


Introduction
The eating patterns of most Americans are not aligned with federal dietary recommendations for health promotion and the prevention of excess weight gain(Reference Kirkpatrick, Dodd and Reedy1-Reference Wilson, Reedy and Krebs-Smith3). Poor dietary intake and related eating behaviours contribute to several common health problems among US paediatric populations, including obesity, dyslipidaemias, insulin resistance, high blood pressure, pulmonary disorders, dental caries and anaemia(4-Reference Ogata and Hayes10). Approximately 18 % of young US individuals are at a weight categorised as obese, 19 % have unfavourable lipid levels, and 14 % have high blood pressure(Reference Hales, Fryar and Carroll11-Reference Perak, Ning and Kit13). Young individuals who gain weight in excess of health recommendations are also more likely to experience weight-related teasing and struggle with psychosocial health problems and poor body image(Reference Neumark-Sztainer, Falkner and Story14,Reference Loth, Wall and Larson15) . Poor body image puts young individuals at risk for engaging in disordered eating and such unhealthy attempts at weight control tend to promote greater weight gain over time(Reference Neumark-Sztainer, Wall and Haines16-Reference Bucchianeri, Fernandes and Loth19). In order to design effective and equitable solutions to these health problems it is important to identify disparities in their burden among the population and contributing nutritional disparities(Reference Ning, Labarthe and Shay20-Reference Henshaw, Garcia and Weintraub25).
In the USA and internationally, there are several disparities in obesity and nutrition-related health conditions among paediatric populations(Reference Dong, Arnold and Peng26-Reference Skinner, Ravanbakht and Skelton33). The prevalence of obesity among young US individuals aged 2–19 years varies from approximately 10 % among Asian children to 24 % among Hispanic children, and is inversely related to the educational attainment of parents(Reference Skinner, Ravanbakht and Skelton33,Reference Ogden, Fryar and Hales34) . Similarly, the odds of elevated blood pressure are higher among adolescents who receive Medicaid health benefits or are uninsured in comparison with adolescents who receive private health insurance benefits(Reference Staiano, Morrell and Hsia32). Differences in dietary intake and eating behaviours across population subgroups are likely contributors to these disparities among children and adolescents(Reference Guerrero, Mao and Fuller30,Reference Isong, Rao and Bind35) . The design of nutrition programmes and policies thus needs to be informed by the most current information on the distribution of nutritional problems, including overall low diet quality, markers of poor dietary intake, unhealthy meal and snack patterns, problematic feeding practices and disordered eating.
Although many national and local programmes are working to eliminate disparities in nutritional and weight-related health, to the best of the authors’ knowledge, no recent reviews focusing on US children and adolescents have been published that comprehensively summarise disparities in dietary intake, eating behaviours and feeding practices. The objective of the present narrative review was to summarise current evidence of disparities in these nutritional problems among young US individuals (2–19 years) according to age, sex, socio-economic status (SES), ethnicity/race and rural–urban location. Markers of poor dietary intake (overall low diet quality, underconsumed and overconsumed dietary components), unhealthy meal and snack patterns, and problematic feeding practices are examined across the life course from early childhood to adolescence; however, the literature on disordered eating is examined with a focus on adolescence in accordance with the prevalence of problems. The evidence base is further discussed in terms of scientific gaps and what future research is needed to better promote equity through programme and policy development.
Methods
The content of the evidence summary that is presented in this review is narrative in approach; however, the scientific literature was systematically searched in order to identify and retrieve relevant studies in a comprehensive manner. An electronic search of the PubMed® and MEDLINE® databases (https://www.nlm.nih.gov/bsd/pmresources.html) was completed to identify peer-reviewed research studies published between January 2009 and January 2019. Research published before January 2009 was not reviewed given the importance of understanding the current distribution of nutritional problems and because there have been many efforts over the past decade to strengthen food and nutrition policies. The following search terms were used in various combinations: toddlers, preschoolers, children, adolescents, disparity, nutrition, dietary intake, fast food, breakfast, meal skipping, family meals, feeding practices, binge eating, disordered eating, and unhealthy weight-control behaviour. Search results, including article titles and abstracts, were examined by the author and the full text of all potentially relevant articles was retrieved for detailed evaluation. Reference citations within identified articles were also examined to ensure that all relevant evidence was retrieved.
Articles had to be published in English, conducted in the USA among a paediatric sample (2–19 years), and address at least one aspect of dietary intake, meal/snack patterns, feeding practices or disordered eating in order to be included in the present review. Studies were included regardless of whether all children (2–19 years) were analysed together or separately according to various age groupings (for example, toddlers and preschool-age children: 2–5 years; middle childhood: 6–11 years; adolescence: 12–19 years). Studies reporting only on breast-feeding, the nutritional wellbeing of infants or outcomes of poor dietary intake (for example, Fe-deficiency anaemia, dental caries) were excluded from the present review.
Three categories of dietary intake markers were defined: overall dietary quality, underconsumed dietary components and overconsumed dietary components. Markers of overall dietary quality were defined to include dietary pattern indexes and scores such as the Healthy Eating Index (HEI)(Reference Guenther, Kirkpatrick and Reedy36,Reference Krebs-Smith, Pannucci and Subar37) . Underconsumed dietary components were defined with reference to the current Dietary Guidelines for Americans and the recommended shifts in intake that this document describes are needed to align with healthy eating patterns(38). Similarly, overconsumed dietary components were defined with reference to the Dietary Guidelines for Americans and the guidance it outlines for limiting juice intake to half the recommended amount for fruits and for limiting intake of added sugars, saturated fat and Na(38,Reference Heyman and Abrams39) .
Results
The literature search of original research addressing various aspects of nutritional wellbeing identified a total of ninety-nine studies, including five studies of overall diet quality(Reference Gu and Tucker40-Reference Thomson, Tussing-Humphreys and Goodman44), forty-five studies that examined underconsumed dietary components(Reference Kirkpatrick, Dodd and Reedy1,Reference Krebs-Smith, Guenther and Subar2,Reference Cutler, Flood and Hannan41,Reference Wallace, Reider and Fulgoni45-Reference Kann, McManus and Harris86) , fifty-three studies that examined overconsumed dietary components(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Wang, Vine and Hsiao53,Reference Davis, Bennett and Befort56-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Khalsa, Kharofa and Ollberding72,Reference Watowicz, Anderson and Kaye75,Reference Guerrero, Ponce and Chung77,Reference Watowicz and Taylor79,Reference de Hoog, Kleinman and Gillman82-Reference Salvo, Frediani and Ziegler84,Reference Kann, McManus and Harris86-Reference Reedy and Krebs-Smith109) , twenty-six studies that examined unhealthy meal and snack patterns(Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49,Reference Eagle, Sheetz and Gurm54,Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82,Reference Kant and Graubard91-Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Piernas and Popkin110-Reference Powell, Nguyen and Han125) , nine studies that examined problematic feeding practices(Reference Ranjit, Evans and Springer52,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Taveras, Gillman and Kleinman97,Reference Larson, Eisenberg and Berge118,Reference Berge, Tate and Trofholz126-Reference Huang, Parks and Kumanyika130) and seven studies of disordered eating behaviours(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131-Reference Lee-Winn, Reinblatt and Mojtabai136) . In addition, recent literature reviews regarding feeding practices(Reference Loth, Fulkerson and Neumark-Sztainer137) and binge eating behaviours(Reference Jennings, Kelly-Weeder and Wolfe138) were identified and used in summarising the results. The detailed summary of identified studies that follows is organised according to aspect of nutritional wellbeing. Tables with details of the included studies are organised such that nationally representative studies relating to dietary intake and eating patterns are included in Table 1, studies relating to feeding practices are included in Table 2, and studies relating to disordered eating are included in Table 3. Given the large number of studies that relate to dietary intake and eating patterns, only the details of nationally representative studies could be given in Table 1; however, all identified studies are represented in the summary of findings below.
Table 1. Patterns in dietary intake, meal frequency and snacking behaviours of nationally representative US paediatric samples (2–19 years) according to age, sex, ethnic/racial minority composition, markers of socio-economic status and rural–urban location*

HEI-2015, Healthy Eating Index 2015; SSB, sugar-sweetened beverages; WIC, Women, Infants and Children; NHANES, National Health and Nutrition Examination Survey; HEI-2010, Healthy Eating Index 2010; CEPC, cup-equivalents per 1,000 calories; HEI-2005, Healthy Eating Index 2005; USDA, United States Department of Agriculture.
* The studies identified in this Table represent peer-reviewed publications that were published or made publicly accessible between January 2009 and January 2019.
