



Childhood obesity is one of the most threatening and alarming public health problems in the world(Reference Chung, Krenek and Magge1). The estimated prevalence of overweight or obesity among children under the age of 5 was approximately 39 million in 2020 and for children aged 5–19 years, it was around 150 million. These numbers are projected to increase to approximately 40 million and 254 million, respectively, by the year 2030(2). Childhood obesity has the potential to persist into adulthood and leads to adverse cardiovascular outcomes or other obesity-related diseases(Reference Kumar and Kelly3,Reference Grossman, Bibbins-Domingo and Curry4) . Therefore, to identify modifiable risk factors for overweight and obesity in children is essential to implement corresponding interventions to reduce the burden of disease.
The aetiology of obesity is complex, and inflammation and oxidative stress are considered to be the key mechanisms of obesity(Reference Fernández-Sánchez, Madrigal-Santillán and Bautista5). Environmental tobacco exposure is a major health problem for children, and exposure to tobacco smoke was associated with increased inflammatory responses, oxidative stress and endocrine disorders, which may promote the development of obesity(Reference Barnoya and Glantz6,Reference Tziomalos and Charsoulis7) . Tobacco exposure mainly includes active smoking and second-hand smoke exposure. Cotinine, a direct metabolite of nicotine in tobacco, is a specific and sensitive marker of recent tobacco smoke exposure(Reference Lang, Dozor and Holbrook8). Previous evidence indicated that higher levels of cotinine were associated with increased risk of childhood obesity in both active and passive smokers(Reference Merianos, Jandarov and Khoury9).
Vitamin-D deficiency is one of the most common nutritional problems, which is considered an anti-inflammatory nutrient, and vitamin-D deficiency may affect the risk of obesity through chronic low-grade inflammation(Reference Wamberg, Pedersen and Rejnmark10). Epidemiological investigations revealed that vitamin-D levels were lower in smokers than in non-smokers, and a positive correlation between tobacco exposure and vitamin-D deficiency was identified(Reference Wang, Wang and Jiang11–Reference Yang, Sato and Saito-Abe13). Animal experiments found that vitamin-D deficiency exacerbated the elevation of proinflammatory cytokines and chemokines caused by tobacco smoke(Reference Heulens, Korf and Cielen14). In addition, vitamin-D and tobacco exposure were found to have combined effects on many diseases such as hypertension in adults(Reference Knihtilä, Huang and Prince15–Reference Wu, Wu and Rao18). Thus, we suspected that vitamin-D and tobacco exposure might have combined effects on the risk of overweight and obesity in children.
This study aimed to explore the combined effects of serum vitamin-D level and tobacco exposure on the risk of overweight and obesity in children based on data from the National Health and Nutrition Examination Surveys (NHANES). The analysis was also stratified by gender, age, race and household smokers.
Methods
Study design and population
This cross-sectional study involved in the data of 19 155 children aged 2–17 years from the NHANES database from 2007 to 2018. The NHANES was a nationally representative survey of nutrition and health condition in the USA (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx). The survey integrated health interviews conducted in respondents’ residences with health measurements carried out at mobile exam centres (MEC). The examination components encompassed medical, dental and physiological measurements, as well as laboratory tests supervised by trained medical personnel(Reference Wang, Zhao and Nie19). In our study, individuals aged 2–18 years with the assessment of height and weight and complete data of serum vitamin-D and cotinine were identified. Participants without complete information of key covariates were excluded. This study has been exempted from an ethical review in our study because this study used the data from public database. The NHANES survey got the NCHS Ethics Review Board (ERB) approval (2007–2008 (Continuation of Protocol #2005-06), 2009–2010 (Continuation of Protocol #2005-06), 2011–2012 (Protocol #2011-17), 2013–2014 (Continuation of Protocol #2011-17), 2015–2016 (Continuation of Protocol #2011-17, and 2017–2018 (Continuation of Protocol #2011-17 & Protocol #2018-01)).
