



1. Introduction
Over the past three decades, countries around the globe have introduced new or extended existing policies addressing long-term care (LTC). In many countries, this involved a considerable extension of public support for LTC. These policies, however, differ largely in terms of the policy mix – e.g. different mixes of cash and in-kind support, home-based care vs. care in institutions or the role of and the support for informal care – as well as the extent and the distribution of public support. Public policies might be targeted in different ways, addressing broad populations in need of LTC, addressing very specific needs or those with the highest care needs, or more selectively targeting those that cannot afford care from their private resources. At the core of these considerations is the objective that LTC needs should be met and that provisions should become available according to the needs of the population. Research on (un)met needs and on (in)equalities in LTC has intensified only over the past decade (Kröger, Reference Kröger2022). Most of this research focuses on in-kind provisions, on the complementarity or substitutability of formal and informal care provisions, and on the extent of unmet needs. Studies on inequalities in the take-up of cash benefits in LTC are still very limited (e.g. Arrighi et al., Reference Arrighi, Davin, Trannoy and Ventelou2015; Ranci and Arlotti, Reference Ranci and Arlotti2019), even though cash-for-care arrangements are a core element of many LTC systems.
This paper contributes to this gap in the literature by exploring the take-up and the distribution of the Austrian LTC allowance. The allowance is a universal cash benefit paid to those in need of LTC reaching a certain minimum level of care needs. The benefit is split into seven levels of care needs and is not means-tested. It is an intermediate provision that is supposed to contribute to covering the costs involved with LTC needs, to facilitate access to LTC services, or to support informal care. This paper analyses whether the take-up and the distribution of this particular benefit reflect needs in terms of age structure and health status of the population. Concerning potential inequalities, the paper studies local variations and analyses whether socio-demographic variables have an impact on inequalities in the take-up and the distribution of LTC allowances. In doing this, the paper adds to the literature in at least three ways. Firstly, while the existing literature on LTC focuses almost exclusively on the distribution of formal and/or informal LTC services (e.g. Albertini and Pavolini, Reference Albertini and Pavolini2017), the focus in this paper is on a universal cash benefit. Secondly, the cash benefit is an intermediary provision. While there is a substitution-complementarity issue for informal care and different kinds of formal services, need is the only principle according to which take-up and level of benefit should vary. The availability and use or non-use of informal or formal care does not impact eligibility for the allowance. Thirdly, the paper can provide novel insights into variations in the take-up of universal cash benefits more generally, as the existing literature on non-take-up largely focuses on means-tested benefits.
2. The care allowance in the Austrian long-term care system
The public LTC system in Austria builds on two main pillars: a universal LTC allowance system (Pflegegeld) and publicly co-funded services provided in institutions and in the community (Österle, Reference Österle, Ranci and Pavolini2013; Trukeschitz et al., Reference Trukeschitz, Österle and Schneider2022). The LTC allowance covers all age groups and is split into seven different levels of care needs, with benefits ranging between € 175.00 in level 1 and € 1,879.50 in level 7 per month as of January 2023. The allowance is not means-tested and is paid to the person in need of care or a legal representative of that person. The specific use of the benefit is not predefined. It can be used to co-pay public services, to pay market services out-of-pocket, but can also be transferred to a family carer or become part of the household income of the user. A declaration of the specific use is not necessary. When moving to a nursing home, the allowance – apart from some pocket money for the resident – is transferred to the respective residential care home as a contribution to covering the nursing home costs.
Access to the LTC allowance is by application, and hence requires the initiative of the person in need of care: the assessment of care needs, detailed in a decree, is then undertaken by a medical doctor during a home visit. In case of a re-assessment, when applying for a higher benefit level, this can also be performed by a nurse. Eligibility requires continuing need for care and support of at least 65 hours per month. The assessment follows a grid for care and support measures that links respective needs with a time value. In case of dementia and for severely disabled children and youth, a flat-rate premium is added. For groups of persons with specific limitations, such as blind persons or in case of paraplegia, a minimum level of care need is defined. In the current LTC debate, the assessment process is not fundamentally questioned, but single cases discussed in the media, statements by advocacy groups or the existence of tools that suggest to ‘optimize’ the outcome in the assessment are indications of potential variability.
Broadly defined coverage (no limitations in terms of age) and the breadth of eligibility in terms of the definition of care needs has led to a take-up rate of more than 5% of the Austrian population. This level stands out in an international comparative perspective (Ranci et al., Reference Ranci, Österle, Arlotti and Parma2019). In terms of generosity, however, it is important to consider the distribution of recipients across the benefit levels. By the end of 2020, almost 50% of recipients were in levels 1 and 2 (28.2% and 21.4% respectively), another third of recipients in benefit levels 3 and 4 (18.5% and 14.6%, respectively), while recipients in benefit levels 5 to seven account for 17.2% of recipients.
In summary, eligibility to the LTC allowance scheme only takes long-term needs (in fact, the time needed to cover certain needs; see above) into consideration. The benefit does not differentiate in terms of age or income. It is independent from the concrete care arrangement and it is not provided as an alternative to informal and/or formal care services. Hence, the distributional aim is to provide an equal cash benefit for equal LTC needs as defined. However, whether this aim is achieved and whether those eligible do in fact take up the benefit was never debated in the national long-term care discourse. Apparently, non-take-up is not assumed to be a problem with a benefit that is well known and long established.
