


Malnutrition affects over 300 million school-aged children throughout the developing world( 1 ). Children who are undernourished are susceptible to decelerated growth rates, with stunting, multiple micronutrient deficiencies, anaemia (particularly Fe-deficiency anaemia), diminished cognitive function, poor school performance, and increased morbidity and mortality( Reference Caulfield, de Onis and Blössner 2 – Reference Eilander, Muthayya and van der Knaap 6 ). Poor dietary quality due to limited intake of a variety of animal source foods (ASF), including milk, is a contributing factor for malnutrition and multiple micronutrient deficiencies among many of these children( Reference Murphy, Gewa and Liang 7 ). Micronutrient deficiencies, particularly Fe, Zn, iodine and vitamin B12 deficiencies, are of particular concern. Micronutrient deficiencies occur in part due to consumption of diets that lack ASF and consist mainly of staple foods such as cereals and legumes that are devoid of vitamin B12 and have high fibre and phytate content, resulting in impaired bioavailability of micronutrients such as Fe and Zn( Reference Hambidge, Miller and Westcott 8 – Reference Watanabe 13 ). In addition, repeated intestinal infections and parasites with resultant diarrhoea contribute to malabsorption, blood loss, malnutrition, and impaired growth and development( Reference Guerrant, Oriá and Moore 14 ).
Fe deficiency with or without anaemia is among the most prevalent and devastating deficiencies in developing countries and results in retarded cognitive and motor development, growth, immune function and physical activity( Reference Stoltzfus 15 – Reference Lozoff, Jimenez and Wolf 18 ). The major causes of Fe deficiency include poor bioavailability of Fe in plant-based diets, inadequate meat consumption (which inherently contains readily absorbable haem Fe), and blood loss due to parasitic infections, particularly hookworm infections( Reference Hunt 11 , Reference Zimmermann and Hurrell 19 , Reference Stoltzfus, Chwaya and Tielsch 20 ). Vitamin B12 deficiency occurs in populations consuming primarily plant-based diets and is associated with delayed development, lethargy, anaemia and poor school performance in children and adolescents( Reference Black 5 , Reference Walker, O'Fallon and Nelson 21 – Reference Louwman, van Dusseldorp and van de Vijver 25 ). Zn deficiency is associated with the impairment of multiple biological functions, including protein synthesis, growth and cell-mediated immunity, and is associated with delays in cognitive development, lower school scores and lower levels of physical activity( Reference Black 26 – Reference Bentley, Caulfield and Ram 28 ). Iodine deficiency of all degrees of severity also contributes to cognitive impairment( Reference Zimmermann, Jooste and Pandav 29 ).
Poor health and nutritional deficiencies affect school performance and impair long-term cognitive development in primary school children, with undernourished children demonstrating lower school attendance, lower school performance scores and more health-related problems than their well-nourished peers( Reference Lozoff, Jimenez and Wolf 18 , Reference Mukudi 30 – Reference Florence, Asbridge and Veugelers 36 ). The adverse effects of macro- and micronutrient deficiencies in infancy and childhood may not be fully reversible and may continue to affect cognitive function into the school age years and adulthood( Reference Guerrant, Oriá and Moore 14 , Reference Lozoff, Jimenez and Wolf 18 , Reference Berkman, Lescano and Gilman 37 , Reference Lukowski, Koss and Burden 38 ). However, some studies have demonstrated improvements in educational attainment and cognitive performance following adequate nutrition or catch-up growth( Reference Maluccio, Hoddinott and Behrman 39 , Reference Crookston, Penny and Alder 40 ). There have been few food-based randomised intervention studies to test the ability of ASF to improve school performance and cognitive function.
Results from the Nutrition Collaborative Research Support Program (NCRSP), an observational study carried out in Kenya, Egypt and Mexico during the mid-1980s, pointed to the need for a randomised controlled feeding intervention study to test for causal linkages between ASF and a number of functional outcomes( Reference Neumann, Bwibo and Sigman 41 ). The NCRSP study showed that diets deficient in ASF and Fe, vitamin B12 and Zn were associated with poor school performance( Reference Neumann, Bwibo and Sigman 41 ). Strong positive statistical associations were observed between children's meat intake and cognitive function, development and growth( Reference Neumann, McDonald and Sigman 42 ). These finding stimulated the Child Nutrition Project (CNP) study, the cluster-randomised feeding intervention trial reported herein, to test for causal relationships between intake of ASF and improvement in health, cognition, school performance and development in schoolchildren( Reference Neumann, Bwibo and Murphy 43 ). Cluster randomisation was selected, as it would have been logistically impossible to prepare and deliver different feedings within the same school or to prepare and deliver feedings to individual households.