Potential covariates and definitions
Age (years), gender (boys or girls), race (White, Black or other), PIR (< 1·3, ≥ 1·3 or unknown), education level (below high school, high school or above high school), birth weight (< 5·5 pounds, ≥ 5·5 pounds or unknown), physical activity (not ideal physical activity, ideal physical activity or unknown), sedentary time (< 5 h, or ≥ 5 h), maternal smoking during pregnancy or not, household smokers (nobody or ≥ 1), energy (kcal), fat (gm), protein (gm) and carbohydrate/fibre and dietary vitamin-D (mcg) were potential covariates analysed in our study.
Physical activity was converted into energy consumption, which was calculated according to the response in the questionnaire. Energy consumption (metabolic equivalent of task × min) = metabolic equivalent of task (metabolic equivalent of task) × the duration of the corresponding activity (min). Ideal physical activity was defined as ≥ 180 metabolic equivalent of task × min/day or ≥ 60 min/day (for children aged 2–11 years old), otherwise it was not ideal physical activity. Through the individual’s daily hours of television, video or computer usage based on in-person interview data and categorised into three groups: < 3 h, 3–6 h and ≥ 6 h(Reference Jia, Wu and Su20).
Main variables
Serum vitamin-D and cotinine levels were main variables.
Serum vitamin-D was calculated as follows:
25 (OH) D2:1 nmol/l = 0·41266 ng/ml.
25 (OH) D3:1 nmol/l = 0·40066 ng/ml.
Vitamin-D (ng/ml) = 25 (OH) D2 × 0·41266 × 0·40066 + 25 (OH) D3. Serum vitamin-D status was classified as 20 ng/ml for adequate and < 20 ng/ml for insufficient(Reference Amrein, Scherkl and Hoffmann21,Reference Fiamenghi and Mello22) .
The serum 25(OH)D concentrations were measured at the National Center for Environmental Health, CDC, Atlanta, GA using the DiaSorin RIA kit (Stillwater MN). The manufacturer reformulated the DiaSorin assay kit used to measure 25(OH)D in NHANES III in 1998 (after completion of NHANES III analyses), incorporating: (1) an improved binding antibody and (2) a modified washing solution to reduce non-specific binding. To evaluate the impact of these changes on observed trends in population serum 25(OH)D levels, a subset of banked serum samples from NHANES III was reanalysed by the CDC laboratory using the reformulated version of the RIA. The NHANES III results obtained with the reformulated assay were compared against those obtained with the original assay for these reanalysed specimens (https://wwwn.cdc.gov/Nchs/Nhanes/vitamind/analyticalnote.aspx?b=2007&e=2008&d=VID_E&x=htm).
Cotinine was identified through the serum levels of cotinine, which was grouped into cotinine ≥ 0·05 ng/ml (the presence of tobacco exposure) and cotinine < 0·05 ng/ml (the absence of tobacco exposure)(Reference Homa, Neff and King23). Serum cotinine is quantified using an isotope dilution-high performance liquid chromatography/atmospheric pressure chemical ionisation tandem mass spectrometry (ID HPLC-APCI MS/MS) method. Briefly, the serum sample is spiked with methyl-D3 cotinine as an internal standard and subjected to a basified solid-phase extraction column for equilibration. Cotinine is extracted from the column using methylene chloride, and the organic extract is concentrated before being injected onto a short C18 HPLC column. The eluate from these injections undergoes APCI-MS/MS monitoring, with quantitation of the m/z 80 daughter ion from the m/z 177 quasi-molecular ion along with additional ions for internal and external standards and confirmation purposes. Cotinine concentrations are determined by comparing native to labelled cotinine ratios in samples against a standard curve (–https://wwwn.cdc.gov/Nchs/Nhanes/2007–2008/COTNAL_E.htm).
Outcome
Overweight and obesity in children was the outcome, which was evaluated by BMI. For children, BMI was converted to a BMI z-score accounting for age and sex using the recommended CDC percentiles. A BMI z-score of ≥ 85th percentile and < 95th percentile indicates overweight status, and a BMI z-score of ≥ 95th percentile indicates obesity(Reference Tsoi, Li and Feng24) (About Child & Teen BMI | Healthy Weight, Nutrition, and Physical Activity | CDC).