3. A review of the literature
While the roots of studying (in)equalities in LTC can be traced back to the late 20th century, a more coherent research agenda has been emerging only in the past decade (for an overview see Kröger, Reference Kröger2022). Most importantly, a growing body of literature explores the impact of socio-economic factors on the use of LTC services or, more specifically, unmet needs or care poverty. The focus of both multi country and single country studies is not only on informal and/or formal care and on institutional care and/or care provisions in the home of the user, but also on potential substitution between different forms of provision (e.g. Albertini and Pavolini, Reference Albertini and Pavolini2017; Rodrigues et al., Reference Rodrigues, Ilinca and Schmidt2018). Two dimensions, that are most relevant for this study, have so far received less attention in this literature: namely, issues of territorial justice in LTC and the (non-)take-up of long-term care related cash benefits.
Considerations of territorial justice, also captured by the concept of “welfare municipalities”, point at the central role of local governments and potential local variations within welfare states. LTC is a welfare state sector with a strong tradition of local responsibilities and, hence, potentially substantial spatial variation in the use of services. Demaerschalk et al. (Reference Demaerschalk, Vanden Boer, Bronselaer, Molenberghs and Declercq2012), for example, have shown that Flemish older persons with similar care needs and similar individual characteristics can receive very different care depending on the municipality in which they live. In an early study for Sweden, Trydegård and Thorslund (Reference Trydegård and Thorslund2001, p. 183) conclude that variations between municipalities are “a greater threat to the principle of equality in care of the elderly than gender and socio-economic differences.” For Denmark, Jensen and Lolle (Reference Jensen and Lolle2013) report wealth of a municipality, local demographics and privatisation as major explanatory variables for local variations in older care. In a qualitative study, Chaney (Reference Chaney2013), studying the impact of devolution on social welfare for older people in the UK, emphasises that local differences that emerge in quantitative studies might be seen as inequitable in terms of needs orientation, but might also be seen as a reflection of the local autonomy and related differences in local priorities and orientations.
The focus of the above research is mainly on services. So far, there has been little exploration of cash benefits in studying spatial inequalities in LTC, even though cash benefits are a major element of care systems in several countries, such as Austria, England, France, Germany, Italy, or Spain. However, the concrete features of these schemes differ a lot, not least between cash benefits bound or not bound to a specific use, and benefits that are paid as an alternative to formal care services or independently from the concrete use (Gori and Luppi, Reference Gori and Luppi2019). For Spain, García-Gómez et al. (Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015) have compared the use of cash transfers and nursing home services and have shown a pro-rich distribution of cash transfers (and a pro-poor distribution for the use of nursing homes). Arrighi et al. (Reference Arrighi, Davin, Trannoy and Ventelou2015) have studied the French allowance program (APA), managed by 94 county councils. In line with other studies, it shows that those better-off and those living with a partner or a daughter are less likely to apply for support. A key result, however, is that take-up is also linked to the generosity of the scheme. In a recent Italian study, the issue of local discretion is studied in connection with the division of central and local roles in LTC policy (Arlotti et al., Reference Arlotti, Parma and Ranci2021). It suggests that the introduction of the national LTC program led to territorial inequalities in uptake because the poorest and most deprived areas used their local discretion to benefit most from the central government programme. Ranci and Arlotti (Reference Ranci and Arlotti2019) explain high non-take-up rates for a novel home care premium in Italy mainly by cost-benefit considerations and underlying attitudes and practices of those eligible. Different from the LTC allowance studied in this paper, the benefit requires users to have a formal care arrangement, or to formalise an existing informal care arrangement and to follow the regulations that come with the formalisation. Hence, in this Italian case, individual considerations around the care arrangement are shown to be more relevant for non-take-up than e.g. a lack of information.
Beyond LTC, research on the (non-)take-up of cash benefits has largely focused on means-tested benefits, in particular social assistance (e.g. Janssens and Marchal, Reference Janssens and Marchal2022; Kühner and Chou, Reference Kühner and Chou2023; Laín and Julià, Reference Laín and Julià2022; Van Gestel et al., Reference Van Gestel, Goedemé, Janssens, Lefevere and Lemkens2022; van Oorschot, Reference van Oorschot1991, Reference van Oorschot1995). In a recent attempt to advance the conceptualisation of benefit coverage and take-up, Nelson and Nieuwenhuis (Reference Nelson and Nieuwenhuis2021) suggest to differentiate between (i) risk pool (which, in LTC, could be the older or the entire population), (ii) the coverage rate (those that are covered by the respective legislation, e.g. those in a social insurance system), (iii) the eligibility rate (those that are eligible for a certain benefit, e.g. an LTC allowance), and (iv) the take-up rate (referring to those, among the eligible population, that actually get a benefit).