Table 2. Patterns in parent feeding practices of relevance to US paediatric populations (2–19 years) according to age, sex, ethnic/racial minority composition, markers of socio-economic status and rural–urban location*
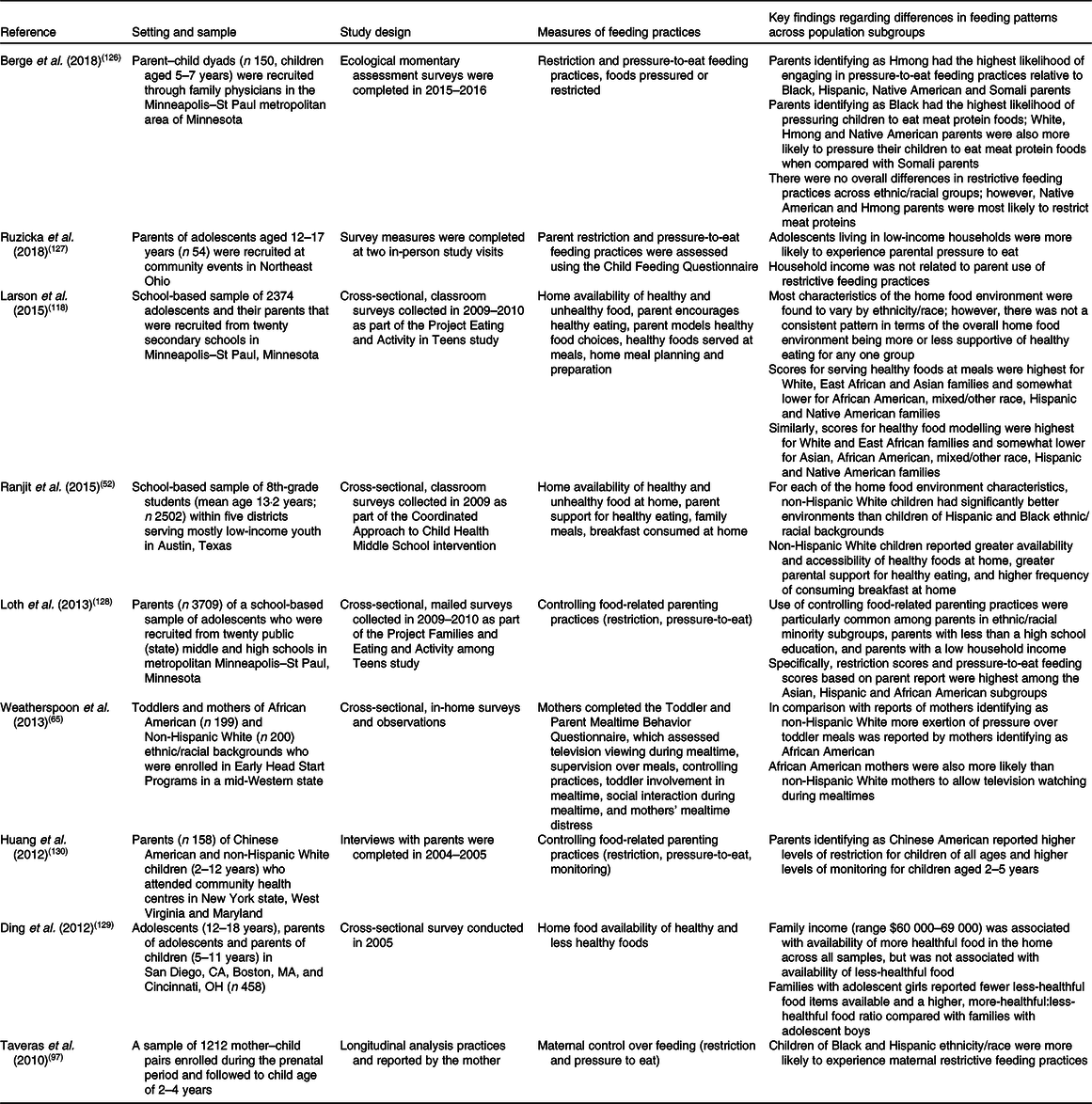
* The studies identified in this Table represent peer-reviewed publications that were published or made publicly accessible between January 2009 and January 2019.
Table 3. Patterns in disordered eating behaviours in US paediatric populations (2–19 years) according to age, sex, ethnic/racial minority composition, markers of socio-economic status and rural–urban location*
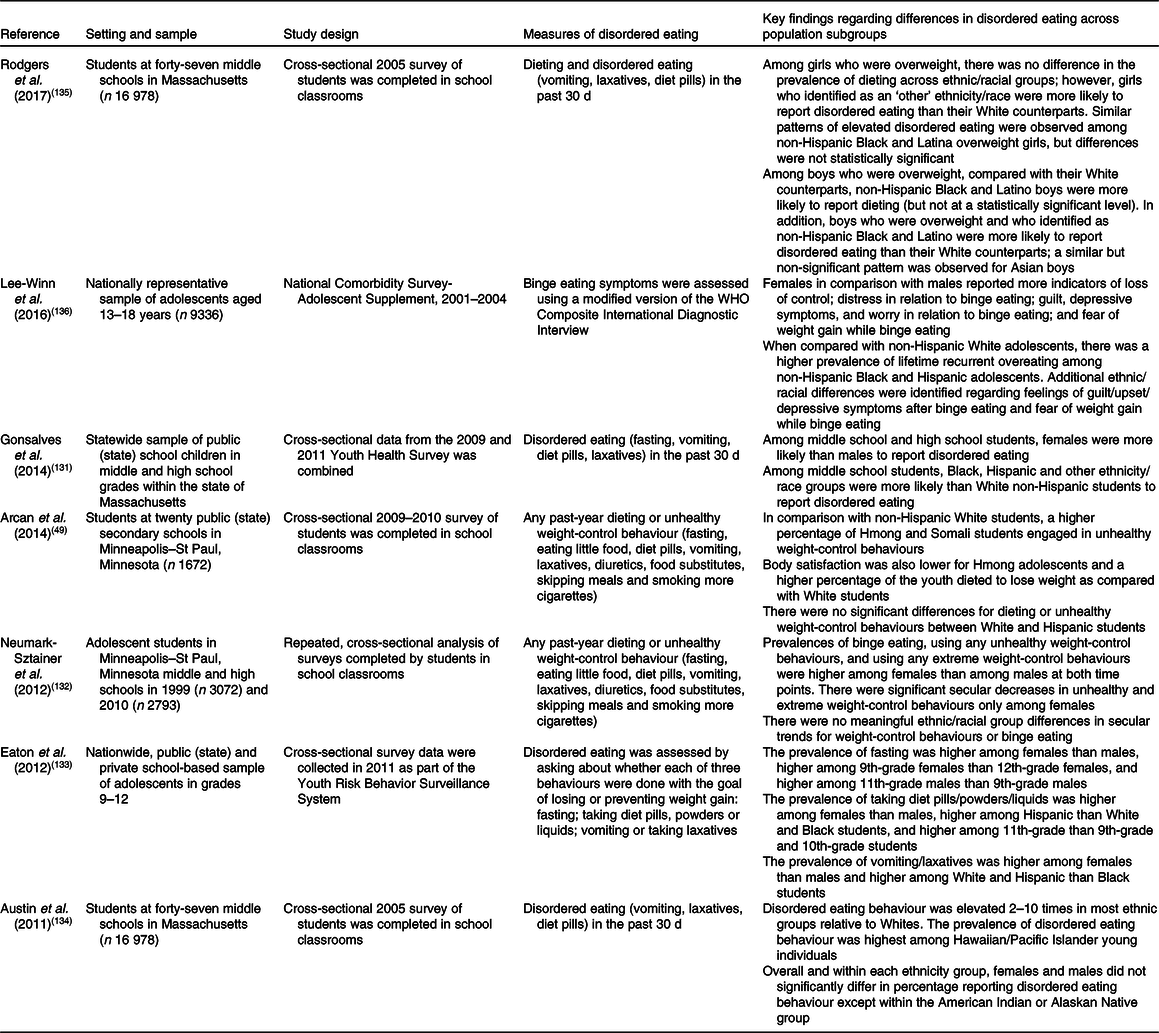
* The studies identified in this Table represent peer-reviewed publications that were published or made publicly accessible between January 2009 and January 2019.
Overall low diet quality
Disparities in overall dietary patterns and quality have been described according to age(Reference Gu and Tucker40,Reference Banfield, Liu and Davis42-Reference Thomson, Tussing-Humphreys and Goodman44) , sex(Reference Gu and Tucker40,Reference Hiza, Casavale and Guenther43) , ethnicity/race(Reference Gu and Tucker40,Reference Cutler, Flood and Hannan41,Reference Hiza, Casavale and Guenther43,Reference Thomson, Tussing-Humphreys and Goodman44) and markers of SES(Reference Gu and Tucker40,Reference Cutler, Flood and Hannan41,Reference Hiza, Casavale and Guenther43) . One example of these studies calculated the Healthy Eating Index 2010 (HEI-2010) score for all child and adolescent participants who completed dietary recalls as part of the National Health and Nutrition Examination Survey over the years 1999 to 2012(Reference Gu and Tucker40). The nationally representative results showed that there was population-level improvement over time in diet quality, but that overall diet quality remained poor (mean score: 50·9 of 100 points) in 2012 and improvements were not equal across population subgroups(Reference Gu and Tucker40). Results showed that older children and adolescents had consistently lower HEI-2010 scores than preschool-aged children, and non-Hispanic Black children and adolescents had consistently lower scores than those who identified with other ethnic/racial groups. There was also evidence that low-SES participants who were enrolled in the Supplemental Nutrition Assistance Program had lower scores than non-participants after the 2003–2004 assessment year(Reference Gu and Tucker40).
