



Background
Type 2 diabetes mellitus (DM) is a chronic disease that causes life-threatening complications and substantially contributes to disability and mortality worldwide (Zheng, Ley, & Hu, Reference Zheng, Ley and Hu2018). The prevalence of type 2 DM has been increasing, affecting 5.9% of the global population in 2021, and is projected to increase to 9.5% (1.27 billion people) by 2050 (Ong et al., Reference Ong, Stafford, McLaughlin, Boyko, Vollset, Smith and Vos2023). Among the key comorbidities of type 2 DM, depression primarily contributes to its mortality and disease burden of type 2 DM. It is a serious, chronic, and relapsing psychiatric disorder that is projected to be among the five leading causes of the disease burden by 2030, similar to diabetes (Mathers & Loncar, Reference Mathers and Loncar2006). Depression is highly prevalent, affecting 16.5% of patients with type 2 DM, which is more than twice the rate of patients without DM (Anderson, Freedland, Clouse, & Lustman, Reference Anderson, Freedland, Clouse and Lustman2001). Patients who were unaware of their diabetic condition had a significantly higher odds ratio (1.8, p < 0.001) for depression than those without DM (Meurs et al., Reference Meurs, Roest, Wolffenbuttel, Stolk, de Jonge and Rosmalen2016). Depression among patients with type 2 DM may have negative health outcomes such as poor glycemic control (Lustman et al., Reference Lustman, Anderson, Freedland, de Groot, Carney and Clouse2000), poor adherence to medical treatment (Gonzalez et al., Reference Gonzalez, Safren, Cagliero, Wexler, Delahanty, Wittenberg and Grant2007), weight gain, type 2 diabetes-related complications (Black, Markides, & Ray, Reference Black, Markides and Ray2003), and low quality of life (Bayani, Shakiba, Bijani, & Moudi, Reference Bayani, Shakiba, Bijani and Moudi2022). Thus, the increasing prevalence of this comorbidity has substantially increased the morbidity and mortality among patients with type 2 DM worldwide. To optimize type 2 DM management, assessment and intervention for individuals at a high risk of comorbid depression is essential.
Among the first-line strategies for type 2 DM treatment, weight management has important clinical implications in both diabetes and comorbid depression. Current guidelines strongly recommend weight reduction among obese and overweight patients to improve glycemic control and reduce the need for hypoglycemic medications (Committee, Reference Committee2021). Weight is also closely related to the risk of depression; underweight and obesity are risk factors for depression (Jung et al., Reference Jung, Woo, Cho, Park, Jeong, Lee and Shin2017), and a bidirectional relationship exists between body weight and depression (Pan et al., Reference Pan, Sun, Czernichow, Kivimaki, Okereke, Lucas and Hu2012). Understanding the relationship between weight change and depression risk in individuals with type 2 DM is crucial for glycemic control and depression management.
Previous studies have mainly focused on the association between baseline body weight and depression risk; however, few studies have examined the association between weight change and depression risk (Choi et al., Reference Choi, Kim, Han, Oh, Suh, Kim and Kim2023; Zhang et al., Reference Zhang, Li, Guo, Xu, Yang, Wang and Liu2022). A Korean study reported that weight variability was related to depression risk among patients with type 2 DM, suggesting that the inflammatory response resulting from weight changes and fat accumulation could contribute to the development of depression (An et al., Reference An, Han, Jung, Yoo, Fava, Mischoulon and Jeon2021). A recent Korean study reported a U-shaped association between weight change and risk of depression among patients with diabetic kidney disease, with a more substantial association with advanced chronic kidney disease (Choi et al., Reference Choi, Kim, Han, Oh, Suh, Kim and Kim2023). A Chinese longitudinal study on 3118 middle-aged individuals demonstrated that weight loss (> −3%) over 2–4 years was associated with a 1.3 times higher depression risk of depression than stable weight (−3 to 3%) (Zhang et al., Reference Zhang, Li, Guo, Xu, Yang, Wang and Liu2022). However, these previous studies had limitations, such as a specific study population prone to fluid retention and edema leading to fluctuating body weight (Choi et al., Reference Choi, Kim, Han, Oh, Suh, Kim and Kim2023), small sample size (Zhang et al., Reference Zhang, Li, Guo, Xu, Yang, Wang and Liu2022), and unclear direction of body weight change (gain or loss) describing body weight variability (An et al., Reference An, Han, Jung, Yoo, Fava, Mischoulon and Jeon2021).