There are two main reasons why eligibility does not lead to take-up. First, those who are potentially eligible may not apply for a benefit, intentionally or unintentionally, because of e.g. a lack of knowledge, language hurdles, individual cost-benefit considerations, hurdles in the process of application, or perceptions about the need and the right to receive a benefit. This is also called primary non-take-up (van Oorschot, Reference van Oorschot1995). Second, an application of an eligible applicant might not lead to a successful claim because the applicant does not complete the application or because of errors, discretion or discrimination that can lead to unequal treatment of cases. This is also called secondary non-take-up (van Oorschot, Reference van Oorschot1995). In fact, discretion or discrimination might not only lead to non-take-up despite being eligible, but could also lead to benefit receipt in cases where criteria are not fulfilled. Finally, non-take-up might be full or partial (e.g. in terms of benefit level), and it can be permanent or temporary (Nelson and Nieuwenhuis, Reference Nelson and Nieuwenhuis2021).
In the literature on whether and why individuals do or do not take up benefits, different approaches are used to classify factors for non-take-up. Laín and Julià (Reference Laín and Julià2022), for example, differentiate between individual and claimant level factors and administrative and institutional level factors. Building on work by van Oorschot (Reference van Oorschot1991), Janssens and Van Mechelen (Reference Janssens and Van Mechelen2022) identify four levels of factors: the client level (benefits, costs, trigger events, network effects and other cognitive and behavioural barriers), the policy design level (benefit type, degree and way of targeting and degree of discretion), the administrative level (information provision, user-friendliness, and internal and external organisation), and finally the broader social and legal context (e.g. the institutional and policy background) impacting the aforementioned levels.
4. Hypotheses
This study explores whether take-up and distribution of the Austrian LTC allowance correspond to needs. The interest of this paper is in the relation between eligibility rate and take-up rate, more specifically whether take-up reflects eligibility. If take-up fully reflects eligibility, local variations in the number of LTC allowance recipients are caused purely by differences in the age structure and health status of the local population (impacting LTC needs). If we identify inequalities in local take-up rates beyond these factors, we argue that they represent primary non-take-up (varying levels of making a claim for the allowance) and/or secondary non-take-up (discretion or discrimination in the drawing of the allowance). Empirically, we cannot directly measure need or factors that lead to primary and secondary non-take-up. Instead, following the literature, we argue that information on education, citizenship, female employment rates and average household size are associated with factors that lead to primary and/or secondary non-take-up, which we explain below in detail.
First, we use the share of residents in a municipality with a university degree. This serves as an indicator for both variations in the health status of the local population and for variations in the take-up rate of LTC allowances. As results of the Austrian health interview survey (ATHIS) indicate, more highly educated people on average have a better subjective health status and suffer less often from chronic diseases (Klimont, Reference Klimont2020). Consequently, we expect a lower number of persons with care needs in municipalities with more highly educated people living there. Additionally, more highly educated people, on average, have a higher income and are wealthier. Accordingly, the receipt of a LTC allowance is of less importance in their cost-benefit considerations (Ranci and Arlotti, Reference Ranci and Arlotti2019), as the LTC allowance accounts for a lower share of income, and out-of-pocket-payments for care are more easily feasible for people with a higher income. Consequently, compared to other persons with a similar health-status a person holding a university degree might apply for LTC allowance less often or at a later stage. Higher average education in a municipality is therefore associated with lower need levels and lower primary take-up.
H1. A higher share of residents with university degree leads to a lower share of LTC allowance recipients in a municipality.
Next, we use the share of foreigners in a municipality. We define a foreigner as a person not holding Austrian citizenship. This variable also serves as an indicator both for variations in the health status and for variations in take-up rates. It is interesting to note that on average persons not holding Austrian-citizenship are younger than persons with Austrian citizenship. In fact, 22 per cent of all Austrian citizens are older than 64 years compared to only 7 per cent of persons with non-Austrian citizenship (Statistik Austria, 2023). On average, persons with non-Austrian citizenship more often report good or very good subjective health and they suffer less often from chronic diseases compared to Austrian citizens (Klimont, Reference Klimont2020). However, these rates differ depending on the migration background: only people from EU/EFTA countries more often report good or very good subjective health compared to Austrians, whereas this share is actually lower for people from Bosnia and Herzegovina, Serbia and Turkey compared to Austrians, even though their average age is below Austrians’ average age. These three population groups represent by far the largest populations from non-EU countries in Austria. For people from other countries (rest of world – ROW) the share of persons reporting good or very good subjective health is higher compared to Austrians.
Additionally, we suppose that foreigners who are in need of care more often do not take-up LTC allowance because of a lack of information about the existence of the benefit, the complexity of the application procedures or because language barriers impede take-up. Finally, the same language barriers or simply discrimination could lead to differences in the assessment of care needs by doctors who are responsible for assessing them. All three factors should lead to a lower share of LTC allowance recipients among foreigners. Hence, the implications of the migration background are rather ambiguous. A better health status of residents from EU/EFTA as well as from ROW countries would lead to an expected lower level of allowance recipients, but the comparatively worse health status of persons from Bosnia and Herzegovina, Serbia, and Turkey would lead to a larger level. For foreigners, except persons from EU/EFTA countries (with the largest group originating from Germany), language and cultural barriers might cause a larger hurdle and hence lead to a lower uptake of the benefit. Summing up, the share of foreigners in a municipality is associated with differences in need, with primary non-take-up (lack of information, language barriers) and secondary non-take-up (language barriers in the assessment process, discretion or discrimination by doctors).