Markers of poor diet: underconsumed dietary components
Disparities in children’s intake of healthful dietary components have been identified and differences described according to age(Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45,Reference Moore, Radcliffe and Liu46,Reference Bailey, Catellier and Jun60,Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63,Reference Herrick, Terry and Afful68,Reference Demmer, Cifelli and Houchins69,Reference Drewnowski, Rehm and Constant73,Reference Watowicz, Anderson and Kaye75,Reference Herrick, Rossen and Nielsen76,Reference Kim, Moore and Galuska78,Reference Storey and Anderson80,Reference Kann, McManus and Harris86) , sex(Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45-Reference Longacre, Drake and Titus48,Reference Herrick, Terry and Afful68,Reference Storey and Anderson71,Reference Drewnowski, Rehm and Constant73,Reference Kim, Moore and Galuska78,Reference Storey and Anderson80,Reference Kant and Graubard85,Reference Kann, McManus and Harris86) , ethnicity/race(Reference Kirkpatrick, Dodd and Reedy1,Reference Cutler, Flood and Hannan41,Reference Moore, Radcliffe and Liu46,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Ranjit, Evans and Springer52,Reference Papanikolaou, Brooks and Reider55,Reference Welker, Jacquier and Catellier59,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Demmer, Cifelli and Houchins67-Reference Keim and Branum74,Reference Herrick, Rossen and Nielsen76-Reference Kim, Moore and Galuska78,Reference Storey and Anderson80,Reference de Hoog, Kleinman and Gillman82-Reference Kann, McManus and Harris86) and markers of SES(Reference Kirkpatrick, Dodd and Reedy1,Reference Cutler, Flood and Hannan41,Reference Moore, Radcliffe and Liu46,Reference Longacre, Drake and Titus48,Reference Wang, Vine and Hsiao53,Reference Eagle, Sheetz and Gurm54,Reference Jun, Catellier and Eldridge62,Reference Vercammen, Moran and Zatz66,Reference Khalsa, Kharofa and Ollberding72,Reference Drewnowski, Rehm and Constant73,Reference Herrick, Rossen and Nielsen76,Reference Watowicz and Taylor79,Reference Storey and Anderson80) . This evidence comes from forty-one studies that were cross-sectional in design or examined trends over time; twenty-nine studies were nationally representative(Reference Kirkpatrick, Dodd and Reedy1,Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45-Reference Kann, McManus and Harris47,Reference Haughton, Wang and Lemon50,Reference Dodd, Briefel and Cabili51,Reference Wang, Vine and Hsiao53,Reference Papanikolaou, Brooks and Reider55,Reference Welker, Jacquier and Catellier59-Reference Fox, Condon and Briefel64,Reference Vercammen, Moran and Zatz66-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Drewnowski, Rehm and Constant73-Reference Herrick, Rossen and Nielsen76,Reference Kim, Moore and Galuska78-Reference Storey and Anderson80,Reference Kant and Graubard85,Reference Kann, McManus and Harris86) (Table 1), eight represented local/regional populations(Reference Cutler, Flood and Hannan41,Reference Longacre, Drake and Titus48,Reference Arcan, Larson and Bauer49,Reference Ranjit, Evans and Springer52,Reference Eagle, Sheetz and Gurm54,Reference Khalsa, Kharofa and Ollberding72,Reference Guerrero, Ponce and Chung77,Reference Kong, Odoms-Young and Schiffer83) and four were convenience samples(Reference Weatherspoon, Venkatesh and Horodynski65,Reference Ling, Zahry and Wasilevich70,Reference de Hoog, Kleinman and Gillman82,Reference Salvo, Frediani and Ziegler84) . More than half of the studies made use of dietary recalls(Reference Kirkpatrick, Dodd and Reedy1,Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45,Reference Moore, Radcliffe and Liu46,Reference Haughton, Wang and Lemon50,Reference Dodd, Briefel and Cabili51,Reference Wang, Vine and Hsiao53,Reference Papanikolaou, Brooks and Reider55,Reference Welker, Jacquier and Catellier59-Reference Fox, Condon and Briefel64,Reference Vercammen, Moran and Zatz66-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Drewnowski, Rehm and Constant73-Reference Herrick, Rossen and Nielsen76,Reference Kim, Moore and Galuska78-Reference Storey and Anderson80,Reference Kong, Odoms-Young and Schiffer83,Reference Kant and Graubard85) , five studies assessed dietary intake with a FFQ(Reference Cutler, Flood and Hannan41,Reference Arcan, Larson and Bauer49,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Ling, Zahry and Wasilevich70,Reference de Hoog, Kleinman and Gillman82) , seven studies used brief survey measures(Reference Kann, McManus and Harris47,Reference Longacre, Drake and Titus48,Reference Ranjit, Evans and Springer52,Reference Eagle, Sheetz and Gurm54,Reference Guerrero, Ponce and Chung77,Reference Ettienne-Gittens, McKyer and Odum81,Reference Kann, McManus and Harris86) and two studies made use of food records(Reference Khalsa, Kharofa and Ollberding72,Reference Salvo, Frediani and Ziegler84) . The combined evidence base most consistently identifies adolescents, females and young individuals from lower-SES households as at risk for poor intake of milk and nutrients of public health concern (i.e. Ca, vitamin D). There is also evidence that younger children and those from higher-SES households tend to consume more fruit and vegetables(Reference Krebs-Smith, Guenther and Subar2,Reference Longacre, Drake and Titus48,Reference Watowicz, Anderson and Kaye75,Reference Kim, Moore and Galuska78) . Although a number of studies examined ethnic/racial differences, the findings have been mixed. As only four other studies were found to have examined rural–urban differences in intake of commonly underconsumed dietary components(Reference Davis, Bennett and Befort56-Reference Liu, Jones and Sun58,Reference Ettienne-Gittens, McKyer and Odum81) , the findings are not summarised here in detail.
Age and sex disparities
Existing studies addressing age and sex disparities have focused on intake of water(Reference Drewnowski, Rehm and Constant73,Reference Watowicz, Anderson and Kaye75,Reference Kant and Graubard85,Reference Kann, McManus and Harris86) , fruit(Reference Krebs-Smith, Guenther and Subar2,Reference Kann, McManus and Harris47,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Demmer, Cifelli and Houchins67,Reference Khalsa, Kharofa and Ollberding72,Reference Herrick, Rossen and Nielsen76,Reference Kim, Moore and Galuska78,Reference Kann, McManus and Harris86) , vegetables(Reference Krebs-Smith, Guenther and Subar2,Reference Kann, McManus and Harris47,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Demmer, Cifelli and Houchins67,Reference Storey and Anderson71,Reference Khalsa, Kharofa and Ollberding72,Reference Kim, Moore and Galuska78,Reference Kann, McManus and Harris86) , dairy products(Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45,Reference Kann, McManus and Harris47,Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Demmer, Cifelli and Houchins67-Reference Demmer, Cifelli and Houchins69,Reference Drewnowski, Rehm and Constant73,Reference Watowicz, Anderson and Kaye75,Reference Kann, McManus and Harris86) and other nutrient-dense foods(Reference Krebs-Smith, Guenther and Subar2,Reference Kay, Welker and Jacquier61,Reference Fox, Condon and Briefel64) , along with fibre and nutrients of public health concern (i.e. Ca, vitamin D)(Reference Wallace, Reider and Fulgoni45,Reference Moore, Radcliffe and Liu46,Reference Bailey, Catellier and Jun60,Reference Demmer, Cifelli and Houchins67,Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Storey and Anderson80) . For example, national data based on the collection of dietary recalls show that young children (2–3 years) are more likely than all other age groups to consume adequate amounts of fruit, orange vegetables, legumes and milk(Reference Krebs-Smith, Guenther and Subar2,Reference Watowicz, Anderson and Kaye75,Reference Kim, Moore and Galuska78) . National data show that adolescent females tend to have the poorest intake of milk, grains, and meats and beans(Reference Krebs-Smith, Guenther and Subar2,Reference Kann, McManus and Harris47) . Analyses focused on Ca and vitamin D have aligned with such findings in showing that these key nutrients provided by milk are more often underconsumed by young individuals aged 9–18 years than children 4–8 years; the percentage of children with inadequate intake tends to increase with age(Reference Wallace, Reider and Fulgoni45,Reference Moore, Radcliffe and Liu46,Reference Demmer, Cifelli and Houchins69) . In regards to water consumption, older children consume a greater volume but there is mixed evidence regarding sex differences(Reference Drewnowski, Rehm and Constant73,Reference Watowicz, Anderson and Kaye75,Reference Kant and Graubard85) .
Socio-economic disparities
The evidence base suggests that intakes of plain water, milk, fruit, vegetables, whole grains, fibre, Ca and vitamin D tend to be poorer among young individuals with fewer household resources(Reference Kirkpatrick, Dodd and Reedy1,Reference Cutler, Flood and Hannan41,Reference Wallace, Reider and Fulgoni45,Reference Moore, Radcliffe and Liu46,Reference Longacre, Drake and Titus48,Reference Wang, Vine and Hsiao53,Reference Eagle, Sheetz and Gurm54,Reference Khalsa, Kharofa and Ollberding72,Reference Drewnowski, Rehm and Constant73,Reference Watowicz and Taylor79,Reference Storey and Anderson80) . National data show that the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) is protective for these young children. Toddlers and preschool-age children who participate in WIC tend to have higher intake of milk and a lower risk of inadequate vitamin D intake when compared with low-income non-participants(Reference Jun, Catellier and Eldridge62,Reference Vercammen, Moran and Zatz66,Reference Watowicz and Taylor79) . A recent analysis of dietary recall data provided by 1542 adolescents in Northern New England confirmed the finding that fruit and vegetable intake is positively related to household income(Reference Longacre, Drake and Titus48). However, just as WIC is protective for young children, the results further showed that being provided meals at school may mitigate income-related disparities for adolescents(Reference Longacre, Drake and Titus48). Among adolescent participants who received school meals there was very little difference in fruit and vegetable intake by household income(Reference Longacre, Drake and Titus48). The results instead highlighted that adolescents’ average intake of fruit and vegetables was low regardless of income(Reference Longacre, Drake and Titus48).
Ethnic/racial disparities
Less consistent evidence has identified ethnic/racial differences in intakes of milk, water, fruit, vegetables, whole grains, PUFA, fibre and nutrients of public health concern (i.e. Ca, vitamin D)(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Ranjit, Evans and Springer52,Reference Papanikolaou, Brooks and Reider55,Reference Welker, Jacquier and Catellier59,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Demmer, Cifelli and Houchins67-Reference Storey and Anderson71,Reference Drewnowski, Rehm and Constant73,Reference Keim and Branum74,Reference Herrick, Rossen and Nielsen76-Reference Kim, Moore and Galuska78,Reference Storey and Anderson80,Reference de Hoog, Kleinman and Gillman82-Reference Kann, McManus and Harris86) . At least nine studies have reported that non-Hispanic White children tend to have higher milk intakes than Black children(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Dodd, Briefel and Cabili51,Reference Welker, Jacquier and Catellier59,Reference Demmer, Cifelli and Houchins67-Reference Demmer, Cifelli and Houchins69,Reference de Hoog, Kleinman and Gillman82,Reference Kann, McManus and Harris86) , but evidence regarding differences in intake between Hispanic and non-Hispanic children is inconsistent(Reference Arcan, Larson and Bauer49,Reference Ranjit, Evans and Springer52,Reference Demmer, Cifelli and Houchins67,Reference de Hoog, Kleinman and Gillman82) . There is similarly inconsistent evidence regarding differences in intake between White and Asian children. Some evidence suggests that Asian children tend to have higher intakes of fruit and vegetables than White children(Reference Cutler, Flood and Hannan41,Reference Haughton, Wang and Lemon50) whereas other findings have indicated Asian girls who identify as Hmong tend to have low vegetable intake(Reference Arcan, Larson and Bauer49). One study found that non-Hispanic Black children consumed more fruit as 100 % juice and less fruit as whole fruit in comparison with non-Hispanic White, Asian and Hispanic children(Reference Herrick, Rossen and Nielsen76). There is also some evidence that non-Hispanic White children consume more plain water, on average, as compared with Mexican American and non-Hispanic Black children(Reference Drewnowski, Rehm and Constant73,Reference Kant and Graubard85) . Total beverage moisture was found to be highest among non-Hispanic White and Mexican American children(Reference Kant and Graubard85).
