


There have been recent attempts to codify behaviours associated with early neglect and institutionalisation (Reference Chisolm, Carter and AmesChisolm et al, 1995; Reference Zeanah, Scheeringa and BorisZeanah et al, 2004) into a psychiatric category. Both DSM–IV and ICD–10 describe reactive attachment disorder, with two subtypes encompassing inhibited and disinhibited behaviour (World Health Organization, 1992; American Psychiatric Association, 1994). Questions remain about the nosology of the syndrome beyond age 5 years (American Academy of Child and Adolescent Psychiatry, 2005), therefore we simply refer to ‘attachment disorder behaviours’. We seek to extend the extant literature by testing two hypotheses: first, that the two subtypes are distinct from one another and from other common behavioural and emotional problems in young children, and second that these behavioural patterns are environmentally mediated. We capitalise on a twin study, a design that provides particular leverage in testing environmental hypotheses.
METHOD
Participants
The sampling frame, described in detail elsewhere (Reference Trouton, Spinath and PlominTrouton et al, 2002), was 13 940 twin pairs from the 1994 and 1995 birth cohorts of the Twins Early Development Study, tested as they reached their eighth birthday. Informed written consent was obtained from all participants. Questionnaires were sent to the parents of 13 940 twin pairs aged 7–9 years, and questionnaires for 6771 pairs (48.6%) were returned. Thirty-five pairs of twins were excluded because of missing data, leaving a final sample of 13 472 twins of average age 7.9 years. There were minor differences between the twin pairs enrolled in the study initially and those for whom questionnaires were returned, in ethnicity (87.5% White mothers in first wave v. 93.9% in current wave), mothers with A-level as highest qualification (11.6% v. 14.1%) and mothers who were working (39.6% v. 43.5%).
Measures
We previously used a questionnaire for reactive attachment disorders in clinical and general population samples aged 5–16 years (Reference Minnis, Rabe–Hesketh and WolkindMinnis et al, 2002). It was a checklist of attachment disorder behaviours of both the inhibited and disinhibited types, as described in ICD–10 (World Health Organization, 1992). During pilot work, items were added at the suggestion of parents and clinicians, the wording of other items was modified (Reference Minnis, Rabe–Hesketh and WolkindMinnis et al, 2002) and items were removed that failed to discriminate between children from the general population and children living in foster care (Reference Millward, Kennedy and TowlsonMillward et al, 2006). The resulting questionnaire used in the present study, the Relationship Problems Questionnaire (RPQ; see online appendix), is an 18-item parent-report questionnaire with an internal consistency (Cronbach's α) of 0.85 in this data-set. It has four possible responses (‘exactly like my child’, ‘like my child’, ‘a bit like my child’ and ‘not at all like my child’), scored 3, 2, 1 and 0 respectively (maximum possible score 54).
The Strengths and Difficulties Questionnaire (SDQ; Reference GoodmanGoodman, 1997) is a 25-item screening instrument for common child mental health problems which has been well validated against other screening instruments such as the Child Behavior Checklist (Reference Goodman and ScottGoodman & Scott, 1999) and against psychiatric diagnosis (Reference Goodman and ScottGoodman & Scott, 1999; Reference Goodman, Ford and SimmonsGoodman et al, 2003). It has sub-scales for emotional problems, conduct problems, hyperactivity, problems with peer relationships and prosocial behaviour. It has three possible responses (‘not true’, ‘somewhat true’ and ‘definitely true’), scored 0, 1 or 2.
Parents completed questions described in detail elsewhere (Reference Asbury, Dunn and PikeAsbury et al, 2003) on the use of discipline, including reasoning, spanking and ignoring misbehaviour, which gave composite scores for ‘parental warmth’, ‘negativity’ and ‘harsh parenting’. For harshness, items were rated on a six-point scale from ‘I rarely or never do this’ to ‘I usually do this’. One-year test–retest reliability was 0.52. Warmth and negativity were rated on a five-point scale from ‘definitely true’ to ‘definitely untrue’, and the 1-year test–retest reliability was 0.50. A measure of general cognitive functioning was derived from verbal and non-verbal cognitive ability tests adapted for telephone administration (Reference Petrill, Rempell and OliverPetrill et al, 2002).