Statistical analysis
Measurement data were described as mean and se, and weighted t test was used for comparison between groups. Enumeration data were described as number and percentage of cases (n (%)), and χ2 test was used for comparison between groups. SDMVPSU, SDMVSTRA and WTMEC2YR were weight used in this study. Missing values are shown in online Supplementary Table 1. The mean matching prediction method was used to fill in the missing variables, and sensitivity analysis was performed before and after missing values manipulation. The results delineated that no significant difference was found between the data of before and after missing values manipulation (online Supplementary Table 2). Potential covariates were identified via univariable weighted logistic regression model. Univariable and multivariate weighted logistic regression models were used to analyse the associations of serum vitamin-D or cotinine levels with overweight and obesity in children as well as the combined effects of serum Vitamin-D and cotinine on the risk of overweight and obesity in children. Subgroup analysis was performed in terms of gender, age, race and household smokers. The relative excess risk due to interaction, the attributable proportion due to interaction (AP) and the synergy index (S) were applied to evaluate the interaction of serum vitamin-D and cotinine on the risk of overweight and obesity in children. OR with corresponding 95 % CI were presented. SAS 9.4 was applied for statistical analysis. P < 0·05 was considered statistical significance.
Results
The characteristics of children with underweight and healthy weight or overweight and obesity
In total, the data of 19 155 children aged 2–18 years old were identified from NHANES database. BMI is crucial for defining overweight and obesity in children. Vitamin-D and cotinine were main variables in this study, missing these data could not be analysed. Among them, those without information on BMI assessment (n 1102), serum vitamin-D (n 4103) and cotinine (n 1167) were identified. Energy intake might affect BMI status of children. Also, individuals without energy intake data were excluded (n 1147). Finally, 11 636 children were included. All the participants were divided into underweight and healthy weight group (n 6998), and overweight and obesity group (n 4638). The screening process of all participants was presented in Fig. 1.

Fig. 1. The flow chart of screening process of subjects. NHANES, the National Health and Nutrition Examination Surveys.
As observed in Table 1 and Table 2, the mean serum vitamin-D level in the overweight and obesity group was lower than the underweight and healthy weight group (25·14 ng/ml v. 28·23 ng/ml). The percentage of participants with serum vitamin-D ≥ 20 ng/ml in the overweight and obesity group was lower than the underweight and healthy weight group (75·81 % v. 84·59 %). The percentage of children with cotinine level ≥ 0·05 ng/ml in the overweight and obesity group was higher than the underweight and healthy weight group (44·25 % v. 39·14 %). More information on the characteristics of participants are depicted in Table 1 and Table 2.
