



In the 1990s, the “hyperdense middle cerebral artery (MCA) sign” on an unenhanced CT scan was recognized as highly specific for an embolic occlusion of the MCA and quite easily seen on an axial cut through that artery’s horizontal segment in the Sylvian fissure. Reference Bastianello, Perallini and Colonnese1,Reference von Kummer, Meyding-Lamade and Forsting2 Although a CT sign with low overall sensitivity for detection of an occluded MCA, it was the only available marker of large vessel occlusion before the introduction of computed tomographic angiography. When found in a patient with sudden contralateral hemiplegia, an urgent neurology consult was sought and, in some cases, one from neurosurgery as well. My personal interest in micro neurosurgery and stroke (I was the principal surgeon in our city for the North American Symptomatic Carotid Endarterectomy Trial) 3 was being increasingly recognized in my hospital.
Given the generally very poor prognosis of patients presenting with proximal MCA occlusion (M1 segment) and hemiplegia (i.e., death or dependency), emergency MCA microsurgical embolectomy was an option, provided that an established MCA territory infarct was not evident on CT. Between 1990 and 1999, we performed 10 MCA embolectomies: 3 based on the hyperdense MCA sign followed by catheter angiography to confirm and the next 7 based on the MCA hyperdense sign alone to save valuable time. The mean time from stroke onset to revascularization in our small series was 4 hours. Postoperative patency was proven in 9 of the 10, with the remaining patient having died from a hemorrhagic transformation shortly after surgery. Follow-up CT imaging showed mostly small deep perforator zone infarctions in eight patients and MCA branch infarcts in four, but there were no whole MCA territory infarctions. At 3–6 months post-stroke, all nine surviving patients had a minor to moderate stroke deficit (modified Rankin score 3 or better). We considered these results in this small case series quite good compared to what we assumed was the natural history with medical management alone.
Intracranial embolectomy was rarely performed but certainly not a new operation in the 1990s. The first MCA embolectomy was reported in 1957 by Welch, Reference Welch4 followed by another report by Jacobson et al. in 1962 Reference Jacobson, Wallman, Schumacher, Flanagan, Suarez and Donaghy5 and a subsequent report in 1963 by Chou. Reference Chou6 An intracranial internal carotid saddle embolus extending into both the MCA and anterior cerebral arteries was microsurgically removed in 1963 by the neurosurgeon Lougheed, who then reported the case in 1965 along with neurologists Gunton and Barnett at the Toronto General Hospital. Reference Lougheed, Gunton and Barnett7 In 1985, Meyer and colleagues at the Mayo Clinic reviewed 64 reported cases of intracranial embolectomies and presented their own series of 20 who underwent embolectomy for acute occlusion of the MCA between 1970 and 1983. Reference Meyer, Piepgras, Sundt and Yanagihara8 Seventy percent of their patients had a fair to good outcome, two died, and collateral flow, as judged from the preoperative angiogram, was the best predictor of a good prognosis. Despite these positive reports (surgical “tour de force” publications, not unlike our own), intracranial embolectomy was almost never done. Patients who could have been considered were not referred to surgeons with the appropriate skill set (and there were not many) within a time frame where revascularization might be successful in averting a major stroke.
The local and then national opinion of presentations of our approach and early results with MCA embolectomies Reference Findlay9 (Figures 1 and 2) was critical, with the operation considered reckless and unproven. Anticipating a poor reception, at the beginning of my presentation at the Canadian Congress in 1997, I warned the audience of mostly neurologists (including several very eminent Canadian stroke neurologists) that “I am going to try to not leave time for questions or comments.” However, the moderator allowed the discussion to proceed over time, providing ample time for (mostly) polite condemnation to ensue.