Thus, we aimed to investigate the association between body weight change and depression incidence among patients with type 2 diabetes, in whom both body weight change and depression are important prognostic factors for controlling glycemia- and diabetes-related complications.
Methods
Data source and study population
We used the Korean National Health Insurance Service (NHIS) nationwide database. The Korean NHIS provides universal health insurance coverage for 97% of the Korean population, excluding 3% of Koreans in the lowest-income bracket who receive medical aid. The Korean NHIS recommends free biennial health check-ups for eligible Korean adults to assess their general health status, including a self-questionnaire on lifestyle behaviors (smoking and alcohol consumption), anthropometric measurements, and laboratory test results. Demographic and claims information for medical utilization, such as diagnosis statements coded by the International Classification of Disease 10th revision (ICD-10) and prescription statements collected by the NHIS, were provided (Cheol Seong et al., Reference Cheol Seong, Kim, Khang, Heon Park, Kang, Lee and Ae Shin2017). This database has been widely used in studies on various health outcomes.
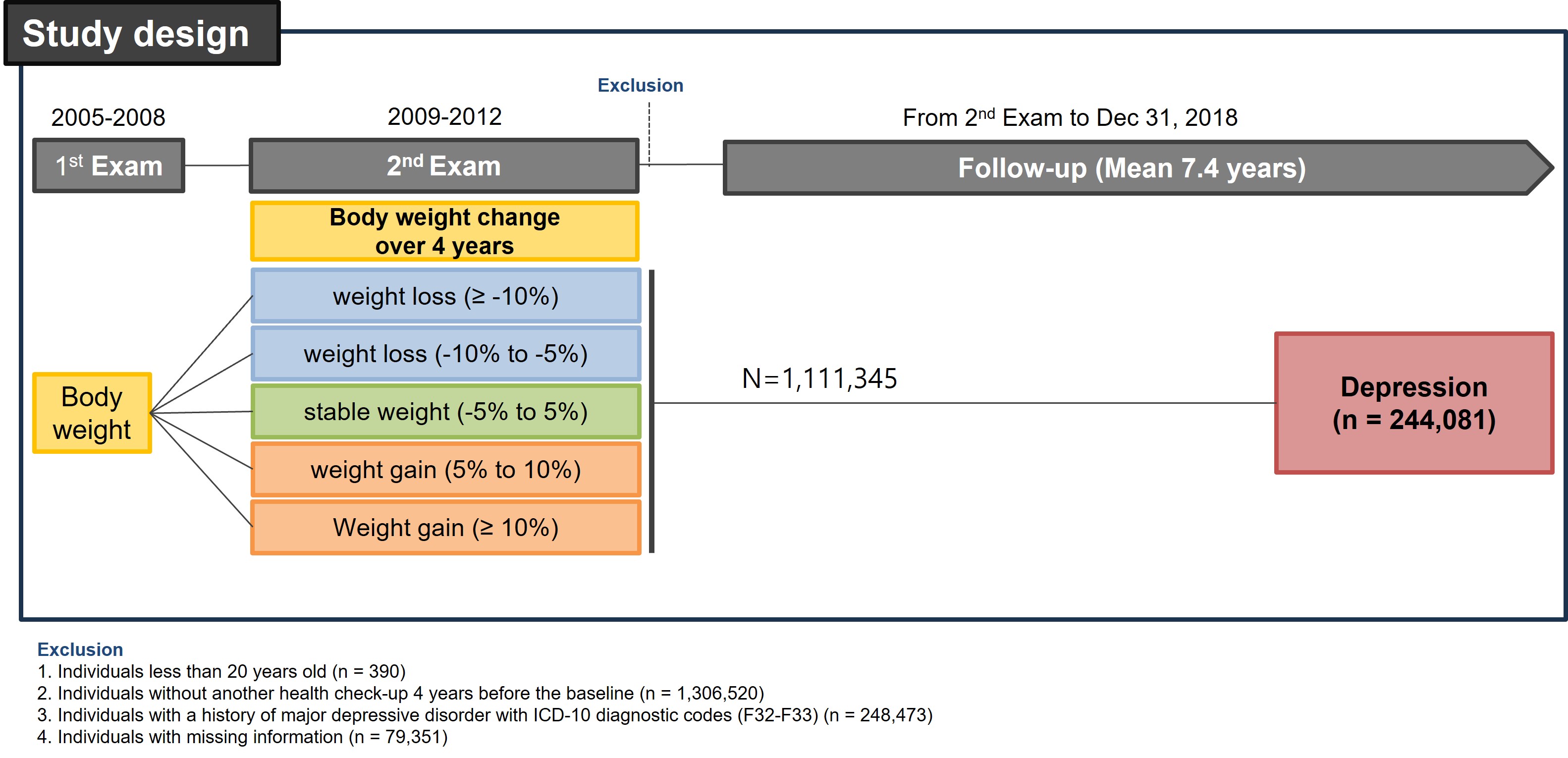
We initially identified 2 746 079 patients with type 2 diabetes who underwent national health check-ups between January 2009 and December 2012. Type 2 diabetes was defined as a claim of prescribed antidiabetic medication under the diagnostic codes of type 2 diabetes (ICD-10: E11-E14) at one or more outpatient care visits or fasting plasma glucose ⩾126 mg/dL during health check-ups, called newly diagnosed type 2 diabetes. The date of the health examination between 2009 and 2012 was considered the baseline. We excluded patients aged <20 years (n = 390), those without another health check-up 4 years before baseline (n = 1 306 520), those with a history of major depressive disorder with ICD-10 diagnostic codes (F32-F33) (n = 248 473), and those with missing information (n = 79 351), leaving a final study population of 1 111 345 individuals (×Fig. 1).