Table 1. The characteristics of participants with different BMI (Mean values with their standard errors; numbers and percentages)
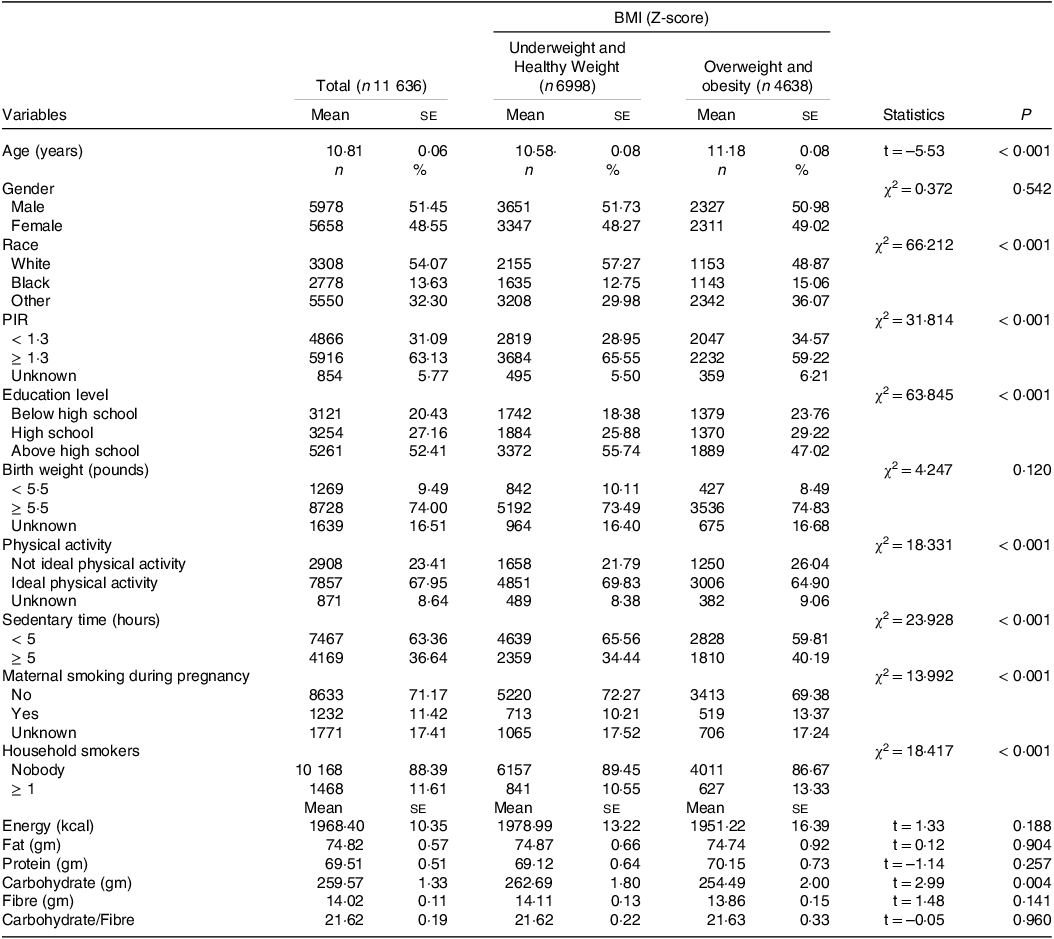
PIR, poverty to income ratio.
Table 2. The serum Vitamin-D and cotinine status of participants with different BMI (Mean values with their standard errors; numbers and percentages)

PIR: poverty to income ratio.
Combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children
The potential covariates are shown in online Supplementary Table 3, which indicated that age, race, PIR, education, birth weight, physical activity, sedentary time, maternal smoking during pregnancy and household smokers were covariates associated with overweight and obesity in children.
In the univariable analysis, serum vitamin-D < 20 ng/ml was associated with increased risk of overweight and obesity in children compared with those with serum vitamin-D ≥ 20 ng/ml (OR = 1·75, 95 % CI: 1·58, 1·95). After adjusting for relevant covariates, the association between serum vitamin-D < 20 ng/ml and elevated risk of overweight and obesity in children was still significant (OR = 1·44, 95 % CI: 1·29, 1·61). The crude model revealed that compared with children with cotinine < 0·05 ng/ml, subjects with cotinine ≥ 0·05 ng/ml was a risk factor for overweight and obesity (OR = 1·23, 95 % CI: 1·12, 1·35). In the adjusted model, the odds of overweight and obesity in children was 1·14 (OR = 1·14, 95 % CI: 1·01, 1·29) in children with cotinine ≥ 0·05 ng/ml. Relative to participants with serum vitamin-D ≥ 20 ng/ml and cotinine < 0·05 ng/ml, increased risk of overweight and obesity was identified in those with serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml (OR = 1·45, 95 % CI: 1·26, 1·68) and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml (OR = 1·62, 95 % CI: 1·38, 1·91) (Table 3). The combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children are exhibited in Fig. 2. No significant interaction between serum vitamin-D and cotinine on the risk of overweight and obesity in children was identified (relative excess risk due to interaction = 0·028, 95 % CI: −0·256, 0·312), AP = 0·017, 95 % CI: −0·157, 0·191), S = 1·047, 95 % CI: 0·654, 1·675)) (online Supplementary Table 4).
Table 3. Combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children (Odds ratios and 95 % confidence intervals)

Ref, reference; PIR, poverty to income ratio.
Model 1: the crude model.
Model 2: adjusted for age, race, PIR, education, birth weight, physical activity, sedentary time, maternal smoking during pregnancy, and household smokers.

Fig. 2. The combined effects of serum Vitamin-D and cotinine on the risk of overweight and obesity in children.
