adolescents. Particular attention should be paid to older adolescents, adolescents from the southern part of Europe and adolescents from families with low socio-economic status.
More specific information about the breakfast habits among European adolescents in larger country samples is needed to facilitate inter-country comparisons.
Conclusions
The majority of the adolescents consumed a ‘low-quality’ breakfast. Older adolescents, adolescents from the southern part of Europe (Greece, Italy and Spain) and adolescents from families with low socio-economic status were more likely to consume a ‘low-quality’ breakfast.
The study highlights the need to promote ‘high-quality’ breakfast among adolescents, particularly to older adolescents, adolescents from southern Europe and adolescents from families with low socio-economic status.
Acknowledgements
The study took place with financial support from the European Community Sixth RTD Framework Programme (Contract FOOD-CT-2005-007034); the Swedish Council for Working Life and Social Research (FAS), the Swedish Heart-Lung Foundation (20090635); and the Spanish Ministry of Health: Maternal, Child Health and Development Network (number RG08/0072). The contents of this article reflect only the authors’ views and the European Community is not liable for any use that may be made of the information contained therein. The writing group takes sole responsibility for the content of this article. None of the authors had a personal of financial conflict of interest. L.H., C.A.V., I.L. and J.R.R. wrote the manuscript and performed the statistical analysis; L.H., C.A.V., I.L., J.R.R., C.L.D., M.C.G., C.C.G., S.G.M., E.G., I.H., A.K., M.K., Y.M., D.M., E.P., K.W., T.D.V., L.A.M. and M.S. contributed to the interpretation and discussion of the results and critically revised the drafted manuscript. The authors thank all the adolescents who took part in the HELENA study.






