


Introduction
It is well known that, even in individuals who show healthy aging, cognitive and emotional abilities such as executive functions and emotional intelligence are negatively affected by age, showing an inverse-U-shaped pattern (Bisiacchi et al., Reference Bisiacchi, Borella, Bergamaschi, Carretti and Mondini2008; Cabello et al., Reference Cabello, Sorrel, Fernández-Pinto, Extremera and Fernández-Berrocal2016). The decline in these abilities is related to the cognitive reserve (CR) concept (Chapko et al., Reference Chapko, McCormack, Black, Staff and Murray2018). CR is a multifaceted construct that refers to the cognitive differences between individuals of the same age that help to fight against brain damage or normal cognitive decline. This concept is used to explain the gap observed between the degree to which a brain is damaged and the visible consequences of such damage. CR relies on both passive and active components (Stern, Reference Stern2009), with the former being related to brain characteristics while the latter refers to the use of cognitive abilities that compensate for the aging process. Given the multifaceted characteristic of the CR concept, it is not easy to find adequate measures for its operationalization. In order to fully capture its components, brain and cognitive measures have been employed. Although the inclusion of brain measures is recommended (Jones et al., Reference Jones, Manly, Glymour, Rentz, Jefferson and Stern2011), cognitive measures have been more thoroughly and frequently used. These include educational level or intelligence, among others (Valenzuela and Sachdev, Reference Valenzuela and Sachdev2006). Previous studies have shown that this active component of the CR, measured through educational level, is a protective factor for cognitive decline (Cabello et al., Reference Cabello, Navarro Bravo, Latorre and Fernández-Berrocal2014; Chapko et al., Reference Chapko, McCormack, Black, Staff and Murray2018; Mohammad et al., Reference Mohammad2020; Neuropathology Group MRC CFAS, 2001; Radanovic, Reference Radanovic2020; Ritchie and Tucker-Drob, Reference Ritchie and Tucker-Drob2018). For instance, Cabello et al. (Reference Cabello, Navarro Bravo, Latorre and Fernández-Berrocal2014) found no differences in emotional intelligence (measured through a performance-based test) between older and younger adults with a university education, while for adults with a primary or secondary education, higher scores were obtained by the younger participants in comparison with the older adults.
Another variable that integrates emotional and cognitive processes and is also sensitive to age is the Theory of Mind (ToM). ToM allows individuals to attribute mental states to others in order to predict their behaviors and act accordingly (Baron-Cohen and Chakrabart, Reference Baron-Cohen, Chakrabart, Baron-Cohen, Tager-Flusberg and Lombardo2013). This ability can be divided into the components of cognitive and emotional empathy. While cognitive empathy refers to the ability to recognize the thoughts or feeling of others, emotional empathy is the drive to appropriately respond to this mental state. Cognitive empathy has been shown to be of importance in a variety of psychological disorders. For instance, deficits in cognitive empathy appear in schizophrenia (De Achával et al., Reference De Achával2010), autism (Baron-Cohen et al., Reference Baron-Cohen2015), social anxiety (Machado-de-Sousa et al., Reference Machado-de-Sousa2010), and dementia (Schroeter et al., Reference Schroeter2018), among others.
Given the complexity of the construct, there are various instruments for measuring cognitive empathy, which focus on its various components. These are based on either self-report, where individuals subjectively estimate their own ability, or performance-based methodologies, where participants have to objectively solve problems by choosing between a set of correct and incorrect response alternatives. A well-validated performance-based test is the “Reading the mind in the Eyes” test (Eyes test) (Baron-Cohen et al., Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb2001; Fernández-abascal et al., Reference Fernández-Abascal, Cabello, Fernández-Berrocal and Baron-Cohen2013). This instrument focuses on evaluating basic and complex mental states by observing the eyes of others (Megías-Robles et al., Reference Megías-Robles, Gutiérrez-Cobo, Cabello, Gómez-Leal, Baron-Cohen and Fernández-Berrocal2020). Specifically, the participant is required to choose one of four words that best fits with each eye image.