The present study evaluated the effect of the CNP feeding intervention trial on school performance in 360 Kenyan schoolchildren using the changes in end-term test scores over five consecutive terms (19 months). It was hypothesised that children supplemented with ASF would show greater improvement in term-end school test scores than those who received plant-based supplements or the control group.
Experimental methods
In the present study, data collected in the CNP cluster-randomised, controlled school feeding intervention study conducted from 1998 to 2001 in rural Kenya were used. No primary school feeding programmes existed in the study area. In the CNP study, two cohorts were enrolled exactly 1 year apart as the schools were closed due to a prolonged teachers' strike during the cohort I study and also because of a prolonged drought. Children in each cohort were given feedings at school and studied for three school terms per year over 2 years for a total of 9 months/year: cohort I from 1998 to 2000 and cohort II from 1999 to 2001. Only data obtained for cohort II are reported herein, since complete end-term test score information was not readily available for cohort I.
Study location
The CNP study was carried out in central Kenya's rural Embu District, Eastern Province, about 193 km northeast of Nairobi. Subsistence farming on one- or two-acre farms is the primary source of foods for households in this area. Detailed descriptions of the study area have been published previously( Reference Neumann, Bwibo and Murphy 43 ). This area was chosen because it had a sufficient number of rural schools, each separated by several kilometres, and due to its location in the Embu region where a cadre of highly trained personnel had carried out measurements previously and had excellent rapport with the community members( Reference Neumann, Bwibo and Sigman 41 ).
Sampling
Of the eighteen schools in an Embu subregion with 2600 households, twelve were chosen based on their size, location and accessibility for food delivery and ongoing assessments as explained in detail previously( Reference Neumann, Bwibo and Murphy 43 ). Schools were randomised into one of the three feeding groups or the Control group via a slightly restricted randomisation process such that the three large schools with more than one standard I classroom could not be randomised to the same feeding condition.
All the children enrolled in standard (grade) I (mean age 7·1 (sd 0·8) years) in September 1999 were considered for inclusion in the cohort II sample of the CNP study. Of the 635 children enrolled in standard I classes in September 1999, data from 216 children who had been held back from the previous year and were repeating standard I (and thus were already participating in the second year of the cohort I study) were excluded from the analysis. The other 419 children who were enrolled in standard I classes for the first time were considered for inclusion in the cohort II sample. Of these children, thirteen did not have data on term test scores available either due to absence from schools on the dates of test administration or failure to complete the tests. An additional forty-six standard I children aged above 9 years were excluded to compare children at similar physical and mental stages. Children excluded from the data collection process were fed along with their classmates when they were present at school. Data from 360 children were included in the present analysis (Fig. 1).
Fig. 1 Study flowchart.
Snack design, preparation and delivery
Children in the feeding group schools were given a mid-morning snack. The Control group did not receive intervention feedings, but participated in all other aspects of the study. At the end of the study, the families in the Control group received one goat per household plus several male goats for the entire Control group.
Snacks were based on a local plant-based stew (githeri) with either added meat or a glass of whole ultra-heat-treated milk. The Plain Githeri group (n 99) received githeri prepared with 3·8 g of additional vegetable oil (Kimbo, Unilever, East African Industries), later found to have been fortified with 70 μg retinol/g throughout the study period. The Milk group (n 105) received githeri plus a glass (250 ml) of ultra-heat-treated whole cows' milk. The Meat group (n 67) received githeri mixed with 85 g of ground beef containing 10–12 % fat obtained frozen from a well-recognised, respected commercial supplier (Farmer's Choice). The Control group (n 89) received no supplemental feeding at school.