Phenotypic factor analysis
Principal components analysis was used to explore the underlying structure of the RPQ. The optimal number of factors was identified using a scree plot (Reference CattellCattell, 1966). Both orthogonal and oblique methods of rotation were tried and all gave similar results. Varimax rotation is the analysis presented here. The twin design was exploited as an opportunity to repeat the factor analysis and see if similar results were produced on both occasions. Data were analysed separately for each member of a twin pair and correlations were calculated between each of the factor loadings. In order to explore whether it is possible to discriminate between attachment disorder behaviours and other mental health problems, the factor analysis included RPQ items plus SDQ items for emotional problems, conduct problems and hyperactivity.
RPQ scores and parenting
We explored the association between RPQ scores and parental warmth/harsh parenting using linear regression analysis controlling for age, gender, paternal social class (Office of Population Censuses and Surveys, 1995) and the child's cognitive ability.
Quantitative genetic analyses
The hypothesis that there is a genetic component to attachment disorder behaviours was tested first by comparing intraclass correlations between RPQ scores for monozygotic twins with those for dizygotic twins, and then by model fitting.
Each genetic factor influencing human behaviour is presumed to contribute only a small amount, and may have an additive effect with other genetic factors. Dominance effects may also be important – dominance is the extent to which the effects of alleles at a locus fail to ‘add up’ to produce genotypic values. If the effect of a locus involves dominance, there are effects of a combination of alleles at that particular locus. Additive and dominant genetic effects are defined so as to be independent of one another (Reference Plomin, DeFries and McClearnPlomin et al, 2001). Environmental factors can be shared, i.e. can be influences that make children growing up in the same family similar, or non-shared, which refers to all other environmental factors (Reference Plomin and DanielsPlomin & Daniels, 1987).
Intraclass correlational analyses
The fact that monozygotic twins share all of their genetic material whereas dizygotic twins share only about 50% can be used to estimate the genetic and environmental influences on attachment disorder behaviours. If shared environmental influences were predominant, twin correlations would be large and similar for monozygotic and dizygotic twins. If non-shared environmental influences were predominant, twin correlations would be small but similar for both types of twins. If, however, genetic influences were significant, monozygotic twin correlations would exceed dizygotic twin correlations.
Model-fitting analyses
Maximum likelihood model-fitting analyses estimate the contributions of additive genetic (A), shared environmental (C), dominance (D) and non-shared environmental effects (E). A model incorporating additive genetic, shared and non-shared environmental effects (ACE model) was considered first. An ADE model, considering dominance effects instead of shared environmental effects, was then fitted and the two compared. A chi-squared goodness-of-fit test was applied to each model (Reference Neale, Boker and XieNeale et al, 2003).