Previous studies have shown how cognitive empathy also varies as a consequence of age, since older people (usually older than 64 years) obtain lower scores on cognitive empathy in comparison with younger people (with age ranges between 17 to 56 years) when using performance tests (Beadle, and De la Vega, Reference Beadle and De la Vega2019; Fischer et al., Reference Fischer, Rourke and Thornton2017; Henry et al., Reference Henry, Philips, Ruffman and Bailey2013; Warrier et al., Reference Warrier2018). Nonetheless, these differences may disappear when the older and younger groups are matched in terms of educational level (both with a higher education level) or other cognitive variables (Duval et al., Reference Duval, Piolino, Bejanin, Eustache and Desgranges2011; Li et al., Reference Li, Wang, Wang, Tao, Xie and Cheng2012), suggesting that educational level and cognitive ability may mitigate the effect of brain aging on cognitive empathy. In addition to the age differences, there is also evidence of gender differences with woman scoring higher than men on cognitive empathy (Warrier et al., Reference Warrier2018). While the previous literature provides us with a starting point for understanding the role of educational level as an active component of the CR in cognitive empathy performance, the existing studies have a number of limitations. For instance, discontinuous samples have often been employed, while there has also been a lack of nonlinear analyses. In order to address this latter limitation, Labouvie-Vief (Reference Labouvie-Vief2009) proposed that the cognitive empathy and age relationship would exhibit an inverted-U-shaped curve, which was later confirmed by O’Brien et al. (Reference O’Brien, Konrath, Grühn and Hagen2013) using self-report instruments. In this latter study, empathy peaked at around 50–60 years of age.
The present study attempts to overcome these limitations through three main objectives. Firstly, we aimed to analyze the effect of age, gender, and educational level on cognitive empathy using the Eyes test, that is, a performance-based test. Secondly, we wanted to ascertain whether the relationship between age and cognitive empathy is linear or quadratic. Our final objective was to examine the moderator role of educational level in the relationship between age and cognitive empathy. On the basis of the findings reported in previous studies, we proposed the following hypotheses:
H1. Women will score higher than men on the Eyes test.
H2. Adults with a higher educational level will score higher on the Eyes test.
H3. Younger and older adults will show lower scores on the Eyes test than middle-age adults, resulting in an inverted-U shaped curve when the scores are plotted as a function of the adult life span.
H4. The age-related decrease on Eyes test scores will be more pronounced in adults with a lower educational level.
Method
Participants and procedure
Our sample was composed of 902 Spanish adults aged between 18 and 79 years (M = 43.53, SD = 11.86), of whom 57.6% were women. With respect to education level, 2.5% of the participants had completed primary-level studies, 10.8% high school, and 86.8% reported having completed a college education. The sample was invited to participate in the test through various social networking and informal advertising channels. None of the participants received financial or other compensation for taking part in the study. They were told that they would receive feedback regarding their scores. The study was carried out in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of the University of Malaga.
Measures
Participants completed the Spanish adaptation of the “Reading the Mind in the Eyes” test (Eyes test; Baron-Cohen et al., Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb2001; Fernández-Abascal et al., Reference Fernández-Abascal, Cabello, Fernández-Berrocal and Baron-Cohen2013). This test includes 36 photographs of male and female eyes depicting emotional states. For each photograph, participants are asked to choose the emotional state that best describes the eyes, choosing between one of four possible emotions. One point is assigned for each correct response, giving a maximum total correct score of 36. In order to avoid task comprehension problems, the participants were provided with an example item to practice with before beginning the task. The Spanish version of the Eyes test shows adequate psychometric properties, similar to those obtained for the original instrument (Fernández-Abascal et al., Reference Fernández-Abascal, Cabello, Fernández-Berrocal and Baron-Cohen2013).
Additionally, sociodemographic information (sex, age, and educational level) was collected using three self-report questions. Education level referred to the level of schooling and was categorized into three groups: primary studies, high school, and college education.
Statistical analysis
All analyses were carried out using SPSS 24 (IBM, Chicago, IL, USA). To test for gender and educational level effects on the Eyes test scores, we conducted a Student’s t test for independent samples and a one-way ANOVA, respectively. Given the relatively large sample size, we reported not only p-values but also Cohen’s d to assess effect sizes (Cohen, Reference Cohen1992). To identify significant effects of age, gender, and educational level (controlling for each of the others) on the Eyes test scores, we created a hierarchical linear multiple regression model. We also included a quadratic term for age in order to test our hypothesis that younger and older adults would achieve lower scores on the Eyes test when compared with middle-aged adults (inverted-U-shaped curve). We conducted the regression in a hierarchical way, first entering gender (Step 1), followed by both age and age-squared (Step 2), and in the third step we entered educational level. In the fourth step, we tested whether there was a significant interaction between age and educational level and between age-squared and educational level by including these interaction terms in the final regression model. Furthermore, the Johnson–Neyman technique (Hayes, Reference Hayes2018) was used to calculate the critical value above which this interaction effect was statistically significant. Finally, we studied the change in the proportion of explained variance (R2) and the relative importance of each variable in the model using squared semi-partial correlation analysis.