Figure 1. Flow chart of the study population.
This study was approved by the Institutional Review Board of Soongsil University (IRB File No. SSU-202003-HR-201-01). The review board waived the requirement for written informed consent because publicly available and anonymous data were retrospectively analyzed.
Definition of body weight change
Body weight change was assessed using body weight measured at the first (4 years before baseline) and second (baseline) health check-ups (online Supplementary Figure 1). As national health check-ups are provided biennially in Korea, applying a 4-year interval enabled us to obtain a sufficient study population to further categorize the group by weight change and to see the effect of relatively long-term weight change. In addition, several previous studies that defined weight change over 4 years have confirmed association with various clinical outcomes.(Kim et al., Reference Kim, Han, Jung, Yoo, Lee, Lee and Kim2022; Son et al., Reference Son, Kwon, Park, Joh, Hwang, Cho and Park2020) The participants were categorized into five groups according to the direction of weight change (weight gain v. weight loss) and percent change in body weight as follows: weight loss of 10% or more (⩾ −10%), weight loss of −10% to ⩾ −5%, stable weight without significant change (⩾ −5% to 5%), weight gain of 5% to 10%, and weight gain of 10% or more (⩾ 10%). This categorization was determined by analyzing the restricted cubic spline curve, depicting the relationship between body weight change as a continuous variable and incidence of depression, which exhibited a U-shaped pattern (online Supplementary Figure 2).