Analyses were carried out using both the total RPQ score and the sub-scales generated in the factor analysis and were done separately for male and female twins. The twins were double-entered so each child appears as twin one and as twin two to help to eliminate any bias due to birth order, and 95% confidence intervals were adjusted accordingly. Behavioural genetic modelling was done using Mx (Reference Neale, Boker and XieNeale et al, 2003) and all other analyses used the Statistical Package for the Social Sciences, Version 11. The covariance matrices were used to input the data into Mx and only same-sex twin pairs were included in the analysis.
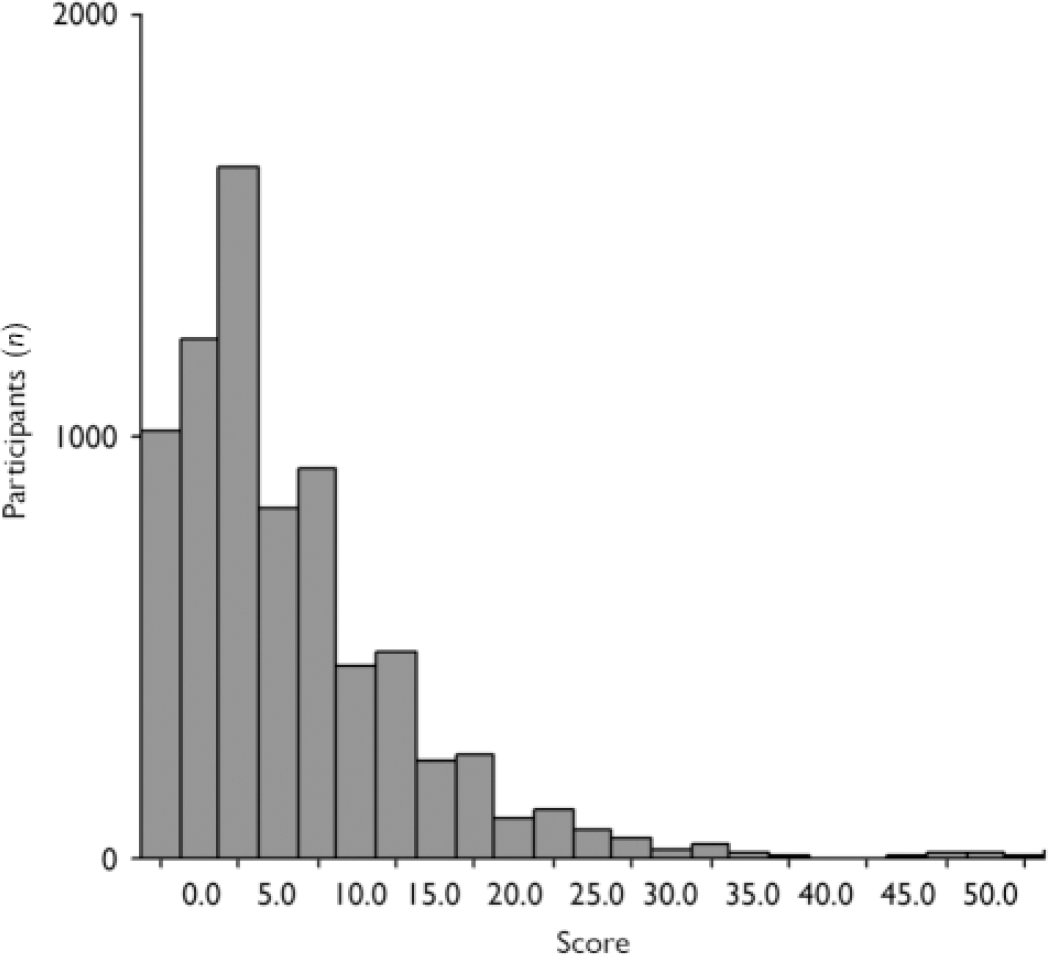
Fig. 1 Distribution of Relationship Problems Questionnaire scores.
RESULTS
Distribution of RPQ scores
The RPQ scores in this population appeared to be continuously distributed, although strongly skewed (Fig. 1).
Factor analysis
For the RPQ factor analysis, a scree plot suggested a three-factor solution. Rotated factor 1 had six questions that loaded highly on it: ‘unpredictable friendliness’, ‘runs away when approached’, ‘false affection’, ‘has no conscience’, ‘aggressive to self’ and ‘looks frozen with fear’. This first rotated factor explained 30% of the variance. Loading highly onto the second factor were ‘gets too physically close’, ‘too cuddly’, ‘too friendly with strangers’ and ‘asks personal questions’; this factor explained 10% of the variance. Four questions loaded highly on the last factor: ‘afraid of new situations’, ‘acts younger than age’, ‘often unhappy’ and ‘very clingy’; this factor explained 7% of the variance. The remaining four questions loaded most highly onto the third factor, but their loadings were fairly equally spread across all three factors. These were removed, one at a time, to see what effect removing them had on the remaining factor loadings. Removing them improved discrimination between the three factors and the final model used 14 questions, each of which loaded clearly and highly onto one of the three factors.
When the factor analysis was repeated for the two members of each twin pair, the correlations between the factor loadings for each of the three factor pairs were 0.998, 0.998 and 0.992 respectively, each with P≤0.001. The first factor appeared to index behaviours indicative of the inhibited form of an attachment disorder. The second factor indexed behaviours that reflect the disinhibited form of attachment disorder. The third factor suggested behaviours typical of behaviourally inhibited temperament (Reference Muris, Meesters and de KanterMuris et al, 2005), which may not be directly linked to attachment disorder. To avoid confusion with inhibited attachment disorder behaviours, we refer to this factor as the ‘temperament factor’.
Items from the conduct problems, hyperactivity and emotional problems (anxiety and depression) scales of the SDQ were then included in the factor analysis along with the 14 remaining RPQ items. The three RPQ sub-scales were still clearly distinct from one another and from the SDQ sub-scales (Table 1), with the exception that the SDQ item ‘nervous/clingy’ loaded with the RPQ temperament subscale rather than with the SDQ emotional problems sub-scale. The RPQ item ‘often unhappy’ did not load with any particular factor.