Results
Table 1 displays the descriptive statistics and results of the Student’s t test and one-way ANOVA. The mean scores for the Eyes test were significantly higher for women than for men, with a small effect size. The one-way ANOVA revealed a significant main effect of education level for scores on the Eyes test, with a medium effect size. Post hoc analyses revealed significant differences between primary studies and college education (p < .0001), and between high school and college education (p < .0001), with college-educated participants obtaining the highest Eyes test scores. Differences between the scores of primary and high-school-educated participants were not significant (p = .06). These results are consistent with our Hypothesis H1 and H2. Supplementary control analysis revealed that the educational level of men and women was similar in our sample, with no significant differences (t = 1,51; p > .10). In addition, no significant interaction was found between gender and educational level for the Eyes test scores (F(2, 886) = .028; p = .97).
Table 1. Descriptive statistics showing gender- and educational-level differences in scores on the Eyes test

*p-value < .05; **p-value < .01.
The results of the final hierarchical regression model are reported in Table 2. In the first step, gender was a significant predictor, indicating that women showed higher scores than men (F(1, 900) = 11.345; p < .001; adjusted ΔR2 = .011, Beta = .12). These findings are in accord with the results for the Eyes test displayed in Table 1 and support our Hypothesis H1. In the second step, we entered the variables age and age-squared, increasing the variance explained (F(2, 898) = 29.032; p < .001; ΔR2 = .066), with younger people showing higher scores on the Eyes test than older people. These results are consistent with our Hypothesis H3 (Figure 1) and indicate that the age at which peak performance is achieved on the Eyes test is 30.5 years. In the third step, we entered the variable educational level. Educational level exerted a significant linear effect, over and above the effects of gender and age, so that participants with a higher educational level showed higher scores on the Eyes test than those with a lower education level (F(1, 897) = 46.060; p < .001; adjusted ΔR2 = .045, Beta = .22), in agreement with the results on the Eyes test shown in Table 1 and providing support for our Hypothesis H2. In the fourth step, we tested the interaction between age and educational level, and between age-squared and educational level by including these variables in the final model (F(2, 895) = 3.256; p < .05; ΔR2 = .006). Only the interaction effect between age and educational level was significant (Beta = .68, p = .012). In addition, the Johnson–Neyman technique showed that 34.84 years was the critical value above which this interaction effect was statistically significant (t = 1.96, p < .05, CI [0.00–2.00]). This implies that the age-related decrease in the Eyes test score is more pronounced among adults with primary and high school education (supporting our Hypothesis H4), but only when they are over 35 years of age (Figure 2).