Study outcomes and follow-up
The primary endpoint of this study was the incidence of major depressive disorder, which we defined as a patient being diagnosed with relevant ICD-10 codes (F32: single episode and F33: recurrent) (Jin et al., Reference Jin, Han, Lee, Shin, Lim, Yoon and Kim2021). The cohort was followed from the date of the second health check-up until the date of incident major depressive disorder diagnosis, death, or until the end of the study period (December 31, 2018), whichever occurred first.
Definition of covariates
Data on smoking status, alcohol consumption, and physical activity were collected using a self-administered questionnaire during the second health check-up (2009–2012). Smoking status was classified as never, former, or current smokers, and alcohol consumption was classified as none (0 g/day), mild to moderate (<30 g/day), or heavy (⩾30 g/day) based on average daily alcohol consumption (Jeong et al., Reference Jeong, Lee, Han, Jeon, Kim, Yoo and Shin2022). Regular physical activity was defined as moderate-intensity physical activity for >30 min at least five times per week or vigorous-intensity physical activity for >20 min at least three times per week.
Type 2 diabetes status was assessed based on the duration of type 2 diabetes (⩾5 years), the number of antidiabetic medications (⩾3), and insulin use. Hypertension was defined when participants had a claim with ICD-10 codes (I10-I13 or I15) and antihypertensive medication or systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg at health check-ups. Dyslipidemia was defined as a claim with code E78 and lipid-lowering medications or a total cholesterol level ⩾240 mg/dL at the health check-up (Kim et al., Reference Kim, Han, Park, Kwon, Kang, Yoon and Lee2018). Income level was categorized based on the monthly insurance premium as it reflects an individual's income and property.
Statistical analyses
Baseline characteristics according to groups categorized by body weight change are presented as mean ± standard deviation for continuous variables and numbers with percentages for categorical variables. Differences in body weight across the groups were compared using analysis of variance and χ2 tests. Standardized differences were calculated to see the effect size of differences in all variables between included and excluded population (Austin, Reference Austin2009). Hazard ratios (HRs) and 95% confidence intervals (CI) for the association between body weight change and depression were analyzed using Cox proportional hazards models. Participants with −5 to 5% body weight changes were regarded as the reference group. Multivariate-adjusted proportional hazards models were used. Model 1 included age and sex as the covariates. Model 2 additionally included income, smoking status, alcohol consumption, regular physical activity, and comorbidities (hypertension, dyslipidemia, and chronic kidney disease). Model 3 included type 2 diabetes status, such as the duration of type 2 diabetes, insulin use, and number of antidiabetic medications. In the sensitivity analysis, (1) we treated body weight change as a continuous variable in both kg and %, (2) we analyzed categorical shifts based on BMI, and (3) we analyzed changes with time-lag (1-,3-and 5-year). In addition, we performed a stratified analysis by age group (<65 years v. ⩾65 years), sex, baseline BMI category, income, incidence of diabetes macrovascular and microvascular complications, diabetes duration, and presence of other psychiatric disorders to observe the different associations of these factors. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and a p-value <0.05 was considered statistically significant.
Results
Baseline characteristics of the study population
The characteristics of the study participants according to the changes in body weight are shown in ×Table 1. The number of participants allocated to each weight change group was 55 851 (5.0%), 173 129 (15.6%), 728 157 (65.5%), 112 156 (10.1%), and 42 052 (3.8%), respectively (weight loss: ⩾ −10%, −10% to −5%, reference: −5% to 5%, weight gain: 5% to 10%, and ⩾10%). years in the group with weight loss were more likely, older (60.7 years in the group with weight loss ⩾ −10% v. 53.3 years in the group with weight gain ⩾ 10%), and women (45.3% in the group with weight loss ⩾ −10% v. 34.9% in the group with weight gain ⩾10%) than in those with weight gain. smokers and non-alcohol drinkers were more prevalent among participants with weight loss than among those with weight gain. Participants with weight loss, especially with ⩾ −10%, were more likely to have ⩾5 years (37.9%) duration of type 2 diabetes, use insulin (13.4%), and be treated with three or more antidiabetic medications (18.7%) than other groups. BMI and waist circumference increased as the degree of body weight change advanced toward weight gain. The individuals who were included were more likely to be men (66.2% v. 56.3%) and those with a high income (38.2% v. 31.4%). Despite statistically significant differences in variables between the included and excluded population, standardized differences were small except for the sex variable (0.204) (online Supplementary Table 1).