Table 1 Rotated factor loadings for 14 of the Relationship Problems Questionnaire items and 14 Strengths and Difficulties Questionnaire items, from a six-factor solution using the principal components extraction method (varimax rotation)

| Item1 | Factor | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |
| RPQ | ||||||
| Temperament items | ||||||
| Afraid of new situations | 0.738 | |||||
| Acts younger than age | 0.462 | |||||
| Very clingy | 0.526 | |||||
| Disinhibited items | ||||||
| Gets too physically close | 0.853 | |||||
| Too cuddly | 0.843 | |||||
| Asks personal questions | 0.463 | |||||
| Too friendly with strangers | 0.851 | |||||
| Inhibited items | ||||||
| Aggressive to self | 0.554 | |||||
| Has no conscience | 0.553 | |||||
| Looks frozen with fear | 0.586 | |||||
| Runs away when approached | 0.711 | |||||
| False affection | 0.703 | |||||
| Unpredictable friendliness | 0.758 | |||||
| SDQ | ||||||
| Hyperactivity | ||||||
| Restless, overactive | 0.698 | |||||
| Constantly fidgeting/squirming | 0.664 | |||||
| Easily distracted | 0.767 | |||||
| Thinks things out before acting | 0.541 | |||||
| Sees tasks through to the end | 0.737 | |||||
| Conduct problems | ||||||
| Steals | 0.633 | |||||
| Temper tantrums | 0.455 | |||||
| Obedient | 0.477 | |||||
| Often fights/bullies others | 0.580 | |||||
| Often lies/cheats | 0.683 | |||||
| Emotional problems | ||||||
| Many worries | 0.699 | |||||
| Many fears/easily scared | 0.565 | |||||
| Unhappy/tearful | 0.638 | |||||
| Nervous/clingy | 0.635 | |||||
RPQ scores and parenting variables
There were significant associations between both the inhibited and disinhibited subscales and harsh parenting and parental negativity, and significant negative associations between both sub-scales and parental positivity (Table 2) after controlling for age, gender and cognitive ability, which partially confounded these relationships (not social class, which did not act as a confounder).
Table 2 Linear regression analysis of the association between harsh parenting, parental negativity and positivity, and the Relationship Problems Questionnaire1 inhibited and disinhibited sub-scales.
| Variable | β | t | P |
|---|---|---|---|
| Harsh parental discipline v. RPQ inhibited sub-scale1 (n=3656)2 | |||
| Age | -0.050 | -3.076 | 0.002 |
| Gender | 0.127 | 7.904 | <0.001 |
| Cognitive ability at 7 years | -0.062 | -3.806 | <0.001 |
| RPQ inhibited sub-scale | 0.163 | 10.004 | <0.001 |
| Harsh parental discipline v. RPQ disinhibited sub-scale1 (n=3684) | |||
| Age | -0.049 | -3.042 | 0.002 |
| Gender | 0.138 | 8.569 | <0.001 |
| Cognitive ability at 7 years | -0.064 | -3.951 | <0.001 |
| RPQ disinhibited sub-scale | 0.133 | 8.183 | <0.001 |
| Parental negativity v. RPQ inhibited sub-scale3 (n=4753) | |||
| Gender | 0.052 | 3.663 | <0.001 |
| Social class | -0.038 | -2.685 | 0.007 |
| RPQ inhibited sub-scale | 0.190 | 13.284 | <0.001 |
| Parental negativity v. RPQ disinhibited sub-scale3 (n=4786) | |||
| Gender | 0.069 | 4.844 | <0.001 |
| Social class | -0.045 | -3.115 | 0.002 |
| RPQ disinhibited sub-scale | 0.146 | 10.203 | <0.001 |
| Parental positivity v. RPQ inhibited sub-scale4 (n=3659) | |||
| Gender | 0.044 | 2.718 | 0.007 |
| Cognitive ability at 7 years | 0.057 | 3.453 | 0.001 |
| RPQ inhibited sub-scale | -0.142 | -8.590 | <0.001 |
| Parental positivity v. RPQ disinhibited sub-scale4 (n=3688) | |||
| Gender | 0.033 | 1.988 | 0.047 |
| Cognitive ability at 7 years | 0.065 | 3.907 | <0.001 |
| RPQ disinhibited sub-scale | -0.065 | -3.950 | <0.001 |
Developing sub-scales of the RPQ
Sub-scales of the RPQ were developed from the results of the factor analysis for use in behavioural genetics analyses (see Table 1). The ‘inhibited’ sub-scale included the six questions that loaded highly onto factor 1. The ‘disinhibited’ sub-scale comprised the four questions that loaded highly onto factor 2. The inhibited and disinhibited sub-scale scores are only modestly correlated (0.443) with each other and with the SDQ sub-scales (0.176–0.318). The behavioural genetics analyses were performed both for the whole 18-item RPQ and for the sub-scales.