H2a. A higher share of foreigners from EU/EFTA and ROW countries in a municipality leads to a lower share of LTC allowance recipients.
H2b. A higher share of foreigners from Bosnia and Herzegovina, Serbia as well as Turkey in a municipality leads to either a higher or lower share of LTC allowance recipients.
Building on the results in Arrighi et al. (Reference Arrighi, Davin, Trannoy and Ventelou2015), we use two variables – the female employment rate and average household size – as indicators for an informal care potential. If fewer informal caregivers are available, external care may be sought at an earlier stage of dependency. Accordingly, persons with a care need may apply for LTC allowance more quickly if no informal carer is available. This could be the case for older people living alone or in situations where family members are in employment. Both measures serve as indicators for primary non-take-up, mostly reflecting perceptions about need for support.
H3. A higher female employment rate and a lower average household size in a municipality are associated with a higher share of LTC allowance recipients.
Finally, we expect local variations in non-take-up and in the distribution of allowances to be higher for lower care levels. In this case, not only are benefits smaller (hence, lowering the cost-benefit incentive to go through the application process), but it is also largely left to the individual in need of care or close family members, and potentially to the GP, to know and to decide whether a step is to be taken to apply for the LTC allowance. This involves several aspects that have been discussed in the literature (Janssens and Van Mechelen, Reference Janssens and Van Mechelen2022; van Oorschot, Reference van Oorschot1995), including the self-perceived need for financial support or the perceived right to receive support, the availability of information and the ability to take the necessary steps. In case of more severe care needs, either as a result of progressing chronic illness or as a result of a sudden ill health event, it is more likely that contacts with the professional system support or even require the process of application. Eligibility for a place in a nursing home, for example, usually requires a minimum level of care needs, most commonly level 3 or 4. In these cases, the person in need of care or family members are more strongly driven to initiate a (re-)assessment of care needs. The fact that contact to or advice by the professional system helps in the process of benefit application and receipt is generally known from other social benefits, in particular social assistance (e.g. Fuchs et al., Reference Fuchs, Gasior, Premrov, Hollan and Scoppetta2020). Hence, the probability of applying for and receiving LTC allowance rises with higher levels of care need regardless of the personal circumstances of an individual person, while socio-demographic inequalities are potentially more pronounced for benefit levels 1 and 2.
H4. The impact of socio-demographic factors on an unequal distribution of LTC allowances on the municipal level is more pronounced for benefit levels 1 and 2.
5. Data and methods
We combine three data sources for the analyses. The first data set comprises information on the number of LTC allowance recipients for each care level in each Austrian municipality for the years 2013 to 2020. These administrative data were provided by the Austrian Ministry of Social Affairs, Health, Care and Consumer Protection. The second data set contains information on the socio-demographic structure of the population on a municipal level for the years 2013 to 2020. This data set includes the number of persons aged 75 and older, the average age of the population, the average household size, the female employment rates, the share of residents with a university degree and the share of foreigners, i.e. persons not holding Austrian citizenship, in a municipality. The information was retrieved from the statistical atlas provided by the Austrian statistical office (Statistik Austria, 2022). The third data set contains information about the health status of the population. More precisely, we use results from ATHIS 2014 and 2019. For these data, the smallest level of regional disaggregation is roughly equivalent to the NUTS 3 level.
The information on the number of LTC allowance recipients was initially provided on the basis of postal codes. In order to be able to merge this information with information on the socio-demographic structure of a municipality, we converted the variable from a postal code level to a municipal level (see Pennerstorfer, Reference Pennerstorfer2021). The unit of observation in our data set is the municipality. In total, we use information on the number of adult LTC allowance recipients in all 2117 Austrian municipalities for the years 2013 to 2020. Overall, 28.4% of all residents 75+ receive LTC allowance with care level 1 or 2, and 18.0% of all residents 75+ receive LTC allowance with care levels 4 to 7. Although payment of LTC allowance is not restricted to residents 75+, we use this population because this is the group with the highest incidence of LTC (BMSGPK, 2021). As a result, the proportions become larger in absolute terms, but results would be qualitatively similar if the shares were calculated based on the whole population.
In order to test the hypotheses, we first estimate two models using fixed-effects regressions for the years 2013 to 2020. As dependent variables, we use the share of LTC allowance recipients with care level 1 or 2 over the residential population aged 75 years and older (model 1) and the share of LTC allowance recipients with care levels 4 to 7 over the residential population aged 75 and older (model 2). We focus on levels 1 and 2 in model 1 and on levels 4 to 7 in model 2, to differentiate between groups of beneficiaries that are either less or more likely to already be in contact with social service providers and, hence, the latter becoming or not becoming an agent for application. In level 3, cases in which those in need of care or close family members initiate an application and cases in which this process is supported or even initiated by the system, are more mixed. Therefore, level 3 is excluded from the analysis. By separating the levels of care need, we are able to test hypothesis 4, which examines whether potential relationships between socio-demographic variables and the local variation of LTC allowance recipients differ between lower and higher levels of care need.