The three snacks were isoenergetic (approximately 1300 kJ/feeding) (Table 1). Snacks met approximately one-fifth of the recommended energy intake for children aged 6–9 years( Reference Otten, Hellwig and Meyers 44 ). Iodised salt was used. Stringent quality control measures were monitored by the analysis of the nutrient content of the test feedings two to three times per year. Detailed descriptions of the food preparation methods and quality control measures have been published previously( Reference Murphy, Gewa and Liang 7 , Reference Neumann, Bwibo and Murphy 43 , Reference Murphy, Gewa and Grillenberger 45 ).
Table 1 Nutrient content of cohort II school intervention snacks*
* Adapted with permission from Neumann et al. ( Reference Neumann, Bwibo and Murphy 43 ).
Snacks were delivered to each school and given to each child in a covered bowl labelled with their study number. A trained feeding assistant distributed the numbered bowls to each study child, observed the child during feeding, and collected and covered the bowls for measurement of leftovers in the test kitchen, by weighing solids using a beam balance and measuring the volume of milk. The adherence to consumption of the assigned snack by the children was very high; in 99·4 % of the feeding sessions, the children consumed all the food provided( Reference Gewa, Murphy and Bwibo 46 ). The feeding assistants were trained to observe the children during snack time to ensure that no sharing occurred and that spillage and unconsumed portions were recorded. If a child was absent, that child's uneaten portion was returned to the kitchen. Snacks were served at mid-morning each day when the schools were in session over a period of 19 months from September 1999 to December 2001, a total of five school terms. School terms lasted for 3 months with a 1-month break between each term. No snacks were given during school vacations or holidays.
End-term test scores
At the end of each school term, all the students in each school were tested in Arithmetic, English, Kiswahili, Mother tongue (Kiembu), Science/Agriculture, Geography/Civics/Culture/Religion, Arts/Crafts and Music. These zone-wide tests were standardised tests designed by the Kenyan Ministry of Education, with identical questions for each school. Test patterns were changed slightly from term to term by the Ministry of Education based on the curriculum. Question papers were distributed by the district and zonal offices of the Ministry of Education, and the tests were administered by the classroom teachers. The level of difficulty of the test content was increased during each term to capture new topics taught in the curriculum. For the present study, end-term test scores were collected and recorded for each child over five successive terms from September 1999 to December 2000 from records in Head Teacher's office in each school. The maximum number of points in each individual academic subject test was 50, with one point per correct answer. The maximum possible total score in all the term examinations was a sum of 350 points from tests of seven individual academic subjects. Test scores obtained in term 1 were treated as baseline scores for the study children.
Socio-economic status
Data on the socio-economic status (SES) of the participating households were collected through interviews with household heads at baseline. The details of the SES scale and items used in the scale have been published previously, and the SES scale and items were created in consultation with the Kenyan Central Bureau of Statistics, one of the best-known and highly respected statistical groups in Kenya, with input from local leaders and household members( Reference Neumann, Bwibo and Sigman 41 , Reference Neumann, Bwibo and Murphy 43 ). The scale was used in a previous study carried out in this region( Reference Neumann, Bwibo and Sigman 41 ).
Maternal literacy and educational attainment
Maternal literacy (n 305) was assessed by testing the ability of each child's mother to read and comprehend passages of text from graded local Kiembu school textbooks selected to reflect different levels of difficulty. The tests were administered in either Kiembu, the predominant local spoken language (92·9 %), or English (7·1 %), based on the participant's preference. The test score was equal to the total number of pages read aloud for which two of three questions were answered correctly. The cognitive assessment team that carried out the literacy tests consisted of three local women trained by a psychologist and child development expert, who had worked in Kenya in the NCRSP field study with the same field staff. The team was supervised by the Kenyan project psychologist who had a Master's degree and interacted frequently with the field staff, reviewed data collection techniques and helped with quality control. For quality control purposes, 10 % of the mothers were tested simultaneously by two testers. There was perfect agreement between the scores recorded by each of the testers in these cases( Reference Whaley, Sigman and Neumann 47 ). Periodically, the psychologist/child development expert travelled to Kenya to review data collection procedures and quality. Information regarding maternal school grade attainment was included in the household SES questionnaire.
School attendance
The total number of school days per term that each child attended school was recorded. Attendance information was obtained from each classroom teacher's daily records as well as from the daily intervention feeding logs maintained by the feeding assistant at each school.