Table 2. Regression analysis for Eyes test scores and gender, age, and educational level: final model

*p-value < .05; **p-value < .01.

Figure 1. Estimated age trajectory of scores on the Eyes test, using unstandardized predicted values.
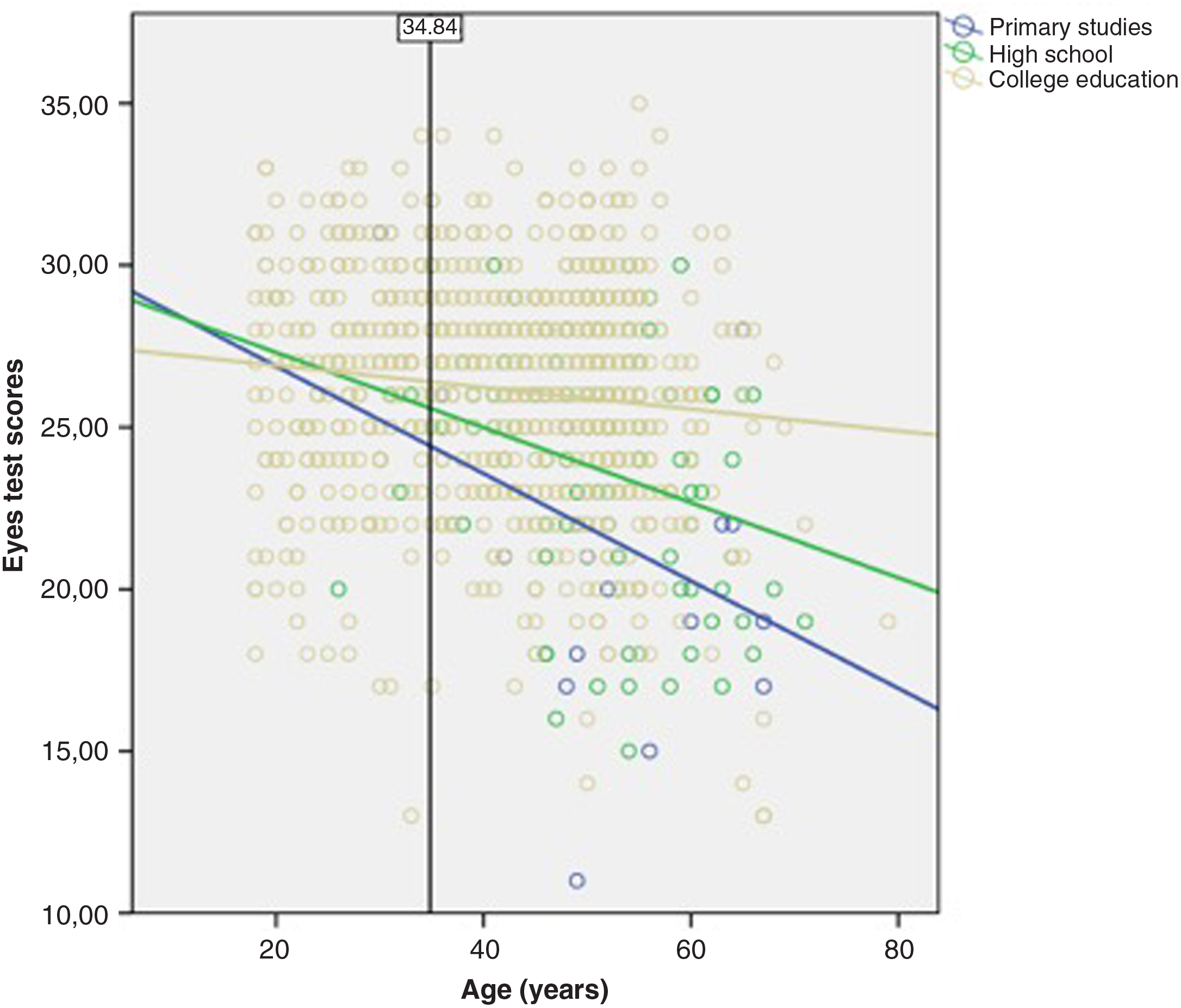
Figure 2. The interaction effect of age and educational level in Eyes test scores. The critical value (34.84 years) after which this interaction effect was statistically significant was calculated using the Johnson–Neyman technique.
Zero-order and semi-partial correlations are shown in Table 2. This analysis revealed that educational level is the most important predictor of the Eyes test score.
Discussion
The present study aimed to analyze the pattern of changes in cognitive empathy across the age span as a function of CR measured through the participant’s educational level (primary, high school, or college education). For this purpose, various statistical analyses were carried out to explore the effect of educational level, together with gender and age, on cognitive empathy in a sample covering a large range of adult ages (18 to 79 years).
Consistent with our Hypothesis H1, preliminary analyses revealed that the women in our sample scored higher on the Eyes test than men, although with a small effect size. This result is also in accord with previous studies where women appear to show a greater ability on cognitive empathy (Warrier et al., Reference Warrier2018). In addition, Hypothesis H2 is also supported, since participants with a higher educational level achieved higher scores on the Eyes test than those with a lower educational level. Specifically, participants with a college education obtained significantly higher scores on cognitive empathy than those educated to primary or high school level, which is consistent with previous studies that measured other cognitive variables (Cabello et al., Reference Cabello, Navarro Bravo, Latorre and Fernández-Berrocal2014; Chapko et al., Reference Chapko, McCormack, Black, Staff and Murray2018; Mohammad et al., Reference Mohammad2020; Neuropathology Group MRC CFAS, 2001; Radanovic, Reference Radanovic2020; Ritchie and Tucker-Drob, Reference Ritchie and Tucker-Drob2018).
Looking further at the data, the results of our regression analysis provided support for Hypothesis H3. This analysis revealed that the relationship between age and scores on the Eyes test fits an inverted-U curve pattern and indicates that the age at which peak performance is achieved is 30.5 years. Our findings are consistent with those of previous studies that have evaluated cognitive empathy with self-report instruments (O’Brien et al., Reference O’Brien, Konrath, Grühn and Hagen2013) and other variables (Bisiacchi et al., Reference Bisiacchi, Borella, Bergamaschi, Carretti and Mondini2008; Cabello et al., Reference Cabello, Sorrel, Fernández-Pinto, Extremera and Fernández-Berrocal2016). In addition, this analysis revealed that educational level was the best predictor of cognitive empathy above and beyond the age and gender variables. In particular, and again consistent with Hypothesis H2, superior scores on the Eyes test were found for the participants with a college education.