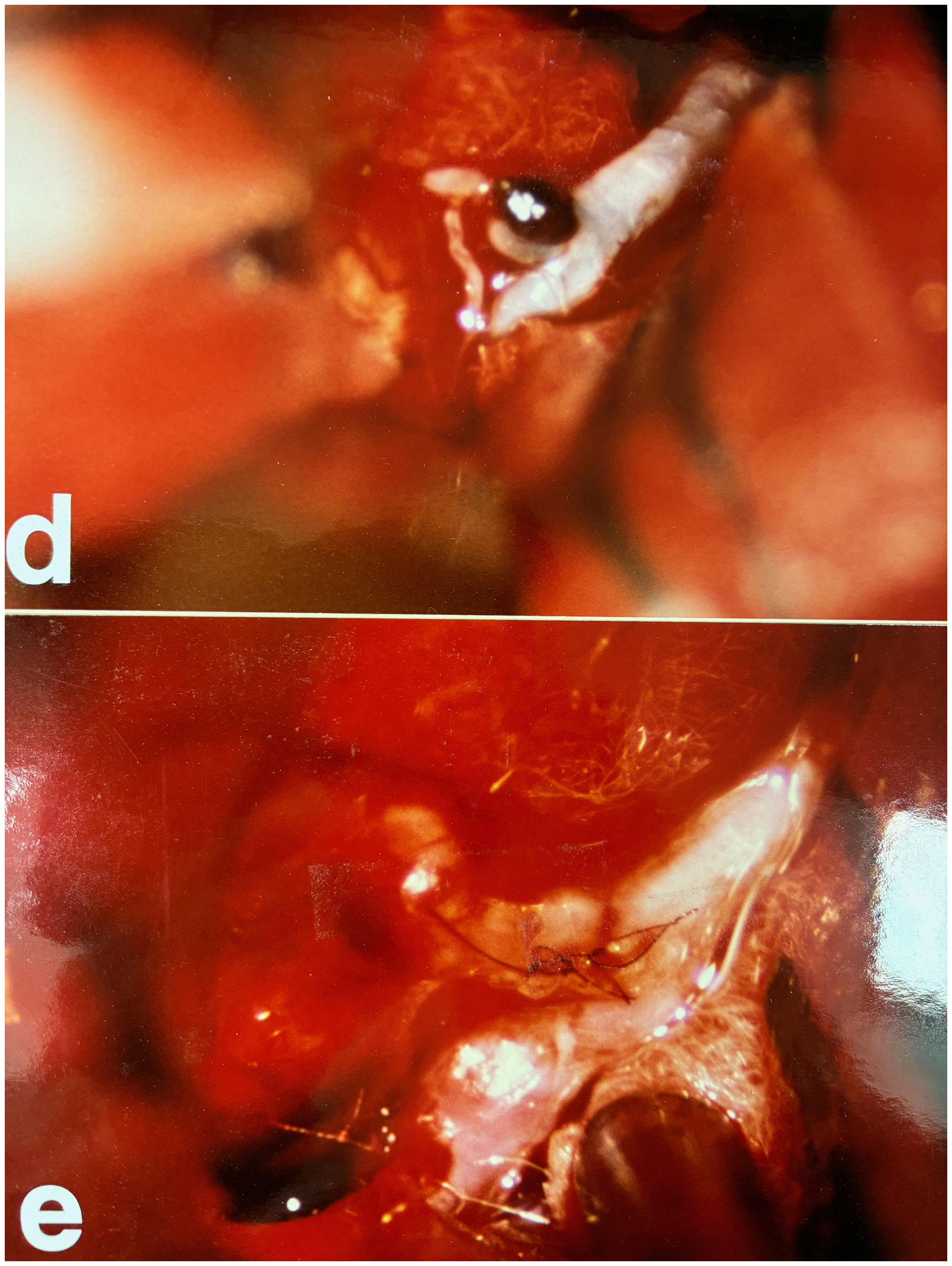
Figure 1. Photographs of a left middle cerebral artery embolectomy microembolectomy. Panel “d” shows thrombus herniating from an arteriotomy in the inferior M2 division, and panel “e” shows the arteriotomy closure with three interrupted 9-0 Prolene sutures.