Food intake
The home food intake of the children was measured through 24 h semi-quantitative recall interviews with their mothers or caretakers. At baseline, three recall interviews were conducted (each 1 week apart), and the intake values for the 3 weeks were averaged to obtain values for the baseline intake of energy and other nutrients. Subsequent recall measures were recorded every 2 months over a 16-month period. Average home food intake was calculated across the eight single post-baseline recall visits. The recalls were administered at the homes of the children by trained enumerators using household measures and samples of local foods (i.e. fruits and vegetables) to assess size. This method, energy and nutrient intake calculations, and quality control measures have been described in detail previously( Reference Murphy, Gewa and Liang 7 , Reference Neumann, Bwibo and Murphy 43 , Reference Gewa, Murphy and Neumann 48 ). For the calculation of changes in average individual nutrient intake from baseline to follow-up, home food intake data collected at follow-up and baseline and nutrient estimates associated with the different snack types at follow-up were used. Follow-up home food nutrient estimates for the study children were based on eight recalls of daily intake over a four-term period from September 1999 to December 2000.
Other covariates
Data regarding morbidity, anthropometry, children's cognitive development measured using Raven's Progressive Matrices (RPM), verbal meaning, and arithmetic tests and physical activity were collected using methods described in previous publications( Reference Neumann, Bwibo and Murphy 43 , Reference Whaley, Sigman and Neumann 47 , Reference Grillenberger, Neumann and Murphy 49 ).
Protection of human research participants
The present study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human research participants were approved by the Human Subjects Protection Committee of the University of California, Los Angeles, the Ethics Committee of the University of Nairobi, School of Medicine, and the Office of the President in Kenya. Verbal informed consent from parents and assent from children were obtained. Verbal consent was witnessed and formally recorded. The investigators also obtained community permissions via community meetings. Verbal permission was obtained from the Provincial Office of Education, the Director of the Zonal Office of Education, and the Head Teacher (principal) of each school and from each classroom teacher to obtain the end-term test scores of the children.
Statistical analysis
Differences in baseline characteristics between the feeding groups were determined using ANOVA. If overall differences were significant, then pairwise differences were examined to determine which groups were different from each other.
Outcome variables were the test scores in end-term academic tests of seven subjects (English, Arithmetic, Kiswahili, Kiembu, science, geography, arts) and the total test scores. The total score for each child was calculated by adding the test scores in seven subjects in each term. In ANOVA tests of baseline test scores, all the available data were used. A child was considered to have missing data for the total test score in a given term if he or she was missing a score for any academic subject test in an end-term examination.
Longitudinal models( Reference Weiss 50 ) were fit to test scores using the Statistical Analysis Systems mixed procedure version 9 (SAS Institute, Inc.) with an unstructured covariance matrix and time × school interaction model with a separate mean for each school in each term. Additional predictor variables included maternal literacy and highest school grade attained, household SES, children's school attendance, children's RPM scores, school, children's baseline age, sex, morbidity score, malaria status, anaemia status, anthropometry and baseline energy intake. Differences were considered statistically significant at P< 0·05. As there were three schools in each study group, estimates of the study group means in a given term were estimated as the average of the means of the three schools in that term.
For each child, average follow-up nutrient intake was calculated by averaging the intake recorded at eight post-baseline recall visits including the contributions of the Meat, Milk and Plain Githeri feedings. To identify the possible effects of nutrients on test scores, average nutrient intake and average nutrient intake × time interaction were used as predictors in the previous models with separate analyses being carried out for each nutrient of interest and test scores in each subject. If the coefficient of the average nutrient intake × time interaction is positive, then increased nutrient intake is associated with increased changes in test scores from term 5 − term 1. To make this interaction more interpretable, we subtracted the estimated change in test scores (term 5 − term 1) for a hypothetical student at the 90th percentile of the average follow-up nutrient intake distribution from the estimated change in test scores (term 5 − term 1) for a hypothetical student at the 10th percentile of the average follow-up nutrient intake distribution, holding all other predictors constant.
Results
Baseline findings
At baseline, there were no significant differences between the feeding groups for most of the variables, except for years of school completed by the mothers, which was highest in the Control group (Table 2). Across the feeding groups, the average of maternal literacy was between the 7th and 9th grade levels, with individual levels ranging from 0 to 12th grades. At baseline, baseline maternal literacy above the 8th grade when compared with maternal literacy below the 8th grade was associated with higher end-term test scores in every academic subject and total test scores (P <0·001). However, there were no significant differences between the feeding groups for maternal literacy at baseline.