Behavioural genetics analysis of total RPQ scores
The correlation for the 18-item RPQ items in male monozygotic twins was 0.917 (P<0.0001) and 0.599 for male dizygotic twins. This marked difference in monozygotic v. dizygotic correlation gives a clear indication of a strong genetic influence. To test this hypothesis, an ACE model was fitted and provided a significantly good fit (χ2 goodness-of-fit test), whereas the ADE model was a poor fit. Parameter estimates are shown in Table 3.
Table 3 Estimates from the ACE model based on the Relationship Problems Questionnaire and its ‘inhibited’ and ‘disinhibited’ sub-scales

| Males (n=4474) % (95% CI) | Females (n=4706) % (95% CI) | |
|---|---|---|
| RPQ — 18 items | ||
| Additive genetic | 63.5 (57.3-69.7) | 35.2 (31.7-38.8) |
| Shared environment | 28.2 (22.1-34.1) | 55.7 (51.7-59.7) |
| Non-shared environment | 8.2 (7.5-8.9) | 9.1 (8.3-9.9) |
| Inhibited sub-scale | ||
| Additive genetic | 64.5 (57.2-72.4) | 21.9 (16.8-27.7) |
| Shared environment | 24.3 (16.4-31.6) | 62.2 (57.0-67.0) |
| Non-shared environment | 11.2 (10.15-12.32) | 15.9 (14.5-17.4) |
| Disinhibited sub-scale | ||
| Additive genetic | 77.0 (69.2-85.5) | 54.8 (48.5-61.7) |
| Shared environment | 14.9 (6.4-22.7) | 36.4 (29.4-42.8) |
| Non-shared environment | 8.1 (7.4-9.0) | 8.8 (8.0-9.7) |
Behavioural genetic modelling assumes multivariate normality, but these data were highly skewed to the left. Various transformations of the data were unsuccessful in producing a normal distribution. More importantly, if a suitable transformation was achieved, this would almost certainly lead to a loss of much of the important information relating to the variation. However, the ACE model gives almost identical results to those produced by the correlation calculations, which make no assumption about the distributions of the data.
The same analyses were performed on the female twin data. Total RPQ scores for female monozygotic twins are highly correlated (correlation coefficient 0.914). The female dizygotic twins were more highly correlated (correlation coefficient 0.716) than the male dizygotic twins (0.599). The ACE model was fitted and again the ω2 goodness-of-fit test indicated that this was the best fit. The ADE model again demonstrated a significant reduction in fit. Parameter estimates are shown in Table 3. The confidence intervals for additive genetic effects and shared environment do not overlap when comparing males and females, indicating that they are significantly different.
Behavioural genetics analysis of inhibited and disinhibited sub-scales
It was clear that there is genetic influence on the inhibited sub-scale scores, as the monozygotic correlation was 0.880 for males and 0.846 for females, compared with dizygotic correlations of 0.571 and 0.713 respectively for males and females. For the disinhibited sub-scale the monozygotic correlation was 0.923 for males and 0.918 for females, compared with dizygotic correlations of 0.533 and 0.616 respectively for males and females. Model fitting found that the ACE models again gave the best fit compared with the ADE model and estimates are shown in Table 3. For males, the majority of the variance in the inhibited and disinhibited sub-scales was explained by additive genetic effects. This was also true for the disinhibited sub-scale for females, whereas for the inhibited sub-scale the majority of the variance was explained by shared environmental effects. Again, the contribution of additive genetic effects and shared environment was significantly different for males and females.
DISCUSSION
Our findings demonstrate that behaviours suggestive of attachment disorder can be identified in school-age children from the general population, are associated with harsh parenting and can be discriminated from conduct problems, emotional problems and hyperactivity. In this first twin study of these behaviours, we have shown that both genes and environment have a significant role in their aetiology.
Genetic effects appear particularly important for boys. Interestingly, Zeanah & Fox (Reference Zeanah and Fox2004) have postulated that temperamental factors such as withdrawn–inhibited behaviour or impulsivity may put a child at greater risk of attachment disorder in the context of maltreatment. They give the example of 20-month-old twins who were raised in the same seriously neglectful environment; the boy developed disinhibition, whereas the girl became emotionally withdrawn and inhibited (Reference Hinshaw–Fuselier, Boris and ZeanahHinshaw-Fuselier et al, 1999). Quite what the gender modification of the genetic effect means is not yet clear and requires replication, but a range of biological candidates could be investigated in this context, including stress hormones and neuropeptides.