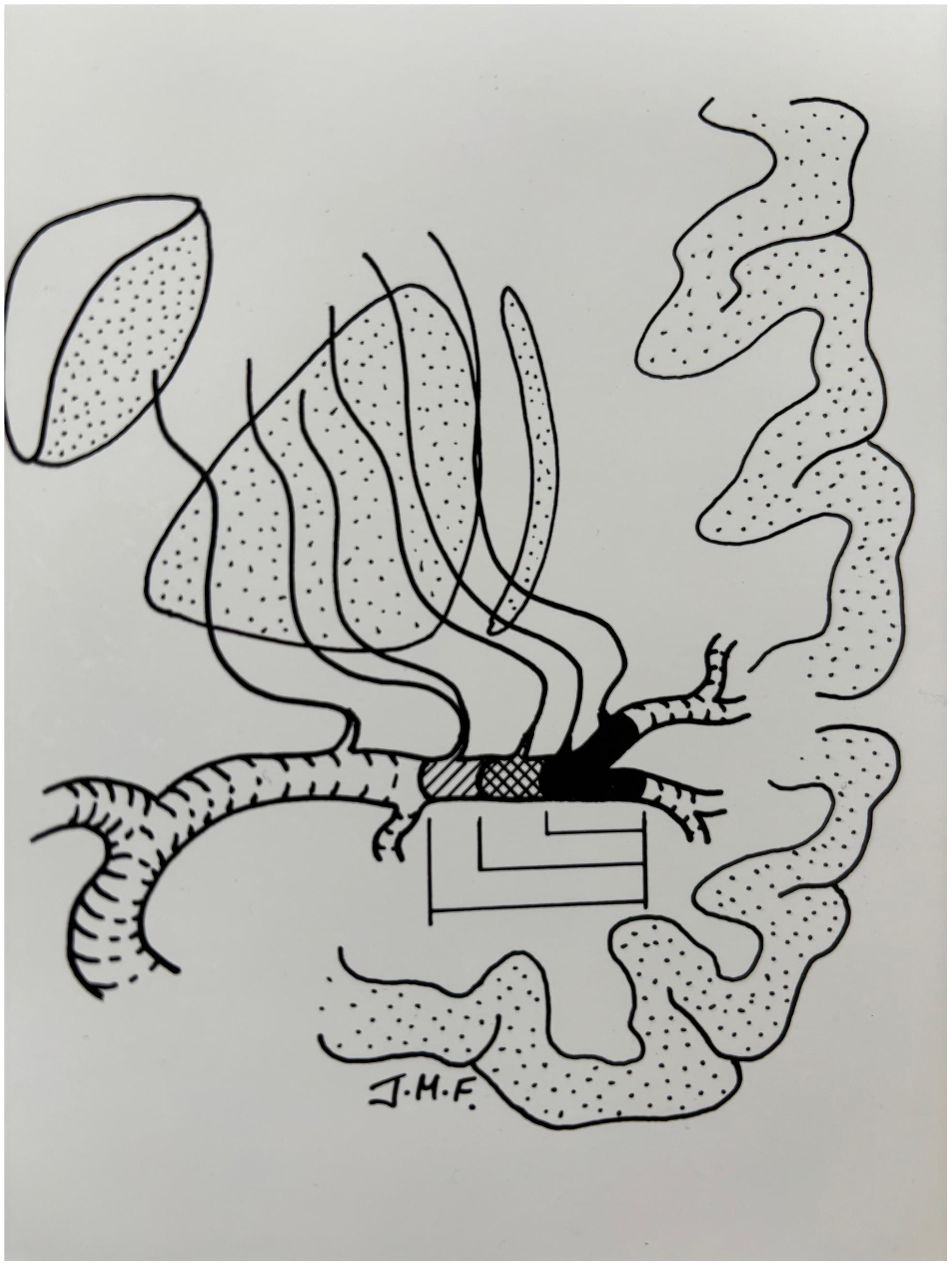
Figure 2. A diagram explaining the size and extent of the deep “perforator” infarcts uniformly seen in our middle cerebral artery embolectomy case series.