Markers of poor diet: overconsumed dietary components
There is much evidence of disparities according to age(Reference Wang, Vine and Hsiao53,Reference Bailey, Catellier and Jun60,Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88,Reference Piernas and Popkin89,Reference Dunford and Popkin93,Reference Wang, Guglielmo and Welsh98,Reference Carriquiry, Moshfegh and Steinfeldt102-Reference Reedy and Krebs-Smith109) , sex(Reference Kann, McManus and Harris47,Reference Wang, Vine and Hsiao53,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88-Reference Mendez, Sotres-Alvarez and Miles90,Reference Tate, Dillaway and Yarandi95,Reference Wang, Guglielmo and Welsh98,Reference Nickelson, Lawrence and Parton103-Reference Slining and Popkin105,Reference Ervin, Kit and Carroll108) , ethnicity/race(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Ranjit, Evans and Springer52,Reference Welker, Jacquier and Catellier59,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82-Reference Salvo, Frediani and Ziegler84,Reference Kann, McManus and Harris86-Reference Rosinger, Herrick and Gahche88,Reference Kant and Graubard91-Reference Dunford and Popkin93,Reference Bleich and Wolfson96-Reference Wang, Guglielmo and Welsh98,Reference Nickelson, Lawrence and Parton103-Reference Han and Powell106,Reference Ervin, Kit and Carroll108,Reference Reedy and Krebs-Smith109) and markers of SES(Reference Jun, Catellier and Eldridge62,Reference Watowicz and Taylor79,Reference Dunford, Poti and Popkin87,Reference Larson, Story and Eisenberg92-Reference Tate, Dillaway and Yarandi95,Reference Wang, Guglielmo and Welsh98,Reference McElligott, Roberts and Varadi99,Reference Nickelson, Lawrence and Parton103,Reference Slining and Popkin105,Reference Han and Powell106) in children’s intake of dietary components that tend to be consumed in excess. This evidence is based on thirty-seven cross-sectional analyses(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Wang, Vine and Hsiao53,Reference Welker, Jacquier and Catellier59-Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Khalsa, Kharofa and Ollberding72,Reference Watowicz, Anderson and Kaye75,Reference Guerrero, Ponce and Chung77,Reference Watowicz and Taylor79,Reference de Hoog, Kleinman and Gillman82-Reference Salvo, Frediani and Ziegler84,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88,Reference Guerrero and Chung94,Reference Tate, Dillaway and Yarandi95,Reference Taveras, Gillman and Kleinman97-Reference McElligott, Roberts and Varadi99,Reference Quader, Zhao and Gillespie101,Reference Nickelson, Lawrence and Parton103,Reference Ervin, Kit and Carroll108,Reference Reedy and Krebs-Smith109) and thirteen studies of secular trends over time(Reference Dunford, Poti and Popkin87,Reference Piernas and Popkin89-Reference Dunford and Popkin93,Reference Bleich and Wolfson96,Reference Powell, Smith-Taillie and Popkin100,Reference Carriquiry, Moshfegh and Steinfeldt102,Reference Ervin and Ogden104-Reference Fulgoni and Quann107) ; thirty-six studies were nationally representative (Table 1)(Reference Kirkpatrick, Dodd and Reedy1,Reference Kann, McManus and Harris47,Reference Haughton, Wang and Lemon50,Reference Dodd, Briefel and Cabili51,Reference Wang, Vine and Hsiao53,Reference Welker, Jacquier and Catellier59-Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Vercammen, Moran and Zatz66-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Watowicz, Anderson and Kaye75,Reference Watowicz and Taylor79,Reference Kann, McManus and Harris86-Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Bleich and Wolfson96,Reference Wang, Guglielmo and Welsh98,Reference Powell, Smith-Taillie and Popkin100-Reference Carriquiry, Moshfegh and Steinfeldt102,Reference Ervin and Ogden104-Reference Reedy and Krebs-Smith109) , eight represented local/regional populations(Reference Arcan, Larson and Bauer49,Reference Ranjit, Evans and Springer52,Reference Khalsa, Kharofa and Ollberding72,Reference Guerrero, Ponce and Chung77,Reference Kong, Odoms-Young and Schiffer83,Reference Larson, Story and Eisenberg92,Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97) and six studies enrolled convenience samples(Reference Weatherspoon, Venkatesh and Horodynski65,Reference de Hoog, Kleinman and Gillman82,Reference Salvo, Frediani and Ziegler84,Reference Tate, Dillaway and Yarandi95,Reference McElligott, Roberts and Varadi99,Reference Nickelson, Lawrence and Parton103) . More than half of the studies made use of dietary recalls(Reference Kirkpatrick, Dodd and Reedy1,Reference Haughton, Wang and Lemon50,Reference Dodd, Briefel and Cabili51,Reference Wang, Vine and Hsiao53,Reference Welker, Jacquier and Catellier59-Reference Fox, Condon and Briefel64,Reference Vercammen, Moran and Zatz66-Reference Demmer, Cifelli and Houchins69,Reference Storey and Anderson71,Reference Watowicz, Anderson and Kaye75,Reference Watowicz and Taylor79,Reference Kong, Odoms-Young and Schiffer83,Reference Dunford, Poti and Popkin87-Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Bleich and Wolfson96,Reference Wang, Guglielmo and Welsh98,Reference Powell, Smith-Taillie and Popkin100-Reference Carriquiry, Moshfegh and Steinfeldt102,Reference Ervin and Ogden104-Reference Reedy and Krebs-Smith109) , five studies assessed dietary intake with a FFQ(Reference Arcan, Larson and Bauer49,Reference Weatherspoon, Venkatesh and Horodynski65,Reference de Hoog, Kleinman and Gillman82,Reference Larson, Story and Eisenberg92,Reference Taveras, Gillman and Kleinman97) , eight studies used brief survey measures(Reference Kann, McManus and Harris47,Reference Ranjit, Evans and Springer52,Reference Guerrero, Ponce and Chung77,Reference Kann, McManus and Harris86,Reference Guerrero and Chung94,Reference Tate, Dillaway and Yarandi95,Reference McElligott, Roberts and Varadi99,Reference Nickelson, Lawrence and Parton103) and two studies made use of food records(Reference Khalsa, Kharofa and Ollberding72,Reference Salvo, Frediani and Ziegler84) . The studies identified for the present review suggest that adolescents and males are most likely to report overconsumption of energy-dense, nutrient-poor foods and beverages and excess Na consumption(Reference Watowicz, Anderson and Kaye75,Reference Kann, McManus and Harris86,Reference Carriquiry, Moshfegh and Steinfeldt102) . Similarly consistent evidence suggests that young individuals from lower-SES households and individuals who identify their race as Black are most likely to report a high intake of sugar-sweetened beverages(Reference Kann, McManus and Harris47,Reference Dodd, Briefel and Cabili51,Reference Welker, Jacquier and Catellier59,Reference Khalsa, Kharofa and Ollberding72,Reference Watowicz and Taylor79,Reference Kong, Odoms-Young and Schiffer83,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88,Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Wang, Guglielmo and Welsh98,Reference Han and Powell106,Reference Reedy and Krebs-Smith109) . An additional three cross-sectional studies were found to have used national data to examine and report on mixed evidence of rural–urban differences in patterns of overconsumption(Reference Davis, Bennett and Befort56-Reference Liu, Jones and Sun58). Two of the three studies that examined rural–urban differences were based on dietary recall data(Reference Davis, Bennett and Befort56,Reference Liu, Jones and Sun58) , and one used brief survey measures to assess intake(Reference Kenney, Wang and Iannotti57). One study showed that young individuals (2–11 years) in rural areas consume more total energy on average than their urban counterparts(Reference Liu, Jones and Sun58). In contrast, another study compared adolescents living in an inner-city area with those in a suburban area and found no differences in dietary pattern(Reference Tate, Dillaway and Yarandi95).
Age and sex disparities
Research on age and sex disparities has addressed intakes of sugar-sweetened beverages, sweet and salty snack foods, added sugars, Na, saturated fats and total energy. National data indicate that low-nutrient, energy-dense sweets and sugar-sweetened beverages are commonly consumed at a young age and the percentage of young individuals who consume them on a given day is directly related to age(Reference Welker, Jacquier and Catellier59,Reference Kay, Welker and Jacquier61,Reference Saavedra, Deming and Dattilo63,Reference Fox, Condon and Briefel64,Reference Herrick, Terry and Afful68,Reference Demmer, Cifelli and Houchins69,Reference Khalsa, Kharofa and Ollberding72,Reference Watowicz, Anderson and Kaye75,Reference Nickelson, Lawrence and Parton103,Reference Fulgoni and Quann107) . One national study found that 41 % of 2-year-olds and 49 % of 3-year-olds consumed a sugar-sweetened beverage on a given day(Reference Welker, Jacquier and Catellier59). Adolescents have the highest mean energy consumed from sugar-sweetened beverages and highest percentage of total energy consumed from sugar-sweetened beverages(Reference Watowicz, Anderson and Kaye75,Reference Rosinger, Herrick and Gahche88,Reference Reedy and Krebs-Smith109) . Adolescents also have the highest prevalence of excess dietary Na intake and, in contrast with young children, consume more solid fats from fried potatoes than from milk(Reference Carriquiry, Moshfegh and Steinfeldt102,Reference Reedy and Krebs-Smith109) . Existing studies consistently show males as compared with females tend to report higher intake of sugar-sweetened beverages, added sugars and total energy(Reference Kann, McManus and Harris47,Reference Wang, Vine and Hsiao53,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88,Reference Piernas and Popkin89,Reference Powell, Smith-Taillie and Popkin100,Reference Ervin and Ogden104,Reference Ervin, Kit and Carroll108) . National surveillance data based on dietary recalls with adolescents suggest that this difference may be in part due to males consuming larger portions and more energy at meals than females(Reference Piernas and Popkin89). The 2011–2014 national surveillance data additionally indicate that a slightly higher percentage of males than females (64·5 v. 61·3 %) consumed at least one sugar-sweetened beverage on the given day of their dietary recall(Reference Rosinger, Herrick and Gahche88). These same data show that males consumed more energy from sugar-sweetened beverages compared with females across all age groups, with the exception of children aged 2–5 years(Reference Rosinger, Herrick and Gahche88). One notable contradiction to these findings came from a study in a convenience sample of Black adolescents and indicated that females consumed foods higher in fat and energy than males(Reference Tate, Dillaway and Yarandi95).
