


The traditional Mediterranean diet (MD) is the heritage of millennia of exchanges of people, cultures and foods of all countries around the Mediterranean basin. It has been the basis of food habits during the twentieth century in all countries of the region, originally based on Mediterranean agricultural and rural models. However, the traditional MD is now progressively eroding due to the widespread dissemination of the Western-type economy, urban and technology-driven culture, as well as the globalisation of food production and consumption, related to the homogenisation of food behaviours in the modern era.
Since the Seven Countries Study in the 1950s, we know which foods were more or less frequently consumed in the Mediterranean area(Reference Keys, Menotti and Karvonen1), a pattern followed mainly by poor rural societies(Reference Trichopoulou2). This led to defining the MD as a dietary pattern rich in plant foods (cereals, fruits, vegetables, legumes, tree nuts, seeds and olives), with olive oil as the principal source of added fat, along with high to moderate intakes of fish and seafood, moderate consumption of eggs, poultry and dairy products (cheese and yoghurt), low consumption of red meat and a moderate intake of alcohol (mainly wine during meals).
The pioneer Seven Countries Study and numerous and increasing recent epidemiological studies have established the health benefits associated with the adherence to the Mediterranean diet pattern (MDP), mainly in relation to reducing the risk of developing the metabolic syndrome, type 2 diabetes, CVD and some neuro-degenerative diseases and cancers(Reference Serra-Majem, Roman and Estruch3–Reference Meydani6).
This healthy, traditional MDP has been popularised since 1995 using the world famous pyramid representation that graphically highlights the food groups to be consumed daily, weekly or less frequently(Reference Willett, Sacks and Trichopoulou7). In addition, in 1995, an index or score was introduced to evaluate the adherence to the MDP, allowing the study of its associated health effects(Reference Trichopoulou, Ocurrís-Blazos and Wahlqvist8). Within the scientific community, there is a consensus on what constitutes the traditional MDP, mentioned above, but issues have been raised about the need to update the present recommendations considering the new lifestyle, dietary, sociocultural, environmental and health challenges the current generations of different countries and sectors of the population are facing, especially low-income groups in which the prevalence of CVD has risen along with the shift from the traditional MD. The following issues, among others, arise and need to be addressed: (i) consumption of fresh, minimally processed, local and seasonal foodstuffs; (ii) the balance between energy-dense and nutrient-dense foods in relation to reduced energy expenditure and the obesity epidemic; (iii) availability, sustainability, accessibility and cost of recommended foods; (iv) adaptation to various geographical, socio-economic and cultural contexts; and (v) understanding the MD as an intangible space for creativity and intercultural dialogue and a common cultural heritage shared by all Mediterranean populations(Reference Reguant-Aleix, Arbore and Bach-Faig9).
The incorporation of food consumption as a basic area in Anthropology and Sociology after the 1930s – after the pioneering works of Audrey Richards and Margaret Mead – has brought light to the study of nutrition understood also as a social and cultural process in permanent flux(Reference Heine10). Food represents much more than a pure act of survival for human evolution; eating is a social and cultural phenomenon, while nutrition is a physiological and health issue(Reference Contreras11).
After the recognition of the MD as an Intangible Cultural Heritage of Humanity by UNESCO in 2010(12, 13), considering the worldwide interest in the MDP and taking as a framework all the mentioned aspects, scientists present a consensual renewed communication tool for the general public, health professionals and stakeholders. This is a new pyramid with which scientists hope to contribute to a much better adherence to this healthy dietary pattern and its way of life in the Mediterranean area and other countries in the near future.
Consensus on a new pictorial representation of the Mediterranean diet pyramid
The Mediterranean Diet Foundation together with the Forum on Mediterranean Food Cultures initiated the dialogue and process of gathering scientific opinion among international experts to develop a consensus position on a new revised MD pyramid representation (Fig. 1). The new revised MD and food lifestyle pyramid (as a schema) arises from the internal dialogues among scientific experts of the Mediterranean Diet Foundation's International Scientific Committee and further discussions from a meeting held in the framework of the III CIISCAM Conference ‘The Mediterranean Diet today, a model of sustainable diet’ in Parma (Italy; Fig. 1).