To be fair, 1997 was a time when a “proven” reperfusion treatment had just arrived on the stroke scene, namely, the thrombolytic agent recombinant human tissue plasminogen activator (rt-PA or simply t-PA, aka “alteplase”), administered intravenously (10% of a 0.9 mg/kg dose given as a bolus and the remainder infused over the following hour) within 3 hours of stroke onset, provided the patient’s CT scan was relatively normal. 10 The NINDs trials showed that compared to patients given placebo, patients treated with t-PA were at least 30% more likely to have no or minimal disability at 3 months. Intravenous alteplase given in the emergency department versus an emergency craniotomy for an acute ischemic stroke was no contest, and acute stroke referrals to our neurosurgical service soon ended. The NINDs t-PA trial led to a new standard of care, and acute stroke protocols were established by emerging “stroke services,” generally led by neurologists.
Interventional neuroradiology was becoming established as a subspecialty in the 1990s, and there was a growing interest in intraarterial thrombolysis for acute ischemic stroke. Large vessel occlusions were the target, where the likelihood of successful recanalization with intravenously administered alteplase was increasingly recognized as being less likely than in more distal occlusions. Reference Tomsick, Brott and Barsan11 The “Prolyse in Acute Cerebral Thromboembolism Trials (PROACT)” I and II were published in 1998 and 1999, respectively. Reference Del Zoppo, Higashida and Furlan12,Reference Furlan, Higashida and Wechsler13 In brief, intraarterial recombinant pro-urokinase (“prolyse” another thrombolytic agent), given within 6 hours of stroke onset and administered through a microcatheter directly proximal and into emboli, resulted in a higher rate of recanalization than placebo and improved outcome. Prolyse was never approved by the FDA for acute stroke, which cited the need for a larger confirmatory trial that was never performed. When the FDA revoked prolyse’s GMP (Good Manufacturing Process) certificate, it became unavailable for use, and for a time, alteplase was used instead but also recognized as being far too slow. Faster, more effective endovascular revascularization techniques were needed and indeed were in development.
In 2000, Chopko and colleagues published the first reported case of a transfemoral endovascular “mechanical” clot retrieval of an MCA embolus using a “gooseneck snare” after an unsuccessful attempt at intraarterial thrombolysis. Reference Chopko, Kerber, Wong and Georgy14 The 38-year-old patient made a rapid recovery. The era of trans-arterial mechanical thrombectomy began with the development of the corkscrew-like “MERCI” (Mechanical Embolus Removal in Cerebral Ischemia) clot retriever device, designed at the University of California in 2001 and the first device approved in the USA to remove intracranial emboli in 2004. Reference Smith and Furlan15 The feasibility and efficacy of this first-generation clot retriever were soon established in a prospective nonrandomized multicenter study. Reference Smith, Sung and Starkman16 About one-half of the 141 patients in whom the device was deployed were recanalized, and roughly one-half of those patients had a good outcome, a highly significant difference from the patients in whom recanalization was not achieved.
The off-label use of arterial stents as clot retrievers (i.e., stenting the clot and then pulling out the stent along with the clot) were soon recognized to be more effective and safer than the MERCI device, which opened the stroke field to devices designed specifically for neuro-interventional use. Randomized trials comparing mechanical thrombectomy to medical care-alone treatment in eligible patients quickly confirmed the efficacy of this approach Reference Berkhemer O.A.Fransen and Beumer17–Reference Jovin, Chamorro and Cobo21 (the Berkhemer et al. MRCLEAN study especially persuasive Reference Berkhemer O.A.Fransen and Beumer17 ), and in 2015, the American Heart and Stroke Association published guidelines stating that mechanical thrombectomy had Class 1, Level A evidence for efficacy and should be provided to patients at centers with endovascular capability. Reference Powers, Derdeyn and Biller22 A paradigm shift in stroke care had taken place.