Socio-economic disparities
A growing number of studies have provided evidence of differences in dietary patterns according to SES markers. Most existing evidence suggests that sugar-sweetened beverage, juice and added sugar consumption tends to be higher among young individuals with fewer household resources(Reference Jun, Catellier and Eldridge62,Reference Vercammen, Moran and Zatz66,Reference Khalsa, Kharofa and Ollberding72,Reference Watowicz and Taylor79,Reference Guerrero and Chung94,Reference Wang, Guglielmo and Welsh98,Reference McElligott, Roberts and Varadi99,Reference Han and Powell106) , but that those with limited household resources have lower or comparable intakes of sweets and solid fats(Reference Kirkpatrick, Dodd and Reedy1). There is also some evidence that recent trends in snacking may lead to changes in SES-related patterns of disparities. An analysis of national trends in Na intake based on dietary recalls found that there was an increase from 1977 to 2014 in the proportion of Na intake derived from snacks among all sociodemographic groups, but that young individuals (2–18 years) in the lowest-household education (less than high school) and lowest-household income (less than 185 % of the Federal Poverty Level) groups had the largest increases in Na intake from snacks over time(Reference Dunford, Poti and Popkin87). It was notable that children in the lowest-income compared with the highest-income group had significantly lower Na intakes from snacks in 1977–1978 whereas there was no difference in Na intakes between these groups in 2011–2014(Reference Dunford, Poti and Popkin87). National data further indicate that toddlers and preschoolers enrolled in WIC have a higher risk of excessive Na intake than higher-income non-participants(Reference Jun, Catellier and Eldridge62).
Ethnic/racial disparities
Research on ethnic/racial differences in intake of overconsumed dietary components has found a similarly mixed pattern of disparities. Several studies suggest that intake of sugar-sweetened beverages is higher among children of Black race and lower among children of Asian race than among non-Hispanic White children(Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49-Reference Dodd, Briefel and Cabili51,Reference Welker, Jacquier and Catellier59,Reference Herrick, Terry and Afful68,Reference Demmer, Cifelli and Houchins69,Reference de Hoog, Kleinman and Gillman82-Reference Salvo, Frediani and Ziegler84,Reference Kann, McManus and Harris86,Reference Rosinger, Herrick and Gahche88,Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Wang, Guglielmo and Welsh98,Reference Han and Powell106,Reference Reedy and Krebs-Smith109) ; however, some evidence suggests that intake of sugar-sweetened beverages varies across Asian subgroups(Reference Guerrero, Ponce and Chung77). A small number of studies have found that Black children consume more Na and unhealthy foods such as desserts, chips (crisps) and other energy-dense snacks(Reference Ranjit, Evans and Springer52,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Storey and Anderson71,Reference Kong, Odoms-Young and Schiffer83,Reference Larson, Story and Eisenberg92) . Among young children (2–4 years), nationally representative data suggest that more non-Hispanic White children consume some forms of sugary snack foods on a given day in comparison with non-Hispanic Black (for example, ice cream, pudding) and Hispanic children (for example, candy)(Reference Welker, Jacquier and Catellier59). National survey data also suggest that non-Hispanic White children are less likely than Hispanic children to meet recommendations for limiting intake of solid fats and added sugars and have higher intakes of solid fats and added sugars in comparison with Black children(Reference Kirkpatrick, Dodd and Reedy1,Reference Demmer, Cifelli and Houchins67,Reference Powell, Smith-Taillie and Popkin100,Reference Ervin and Ogden104,Reference Ervin, Kit and Carroll108) . Non-Hispanic Black children had the largest recent secular increases in Na intake from snacks out of all ethnic/racial groups(Reference Dunford, Poti and Popkin87). National surveillance data for 2011–2014 showed that, based on dietary recalls, Black children had the highest mean Na intake from snacks, representing more than a doubling in mean Na intake from 1977 to 2014(Reference Dunford, Poti and Popkin87).
Unhealthy meal and snack patterns
There is growing evidence that disparities in certain eating patterns such as the frequent skipping of main meals, infrequent eating with other household members as part of family meals, and frequent consumption of meals and snacks prepared away from home may be important contributors to disparities in dietary quality(Reference Larson, Miller and Watts139,Reference Fulkerson, Larson and Horning140) . Whereas little research has examined rural–urban differences in the eating patterns of children, several studies have documented disparities according to age(Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Piernas and Popkin110,Reference Poti and Popkin111,Reference Berge, Truesdale and Sherwood115-Reference Larson, MacLehose and Fulkerson117,Reference Deming, Reidy and Fox119-Reference Vikraman, Fryar and Ogden123,Reference Powell, Nguyen and Han125) , sex(Reference Kann, McManus and Harris47,Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Dunford and Popkin93,Reference Neumark-Sztainer, Wall and Fulkerson116,Reference Larson, MacLehose and Fulkerson117,Reference Powell, Nguyen and Han125) , ethnicity/race(Reference Cutler, Flood and Hannan41,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49,Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82,Reference Kann, McManus and Harris86,Reference Kant and Graubard91-Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Larson, Hannan and Fulkerson112,Reference Masters, Stanek Krogstrand and Eskridge113,Reference Berge, Truesdale and Sherwood115-Reference Larson, MacLehose and Fulkerson117,Reference Vikraman, Fryar and Ogden123,Reference Powell, Nguyen and Han125) and markers of SES(Reference Cutler, Flood and Hannan41,Reference Larson, Story and Eisenberg92,Reference Dunford and Popkin93,Reference Larson, Hannan and Fulkerson112-Reference Chi, Dinh and da Fonseca114,Reference Neumark-Sztainer, Wall and Fulkerson116,Reference Larson, MacLehose and Fulkerson117,Reference Kant and Graubard124,Reference Powell, Nguyen and Han125) . The existing evidence summarised here is based on eighteen cross-sectional analyses(Reference Cutler, Flood and Hannan41,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49,Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82,Reference Kann, McManus and Harris86,Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Masters, Stanek Krogstrand and Eskridge113-Reference Berge, Truesdale and Sherwood115,Reference Larson, MacLehose and Fulkerson117-Reference Deming, Reidy and Fox119,Reference Wang, van der Horst and Jacquier121-Reference Vikraman, Fryar and Ogden123,Reference Powell, Nguyen and Han125) and nine studies of secular trends over time(Reference Kant and Graubard91-Reference Dunford and Popkin93,Reference Piernas and Popkin110-Reference Larson, Hannan and Fulkerson112,Reference Neumark-Sztainer, Wall and Fulkerson116,Reference Rehm and Drewnowski120,Reference Kant and Graubard124) ; thirteen studies were nationally representative (Table 1)(Reference Kann, McManus and Harris47,Reference Kann, McManus and Harris86,Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Piernas and Popkin110,Reference Poti and Popkin111,Reference Masters, Stanek Krogstrand and Eskridge113,Reference Deming, Reidy and Fox119-Reference Wang, van der Horst and Jacquier121,Reference Vikraman, Fryar and Ogden123-Reference Powell, Nguyen and Han125) , eleven represented local/regional populations(Reference Cutler, Flood and Hannan41,Reference Arcan, Larson and Bauer49,Reference Guerrero, Ponce and Chung77,Reference Larson, Story and Eisenberg92,Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Larson, Hannan and Fulkerson112,Reference Neumark-Sztainer, Wall and Fulkerson116-Reference Larson, Eisenberg and Berge118,Reference Fink, Racine and Mueffelmann122) , and three were conducted within intervention and clinic-based samples(Reference de Hoog, Kleinman and Gillman82,Reference Chi, Dinh and da Fonseca114,Reference Berge, Truesdale and Sherwood115) . Among these studies, eating patterns were assessed by a mix of assessment tools, including 24 h recalls(Reference Kant and Graubard91,Reference Dunford and Popkin93,Reference Piernas and Popkin110,Reference Poti and Popkin111,Reference Deming, Reidy and Fox119-Reference Wang, van der Horst and Jacquier121,Reference Vikraman, Fryar and Ogden123-Reference Powell, Nguyen and Han125) , food records(Reference Poti and Popkin111), FFQ(Reference Cutler, Flood and Hannan41,Reference Arcan, Larson and Bauer49,Reference Larson, Story and Eisenberg92) and brief survey measures(Reference Kann, McManus and Harris47,Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82,Reference Kann, McManus and Harris86,Reference Guerrero and Chung94,Reference Taveras, Gillman and Kleinman97,Reference Larson, Hannan and Fulkerson112-Reference Larson, Eisenberg and Berge118,Reference Fink, Racine and Mueffelmann122) . The evidence base collectively suggests that these problematic eating patterns are most prevalent among adolescents, young individuals from low-SES backgrounds, and young individuals who identify with an ethnicity/race other than non-Hispanic White. Meal skipping tends to be most common among adolescent females(Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,141) .
Age and sex disparities
National survey data indicate that young children (2–5 years) have the greatest number of snacks on a given day and the proportion of total energy intake contributed by snacks is highest for this age group(Reference Dunford and Popkin93,Reference Deming, Reidy and Fox119,142) . In contrast, national survey data show that the prevalence of skipping one or more main meals is highest among adolescents (39 % of males, 45 % of females) and females(Reference Kann, McManus and Harris86,141) . Having two or more snacks per d is common among adolescents who skip meals(141). Young children participate in family meals more frequently than older children(Reference Fink, Racine and Mueffelmann122). Population-based research among adolescents in Minnesota has further provided evidence that middle adolescence is a period when young individuals are particularly likely to have infrequent family meals and skip meals, with females being at greatest risk(Reference Larson, Story and Eisenberg92,Reference Neumark-Sztainer, Wall and Fulkerson116,Reference Larson, MacLehose and Fulkerson117) . Among the 2540 young individuals who were surveyed in the 2009–2010 school year, only 37 % of high school students and 36 % of females reported eating each main meal (breakfast, lunch, dinner) on five or more days a week as compared with 45 % of middle school students and 46 % of males(Reference Larson, Story and Eisenberg92). Likewise, the Minnesota survey data suggest that high school students tend to obtain meals and late-night snacks from fast food restaurants more often than middle school students(Reference Larson, Story and Eisenberg92,Reference Larson, Hannan and Fulkerson112) . National survey data show that food and beverages obtained from fast food restaurants contribute more energy to the diets of adolescents compared with younger children and adolescent males have higher daily energy intake from fast food compared with females(Reference Rehm and Drewnowski120,Reference Vikraman, Fryar and Ogden123,Reference Powell, Nguyen and Han125) . The likelihood of eating at a restaurant on a given day does not differ between younger (2–5 years) and older (6–11 years) children(Reference Powell, Nguyen and Han125).