Subgroup analysis of the combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children
Gender
Serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml were related to increased risk of overweight and obesity in boys. Serum vitamin-D ≥ 20 ng/ml and cotinine ≥ 0·05 ng/ml, serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml were associated with elevated risk of overweight and obesity in girls (Table 4).
Table 4. Subgroup analysis of the combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children (odds ratios and 95 % confidence intervals)
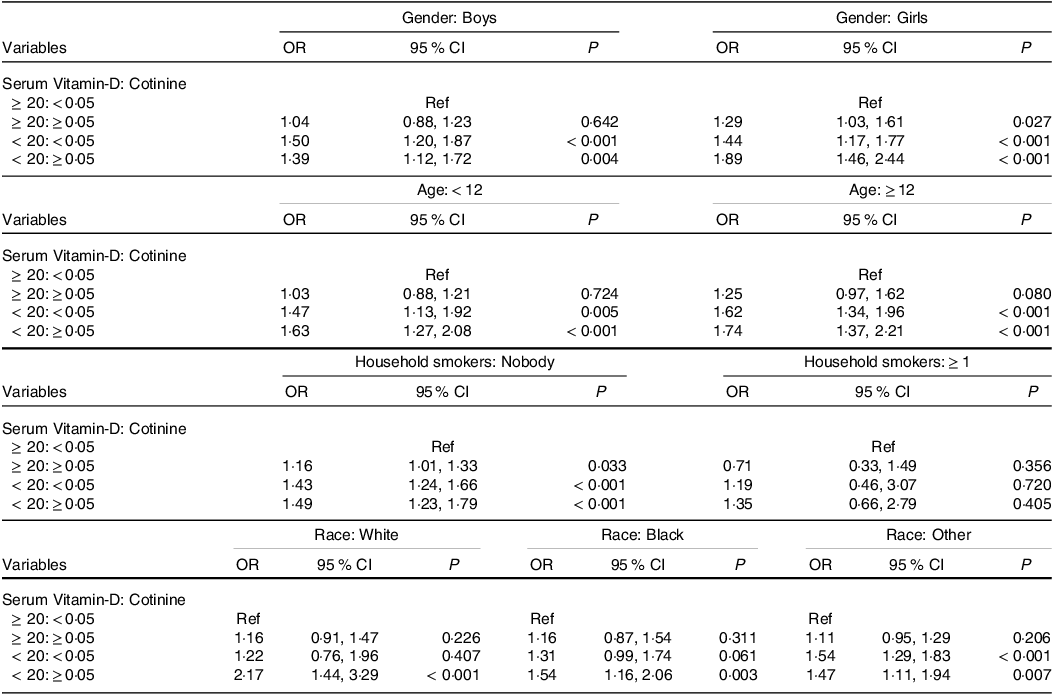
PIR, poverty to income ratio; Ref, reference.
Model 1: the crude model.
Model 2: if not stratified, adjusted for age, race, PIR, education, birth weight, physical activity, sedentary time, maternal smoking during pregnancy, and household smokers.
Age
Serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml were related to increased risk of overweight and obesity in both participants aged < 12 years and ≥ 12 years (Table 4).
Household smokers
Serum vitamin-D ≥ 20 ng/ml and cotinine ≥ 0·05 ng/ml, serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml were associated with elevated risk of overweight and obesity in subjects with household smokers (Table 4).
Race
The increased risk of overweight and obesity was observed in White or Black with serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml. Serum vitamin-D < 20 ng/ml and cotinine < 0·05 ng/ml and serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml were associated with elevated risk of overweight and obesity in other races (Table 4).
Discussion
The present study evaluated the associations of serum vitamin-D level and tobacco exposure with the risk of overweight and obesity in children. In addition, the combined effects of serum vitamin-D level and tobacco exposure on the risk of overweight and obesity in children were investigated. The results revealed that serum vitamin-D < 20 ng/ml or cotinine ≥ 0·05 ng/ml was associated with increased risk of overweight and obesity in children. Moreover, we observed the combined effects of serum vitamin-D and cotinine on the risk of overweight and obesity in children. The findings might provide a reference for achieving benefits through the joint implementation of multiple risk prevention and control strategies in the future.