Finally—and of particular importance for the purposes of the present study—the results revealed a significant interaction between age and educational level, indicating that the age-related decrease in cognitive empathy seems to be mitigated in those individuals with a higher educational level, which is also in line with the findings of previous studies using other performance-based tasks and cognitive measures (Duval et al., Reference Duval, Piolino, Bejanin, Eustache and Desgranges2011; Li et al., Reference Li, Wang, Wang, Tao, Xie and Cheng2012) and our Hypothesis H4. Moreover, these differences appear to only be significant when participants are aged over 35 years. This result is consistent with the previous literature showing how the decline of certain cognitive skills and brain regions may begin in the early 30s (Deary et al., Reference Deary2009; Salthouse, Reference Salthouse2009). We suggest that from these ages, when the cognitive decline begins, educational level could be an active component of our CR that buffers the decline in cognitive empathy.
Therefore, the present study has shed light on the effect of CR on the capacity to show cognitive empathy throughout adulthood. These findings have important clinical implications. In particular, the data reported here suggest that lower educated people aged 35 years and above are particularly at risk of showing age-related decline in cognitive empathy. Future research and clinical intervention should thus focus on improving cognitive empathy abilities in this population, which is particularly important given the association between this ability and mental health (De Achával et al., Reference De Achával2010; Machado-de-Sousa et al., Reference Machado-de-Sousa2010).
Our research is not without certain limitations. Firstly, there is a lack of participants who met the criteria of primary-level education in early adulthood, since participants with a primary level of education tend to be advanced in age. Nonetheless, we obtained similar results with our high-school-educated participants, which diminishes the importance of this limitation. Secondly, our study evaluated CR only through the education level of the participants. Following Chapko et al. (Reference Chapko, McCormack, Black, Staff and Murray2018) and Jones et al. (Reference Jones, Manly, Glymour, Rentz, Jefferson and Stern2011), it would also be of interest to employ neuroimaging techniques to measure CR as well as other complementary behavioral measures. Therefore, future research studies should aim to replicate these results using additional measures. In a similar vein, future lines of investigation should aim to evaluate these results with alternative cognitive empathy instruments in order to address the complexity of this construct (Decety et al., Reference Decety, Smith and Norman2018), together with the assessment of the emotional empathy component. Finally, given the cross-sectional nature of this study, our results might have been impacted by a cohort effect, which could be avoided in future research by conducting longitudinal studies.
In conclusion, CR, measured through educational level, appears to be a protective factor not only for the decline of cognitive and emotional intelligence (Cabello et al., Reference Cabello, Navarro Bravo, Latorre and Fernández-Berrocal2014; Chapko et al., Reference Chapko, McCormack, Black, Staff and Murray2018; Ritchie and Tucker-Drob, Reference Ritchie and Tucker-Drob2018), but also for the cognitive empathy ability. Our study contributes to the CR literature by showing the educational level required to prevent an age-related decrease in cognitive empathy in individuals from the age of 35 years and sheds light on the existing relationship between cognitive empathy and age by showing that it takes the form of a quadratic pattern.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Source of funding
This work was supported by The Spanish Ministry of Economy, Industry, and Competitiveness (project: PSI2017-84170-R to P.F-B.) and by Junta de Andalucía (project: UMA18-FEDERJA-137 to A.M-R; and UMA18- FEDERJA-114 to P.F-B and R.C.).
Description of authors’ roles
All authors contributed to the conception and design of the study and approved the submitted version and agreed to be accountable for all aspects of the work. MJG-C, RC, AM-R, and RG-L contributed to the acquisition of the data. MJG-C and PF-B organized the database. RC and PF-B performed the statistical analysis. MJG-C wrote the first draft of the manuscript. RC, AM-R, RG-L, SB-C, and PF-B revised it critically for important intellectual content.
Acknowledgments
SB-C was funded by the Autism Research Trust, the Wellcome Trust, the Templeton World Charitable Foundation, and the NIHR Biomedical Research Centre in Cambridge, during the period of this work. SB-C received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No 777394. The JU receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA and AUTISM SPEAKS, Autistica, SFARI. The research conducted by SB-C was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East of England at Cambridgeshire and Peterborough NHS Foundation Trust. The views expressed are those of the author(s) and not necessarily those of the NHS, NIHR, or Department of Health and Social Care.
Ethical statement
The Research Ethics Committee of the University of Málaga approved the study protocol (14-2019-H) as part of the project PSI2017-84170-R. Participants gave informed consent and were assessed in accordance with the Helsinki declaration





 Open access
Open access