Fig. 1 The process in the development of the new modern Mediterranean diet pyramid (MDF, Mediterranean Diet Foundation; CIISCAM, International Inter-University Center for Mediterranean Food Culture Studies)
This pyramid results from the aforementioned scientific consensus among experts and is based upon the latest research in the field of nutrition and health, scientific evidence around the healthiness of the MD dietary pattern and its role in the prevention of many chronic diseases by large epidemiological studies published in hundreds of peer-reviewed scientific journal articles during recent decades(Reference Serra-Majem, Roman and Estruch3, Reference Sofi, Cesari and Abbate4).
The final design of the MD pyramid today (Fig. 2) and a brief complementary text for the general public (Fig. 3) have been developed by the gathered opinions of the Mediterranean Diet Foundation Expert Group that includes the Mediterranean Diet Foundation's International Scientific Committee expertise, the in situ discussions by a representative group of members that met within the Barcelona VIII International Congress on the Mediterranean diet (Fig. 1), and several other experts who provided support on the design, editing and translation to ten different languages (English, French, Italian, Spanish, Catalan, Basque, Galician, Greek, Portuguese and Arabic; see acknowledgements).
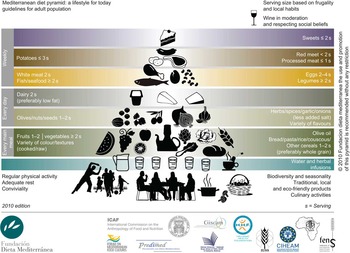
Fig. 2 (colour online) Mediterranean diet pyramid: a lifestyle for today

Fig. 3 (colour online) The Mediterranean diet pyramid's brief complementary text for the general public

Fig. 3 (Continued)

Fig. 3 (Continued)
Thus, the main purpose of this initiative is to foster dialogue among scientists and experts in public health nutrition, food sciences, metabolism, anthropology, sociology, biology, agriculture and environmental and cultural heritage in order to obtain a common representation of the MDP in the Mediterranean area, meant for non-profit use and promotion without restrictions.
The Mediterranean diet pyramid: a lifestyle for today
The pyramid reflects the changing process that the MD is undergoing within the Mediterranean societies. This new graphic representation (Fig. 2) was conceived as a simplified main frame pyramid, to be adapted to the specific realities of different countries (e.g. portion sizes) and variations in the dietary pattern related to the various geographical, socio-economic and cultural contexts of the Mediterranean region. These guidelines (2010 edition) might be periodically updated according to new consensus and suggestions.
By expressing the goals in terms of foods and referring to a dietary pattern based on a cultural model, the new pyramid may contribute to a higher compliance among the general population. In order to preserve the Intangible Cultural Heritage, adapting the cultural specificity of each food practice to its socio-economic and environmental context is necessary. Thus, the pyramid is developed as a tool to help us adopt a healthier and sustainable lifestyle.
The recommendations target the healthy adult population (18–65 years old) and should be adapted to the special needs of children, pregnant women and those suffering from health conditions.
Mediterranean diet pattern
The new MD pyramid provides key elements for the selection of foods, both quantitative and qualitative, indicating the relative proportions and consumption frequency of servings of the main food groups that constitute the MDP. The pattern includes all food groups, and it is just a question of variety of food and culinary techniques, along with adequate frequencies and quantities in the daily diet that make it healthy or unhealthy. A wide variety of foods in the diet minimises the possibility of deficiencies of a particular nutrient. In fact, a higher adherence to the MDP has been associated with a better nutrient profile, with a lower prevalence of individuals showing inadequate intakes of micronutrients in comparison to other patterns such as the Western pattern(Reference Serra-Majem, Bes-Rastrollo and Román-Viñas14).
Plant-origin foods are situated at the base of the pyramid. They provide key nutrients, fibre and protective substances that contribute to general well-being, satiety and the maintenance of a balanced diet, and thus should be consumed in high proportions and frequency. This MD core, based on plant-origin foods, is responsible for the prevention of many chronic diseases and for weight control(Reference Sofi, Cesari and Abbate4, Reference Buckland, Bach-Faig and Serra-Majem15).
The graphic representation follows the previous pattern: at the base, food items that should sustain the diet and provide the highest energy intake, and at the upper levels, foods to be eaten in moderate amounts such as those of animal origin and/or rich in sugars and fats that should be eaten in moderation and some of them left for special occasions. Meals have an essential role in the MD(16), and thus the importance of the meal and its composition is emphasized in the new representation. A balanced composition of the main meals should include fruits, vegetables and cereals, complemented in a lower contribution to daily energy intake with other plant foods, dairy products and protein sources.