Shared environment explained more variance in females than in males. Although this could perhaps be accounted for by a greater similarity in parental behaviour with girls than with boys, it is an intriguing finding. As the shared environmental effect that is likely to be of most importance in the aetiology of attachment disorder is maltreatment (Reference Zeanah and FoxZeanah & Fox, 2004), this needs to be further investigated in maltreated children.
In terms of genes that might be involved, an X-linked genetic–environmental interaction has been found in the development of conduct disorder (Reference Caspi, McClay and MoffittCaspi et al, 2002) as well as a link between the dopamine D4 receptor gene (DRD4) and disorganised attachment (Reference Lakatos, Toth and NemodaLakatos et al, 2000). It is early days in molecular genetic attachment research, but our findings reinforce the notion that this might be a fruitful future direction.
Methodological considerations
We used the RPQ as a screening tool in a community sample, and do not assert that the children reported as demonstrating these behaviours had reactive attachment disorder; in order to define such disorder, detailed diagnostic examinations would be required and, according to DSM–IV, symptoms would have had to be present before the age of 5 years (American Psychiatric Association, 1994). We are not certain whether mothers or fathers completed the parent-report questionnaires, which could have affected the results. This kind of population-based research requires simple tools, and complements but does not replace more clinically focused research.
Our study is limited by factors known to apply to twin studies in general (Reference MaccobyMaccoby, 2000). For example, correlations between twins’ scores could be affected by reporting bias on the part of parents. The skewness of the distribution might have limited the model-fitting analysis, but is unlikely to have seriously affected the interpretation of the results, because the correlational calculations (which do not depend on a normal distribution) gave very similar results. The response rate of just less than 50% means that the sample may differ systematically from the general population in known and unknown ways. We are likely to have lost to follow-up the participants with the most significant psychosocial problems, so it is particularly interesting that even in a sample that was probably healthier than the general population, behaviours suggestive of attachment disorder were identified.
To our knowledge, no diagnostic instrument yet exists for attachment disorder in children of this age, but one is currently being developed by our group and will include information from parents, teachers and observation of the child. Only future research will determine whether these behaviours do, in fact, predict a diagnosis of attachment disorder and one method would be to follow up children who had high RPQ scores with a detailed diagnostic assessment. For a disorder in which some behaviours, such as overfriendliness, are on a continuum with normal behaviour, the lack of more detailed clinical information may increase the likelihood of false positive responses.
Two of the items that loaded on the ‘inhibited’ factor – ‘has no conscience’, and ‘false affection’ – are not part of the DSM or ICD classification of inhibited reactive attachment disorder. False affection would perhaps be expected to load with the disinhibited factor, although recent research has suggested that clinically the two subtypes can be mixed (Reference Zeanah, Scheeringa and BorisZeanah et al, 2004). Including these two items would broaden the phenotype of inhibited reactive attachment disorder and, as there is consensus that the inhibited phenotype is less well defined than the disinhibited phenotype (American Academy of Child and Adolescent Psychiatry, 2005), clarity about the nosological boundaries of the inhibited disorder will be an important future research focus. In the light of this apparent broadening, it is reassuring that our factor analysis suggests clear demarcation between both attachment disorder subtypes and other forms of child psychopathology such as conduct disorder.
This research design allowed us to examine attachment disorder behaviours as they were distributed in a sample approximating the general population, their discrimination from behaviours suggestive of other disorders and the possibility of genetic mediation. The significant associations between RPQ scores and indices of harsh or negative parenting suggest we are investigating the same domain of functioning (but perhaps less extreme behaviours) that we would be investigating in a maltreated sample. A study of maltreated or severely neglected twins might yield different findings regarding the balance of genetic and environmental influence, but would be difficult if not impossible to construct.
Clinical implications
Attachment disorder behaviours have previously been considered in samples of children who are known to have been maltreated or institutionalised. These data demonstrate that attachment disorder behaviours are present in the general population, are associated with harsh or negative parenting behaviour and may be mediated by both environment and genetics. The clear demarcation, in our factor analysis, of reactive attachment disorder behaviours from other forms of psychopathology may help clinicians develop appropriately targeted treatments for these behaviours. Future research identifying the candidate genes and the types of environments that have a causal role will have a major impact on prevention and intervention strategies.







eLetters
No eLetters have been published for this article.