Estimating fixed-effects regressions has the advantage to control for all time-constant variance between municipalities, which could explain the dependent variable. One such example is the question whether a care home is located in a municipality. In such a case, the share of LTC allowance recipients in such a municipality is higher, but controlled for as a fixed-effect. Importantly, regional variation of the local population’s average health status is also controlled for with a municipality-fixed effect, as long as this variation is relatively stable over time. The coefficients thus represent the effect on the share of LTC allowance recipients over the residential population aged 75 years and older when the socio-demographic structure of the population within a municipality changes over time. Apart from the variables of interest, which are the share of persons with a university degree in a municipality, the shares of foreigners, the female employment rate and the average household size – we include the average age of the residents in the municipality as well as year-fixed-effects as control variables.
Since data on regional variations of the health status of the population is available only for two years – 2014 and 2019 – we cannot add subjective health as an independent variable to the fixed-effects model. Instead, in a second step we estimate pooled cross-section OLS regressions for those two years that include the average subjective health of the population 75+ in a ‘provision region’ (Versorgungsregion). The Austrian health system is divided into 32 such provision regions, which are roughly equivalent to the NUTS 3 level. The addition of the average subjective health on a regional level as an independent variable helps separating between the three factors that explain local variations of levels of LTC allowance recipients. This way we can (partly) separate variations in care needs from varying application rates or discretion in the assessment of needs by doctors. We opted for subjective health in the main specification because we think that a person may become active in applying for the LTC allowance if s/he subjectively feels not to be in a good health status.
As in the fixed-effects models, the share of LTC allowance recipients with care level 1 or 2 over the residential population aged 75 years and older (models 3 and 4) and the share of LTC allowance recipients with care levels 4 to 7 over the residential population aged 75 and older (models 5 and 6) serve as dependent variables. In addition to the independent variables that are included in the fixed- effects models we include a variable that indicates average subjective health in a provision region, a dummy variable representing whether a care home is located in the municipality, and a variable on the urban-rural classification of a municipality. In ATHIS, subjective health is measured on a scale ranging from 1 ‘very good’ to 5 ‘very bad’. We calculated the mean values for this variable for the population aged 75 years or older for each provision region and used these averages to capture variation in the health status of the population 75+ in Austria for the OLS regressions. The dummy variable which indicates whether a care home is located in the municipality is necessary because municipalities with care homes naturally have higher shares of LTC allowance recipients compared to municipalities without one. The variable on the urban-rural typology, provided by Statistik Austria (2022), includes eleven categories with higher values indicating a more rural area. We add this variable as a control variable because data on informal care in Austria have shown variation between rural and urban settings (Nagl-Cupal et al., Reference Nagl-Cupal, Kolland, Zartler, Mayer, Bittner, Koller and Stöhr2018). The OLS regressions are estimated with clustered standard errors on the regional level of a ‘provision region’. Tables A1 (Fixed-effects regressions) and A2 (Pooled cross-section regressions) in the Online Appendix display summary statistics of the sample.
6. Results
Table 1 presents the results of the fixed-effects models. The dependent variable in model 1 is the share of LTC allowance recipients with care level 1 and 2, while model 2 displays the results for higher care levels (levels 4 to 7). Turning to the results of model 1 first, we find that a higher share of residents with a university degree and a higher share of residents from EU/EFTA countries as well as from ROW countries among the residents are associated with a lower share of LTC allowance recipients as hypothesized in H1 and H2a. The coefficient for the share of residents from Turkey, Serbia and Bosnia and Herzegovina is negative, indicating that primary and/or secondary non-take-up seem to prevail over the worse average health status. While the coefficient for the female employment rate is not statistically significant, we find that a higher average household size in a municipality is associated with a lower share of LTC allowance recipients, which is in line with H3. A higher average age of residents in a municipality leads to relatively fewer LTC allowance recipients with low levels of care need.