Table 2 Baseline characteristics by study group (Mean values and standard deviations)
SES, socio-economic status; RPM, Raven's Progressive Matrices; WAZ, weight-for-age z-score; HAZ, height-for-age z-score; MUAC, mid-upper arm circumference; TSF, triceps skinfold.
* Mean value was significantly different from that of the Meat group (F(3,281) = 3·28, P= 0·021; ANOVA tests).
The baseline home intake of energy, protein and folate was significantly higher in children in the Plain Githeri group than in those in the Milk group (P< 0·05) (Table 3). The intake of available Fe was significantly higher in children in the Plain Githeri group than in those in the Milk and Control groups (P< 0·05).
Table 3 Baseline home food intake, follow-up (FU) intake including school snack, and change in nutrient intake from baseline to FU by study group∥ Reference Hambidge, Miller and Westcott¶ (Mean values and standard deviations)

* Mean values were significantly different from those of the Milk group (P< 0·05; ANOVA).
† Mean values were significantly different from own baseline value (P< 0·05; paired t test).
‡ Mean values were significantly different from those of the Control group (P< 0·05; ANOVA).
§ Mean values were significantly different from those of the Meat group (P< 0·05; ANOVA).
∥ Comparisons of baseline means between the groups and FU means between the groups were made using ANOVA tests.
¶ Paired t tests were used to assess the change in mean nutrient intake from baseline to FU for each of the groups. Change values were calculated for children with both baseline and FU values and thus may not exactly equal FU value minus baseline value due to missing data at either baseline or FU.
** Baseline nutrient intake values are the average of intake values recorded in three dietary recalls.
†† FU nutrient intake values are the average of eight dietary recalls over a 16-month period and include the nutrient values from the school snack.
‡‡ Changes in nutrient intake values were calculated from baseline and FU values. Values may not exactly equal the FU intake value minus the baseline intake value due to some missing FU intake data.
Baseline test scores (zone-wide end-term scores in the term before the start of the feeding intervention) indicated that the Plain Githeri group scored significantly higher than the Meat group and the Control group in English, Kiembu, Science and Arts and significantly higher than the Milk and Meat groups in Kiswahili (Table 4). The Plain Githeri group had significantly higher scores than the Meat group in Arithmetic and significantly higher total test scores. The Milk group had significantly higher scores than the Meat group in English and significantly higher total combined scores.
Table 4 Baseline (term 1) end-term test scores by group (Mean values and standard deviations)
* Mean values were significantly different from those of the Meat group (P< 0·05; ANOVA test; pairwise t test).
† Mean values were significantly different from those of the Control group (P< 0·05; ANOVA test; pairwise t test).
‡ Mean value was significantly different from that of the Milk group (P< 0·05; ANOVA test; pairwise t test).
Intervention results
In the total sample, attendance was a significant predictor of end-term test scores; however, no significant trends towards greater attendance were observed in the Meat and the Milk groups over the study period. For all the feeding groups, maternal literacy was a significant predictor of total end-term test scores in all the academic subjects except in Arts. Children with mothers with low baseline literacy levels (below 8th grade) showed significantly greater improvements (term 5 − term 1) than those with mothers with high baseline maternal literacy levels (above 8th grade) (P< 0·05).
Change in test scores compared with baseline test scores
Comparisons of the final term test scores (term 5) and baseline test scores revealed significant improvements in the test scores of the Meat group in six subjects compared with the baseline test scores (P< 0·05) (Fig. 2). The Milk group showed significant improvements in test scores in five of the eight scores. The test scores of the Plain Githeri and Control groups in Arts in term 5 were significantly better than those at baseline, but lower than those at baseline in the other academic subjects. All the groups had lower test scores in Science in term 5 than at baseline.