The pyramid establishes dietary daily, weekly and occasional guidelines in order to follow a healthy and balanced diet.
Every day
• Main meals should contain three basic elements, which can also be found throughout the day:
– Cereals: one or two servings per meal in the form of bread, pasta, rice, couscous and others. Preferably whole grain, since processing normally removes fibre and some valuable nutrients (Mg, Fe, vitamins, etc.)(Reference Slavin17).
– Vegetables: two or more servings per meal. In order to ensure vitamin and mineral daily intakes, at least one of the servings should be consumed raw (one meal/d)(Reference Tang, Zirpoli and Guru18).
– Fruit: one or two servings per meal, as the most frequently chosen dessert. The concept of ‘variety in colours and textures’ is highlighted, in the case of fruit and vegetables, in order to ensure a wide variety of antioxidants and protective compounds(Reference Khoo, Prasad and Kong19).
• A daily intake of 1·5–2 l of water (equivalent to six to eight glasses) should be guaranteed. Proper hydration is essential to maintaining the corporal water equilibrium, although needs may vary among people due to age, physical activity, personal circumstances and weather conditions. It should be consumed freely, bottled or from the tap, when hygienic circumstances allow it. In addition to water, sugar-free herbal infusions and tea, and low-sodium and low-fat broths may help to complete the requirements.
• Dairy products should be present in moderate amounts (two servings per day), with a preference for low-fat dairy, traditionally in the form of yoghurt, cheese and other fermented dairy products. Although their richness in Ca is important for bone and heart health, dairy products can be a major source of saturated fat(Reference Ascherio20).
• Olive oil is located at the centre of the pyramid; it should be the principal source of dietary lipids because of its high nutritional quality (especially extra virgin olive oil). Its unique composition gives it a high resistance to elevated temperatures, and it is recommended for both cooking(Reference Casal, Malheiro and Sendas21) and dressings. Olive oil has been reported to be inversely associated with some cancers and is known to positively affect blood lipids and cardiovascular systems(Reference Bertuzzi, Tavani and Negri22–Reference Pelucchi, Bosetti and Negri26). This may be related to its high content of monounsaturated oleic acids and abundance of antioxidant compounds, which are primarily present in virgin olive oil(Reference Corona, Spencer and Dessì27). Traditionally, vegetables and other plant foods are cooked with olive oil, thus amplifying their nutritional value.
• Olives, nuts and seeds are good sources of healthy lipids, proteins, vitamins, minerals and fibre(Reference Sabaté, Ros and Salas-Salvadó28). A reasonable consumption of olives, nuts and seeds (such as a handful) make for a healthy snack choice.
• Spices, herbs, garlic and onions are a good way to introduce a variety of flavours and palatability to dishes and allow for a reduction in salt use, as salt is one of the main contributing factors to the development of hypertension among predisposed individuals(29). Herbs and spices are good sources of micronutrients and antioxidant compounds and also contribute to the regional identities of Mediterranean dishes.
• Respecting religious and social beliefs, a moderate consumption of wine and other fermented beverages during meals (one glass per day for women and two glasses per day for men, as a generic reference) is present in the MDP(Reference Mink, Scrafford and Barraj30–Reference Vilavalur, Otani and Singal32).
Weekly
Consumption of a variety of plant- and animal-origin proteins is recommended. Traditional Mediterranean dishes do not usually have animal-origin protein foods as the main ingredient but rather as a source of flavour.
• Fish and shellfish (two or more servings), white meat (two servings) and eggs (two to four servings) are good sources of animal protein. Fish, white meat (poultry, turkey, rabbit, etc.) and eggs provide high-quality protein. Fish and shellfish are a good source of healthy protein and lipids. Varied consumption (of oily fish, lean fish and shellfish) is recommended. Fish (especially those high in lipids) and shellfish consumption has been reported to reduce the risk of CHD and they have anti-inflammatory properties due to their content of long chain n-3 PUFA(Reference Kris-Etherton, Harris and Appel33, Reference Simopoulos34). White meat is also a good source of lean protein without the high levels of saturated fat found in some red meat cuts. Egg consumption, including those used in cooking as well as baking, should be between two and four times per week.
• Consumption of red meat (less than two servings, preferably lean cuts) and processed meats (less than one serving) should be small in both quantity and frequency as the intake of such meats has been consistently associated with some chronic diseases (cancers and CHD)(Reference Micha, Wallace and Mozaffarian35, 36).