Table 1. Baseline characteristics

Q1, quartile 1; CKD, Chronic kidney disease; T2DM, type 2 diabetes mellitus; BMI, body mass index; BP, blood pressure; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol.
a Geometric mean with 95% confidence interval.
Values are presented as the mean ± standard deviation for continuous variables and as numbers (%) for categorical variables.
Associations between body weight change and depression incidence
During a median follow-up of 7.4 years (interquartile range 6.1–8.6), 244 081 cases of incident depression were identified (Table 2 and Fig. 2). Both weight loss (HR 1.17, 95% CI 1.15–1.19 for ⩾ −10%; HR 1.07, 95% CI 1.06–1.08 for −10% to −5%) and weight gain (HR 1.06, 95% CI 1.04–1.08 for ⩾ 10%; HR 1.02, 95% CI 1.01–1.04 for 5% to 10%) were associated with higher depression risk than the stable weight group (−5% to 5%).
Table 2. Hazard ratios (95% confidence interval) for depression incidence according to weight change

IR, incidence rate; PY, person-years; HR, hazard ratio; CI, confidence interval.
Model 1 was adjusted for age and sex.
Model 2 was adjusted for income, smoking status, alcohol consumption, regular physical activity, and comorbidities (hypertension, dyslipidemia, and chronic kidney disease) in addition to the covariates in Model 1.
Model 3 was adjusted for the duration of type 2 diabetes mellitus, insulin use, number of antidiabetic medications (⩾3), and covariates in model 2.

Figure 2. Associations between body weight change and risk of depression among patients with type 2 diabetes mellitus.
In sensitivity analyses treating body weight change as a continuous variable, weight gain body weight change was associated with a lower risk of depression (HR 0.97, 95% CI 0.97–0.98 per 1SD of change in kg; and HR 0.98, 95% CI 0.97–0.98 per 1SD of change in %) (online Supplementary Table 2). Absolute change in body weight change, which reflects weight loss and weight gain, was associated with a higher risk of depression (HR 1.04, 95% CI 1.03–1.04 per 1SD of absolute change in weight (kg) and HR 1.04, 95% CI 1.03–1.04 per 1SD of absolute change in weight (%)). Categorical shifts toward weight loss from BMI 18.5–25 to BMI <18.5 and from BMI ⩾ 25 to BMI < 18.5 were associated with a higher risk of depression (HR 1.21, 95% CI 1.16–1.26 and HR 1.37, 95% CI 1.09–1.74) compared to those remaining in the same BMI category (online Supplementary Table 3). Categorical shifts toward weight gain were not significantly associated with depression risk. The lag time results were consistent with the main findings (online Supplementary Table 4).
Stratification analyses by covariates
Age- and sex-stratified analyses yielded results that were consistent with those of the total study population, revealing a U-shaped association (online Supplementary Table 5). A significant interaction between age, sex, and weight change in the incidence of depression was observed (all p < 0.001). A higher risk of depression related to weight loss was more prominent among participants aged <65 years than those aged ⩾65 years (HR 1.23, 95% CI 1.20–1.26 v. HR 1.12, 95% CI 1.10–1.15 for ⩾ −10% of weight loss). A higher risk of depression related to weight change (weight gain and weight loss) was more prominent among men than women (HR 1.29, 95% CI 1.26–1.32 v. HR 1.08, 95% CI 1.06–1.10 for ⩾ −10% of weight loss; HR 1.09, 95% CI 1.05–1.12 v. HR 1.03, 95% CI 0.99–1.06 for ⩾10% of weight gain).