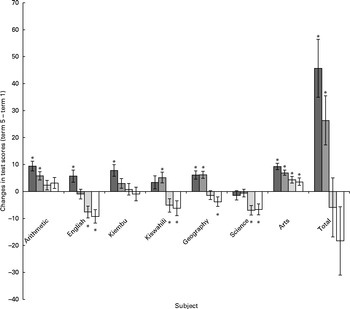
Fig. 2 Change in test scores by group compared with baseline test scores (term 5 − term 1). Values show the change in test scores (term 5 − term 1) in each academic subject. Values are means, with their standard errors represented by vertical bars. * Mean values were significantly different between own term 5 and term 1 (baseline) scores (P< 0·05). ![]() , Meat;
, Meat; ![]() , milk;
, milk; ![]() , plain Githeri; □, control.
, plain Githeri; □, control.
Changes in nutrient intake compared with baseline values
Energy intake increased for all the four groups (Table 3). In the Meat and Milk groups, the intake of all nutrients improved significantly. However, in the Milk, Plain Githeri and Control groups, intake averaged below the recommended intake levels for available Fe (estimated average requirement = 4·1mg/d for children aged 4–8 years) and Zn (estimated average requirement = 4·0 mg/d for children aged 4–8 years)( Reference Otten, Hellwig and Meyers 44 ). The intake of vitamin B12 in the Control and Plain Githeri groups was below the recommended levels (estimated average requirement = 1·0 μg for children aged 4–8 years)( Reference Otten, Hellwig and Meyers 44 ).
Changes in the test scores of each feeding group compared with changes in those of the Control group
Because the intervention groups had to be compared with the Control group also, differences (term 5 − term 1) in the mean test scores of each feeding group minus differences in the mean test scores of the Control group were calculated (Table 5). Children in the Meat group, and to a lesser extent those in the Milk group, exhibited greater positive changes in test scores compared with those in the Plain Githeri and Control groups. The Meat group showed significant improvements in test scores compared with the Control group in six of the seven subjects (Arithmetic, English, Kiembu, Kiswahili, Geography and Arts) and in the overall total test scores. The Milk group showed significant improvements in test scores compared with the Control group in five subjects (English, Kiswahili, Geography and Science) and in the overall total test scores. The changes in the test scores of the Plain Githeri group were not significantly different from those in the test scores of the Control group in any academic subject.
Table 5 Pairwise comparisons of changes in test scores (term 5 (T5) mean−term 1 (T1) mean)† ‡ (Mean values with their standard errors)

* P< 0·05.
† Values are the difference in changes in mean test scores (T5 − T1) between the studied groups.
‡ Note: End-term tests administered in different terms are not identical, so a decrease in test scores does not denote a decrease in knowledge. Test content had an increasing level of difficulty each term, meant to capture new topics taught in the curriculum.
Comparisons between the groups
Inter-group comparisons for change in mean test scores from baseline to term 5 in each academic subject showed that changes in the total test scores of the Meat and Milk groups were significantly greater than those in the total test scores of the Control group (Table 5). The Meat group was significantly higher in test scores than the Plain Githeri group in six subjects (Arithmetic, English, Kiembu, Kiswahili, Geography and Arts) and in the total test scores, and it showed significant improvements in test scores compared with the Control group in all the subjects except in Science. The changes in the test scores of the Milk group were significantly greater than those in the test scores of the Plain Githeri and Control groups in English, Kiswahili, Geography and Science. Compared to each other, the Meat and Milk groups were only significantly different for English scores, with the Meat group showing a significant improvement compared to the Milk group.
Effects of nutrient intake on changes in test scores
Of the twelve nutrients tested, seven nutrients were significant contributors to the change in test scores (Table 6). A positive outcome represents a better performance in the school test by the 90th percentile group (high intake) than by the 10th percentile group (low intake). A negative outcome indicates that the lower-intake group outperformed the high-intake group. The intake of Fe and vitamin B12 predicted the largest change in test scores in three subjects each, although the effect of vitamin B12 on test scores in Science was negative. The change in test scores in English and Science was not related to nutrient intake. Micronutrient intake associated with the meat and milk snacks significantly predicted increases in test scores in six of the eight test scores over time.
Table 6 Change in test scores (term 5−term 1) due to differential nutrient intake (that of a child at the 90th percentile nutrient intake minus that of the child at the 10th percentile nutrient intake)†
* The change is significant (P< 0·05).
† The estimated values of the level of improvement a child at the 90th percentile of nutrient intake would show in school test scores from term 1 to term 5 minus those of the level of improvement that the child at the 10th percentile (low intake) would show from term 1 to term 5 are reported. A positive outcome indicates that the high-intake child would improve more than the low-intake child; a negative outcome indicates that the lower-intake child would improve more than the high-intake child.