• The combination of legumes (more than two servings) and cereals is a healthy plant protein and lipid source that should be considered as a meat alternative(Reference Rochfort and Panozzo37, Reference Bazzano, He and Ogden38).
• Potatoes are also included on the weekly level (three or fewer servings per week, preferably fresh), as they are a part of many traditional recipes with meat and fish. They should be consumed in moderation(Reference Mozaffarian, Hao and Rimm39) as they have a high glycaemic index(Reference Willett, Manson and Liu40) and are most commonly prepared fried.
Occasionally
In the top vertex of the pyramid are the foods rich in sugars and unhealthy fats (sweets). Sugar, candies, pastries and beverages such as sweetened fruit juices and soft drinks should be consumed in small amounts and set aside for special occasions. These foods are energy dense and are likely to contribute to weight gain(Reference Mozaffarian, Hao and Rimm39). Simple sugars, which are abundant in sweets, pastries, fruit juices and soft drinks, have been associated with an increased occurrence of tooth decay(36).
Cultural and lifestyle elements
Along with recommendations regarding the proportion and frequency of food consumption, the incorporation of cultural and lifestyle elements is one of the innovations of the pyramid. Adopting a healthy lifestyle and preserving cultural elements should also be considered in order to acquire all the benefits from the MD and to preserve this cultural heritage. These concepts represented outside of the pyramid, but at its base, are as follows.
Moderation
Serving sizes should be based on frugality and moderation, to adapt the urban and modern lifestyles to energy needs. This aspect is emphasised due to the major public health challenge of obesity. The portion sizes of the foods represented at the bottom should be larger and consumed frequently as they provide satiety along with moderate amounts of energy, and those foods at the upper levels should be consumed in smaller amounts and less frequently due to their high fat and simple sugar contents. Serving sizes should reflect autochthonous peculiarities and local habits, thus adapting to the specific realities of each country and region.
Socialisation
The conviviality aspect is important for the social and cultural value of the meal beyond nutritional aspects. In this sense, several factors related to food (understood as a social fact) must be kept in mind, such as culinary activities, knowledge transmitted from generation to generation and time devoted to meals related to the daily pace of life. All these aspects contribute to generating or strengthening sociability, communication and the identity of communities. Sharing food in the company of family and friends around the table represents social support and a sense of community(Reference Medina41). The pleasure associated with the conviviality of meals may positively affect food behaviours, and in return, health status(Reference De Garine42).
Culinary activities
The development of culinary activities such as cooking, making crafts, the organisation of domestic space and other techniques associated with food is basic for the social reproduction of the identity of each particular culture(Reference Heine10). Thus, devoting enough time and space for such culinary activities is stressed, giving account to their role in everyday meals, celebrations and religious festivals in every culture.
Physical activity
Regular practice of moderate physical activity (at least 30 min throughout the day) serves as a basic complement to the diet by balancing energy intake, maintaining healthy body weight and providing many other health benefits(36). Physical activity not only involves sports such as football, dancing, jogging, cycling, etc. but also walking, taking the stairs v. the lift, housework, gardening, etc. Practising leisure activities outdoors(Reference Thompson, Boddy and Stein43), and preferably with others, makes them more enjoyable and strengthens the sense of community.
Adequate rest
Resting during the day (nap) as well as adequate night sleep is also part of a healthy and balanced lifestyle. Scientific evidence has shown that a short rest after eating is a healthy and traditional Mediterranean habit that helps promote a balanced lifestyle(Reference Ficca, Axelsson and Mollicone44). An after-meal nap is an increasingly widespread habit in Mediterranean countries and throughout Europe.
Seasonality
The preference for seasonal, fresh and minimally processed foods may in most cases maximise the content of protective nutrients and substances in the diet. Currently and due to the modern lifestyle, the consumption of fresh foods is being substituted by other processed foods. However, progress in modern technology minimises nutrient loss and offers healthy alternatives(Reference Sizer and Whitney45). Especially in the case of fresh products, several factors influence their nutritional value: the growing methods used, the specific variety chosen, ripeness when harvested, post-harvest handling, storage, extent and type of processing, and the distance transported(46). Thus, all the decisions and practices along the food system – from seed to table – affect the nutrient content of foods.