A U-shaped association between body weight change and depression incidence was consistently observed across groups according to the duration of type 2 diabetes. A significant interaction was observed between body weight change and type 2 diabetes duration with respect to the incidence of depression (p < 0.001). Patients with newly diagnosed type 2 diabetes had a more prominent association between body weight loss (HR 1.21, 95% CI 1.16–1.26) and body weight gain (HR 1.10, 95% CI 1.05–1.14) and depression incidence than those with a type 2 diabetes duration of 1–4 years. Those who did not have other comorbid psychiatric diagnoses had a more prominent association between weight loss and the incidence of depressive disorder (HR 1.16, 95% CI 1.14–1.19) than those who had other comorbid psychiatric diagnoses (HR 1.07, 95% CI 1.04–1.09). No significant interaction was observed between body weight and depression risk based on income, baseline BMI, or incidence of macro/microvascular complications, revealing a consistent U-shaped association (online Supplementary Tables 5 and 6).
Discussion
In this large nationwide study, we investigated the relationship between body weight change and depression risk in patients with type 2 diabetes. We discovered U-shaped associations between body weight change and depression risk, with a 17% and 5% higher risk of depression among patients with weight loss and weight gain, respectively, than among those with stable weight. In the stratification analyses, the U-shaped association with body weight change was stronger in men, those younger than 65 years, and those with newly diagnosed type 2 diabetes than in their counterparts.
Several studies have reported that being underweight or obese was associated with depression (de Wit, van Straten, van Herten, Penninx, & Cuijpers, Reference de Wit, van Straten, van Herten, Penninx and Cuijpers2009; Jung et al., Reference Jung, Woo, Cho, Park, Jeong, Lee and Shin2017), and the association between changes in body weight and depression incidence has rarely been investigated. According to a study on postmenopausal women, weight gain around menarche was associated with recurrent depression (odds ratio = 1.26, 95% CI 1.03–1.56) via insulin resistance (Perquier, Lasfargues, Mesrine, Clavel-Chapelon, & Fagherazzi, Reference Perquier, Lasfargues, Mesrine, Clavel-Chapelon and Fagherazzi2014). The Australian Longitudinal Study on Women's Health demonstrated that weight gain was not associated with the incidence of depression based on findings from the time-lagged analysis, suggesting possible reverse causality (Singh, Jackson, Dobson, & Mishra, Reference Singh, Jackson, Dobson and Mishra2014). However, our findings with a time lag support the hypothesis that weight change preceding depression occurrence could be a risk factor for depression in patients with type 2 diabetes. This discrepancy might be caused by the different characteristics of the study populations (healthy community people v. patients with type 2 diabetes in our study). Metabolically unhealthy individuals with obesity, rather than metabolically healthy individuals with obesity, are more likely to have an elevated risk of developing depressive symptoms, probably because of peripheral inflammatory responses to inflammatory cytokines in the brain (Hamer, Batty, & Kivimaki, Reference Hamer, Batty and Kivimaki2012).
The pathophysiological mechanisms underlying the association between body weight change and depression are uncertain. Immunometabolic dysregulation, including chronic low-grade inflammation, oxidative stress, and disruption of neuroendocrine regulation (such as insulin resistance) or energy metabolism, has been proposed as a core mechanism in depression and cardiometabolic diseases (Penninx, Milaneschi, Lamers, & Vogelzangs, Reference Penninx, Milaneschi, Lamers and Vogelzangs2013).