Increases in test scores associated with nutrient intake were observed for Arithmetic, Kiembu, Kiswahili, Geography and Arts, and there were increases in the total test scores. Test scores in English and Science were not related to the intake of the nutrients listed in Table 6, with the exception of vitamin B12, which had a negative effect on the test scores in Science. Higher intake of Fe predicted higher test scores in Kiembu, Kiswahili and Geography and higher total test scores. Higher intake of vitamin B12 predicted better performance in Arithmetic, Geography and Arts, but worse performance in Science. Five nutrients contributed significantly to the change in test scores in Kiembu and Geography. The change in test scores in Arithmetic was predicted by the intake of folate and vitamin B12. Test scores in both Kiembu and Kiswahili were significantly affected by higher intake of folate, Fe and available Fe. Test scores in Kiembu were also significantly predicted by energy intake per kg body weight and Zn intake. Test scores in Geography improved significantly with higher intake of Fe, energy per kg of body weight, vitamin B12, Zn and riboflavin. Test scores in both Geography and Kiembu increased with higher intake of five different nutrients. Test scores in Arts improved with the intake of folate, available Fe and vitamin B12. Increases in total combined scores were significantly associated with the intake of folate, Fe and energy per body weight. The intake of basal Zn, normative Zn, energy, vitamin B6 and protein was not significantly related to changes in test scores.
Discussion
The intake of a school snack containing ASF (meat or milk) significantly predicted improvement in test scores over time. The snacks served in the CNP study were isoenergetic, but targeted different existing nutrient gaps in Kenyan school children's diet, mainly animal source protein, available Zn, available Fe and vitamin B12. The present study is the first cluster-randomised, controlled feeding intervention study to demonstrate the impact of ASF on children's academic performance. Meat, and to a slightly lesser extent milk, supplementation resulted in significantly better test score improvements in key academic subjects (Arithmetic, English, Kiswahili and Geography) and total test scores compared with the other groups.
Data obtained from cohort I, which cohort II replicates, indicate that there were no significant changes in home food intake over the 2 years of the study, except in the energy and protein intake of children in the Meat group at home( Reference Gewa, Murphy and Weiss 51 ). This may be due to their improved appetite and their increased activity levels. The meat snack had the greatest amount of bioavailable Fe and Zn, which are known to improve appetite. Children in the Meat group also exhibited significant increases in physical activity levels and lean body mass( Reference Neumann, Jiang and Weiss 52 – Reference Neumann, Murphy and Gewa 54 ).
The improvements in test scores observed in the Meat group are impressive, given that at baseline the Meat group had the lowest test scores among all the groups in all but one academic subject and lowest total test scores. Yet, following the intervention feedings, the Meat group had the highest total test scores and also obtained the highest test scores in several academic subjects. The Milk group obtained higher test scores than the other groups in certain academic subjects (Table 5); however, in no academic subject were the scores of the Milk group significantly higher than those of the Meat group. The previously published results regarding cognitive performance in cohort I of the present study indicated a greater improvement in the RPM scores of the Meat group than in those of all the other groups( Reference Whaley, Sigman and Neumann 47 , Reference Neumann, Murphy and Gewa 54 ). In a combined analysis of cohorts I and II also, the Meat group showed greater improvements in the RPM scores than all the other groups( Reference Neumann, Murphy and Bwibo 55 ). The cognitive improvement in children of the Meat group may account for their improved school test scores.
Possible mechanisms for changes in test scores include higher cognitive scores, increased physical activity levels and exploratory and leadership behaviours, improvements in morbidity, and the presence of micronutrients that affect learning and brain function. The findings demonstrate that an increased intake of micronutrients such as folate, Fe, available Fe, Zn and vitamin B12 and energy per kg body weight and riboflavin is directly related to the improvement in test scores and learning. The ingredients of the meat snack were rich in energy, Zn, Fe and vitamin B12. The milk snack contained energy, Ca, vitamin B12, vitamin A and riboflavin. Fe, Zn, folate, vitamin B12 and energy are important for cognition and learning( Reference Louwman, van Dusseldorp and van de Vijver 25 , Reference Lukowski, Koss and Burden 38 , Reference Sandstead, Penland and Alcock 56 – Reference Nguyen, Gracely and Lee 58 ), and vitamin A affects child mortality and morbidity( Reference Imdad, Herzer and Mayo-Wilson 59 ), which in turn affect school attendance and readiness to learn.