TABLE 1. Results of fixed-effects regressions
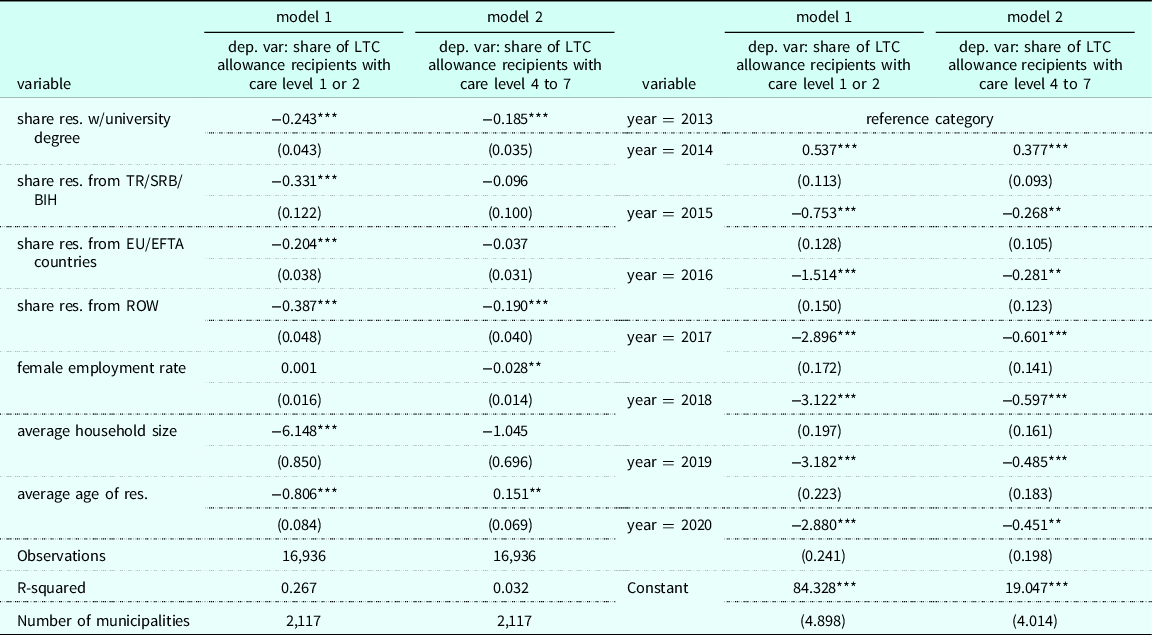
Notes: Standard errors in parentheses; *** p<0.01, ** p<0.05, * p<0.1
Overall, model 2 reveals fewer statistically significant results, as hypothesized in H4. Additionally, many coefficients are of lower substantial size, which is also in line with H4. The socio-demographic structure of the population on a municipal level is of less relevance in terms of explaining variations in the share of LTC allowance recipients with higher care needs. The coefficient for the share of residents with a university degree is lower compared to model 1. Similarly, the effect for the share of residents with a ROW nationality is much lower in model 2. The coefficients of the share of residents with an EU or EFTA nationality or a Turkey, Serbia or Bosnia and Herzegovina nationality are statistically insignificant in model 2. In contrast to our expectations, a higher female employment rate in a municipality is associated with a lower share of LTC allowance recipients with care levels 4 to 7. The coefficient for the average household size is statistically not significant. Unsurprisingly, as the average age of the residents in a municipality increases, we find a higher share of persons with high care needs.
Table 2 presents the results for the pooled OLS regressions. Models 3 and 4 show the results with the share of LTC allowance recipients with care level 1 or 2 as a dependent variable, while models 5 and 6 display results for higher care levels (4 to 7). Models 3 and 5 include the average subjective health variable as an independent variable, while models 4 and 6 do not. This way, we can evaluate how results change once we control for regional variations in subjective health.
TABLE 2. Results of the pooled OLS regressions
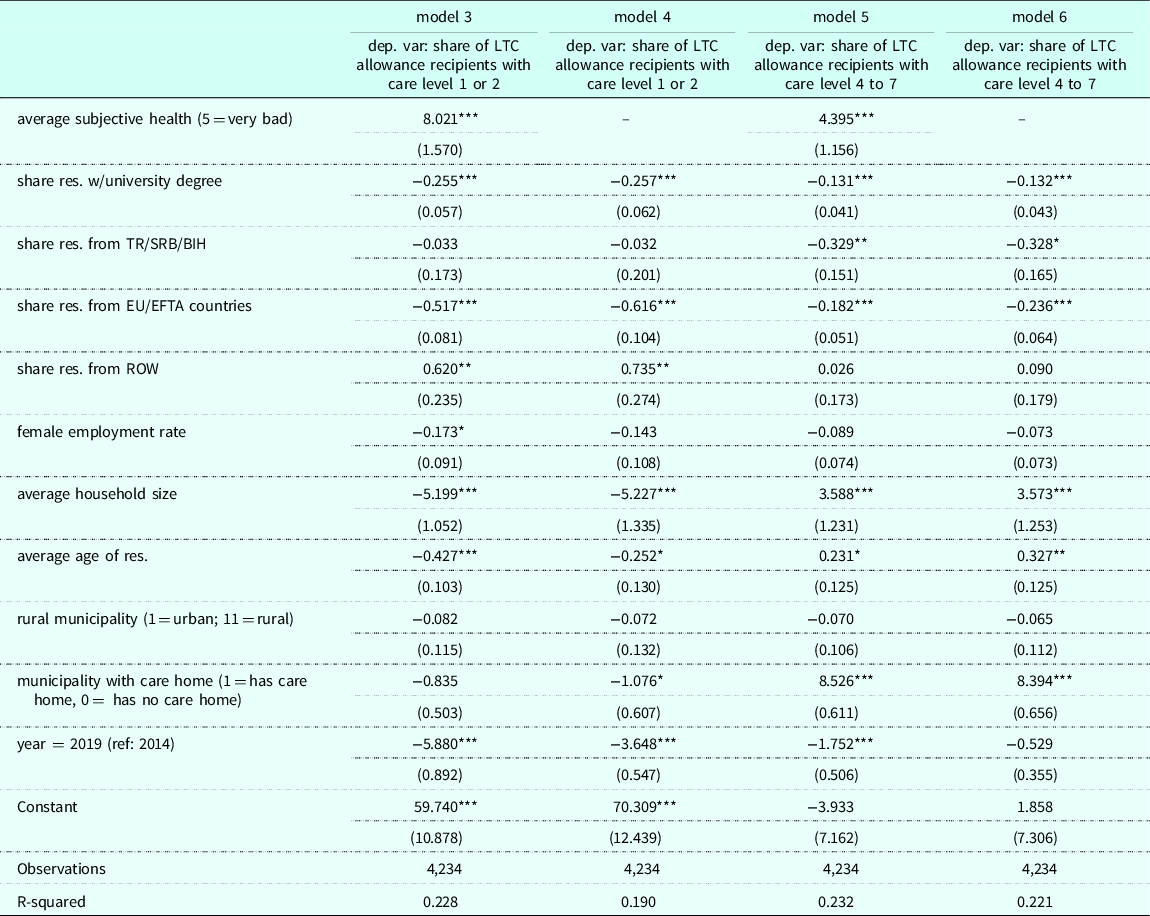
Robust standard errors in parentheses; *** p<0.01, ** p<0.05, * p<0.1
Unsurprisingly, worse average subjective health in a region is associated with a higher share of LTC allowance recipients for all care levels. Turning to the independent variables that were also part of the fixed-regressions, we find that by and large many results are similar. Our main interest in this table, however, lies in the comparison between the models with the subjective health variable as an independent variable and those without. Comparing model 3 to model 4, as well as model 5 to model 6, we find no large differences. The coefficients of the variables of interest remain relatively stable once the regional average subjective health variable is included in the model. This variable partly controls for regional differences in subjective health and consequently differences in care need. Thus, the residual effect of the socio-demographic variables can rather be attributed to the other two reasons for a local variation in the share of LTC allowance recipients: primary or secondary non-take-up.
Additionally, we performed a number of robustness checks. To this end, we altered both dependent and independent variables. Table A3 in the Online Appendix displays results for the fixed-effects regressions with alternative dependent variables. Models 7 and 8 in this table use the share of LTC allowance recipients over the population 70 years or older instead of using that of the population 75 years or older in the denominator; model 9 additionally includes care level 3 instead of using care levels 1 and 2 only. As expected, the results for models 7 and 8 are very similar to the main specification, but the coefficients are smaller in absolute values due to the lower shares resulting from the larger population size on which the share is based. The results in model 9, which are estimated with a dependent variable that includes care level 3 in the calculation of the share of LTC allowance recipients, barely differ from the main specification.