Socio-economic and ethnic/racial disparities
Several studies on SES and ethnic/racial differences in eating patterns have focused on adolescent populations(Reference Cutler, Flood and Hannan41,Reference Kann, McManus and Harris47,Reference Arcan, Larson and Bauer49,Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Larson, Hannan and Fulkerson112) , but a growing number of studies have also assessed patterns among younger children(Reference Guerrero, Ponce and Chung77,Reference de Hoog, Kleinman and Gillman82,Reference Guerrero and Chung94,Reference Vikraman, Fryar and Ogden123-Reference Powell, Nguyen and Han125) . Despite evidence of some overall secular improvement in the frequency of eating main meals, national survey data and Minnesota survey data similarly show that skipping breakfast occurs more often among adolescents from low-SES backgrounds and those who identify as non-Hispanic Black or Native American(Reference Kann, McManus and Harris47,Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Powell, Nguyen and Han125,143,144) . Secular trend data also show that significant decreases in the frequency of eating food from fast food restaurants have occurred among most groups of Minnesota adolescents but not among those from the lowest-SES backgrounds and young individuals who identify as non-Hispanic Black or Native American(Reference Larson, Hannan and Fulkerson112). Likewise, among adolescents in Minnesota, secular trend data showed that weekly family meal frequency decreased from 4·0 times in 1999 to 3·6 times in 2010 among adolescents from the lowest-SES backgrounds and conversely increased from 4·2 times in 1999 to 4·5 times in 2010 among adolescents from the high-middle-SES group(Reference Neumark-Sztainer, Wall and Fulkerson116). The results of this study also showed a secular decrease in family meal frequency among adolescents of Asian race(Reference Neumark-Sztainer, Wall and Fulkerson116), but findings in regards to ethnic/racial disparities in family meals have been mixed across other studies(Reference Ranjit, Evans and Springer52,Reference Larson, MacLehose and Fulkerson117,Reference Larson, Eisenberg and Berge118) .
One study on ethnic/racial disparities among 15 902 preschool-aged and school-aged children (2–11 years) in California found that low-income children were less likely to have consumed food from a fast food restaurant in the past week and evidence that Latino children and Asian children were more likely than non-Hispanic White children to consume food from a fast food restaurant(Reference Guerrero and Chung94). Preschool-age Latino and non-Hispanic Black children born in Massachusetts were found to more often consume food from a fast food restaurant in another study(Reference de Hoog, Kleinman and Gillman82). In regards to family meals patterns, a study among 1134 urban households with young children showed that preschool-age children (2–5 years) of non-Hispanic White race had more frequent breakfast family meals compared with non-Hispanic Black children and non-Hispanic multiracial children. However, among the young urban children, no ethnic/racial differences were observed in the frequency of total family meals or eating together as a family at lunch or dinner(Reference Berge, Truesdale and Sherwood115). Only one other study addressing disparities in family meals among young children (up to age 4 years) was identified(Reference Taveras, Gillman and Kleinman97). This cross-sectional analysis of data collected from a prospective cohort conversely found that Black children ate fewer meals together with their family as compared with White and Hispanic children(Reference Taveras, Gillman and Kleinman97).
Problematic feeding practices
Demographic patterns in the feeding practices of parents and other caregivers probably also contribute to disparities in dietary quality among young individuals. Recommendations for the promotion of healthy eating patterns include the use of developmentally appropriate feeding practices across the life course from early childhood to adolescence(Reference Shloim, Edelson and Martin145-Reference O’Connor, Masse and Tu148). It is important that caregivers are responsive to the hunger and satiety cues of their children, make healthy foods available and accessible at home, eat meals together with their children (see above discussion of family meals) and model the consumption of healthy foods(Reference Shloim, Edelson and Martin145,Reference O’Connor, Masse and Tu148) . Few studies to date have addressed rural–urban differences or the demographic patterning of feeding practices(Reference Loth, Fulkerson and Neumark-Sztainer137).
Recent research on disparities in the use of feeding practices has addressed parental control over feeding, the types of food made available at home, and parental modelling of healthy food choices among young children(Reference Weatherspoon, Venkatesh and Horodynski65,Reference Taveras, Gillman and Kleinman97,Reference Berge, Tate and Trofholz126,Reference Huang, Parks and Kumanyika130,Reference Gaffney, Brito and Kitsantas149) as well as older children and adolescents (Table 2)(Reference Ranjit, Evans and Springer52,Reference Masters, Stanek Krogstrand and Eskridge113,Reference Larson, Eisenberg and Berge118,Reference Ruzicka, Darling and Fahrenkamp127-Reference Huang, Parks and Kumanyika130,Reference Loth, MacLehose and Larson150) . This research evidence is based on eight cross-sectional analyses(Reference Ranjit, Evans and Springer52,Reference Weatherspoon, Venkatesh and Horodynski65,Reference Larson, Eisenberg and Berge118,Reference Berge, Tate and Trofholz126-Reference Huang, Parks and Kumanyika130) and one longitudinal analysis(Reference Taveras, Gillman and Kleinman97); five studies represented local/regional populations(Reference Ranjit, Evans and Springer52,Reference Taveras, Gillman and Kleinman97,Reference Larson, Eisenberg and Berge118,Reference Loth, MacLehose and Fulkerson128,Reference Ding, Sallis and Norman129) and four studies involved a convenience sample(Reference Weatherspoon, Venkatesh and Horodynski65,Reference Berge, Tate and Trofholz126,Reference Ruzicka, Darling and Fahrenkamp127,Reference Huang, Parks and Kumanyika130) (Table 2). The research studies have used brief survey and interview tools to assess feeding practices with much variation across studies regarding the number of practices assessed and the measures used to assess specific practices.
The one longitudinal study of young children collected data on feeding practices for 1343 White, 355 Black, and 128 Hispanic mother and child pairs using in-person interviews and mailed questionnaires(Reference Taveras, Gillman and Kleinman97). Multiple assessments were conducted over the course of development from the prenatal period up to 4 years of age(Reference Taveras, Gillman and Kleinman97). Analysis of these data showed that Black and Hispanic children were more likely than White children to have experienced maternal control over feeding as defined by the restriction of energy-dense food options and pressuring children to eat(Reference Taveras, Gillman and Kleinman97). Few studies have addressed parental control over the feeding of adolescents; however, existing evidence for young children and for adolescents suggests that controlling practices are more often used by parents who identify with ethnic/racial minority groups (Hispanic, Asian, Black), parents with less than a high school education and parents with low household incomes(Reference Weatherspoon, Venkatesh and Horodynski65,Reference Berge, Tate and Trofholz126-Reference Loth, MacLehose and Fulkerson128,Reference Huang, Parks and Kumanyika130) . The existing research likewise indicates that young individuals in ethnic/racial minority subgroups and those from lower-SES households tend to have fewer healthful foods available at home than their peers but similar or more limited access to less-healthful foods at home(Reference Ranjit, Evans and Springer52,Reference Larson, Eisenberg and Berge118,Reference Ding, Sallis and Norman129,Reference Loth, MacLehose and Larson150) .
Disordered eating behaviours
A small number of studies have also examined whether there are sex and ethnic/racial disparities in the prevalence of using unhealthy weight-control behaviours and binge eating (Table 3). The existing evidence on unhealthy weight-control behaviours that is summarised here is based on five cross-sectional analyses(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131,Reference Eaton, Kann and Kinchen133-Reference Rodgers, Peterson and Hunt135) and one study of secular trends over time(Reference Neumark-Sztainer, Wall and Larson132); one study was nationally representative(Reference Eaton, Kann and Kinchen133), one represented a statewide sample of secondary students in Massachusetts(Reference Gonsalves, Hawk and Goodenow131), two represented secondary students in urban areas of Minnesota(Reference Arcan, Larson and Bauer49,Reference Neumark-Sztainer, Wall and Larson132) and two studies were conducted among students enrolled at baseline of an overweight prevention study in Massachusetts(Reference Austin, Spadano-Gasbarro and Greaney134,Reference Rodgers, Peterson and Hunt135) . All six of these studies used brief survey tools to assess the use of dieting and three to nine specific unhealthy weight-control behaviours. Four studies focused on unhealthy weight-control behaviours in the past 30 d(Reference Gonsalves, Hawk and Goodenow131,Reference Eaton, Kann and Kinchen133-Reference Rodgers, Peterson and Hunt135) and two studies focused on use in the past year(Reference Arcan, Larson and Bauer49,Reference Neumark-Sztainer, Wall and Larson132) . Evidence regarding disparities in binge eating was recently summarised as part of an integrative literature review(Reference Jennings, Kelly-Weeder and Wolfe138) that described six relevant USA-based studies and one more recent study(Reference Lee-Winn, Reinblatt and Mojtabai136) was additionally identified; these studies have made use of heterogeneous measurement tools.
There were no studies identified that had examined rural–urban differences in disordered eating and the existing research focuses solely on adolescent populations. Most studies that have examined sex differences(Reference Gonsalves, Hawk and Goodenow131-Reference Austin, Spadano-Gasbarro and Greaney134) found the prevalence of disordered eating to be higher among females than males. Additionally, there is mixed evidence regarding differences in the prevalence of disordered eating between ethnic/racial groups(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131-Reference Rodgers, Peterson and Hunt135,Reference Jennings, Kelly-Weeder and Wolfe138) .
Ethnic/racial disparities
Studies that have identified ethnic/racial differences in disordered eating have, in general, found evidence that the prevalence is lower among non-Hispanic White adolescents than other groups(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131,Reference Eaton, Kann and Kinchen133,Reference Austin, Spadano-Gasbarro and Greaney134,Reference Jennings, Kelly-Weeder and Wolfe138) . For example, a large survey of 16 978 middle school students in Massachusetts asked students to report on vomiting, use of laxatives and use of diet pills in the past month to lose weight(Reference Austin, Spadano-Gasbarro and Greaney134). The prevalence of using any of these extreme weight-control behaviours was elevated two to ten times in most ethnic/racial groups relative to reported use by non-Hispanic White students and observed differences remained after accounting for weight status, self-perceived weight status and neighbourhood poverty(Reference Austin, Spadano-Gasbarro and Greaney134). Similarly, a recent literature review identified two studies of binge eating that have found a higher prevalence among Hispanic adolescents, one study that found evidence of a higher prevalence among Black adolescents and one other study that found binge eating to be more common among Native American adolescents; three studies found no evidence of ethnic/racial disparities(Reference Jennings, Kelly-Weeder and Wolfe138). Additional research further suggests that ethnic/racial differences in binge eating may vary across symptoms. One illustrative study found that Hispanic adolescents may be more afraid of weight gain while binge eating than non-Hispanic Black adolescents(Reference Lee-Winn, Reinblatt and Mojtabai136). The interpretation of these studies and others that have not found strong evidence of ethnic/racial disparities should consider that across studies there was variability in the composition of adolescents enrolled, the types of unhealthy weight-control behaviours and characteristics of binge eating explored, and also the measurement tools and definitions established to determine prevalence(Reference Jennings, Kelly-Weeder and Wolfe138).