First, chronic inflammation might play a key role in the association between weight change and depression. The cytokine-induced depression observed in patients with cancer or hepatitis C treated with interferon (IFN)-alpha supports the role of inflammatory processes in depression pathophysiology. IFN is frequently associated with the development of major depression in approximately 50% of patients unless prophylactically treated with antidepressants (Raison et al., Reference Raison, Woolwine, Demetrashvili, Borisov, Weinreib, Staab and Miller2007). In the immunometabolic depression conceptual model, a chronic low-grade inflammation cloud activates a repertoire of several behavioral symptoms (appetite and sleep alterations, fatigue, and weakness) called sickness behavior, and develops into depressive syndrome at a later stage (Milaneschi, Lamers, Berk, & Penninx, Reference Milaneschi, Lamers, Berk and Penninx2020). In addition, subclinical inflammation can precede weight loss and gain in older adults (Barzilay, Forsberg, Heckbert, Cushman, & Newman, Reference Barzilay, Forsberg, Heckbert, Cushman and Newman2006). Elevated concentrations of fibrinogen and C-reactive protein have also been reported before weight gain in diverse, healthy adults, and predate diminished appetite and weight loss, especially in chronic conditions (Barinas-Mitchell, Cushman, Meilahn, Tracy, & Kuller, Reference Barinas-Mitchell, Cushman, Meilahn, Tracy and Kuller2001).
Second, hypothalamic-pituitary-adrenal (HPA) axis activation may be linked to weight change and depression. Urine cortisol levels were elevated in both men and women with obesity in a clinical study, revealing a U-shaped pattern between BMI and cortisol levels, with the lowest cortisol levels in overweight to class I obese groups (Schorr, Lawson, Dichtel, Klibanski, & Miller, Reference Schorr, Lawson, Dichtel, Klibanski and Miller2015). Hypercortisolemia with caloric excess and restriction may contribute to increased adiposity and decreased bone and muscle mass, leading to weight gain and loss. Hyperactivity of the HPA axis and elevated cortisol levels in response to psychosocial stress are hallmarks of depression (Malhi & Mann, Reference Malhi and Mann2018). Furthermore, patients with type 2 diabetes are predisposed to high corticosteroid sensitivity and blunt responsivity to stress (for example, unchanged corticosteroid sensitivity following exposure to stress) in contrast to decreased corticosteroid sensitivity in healthy controls (Carvalho et al., Reference Carvalho, Urbanova, Hamer, Hackett, Lazzarino and Steptoe2015). Such alterations in the cortisol response among patients with type 2 diabetes may deteriorate glycemic control via insulin resistance and an enhanced cortisol effect.
Third, weight loss and gain are accompanied by unfavorable changes in body composition, such as body fat and lean body mass. During a negative energy balance, the loss of lean body mass is induced by the inhibition of protein synthesis and promotion of protein breakdown, which increases the risk of sarcopenia, especially in vulnerable populations (for example, people with type 2 diabetes) (Cava, Yeat, & Mittendorfer, Reference Cava, Yeat and Mittendorfer2017). During weight gain, individuals gain more fat mass than lean body mass and have body fat redistribution, such as a higher waist-to-hip circumference ratio and visceral adipose tissue than controls (Mayer et al., Reference Mayer, Walsh, Pierson, Heymsfield, Gallagher, Wang and Glasofer2005). These unfavorable changes in body composition (sarcopenia) (Chang, Hsu, Wu, Huang, & Han, Reference Chang, Hsu, Wu, Huang and Han2017) and fat distribution (abdominal obesity) (Hryhorczuk, Sharma, & Fulton, Reference Hryhorczuk, Sharma and Fulton2013) could be risk factors for depression. Moreover, DM increases chronic oxidative stress and inflammation, leading to sarcopenic obesity and depression (Oguntibeju, Reference Oguntibeju2019).