Table A4 in the Online Appendix displays results of the fixed-effects regression with varying independent variables. Instead of the share of residents with a university degree in a municipality, we use the average pension level as an indicator for socio-economic status. Next, the foreigner share was measured with only two variables instead of three, differentiating between EU/EFTA nationals and persons from ROW countries (including persons from Turkey, Serbia and Bosnia and Herzegovina). The share of single households in a municipality was used as an alternative to the average household size. The results for this specification differ from the main specification in two ways: the coefficients for both the average pension level and the share of single households are not statistically significant. We argue that education is a better indicator for the socio-economic status of the residents of a municipality than pensions because the latter fail to account for differences in living costs and wealth.
Finally, we used alternative variables for the pooled cross-section model (see Table A5). Instead of average subjective health, a variable containing the mean agreement to five questions concerning activities of daily living (ADLs) in ATHIS was included, whereby value 1 indicates having no difficulties performing a task and value 4 not being able to perform the task. Instead of the dummy variable that specifies whether a care home is located in the municipality, the number of care beds in a municipality was used. Again, the results barely differ from the main specification. Summing up all robustness checks, we find that the regression results are hardly affected by the modifications, strengthening our confidence in the main findings.
7. Discussion and Conclusion
This paper argued that three factors can help explain local variations in the take-up and distribution of LTC allowances: the varying health status of the residents and consequently their varying care needs, differences in making or not making an application (primary non-take-up) and discrepancies in the process of awarding a benefit in case of similar care needs (secondary non-take-up). By estimating fixed-effects regressions and by including the regional average subjective health status in the OLS regressions, we can partly rule out differences in the distribution of care needs as the reasons for the local differences in the shares of LTC allowance recipients. An unequal distribution of LTC allowances in municipalities changed very little when a health status variable was added. Consequently, we emphasize the importance of primary non-take-up as well as discretion and discrimination in the assessment of care needs to explain local variations in the distribution of LTC allowances.
In terms of socio-demographic factors impacting the take-up and distribution of LTC allowances, most of our hypotheses are confirmed. A higher share of residents with a university degree is associated with a lower share of LTC allowance recipients. Similarly, more residents from EU/EFTA in a municipality are also associated with a lower share of LTC allowance recipients, as hypothesized. The effect for ROW residents differs between the fixed-effects and pooled OLS regressions. This may be explained by the fact that the pooled OLS regression takes variation between municipalities into account, while the fixed effects regression analyses effects over time. As the group of ROW residents is quite heterogeneous and concentrated in larger cities, the variable picks up a ‘big city’ effect in the pooled OLS regression.