There was also variability across the studies regarding accounting for ethnic/racial group differences in weight status. As young individuals who are at a BMI categorised as overweight/obese are more likely to engage in unhealthy weight-control behaviours(Reference Neumark-Sztainer, Story and Hannan151), differences in weight status across groups could at least in part explain observed disparities in disordered eating. Among young individuals at an overweight BMI, Rodgers et al. found that non-Hispanic Black and Latino males were more likely to report disordered eating than White males but observed no ethnic/racial differences among overweight females(Reference Rodgers, Peterson and Hunt135). Further, none of the studies addressed the excess burden of food insecurity among ethnic/racial minority groups and the potential contribution of food insecurity to observed disparities in disordered eating(Reference Tester, Lang and Laraia152,Reference Bruening, MacLehose and Loth153) .
Discussion
The present review described recent evidence of disparities in nutritional problems among US child and adolescent populations (2–19 years) according to age, sex, markers of SES, ethnicity/race and geographic location. The findings identified adolescent females, young individuals from lower-SES households and young individuals of non-Hispanic Black ethnicity/race as particularly vulnerable populations for whom targeted strategies should be developed to address evidence of increased risk in regards to multiple aspects of nutritional wellbeing. There is an urgent need for research to build a more in-depth understanding of these disparities, including the contributions of environmental factors and food insecurity, and to fill a large gap in evidence regarding the potential existence of rural–urban differences. Nutrition and health professionals can use the existing evidence in advising the development of programmes and policies, and to design studies addressing the limitations of this scientific knowledge base. The existing evidence has several limitations relating to the accuracy of self-reported dietary data; the need for standard measures and definitions of disordered eating; the focus on individual dietary components v. patterns; the complexities of categorising SES, ethnicity/race and rural and urban areas; and the cross-sectional nature of most research designs. It will be critical for future studies to fulfill standing research needs in order to better inform public health improvement strategies and promote equity in nutritional health.
Adolescent females were identified by the present review as a target population for interventions based on evidence showing a high prevalence of multiple nutritional problems within this demographic subgroup. Adolescents as a group had lower overall diet quality scores than preschool-aged children and higher intake of sugar-sweetened beverages than children at earlier stages of development(Reference Gu and Tucker40,Reference Wang, Vine and Hsiao53,Reference Rosinger, Herrick and Gahche88,Reference Dunford and Popkin93,Reference Poti and Popkin111) . Female adolescents were also more likely than other demographic groups to report poor intake of milk, grains, and meats and beans(Reference Krebs-Smith, Guenther and Subar2,Reference Wallace, Reider and Fulgoni45) . The life stage of adolescence is a time when young individuals, especially females, are most likely to have infrequent family meals and to skip meals(Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Neumark-Sztainer, Wall and Fulkerson116) . Further, most studies of disordered eating among adolescents have found that prevalences of unhealthy weight-control behaviours and binge eating are higher among females than males(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131-Reference Eaton, Kann and Kinchen133,Reference Lee-Winn, Reinblatt and Mojtabai136) . These findings collectively suggest the potential benefit of integrating content that addresses the importance of consuming nutrient-dense foods and avoiding disordered eating behaviours as part of interventions for adolescent females. The school-based programme New Moves is an example of such an intervention that was designed for adolescent females and guided by the philosophy that if girls feel good about their bodies they will want to take care of their bodies through healthy eating, physical activity and self-acceptance(Reference Neumark-Sztainer, Flattum and Story154,Reference Neumark-Sztainer, Friend and Flattum155) . Accordingly, the objectives of the New Moves Program were designed to address the nutrition problems of poor diet (i.e. eat at least five servings of fruit and vegetables each day, limit pop and other sweetened beverages), unhealthy meal and snack patterns (i.e. eat breakfast every day, choose fruits and vegetables for snacks, pay attention to portion size and to your body’s signs of hunger and fullness), and disordered eating patterns (i.e. avoid dieting and unhealthy weight-control practices) along with body dissatisfaction (i.e. focus on your positive traits)(Reference Neumark-Sztainer, Flattum and Story154). A 9-month follow-up evaluation of the programme among a sample of ethnically/racially diverse adolescent females demonstrated success by increasing the use of portion-control behaviours, decreasing the use of unhealthy weight-control behaviours, and improving body image(Reference Neumark-Sztainer, Friend and Flattum155).
Young individuals from low-SES households were likewise identified as a target population for interventions based on evidence showing a high prevalence of multiple nutritional problems among those who depend on parents/caregivers with limited formal education and income. Overall diet quality and, in particular, intakes of milk, fruit, vegetables, whole grains, Ca and vitamin D tend to be poorer among young individuals from low-SES households(Reference Kirkpatrick, Dodd and Reedy1,Reference Gu and Tucker40,Reference Wallace, Reider and Fulgoni45,Reference Eagle, Sheetz and Gurm54,Reference Jun, Catellier and Eldridge62,Reference Guerrero and Chung94) . The diets of young individuals from low-SES households are also adversely impacted by having higher intakes of sugar-sweetened beverages and added sugars than their peers with more household resources(Reference Jun, Catellier and Eldridge62,Reference Guerrero and Chung94,Reference Wang, Guglielmo and Welsh98) . Studies of eating behaviour have further shown that young individuals from low-SES households tend to skip breakfast and purchase food from a fast food restaurant more often than their peers(Reference Larson, Story and Eisenberg92,Reference Guerrero and Chung94,Reference Larson, Hannan and Fulkerson112) . The home food environments of young individuals from low-SES households have been found to provide less access to healthy foods and to be characterised by more parental control over feeding when compared with the environments of young individuals with more household resources(Reference Ruzicka, Darling and Fahrenkamp127-Reference Ding, Sallis and Norman129). In addition to these challenges, there is evidence that weight-related concerns and disordered eating are prevalent among paediatric populations in low-income communities(Reference Neumark-Sztainer, Wall and Larson132,Reference Tester, Lang and Laraia152,Reference West, Goldschmidt and Mason156-Reference Najjar, Jacob and Evangelista158) . The extent to which food insecurity and parental control over feeding may contribute to the development of disordered eating patterns among lower-income households is an area of ongoing research. Given the elevated prevalence of food insecurity among low-SES households, it may accordingly be important to assess for various weight-related problems (for example, binge eating, unhealthy weight-control behaviours) when intervening with young individuals that have limited household resources(Reference Neumark-Sztainer, Wall and Larson132,Reference Buckingham-Howes, Armstrong and Pejsa-Reitz157,Reference Coleman-Jensen, Rabbitt and Gregory159) . It is also important that programmes and policies addressing food insecurity are designed to provide diverse young individuals with access to nutrient-dense foods. Research studies evaluating the nutritional quality of foods provided to children through weekend backpack programmes have identified such opportunities for improvement (for example, providing more beans, vegetables and essential fatty acids)(Reference Byker and Smith160). More in-depth discussion of disparities in the prevalence of food insecurity is provided below in line with the likely relevance of this public health problem for feeding practices and disordered eating as well as dietary intake and meal and snack patterns.
Several of the studies included in the present review identified young individuals of non-Hispanic Black ethnicity/race as a population group bearing an excessive burden of one or more nutritional problems. Across studies there is consistent evidence that non-Hispanic Black children and adolescents have diets of poorer overall quality and higher intakes of sugar-sweetened beverages and Na from snacks when compared with young individuals of other ethnic/racial backgrounds(Reference Kirkpatrick, Dodd and Reedy1,Reference Gu and Tucker40,Reference Wallace, Reider and Fulgoni45,Reference Kann, McManus and Harris47,Reference Dodd, Briefel and Cabili51,Reference Ranjit, Evans and Springer52,Reference Papanikolaou, Brooks and Reider55,Reference Kenney, Wang and Iannotti57,Reference Welker, Jacquier and Catellier59,Reference Kann, McManus and Harris86-Reference Rosinger, Herrick and Gahche88,Reference Dunford and Popkin93,Reference Wang, Guglielmo and Welsh98) . Young individuals of non-Hispanic Black ethnicity/race also tend to skip breakfast and purchase food from fast food restaurants more often than young individuals of other ethnic/racial backgrounds(Reference Kann, McManus and Harris86,Reference Larson, Story and Eisenberg92,Reference Larson, Hannan and Fulkerson112) . When compared with non-Hispanic White children and adolescents, young individuals of non-Hispanic Black ethnicity/race are more likely to experience parental control over feeding (for example, restriction of energy-dense food options, pressuring to eat) and have fewer healthful foods available to them at home(Reference Ranjit, Evans and Springer52,Reference Taveras, Gillman and Kleinman97,Reference Loth, MacLehose and Fulkerson128) . Although the evidence is mixed with regard to ethnic/racial disparities in the prevalence of binge eating, there is further evidence that adolescents of non-Hispanic Black ethnicity/race are more likely than non-Hispanic White adolescents to use extreme weight-control behaviours and this relationship was particularly evident among male adolescents at an overweight BMI(Reference Gonsalves, Hawk and Goodenow131,Reference Austin, Spadano-Gasbarro and Greaney134,Reference Rodgers, Peterson and Hunt135,Reference Jennings, Kelly-Weeder and Wolfe138) . There is a great need for strategies to address the collective burden of these nutritional problems that are disparately making an impact on non-Hispanic Black young individuals. It is likely that a combination of strategies addressing the root causes of the identified nutritional problems will be most effective in working towards health equity. For example, recent reports have identified the need for strong policies to stop the targeted marketing of sugary drinks and fast foods to individuals of non-Hispanic Black ethnicity/race(Reference Fleming-Milici and Harris161-Reference Harris, Schwartz and Munsell164). In alignment with evidence that food-insecure parents are more likely to use controlling or other compensatory feeding practices(Reference Bauer, MacLehose and Loth165-Reference Feinberg, Kavanagh and Young167), there is also a pressing need to address the excess burden of food insecurity among non-Hispanic Black households and disseminate culturally relevant health promotion messages to parents(Reference Coleman-Jensen, Rabbitt and Gregory159).