From our stratification analyses, young adults (<65 years), men, and those with newly diagnosed type 2 diabetes had a more prominent association between body weight change and depression risk. Thus, the impact of body weight change on the incidence of depression may have been greater in these groups. Older adults generally have a higher prevalence of depression than younger adults, with a lower threshold for depression due to the reduced metabolism of serotonin and noradrenaline (Gottfries, Reference Gottfries1998). A higher susceptibility to depression among women than men due to biological differences, such as estrogen cycling, could be a reason for the higher prevalence of depression among women (Albert, Reference Albert2015). Such high vulnerability to depression among older adults and women might mitigate the differences in the risk of depression based on body weight changes. Regarding the duration of type 2 diabetes, taking antidiabetic agents for a longer duration may partially attenuate the magnitude of the association between body weight change and depression. Previous studies have reported that antidiabetic agents, particularly metformin, which is widely used as the first choice of treatment for type 2 diabetes, can prevent depression through neuroprotective effects (Guo et al., Reference Guo, Mi, Jiang, Xu, Tang, Tian and Wang2014). Furthermore, certain classes of antidiabetic medication may cause weight changes. Thus, those taking antidiabetic agents for longer durations may have a less pronounced relationship between weight change and depression.
The American Diabetes Association and the United States Preventive Services Task Force strongly recommend routine screening for depression and diabetes-related distress in adults with type 2 diabetes, because the co-existence of diabetes and depression can lead to inadequate diabetes control (Owens-Gary et al., Reference Owens-Gary, Zhang, Jawanda, Bullard, Allweiss and Smith2019). Our findings suggest a strategy from the viewpoint of risk stratification for depression incidence; therefore, we can intensively apply screening tools for depression in patients with type 2 diabetes who experience weight gain or loss during their regular visits.
This study has several limitations. First, we used nationwide claims data; thus, we could not distinguish between intentional and unintentional weight change. However, both intentional and unintentional weight loss were associated with depressive symptoms. However, further studies are required to clarify this relationship. Second, reverse causality could exist, although we excluded depression incidence before follow-up and applied a lag-time analysis to minimize this possibility. The average time from depression onset to the first treatment was 3.4 years in Korea. Thus, early or ongoing depressive symptoms may affect body weight. Third, the generalizability to other ethnic groups and the lowest-income groups is limited. In contrast to other ethnic/racial groups, patients with non-obese type 2 diabetes with low insulin secretion capacity are more common in the Korean population. We did not include individuals in the lowest 3% income bracket who were supported by medical aid programs. However, the population in this low-income group was relatively small and did not have a different association from the main findings. Fourth, patients with depressive symptoms might have low adherence to regular follow-up visits as well as national health check-ups; therefore, they are more likely to be excluded from this study population. However, when we compared the risk of depression between those who were included and excluded, there was a small difference in the incidence rate (32.0 v. 32.5 per 1000 person-years, p-value <0.001). Furthermore, our analysis revealed a notable difference between the included and excluded populations, particularly in terms of sex distribution, indicating a potential presence of selection bias. Finally, the absence of data regarding the use of psychotropic medication limited our analysis, despite acknowledging their impact on weight changes through metabolic aberrations.
Conclusions
A U-shaped association between body weight change and risk of depression was observed in this large nationwide cohort study. This suggests that healthcare providers should prioritize patients with type 2 diabetes and weight change (gain or loss) for depression screening to improve their health status.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291724000515.
Data availability statement
Data supporting the findings of this study are available from the Korean NHIS and were used under license for this study (http://nhiss.nhis.or.kr). Restrictions apply to their availability (the data are not publicly available). Data are available upon request with permission from the Korean NHIS.
Acknowledgements
None.
Author contributions
EYK, S-MJ, and KH contributed to the study design and conception. K-NL contributed to the data acquisition and analyses. EYK and S-MJ drafted the manuscript. EYK, S-MJ, YBL, and KH contributed to data interpretation. EYK, S-MJ, YBL, K-NL, and KH revised and approved the final version of the manuscript. KH had full access to all the data analyzed in this study and takes responsibility for the integrity and accuracy of the data analyses. SMJ is the guarantor of the manuscript. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted. All the authors have read and approved the final manuscript.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.








 Open access
Open access