Traditional, local, eco-friendly and biodiverse products
Taking into account the traditional, local, eco-friendly and biodiverse products whenever possible contributes to the preservation of Mediterranean landscapes and sea. The MD should be understood not only as a set of foods but also a cultural model incorporating the whole food chain: the way foods are selected, produced, processed and distributed to the consumers(13, Reference Serra-Majem47). Moreover, the MD, as a plant-centred dietary pattern, further contributes to the preservation of the environment, as it implies a reduction in animal consumption and therefore production compared to Western patterns and, consequently, lowered demands on soil, water and energy resources(Reference Gussow48, Reference Stehfest, Bouwman and Van Vuuren49). All these items express the sustainable character of the MD in an increasingly globalised world(Reference Serra-Majem47, 50, Reference Gussow and Clancy51).
The MD is an example of a sustainable pattern in which agricultural biodiversity plays an important role(Reference Serra-Majem47, Reference Gussow and Clancy51). The variety both among and within species contributes to differences in appearance and taste, as well as micronutrient and phytochemical content(46). However, when making varietal decisions, durability (for instance, to withstand long-distance transport) is sometimes being prioritised over taste and nutritional quality(Reference Goldman, Kader and Heintz52). The large number of endemic species and landscape diversification (cultivated areas, grassland or forest and land use changes over time) that contribute to the biodiversity of the territories bordering the Mediterranean make this area a hot spot of global diversity(Reference Myers, Mittermeier and Mittermeier53). In this sense, agricultural biodiversity provides food variety of plant and animal food products from wild and domesticated sources(Reference Trichopoulou, Vasilopoulou and Hollman54) that foster the nutritional guidelines(Reference Johns and Sthapit55).
The consumption of local and eco-friendly foods has been associated with health and environmental preservation in several ways(50). First, although there is still no unanimous international consensus on the differences in nutrient content between eco-friendly and conventional products(Reference Dangour, Dodhia and Hayter56), some literature surveys of nutritional and sanitary aspects of eco-friendly (organic) foods(57, Reference Lairon58) have reported some higher nutrient contents and marginal pesticide residue contaminations. Second, locally grown and harvested foods are normally given more time to ripen. Third, local food products normally have less distance to travel, thus promoting energy saving and reducing pollution, having a lower contribution to climate change and greenhouse gas emissions if compared to long-travelling food products(Reference Carlsson-Kanyama and González59). Moreover, by buying local foods, farmers are encouraged to diversify their crops and decrease their vulnerability to pests(50). Finally, the consumption of local foods contributes to improving local economies(Reference Horrigan, Lawrence and Walker60).
Traditional knowledge and practices developed through daily observation, interaction within rural communities, transfer production, procurement and consumption techniques and activities are locally transmitted from generation to generation(Reference Contreras11). All those elements ensure positive, responsible, sustainable and healthy behaviours(Reference Gussow48, 50, Reference Johns and Sthapit55) while reproducing the Intangible Cultural Heritage of the Mediterranean Diet(13). The modernisation process, including sociocultural changes and new technologies, has transformed food production and threatens sustainable orders of life, such as local foodstuffs and environmental biodiversity. Thus, countries, communities and cultures that maintain their own traditional food systems are better able to conserve local food specialities with a corresponding diversity of crop varieties and animal breeds(50, Reference Burlingame and Dernini61).
Conclusions
This pyramid is the result of an international consensus and is based on the latest scientific evidence on nutrition and health published in hundreds of scientific articles in recent decades. It contributes to the harmonisation of educational tools used in the promotion of the MD and responds to the need for a common framework in the Mediterranean area, to be adapted to each country's and region's specific realities. The use and promotion of this pyramid is recommended without any restrictions, and the material is available in English, Spanish, Catalan, Galician, Basque, French, Arabic, Italian, Portuguese and Greek.
The ‘Mediterranean diet pyramid: a lifestyle for today' summarises and updates the traditional MD of those areas of the Mediterranean basin that have evolved with modernisation. It is a shared and dynamic cultural heritage that was recognised by UNESCO in 2010. Taking into account its contribution to health and general well-being, we hope to contribute to a much better adherence to this healthy dietary pattern and its way of life with this new graphic representation.