At the same time, developments continued in intravenous thrombolysis. Multiple trials studying alteplase for acute ischemic stroke confirmed its efficacy up to 4.5 hours following stroke onset and up to 9 hours from stroke onset, as well as patients who woke with symptoms, in patients selected based on advanced multimodal CT or MRI imaging. Reference Campbell, Meretoja, Donnan and Davis23 More recently a newer and improved thrombolytic agent, tenecteplase (or “TNK”) has joined and is now supplanting alteplase in stroke treatment. Reference Heran, Lindsay and Gubitz24 Because of its longer half-life (22 vs. 4 minutes for alteplase), it can be administered as a single bolus rather than the less practical bolus and hour-long infusion for alteplase. Compared to alteplase, it also has a much higher affinity for fibrin along with a lower binding affinity for plasminogen activator inhibitor, which at least in theory makes it a more effective thrombolytic agent with a reduced risk of bleeding. Reference Campbell, Mitchell and Churilov25 Clinical trials have demonstrated that tenecteplase is non-inferior to alteplase, Reference Shen, Bao and Tang26 but ease of administration has led increasing use in many jurisdictions Reference Heran, Lindsay and Gubitz24 .
The current state of the art for appropriately screened and selected acute ischemic stroke patients is constantly changing, but currently, it involves urgent revascularization, starting with intravenous TNK followed by endovascular thrombectomy, with eligibility based on clinical presentation, duration of symptoms and CT imaging. Reference Heran, Lindsay and Gubitz24 Mechanical thrombectomy has moved from the operating suite, where I performed it, to the interventional angiography suite armed with ever-improving clot aspiration techniques and technology, making it a growing and lucrative industry now.
The human, hospital and neurovascular equipment resources required for “24/7” stroke service have exploded and are difficult to sustain. Reference Hu, Virani, Shankar and Christian27 The limited availability of stroke experts and interventionalists, as well as finite hospital care capabilities, along with the narrow window of opportunity for intervention, has resulted in significant inequities in acute stroke care across our country and indeed around the world. The greatest source of inequity is geographic, particularly in countries such as Canada, where patients in rural and remote areas are disadvantaged by virtue of the time taken to transfer to metropolitan centers with these services.
I began this review by recalling our much-maligned foray into acute MCA embolectomy operations in the 1990s before the dramatic developments in medical and endovascular stroke management summarized above. Ours was a mechanical embolectomy from the outside, which was impractical, but as it turned out, and despite protests from my senior colleagues at the time, on the right track! And it’s interesting that case reports of this obscure operation still occasionally appear in the literature, in some cases because endovascular treatment is unavailable Reference Hino A.Oka and Hashimoto28 or when thrombolysis either failed Reference Katsuno, Kawasaki, Izumi and Hashimoto29 or was impossible due to a proximal carotid occlusion. Reference Yanagawa, Harada, Kiyomoto, Yamashita and Hatayama30
All I can tell young neurosurgeons who might someday, under some unusual circumstance, consider doing an intracranial embolectomy is to first make sure you have the right instruments (such as an extracranial to intracranial or “EC-IC” bypass kit) and sutures (9-0 Prolene) available. But most importantly, you must have a temporary aneurysm clip poised over the artery proximal to the arteriotomy as you tease that embolus out with micro instruments and gentle suction. Slowly at first, but then bursting out like a cork from a champagne bottle with a blast of arterial blood behind it. It is a very gratifying surgical experience once the tiny arteriotomy is repaired, but as in all vascular operations, proximal control is essential.
Funding statement
None.
Competing interests
None.



 Open access
Open access