Nutrition and health professionals can use the existing evidence in advising the development and monitoring of programmes and policies. In order to promote equity, it is imperative that efforts are made to ensure that the reach of programmes and policies extends to population subgroups with elevated rates of nutritional problems. Further, it is critical that nutrition education messages, programme materials and programme activities be tested to ensure they are culturally and developmentally appropriate for vulnerable population subgroups. There is also a need to monitor and provide technical support as appropriate to ensure full implementation of nutrition policies in settings that serve vulnerable subgroups of children and adolescents. The results of the present literature review demonstrated that nutrition assistance programmes (i.e. programmes designed to increase food security and reduce hunger through access to affordable, healthy food and nutrition education), are vital in addressing socio-economic disparities in nutritional problems; specifically, the WIC Program was found to mitigate income-related disparities in milk intake among young children and the National School Lunch Program (NSLP) was found to likewise mitigate disparities in fruit and vegetable intake for school-age children(Reference Longacre, Drake and Titus48,Reference Jun, Catellier and Eldridge62,Reference Vercammen, Moran and Zatz66,Reference Watowicz and Taylor79) . Ongoing funding and continuous efforts to monitor the reach of nutrition assistance programmes are clearly essential. In addition, the results of the present literature review demonstrated there may be opportunities as part of these programmes to address nutritional problems that are elevated among programme participants (for example, higher risk of excessive Na intake among WIC participants)(Reference Jun, Catellier and Eldridge62). It is similarly important that evidence-based practices be addressed in refining administrative requirements for settings that administer these programmes. For example, secondary schools that offer the NSLP might be required to address elevated rates of disordered eating among adolescent females as part of nutrition education(Reference Arcan, Larson and Bauer49,Reference Gonsalves, Hawk and Goodenow131-Reference Eaton, Kann and Kinchen133,Reference Lee-Winn, Reinblatt and Mojtabai136) .
An extensive and growing body of research has established that there are disparities in food insecurity, participation in nutrition assistance programmes, and several social and physical environmental factors that influence nutritional health and dietary behaviours(Reference Coleman-Jensen, Rabbitt and Gregory159,Reference Larson and Story168) . The research literature on disparities in food security indicates that US children who are born in the country are at lower risk for experiencing household food security when compared with foreign-born children(Reference Arteaga, Potochnick and Parsons169). National surveillance data additionally indicate that rates of experiencing food insecurity are higher than the US national average (11 % of households in December 2018) for the following groups: households with incomes near or below the federal poverty line (29 %), all households with children (14 %) and particularly households with children headed by single women (28 %) or single men (16 %), Black- and Hispanic-headed households (21 and 16 %) and households in principal cities of metropolitan areas (13 %)(Reference Coleman-Jensen, Rabbitt and Gregory159). The prevalence of food insecurity was not found to be significantly higher than the national average in rural non-metropolitan areas (13 %) but was elevated in comparison with the rate in suburbs/exurbs and other metropolitan areas outside principal cities (9 %)(Reference Coleman-Jensen, Rabbitt and Gregory159). The prevalence of severe food insecurity, involving the reduction of food intake and disrupted eating patterns for one or more household members, was similarly patterned for US households(Reference Coleman-Jensen, Rabbitt and Gregory159).
Along with this evidence of disparities in food insecurity, there are data that indicate that gaps exist in access to nutrition assistance programmes and environmental supports for healthy eating. Just over half of the US households (56 %) that were food insecure in 2018 reported participating in one or more of the three largest federal nutrition assistance programmes (Supplemental Nutrition Assistance Program, WIC, NSLP) in the previous month(Reference Coleman-Jensen, Rabbitt and Gregory159). Although food-insecure households may also obtain food from emergency providers in their local community, these data suggest that there are gaps in meeting the needs of many households with children. More specific data on the contributions of major nutrition assistance programmes indicate the Supplemental Nutrition Assistance Program (SNAP) provided assistance to 41 % of food-insecure households, children in 28 % of food-insecure households were provided with free or reduced-price meals through the NSLP, and women or children in 8 % of food-insecure households received food vouchers from the WIC Program(Reference Coleman-Jensen, Rabbitt and Gregory159). National data further indicate that nutrition assistance programmes contribute to the prevention of food insecurity for many low-income households(170). A large share of the children and adolescents who benefit from the NSLP and School Breakfast Program are children from low-income households who are provided with free or reduced-price meals. Over two-thirds of participants in the NSLP received a free lunch and another 6 % received a reduced-price lunch in 2018(170). Likewise, in 2018, 80 % of participants in the School Breakfast Program received a free breakfast and another 5 % received a reduced-price meal(170). Social and physical environmental factors that probably play roles in driving disparities in nutritional problems include unequal local access to healthy food, the targeted marketing of energy-dense food products, resources to prepare food at home, and cultural pressures around eating, body size and body shape. Additional research is, however, needed to clarify the contributions of food insecurity and various environmental factors to disparities, and establish that efforts to improve environments do actually lead to improvements in health equity without having unintended consequences. This research should be guided by a framework that highlights the potential for programmes and policies to have unequal impacts and recognises the importance of ongoing evaluation to identify gaps in implementation and to drive improvements.
To advance the field, several other areas for future research should also be given attention:
-
(a) There is a need to better understand how problematic eating behaviours and dietary patterns may cluster among population groups. Much of the existing research on nutritional disparities has focused on individual dietary components v. patterns and separately addressed multiple, related dietary behaviours. Research that has alternatively examined patterns in dietary behaviours or ranked overall dietary intake quality has been informative and may serve as a useful model for advancing science(Reference Gu and Tucker40). For example, Gu & Tucker(Reference Gu and Tucker40) calculated a HEI-2010 score for all child and adolescent participants in the National Health and Nutrition Examination Survey over the years 1999 to 2012(Reference Gu and Tucker40). The HEI-2010 allowed for examining overall dietary quality with attention to ensuring adequate intake of fruit, vegetables, whole grains, dairy products, protein foods and fatty acids as well as moderating intake of refined grains, Na and ‘empty calories’. Results of the Gu & Tucker(Reference Gu and Tucker40) analysis clarified the need for interventions to address the overall lower dietary quality of young individuals that identify as non-Hispanic Black and those who are eligible for public assistance.
-
(b) Consistent methods for identifying rural and urban areas are needed and should be reported in publications to build understanding of geographic disparities in dietary intake, meal and snack patterns, feeding practices and disordered eating. A prior review of rural–urban disparities in paediatric diet and physical activity patterns described eight different methods of classifying geographic areas(Reference McCormack and Meendering171). There is a need for consensus on the use of a single nuanced definition of rural to allow for greater comparability across studies.
-
(c) Attention to variability in dietary patterns and the validity of self-reported data should receive greater attention in the design of future studies. Most existing studies of disparities have relied on reports of dietary intake at a single point in time. Many studies have made use of strong assessment methods, such as 24 h dietary recalls, and the findings produced from these studies have identified important cross-sectional differences and disparate secular trends. However, little is known regarding how disparities track longitudinally over time to allow for understanding whether trajectories of dietary patterns over the course of development may systematically differ across groups. Only a few studies have examined issues such as how disparities in intake may differ by season (for example, during the school year v. summer)(Reference Wang, Vine and Hsiao53) or for different food subgroups (for example, dark green v. starchy vegetables)(Reference Kirkpatrick, Dodd and Reedy1). It may be informative for more future studies to report on variability in diet as well as more objective measures (i.e. biomarkers such as serum carotenoids) of long-term intake patterns(Reference Woodside, Draper and Lloyd172).
-
(d) Finally, the need for additional research to address disparities in disordered eating behaviours is noteworthy. The comparability of findings across existing studies of disparities is currently limited by the use of inconsistent definitions. Future studies should pay greater attention to the selection of comparable measures and recognising problematic behaviours that occur before middle adolescence. The few identified studies of disordered eating behaviours among middle school students have indicated that it should be a priority to examine disparities among large, population-based samples of preadolescents and early adolescents(Reference Gonsalves, Hawk and Goodenow131,Reference Neumark-Sztainer, Wall and Larson132,Reference Rodgers, Peterson and Hunt135) .
Review limitations
This narrative review of literature had several limitations. It is likely that some relevant literature was missed as the search was limited to peer-reviewed research published within the past decade. There may be value in additionally reviewing reports outside the peer-reviewed literature to address potential publication bias and evaluating patterns in nutritional disparities over a longer period of time. Further, in contrast to most systematic reviews of the literature, the present review did not use a formal process to evaluate the quality of included studies. The literature search focused on the nutritional problems of poor dietary intake (underconsumed and overconsumed components), problematic eating patterns and feeding practices, and disordered eating among US paediatric populations. In developing research plans, it will also be important for reviews to examine physical signs of malnutrition, upstream determinants of disparities in nutritional problems (for example, local food access) and disparities across sexual orientation groups(Reference Calzo, Blashill and Brown173). Further, it will be important for future reviews to examine these same issues with a broader international perspective.
Conclusion
This review provides important information on disparities in nutritional problems among US child and adolescent populations. The findings may be of international interest as many countries across the globe are working to address nutritional disparities among their paediatric populations(Reference Chzhen, Moor and Pickett174-Reference Corvalán, Garmendia and Jones-Smith176). However, there is substantial cross-national variation in the magnitude and direction of disparities that must be attended to in developing responsive programmes and policies(Reference Chzhen, Moor and Pickett174-Reference Corvalán, Garmendia and Jones-Smith176). Whereas the gradient of certain nutritional disparities has been increasing in the USA in recent years, other countries have maintained stable patterns of differences or made progress towards greater equity(Reference Chzhen, Moor and Pickett174). Disseminating information on patterns of US disparities may help to guide research based on cross-national comparisons and is critical to building broad support for US programmes and policies. Identified areas of need for future research in US populations include building a greater understanding of how problematic eating behaviours and dietary patterns may cluster among population groups, developing consistent methods for the identification of rural and urban areas, paying more attention to variability in dietary patterns and the reliability of self-reported dietary data, and developing standard methods for identifying disordered eating that are appropriate for epidemiological studies.
Acknowledgements
The present review was supported in part by the Robert Wood Johnson Foundation Healthy Eating Research Program. The Healthy Eating Research Program had no role in identifying manuscripts for the review or the writing of this article.
N. I. L. identified the scientific manuscripts for inclusion in the present review and drafted the article.
There are no conflicts of interest.