Acknowledgements
The present study was supported by the Mediterranean Diet Foundation, the Spanish Government (Ministerio de Medio Ambiente y Medio Rural y Marino), Interuniversity International Center for Mediterranean Food Cultures Studies (CIISCAM), Fundación Patrimonio Comunal Olivarero, Università Degli Studi di Parma, Istituto Nazionale di Riverca per gli Alimenti e la Nutrizione (INRAN). The authors have no conflict of interest to declare. The authors contributed as follows: A.B.F., E.M.B., D.L., J.R., A.T., S.D., X.F.M., M.B., R.B. and L.S.M.: conceived and designed the study and revised the manuscript; A.B.F.: conducted the literature review and wrote the manuscript; G.M.: further developed some concepts, identified additional references and edited the subsequent drafts of the manuscript; L.S.M.: coordinated the study. All authors have seen and approved the content and contributed to the work. The Mediterranean Diet Foundation Expert Group contributed intellectually and scientifically to the project. The authors thank the members of the Mediterranean Diet Foundation Expert Group (Lluís Serra-Majem (Chair, Las Palmas de Gran Canaria and Barcelona, Spain), Joan Reguant (Andorra la Vella, Andorra), Anna Bach-Faig (Barcelona, Spain), Antonia Trichopoulou (Athens, Greece), Denis Lairon (Marseille, France), Elliot Berry (Jerusalem, Israel), Sandro Dernini (Rome, Italy), Francesc Xavier Medina (Barcelona, Spain), Maurizio Battino (Ancona, Italy), Javier Aranceta (Bilbao, Spain), Tola Atinmo (Ibadan, Nigeria), Juan Miguel Barros (Santiago de Compostela, Spain), Rekia Belahsen (El Jadida, Morocco), Sabah Benjelloun (Rabat, Morocco), Isabel Bertomeu-Galindo (Barcelona, Spain), Barbara Burlingame (Rome, Italy), Marc Caballero-Bartolí (Barcelona, Spain), Carmen Clapés-Badrinas (Barcelona, Spain), Sandrine Couto (Porto, Portugal), Ibrahim Elmadfa (Vienna, Austria), Ramón Estruch (Barcelona, Spain), Amanda Faig (Toronto, Canada), Flaminio Fidanza (Perugia, Italy), Silvia Franceschi (Lyon, France), Joseph Hautvast (Wageningen, Holland), Elisabeth Helsing (Oslo, Norway), Diana Julià-Llobet (Barcelona, Spain), Carlo La Vecchia (Milano, Italy), Aicha Lemtouni (Rabat, Morocco), Abel Mariné (Barcelona, Spain), Miguel A. Martínez-González (Pamplona, Spain), Gemma Miranda (Barcelona, Spain), Ridha Mokni (Tunis, Tunisia), Francisco Mombiela (País, France), Idoia Noain (Ordizia, Spain), Biel Obrador (Barcelona, Spain), Gülden Pekcan (Ankara, Turkey), Suzanne Piscopo (Msida, Malta), Blanca Raidó-Quintana (Barcelona, Spain), Emilio Ros (Barcelona, Spain), Sara Sáez-Almendros (Barcelona, Spain), Jordi Salas-Salvadó (Reus, Spain), Francisco Sensat (Barcelona, Spain), Dimitrios Trichopoulos (Boston, United States), Josep Antoni Tur (Palma de Mallorca, Spain), Maria Daniel Vaz da Almeida (Porto, Portugal) and Walter C. Willett (Boston, MA, USA)) and the 2009 CIISCAM Conference experts (Marie Joseph Amiot-Carlin (Marseille, France), Anna Bach-Faig (Barcelona, Spain), Rekia Belahsen (El Jadida, Morocco), Alfonsina Bellio (Cosenza, Italy), Elliot Berry (Jerusalem, Israel), Barbara Burlingame (Rome, Italy), Carlo Cannella (Rome, Italy), Roberto Capone (Bari, Italy), Davide Cassi (Parma, Italy), Sandro Dernini (Rome, Italy), Lorenzo M. Donini (Rome, Italy), Cosimo Lacirignola (Bari, Italy), Denis Lairon (Marseille, France), Giuseppe Maiani (Rome, Italy), Mario Mancini (Naples, Italy), Francesc Xavier Medina (Barcelona, Spain), Nicolo Merendino (Viterbo, Italy), Martine Padilla (Montpellier, France), Stefano Padulosi (Rome, Italy), Lluís Serra-Majem (Las Palmas de Gran Canaria, Spain), Antonia Trichopoulou (Athens, Greece)) for their contributions.