The remaining hypothesis on the impact of migration backgrounds is rather ambiguous as discussed before. A higher share of foreigners from Bosnia and Herzegovina, as well as Serbia and Turkey, did not lead to a higher share of recipients although their health status is on average worse compared to that of the Austrian population (Klimont, Reference Klimont2020). Since this did not lead to a higher take-up, this is an indication of the importance of primary and/or secondary non-take-up. A lower average household size is associated with a higher share of LTC allowance recipients with care level 1 and 2, which is in line with our expectations. Finally, the overall impact of these factors is stronger for benefit levels 1 and 2 as hypothesized. Coefficients on the female employment rate were, in contrast to our expectations, either not statistically significant or had a negative sign. We argued that female employment rates were an indicator for the informal care potential and thus expected a positive relationship between the share of LTC allowance recipients and female employment rates. However, the relation might be reversed. If need for informal care is low in a municipality, we observe higher female employment.
Of course, there are limitations to our research. First of all, a more detailed health variable could strengthen the analysis. In this analysis, average subjective health is measured only for two years and on a regional rather than municipal level. Ideally, we would need such a variable also on the municipal level and for more years in order to be able to distinguish more clearly between differences in need and non-take-up or discrimination-related assessment of needs. Second, the current data do not allow to clearly differentiate between primary and secondary non-take-up. Information about applications on the municipal level and about determinants for not granting a benefit, as well as qualitative research into individual and structural factors in the process, could contribute to our understanding about which mechanisms contribute to the local variation in the share of LTC allowance recipients. Finally, it is important to note that we use data that are aggregated on a municipal level. Those receiving LTC allowance are not necessarily in the group that has, for instance, a university degree or is from a foreign country. Ideally, we would need individual-level data.
Research on inequalities in LTC has largely focused on unmet needs and the use or non-use of formal and informal care. This particular LTC allowance is different, as it is linked to care needs rather than a specific use of the benefit. Hence, non-take-up does not necessarily imply care poverty. Rather, parts of the population do not use a benefit intended to support individuals in need of care and their family members in covering costs related to LTC. The principle underlying the LTC allowance benefit – namely, providing equal benefits for equal need – is not achieved. Although the LTC allowance is designed as a nationwide policy, surprisingly, we find substantial local variation in its distribution across Austrian municipalities that cannot be explained by variations of the age structure or the health status. Instead, other local demographics can help explain local variations. Different levels of primary and secondary non-take-up among certain groups of residents are an important explanation for these findings.
This research does not allow to clearly disentangle to what extent inequalities are due to not making an application or due to discretion and potential discrimination in the process. Non-take-up is supposed to be related to all four levels of factors as explicated by Janssens and Van Mechelen (Reference Janssens and Van Mechelen2022) – the client level, the policy design level, the administrative level and the broader social and legal context. Drawing policy conclusions will require further research to investigate the relative importance of primary and secondary non-take-up and the relative role of the various factors on the aforementioned four levels. The results, however, already indicate that improving information targeted at specific populations as well as early contacts with key actors in health and social care (in particular doctors and community nurses) are major tools to reduce non-take-up. Similarly, recent studies on non-take-up of means-tested benefits emphasize the importance of pro-actively contacting (Van Gestel et al., Reference Van Gestel, Goedemé, Janssens, Lefevere and Lemkens2022) and personally informing and counselling potential claimants (Laín and Julià, Reference Laín and Julià2022). In the Austrian LTC context, community nursing, initiated in 2021, has potential in this respect. It is an explicit aim of the program to support older people in health and care related issues, to emphasize prevention and health literacy, and to provide information, support and consultancy even before long-term care needs emerge (Gesundheit Österreich GmbH, 2023).
In terms of generalizability of the results, three aspects are important: the role of cash benefits in exploring inequalities in LTC, the role of cash benefits as intermediary support measures, and more generally the study of take-up in universal cash benefits. Previous studies on inequalities in LTC have rarely covered LTC allowances, and even less so cash benefits that are not linked to a specific use. In the latter case, the impact of cash benefits on unmet care needs is of an indirect nature: cash benefits are a major source for covering care-related costs, they can provide symbolic payments for informal carers or be used for co-paying public services or buying services in the market. Additionally, cash benefits can also help establish or incentivize contact between the individual and the LTC system. Significant rates of non-take-up among those with minor LTC needs also lower the chance to make use of other support schemes. Beyond LTC policies, the study contributes to the broader non-take-up literature, which predominantly focuses on means-tested benefits. This analysis observes substantial inequalities in take-up for a universal cash benefit, a benefit that seems well known and simple to understand. This suggests that factors known for causing non-take-up of means-tested cash benefits also work in this case.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0047279423000375
Acknowledgements
The authors would like to thank Sophie Guthmuller and conference participants of 2022 ESPAnet Research Conference for helpful comments on earlier versions of this manuscript. We also thank the Federal Ministry for Social Affairs, Health, Care and Consumer Protection and the Austrian Federation of Social Insurances for providing data. The research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Competing interests
The authors declare none.





 Open access
Open access