In a previous study, a high prevalence of serum 25(OH)D deficiency in children between 4 and 14 years old in Chile (80·4 %) was identified, and the study revealed that obese and overweight children had the highest prevalence of serum 25(OH)D deficiency(Reference Pérez-Bravo, Duarte and Arredondo-Olguín25). In addition, 25-OH-D insufficiency was common in children and adolescents in Bucaramanga, Colombia, which was associated with overweight or obesity(Reference Rojas, Quintero-Lesmes and Gamboa-Delgado26). Akter et al. depicted that vitamin-D deficiency and Vitamin-D receptor gene polymorphisms were correlated with the risk of obesity in children(Reference Akter, Afrose and Sharmin27). The inverse association between serum vitamin-D levels and measures of adiposity in children was also observed(Reference Cunha, Magalhães and Loureiro28). These findings might support the results in the current study, which demonstrated the association between serum vitamin-D < 20 ng/ml and increased risk of overweight and obesity in children. On the other hand, the exposure to in utero maternal smoking and current exposure to household environmental tobacco smoke were found positively associated with childhood overweight/obesity(Reference Chen, Chen and Hsieh29). Another study similarly observed a positive correlation between increasing levels of cotinine and the risk of overweight and obesity in children and adolescents(Reference Luo, Zhang and Lu30). The results of the above studies provide evidence to the findings of our study. We found that cotinine ≥ 0·05 ng/ml was associated with increased risk of overweight and obesity in children.
In prior studies, tobacco smoke exposure was reported to be an independent predictor of vitamin D deficiency in children(Reference Nwosu and Kum-Nji31,Reference Clemente, Argiolas and Bassu32) . The interaction between tobacco smoke exposure and low vitamin D on disease was not reported. In our study, we also did not identify the interaction between tobacco smoke exposure and low vitamin D on the risk of overweight and obesity in children. Therefore, we further explore the joint effects of serum vitamin-D and tobacco smoke exposure on the risk of overweight and obesity in children. We found that the combined effects of serum vitamin-D < 20 ng/ml and cotinine ≥ 0·05 ng/ml on the risk of overweight and obesity in children was identified. The result was allied with formerly published literatures. Previously, Knihtilä et al. found that cumulative tobacco smoke exposure from pregnancy to childhood was associated with dose- and duration-dependent decreases in child lung function at 6 years, and this effect was modulated by gestational vitamin D(Reference Knihtilä, Huang and Prince15). Co-exposure to passive smoking and vitamin D deficiency was reported to be associated with an elevated risk of spontaneous abortion(Reference Lin, Li and Zhang16). Shen et al. found synergistic effects of secondhand smoke and vitamin-D deficiency on the prevalence of hypertension in American women of childbearing age, with more significant effects in women who were overweight or Non-Hispanic Black(Reference Shen, Xu and Li17). The results in our study might help achieve more than expected benefits through the joint implementation of multiple risk prevention and control strategies. Sufficient vitamin-D supplement combined with cotinine exposure prevention might be a novel direction for weight management in children.
There were some limitations in this study. First, only associations among vitamin-D, cotinine exposure and weight in children, whether there were causal relationships still needs exploration. Second, the sample of NHANES was representative of children and adolescents in the USA, and further validation is required in other countries and regions. Third, the data such as diet and lifestyle were obtained by self-report, which may have a certain recall bias. In the future, more well-designed studies concerning the associations of Vitamin-D, cotinine exposure and weight in children were required to verify the findings in the current study.
Conclusions
The associations of serum vitamin-D level and tobacco exposure as well as their combined effects with the risk of overweight and obesity in children were evaluated in this study. The data indicated that serum vitamin-D and cotinine exposure had combined effects on the risk of overweight and obesity in children. These findings might provide an insight that the detection of serum vitamin-D levels and reduction of tobacco exposure might be important in reducing the risk of overweight and obesity in children.
Acknowledgements
None.
This study got the approval from The Science and Technology Commission of Shanghai Municipality (No. 23Y11921100).
Y. L., G. Z. and Y. S. designed the study. Y. L. and G. Z. wrote the manuscript. Y. L., G. Z. and Y. S. collected, analysed and interpreted the data. Y. S. critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
There are no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114524002071









 Open access
Open access