Although milk has a lower content of Fe and Zn, which are extremely important for cognitive development, than meat, the Milk group showed impressive increases in test scores over time. Given the relative differential availability and cost of using various types of meat, fish, fowl and other small animals compared with those of milk, milk should certainly be utilised in school feeding programmes to improve academic performance where sources of a variety of meat are not available or affordable( Reference Djazayery, Rahmani and Pourshariari 60 ). While previous studies have demonstrated that school feeding improves attendance( Reference Taras 61 , Reference Grantham-McGregor 62 ), only a non-significant increase in attendance was observed in the Meat and Milk groups in the present study.
The Plain Githeri and Control groups had lower scores in term 5 than at baseline in English, Kiswahili, Geography and Science and lower total test scores. Children in the Plain Githeri and Control groups may have scored lower than their own baseline scores because they did not progress as well as the other groups academically; thus, as the content of the examinations became harder, their scores were lower than those at baseline. It is important to note that the end-term tests administered in term 1 and in term 5 were not identical. The end-term test content, designed by the Kenyan Ministry of Education, had an increasing level of difficulty each term, meant to capture new topics taught in the curriculum. The results of cognitive testing for these two groups showed improvements in cognition, as indicated by the RPM test scores( Reference Whaley, Sigman and Neumann 47 , Reference Neumann, Murphy and Gewa 54 ).
Although children and their teachers and families were not blinded to their feeding group assignment, the hypotheses of the study were not shared with them at all. The only aspects that may have been known through popular knowledge were some of the health and academic benefits of milk, since milk has been used sporadically in ad hoc school feeding programmes in Kenya. We do not believe that improvements in tests scores are a result of the expectations of school officials and parents, and we do not think that children's ability to correctly answer questions regarding academic subjects was influenced by knowing that they were getting a meat, milk or plain githeri snack or no snack at all.
Another limitation of the present study is that it was not possible to carry out biochemical micronutrient analyses for the cohort II children due to funding limitations. However, biochemical analyses carried out on serum samples obtained from the cohort I children indicated a high prevalence of micronutrient deficiencies such as riboflavin, Zn, Fe, vitamin A and vitamin B12 deficiencies at baseline( Reference Siekmann, Allen and Bwibo 63 ). After the first year of the cohort I study, significant increases in plasma vitamin B12 concentrations were observed in children in the Meat and Milk groups compared with the Plain Githeri and Control groups (P< 0·0005)( Reference Siekmann, Allen and Bwibo 63 ). For other micronutrients, no significant differences were found between the feeding groups or between each feeding group v. the Control group, but it is possible that infections and/or malaria could have obscured the effects( Reference Siekmann, Allen and Bwibo 63 ). As children in cohort II received the same feeding intervention and lived in the same area, it is likely that they experienced changes in micronutrient status similar to those experienced by cohort I. However, we were unable to correlate biochemical results with end-term test scores, since the term scores that we obtained were of the cohort II children and the biochemical data were of the cohort I children.
While the baseline data did not show significant differences in SES at baseline, our subjective observations of the school setting, classroom amenities and teacher absenteeism indicated that school quality, teaching and classroom physical amenities were not equal. Some of the best schools, based upon these observations, were the Plain Githeri schools. A possible reason for the Plain Githeri group not showing the same magnitude of improvement in test scores could be that it had the highest scores at baseline. On the other hand, the Meat group schools were of the poorest quality based upon the above-mentioned observations, yet ended up having higher tests scores in several academic subjects.
The incorporation of a wide variety of micronutrient-rich meat, or milk when meat is not available, by school feeding programmes can be a key component to promote academic success in children. Although there may be problems with long-term sustainability, parent, school and community participation in raising small animals and school gardens is a possible approach to school feeding. A wide variety of small animals, particularly goats, rabbits, poultry and fish, can be important sources of ASF for school feeding programmes. Nutrition education, both for parents and for schoolchildren, through schools and agricultural extension is also needed. The improvement of diet quality for schoolchildren can improve school performance and academic achievement. Improved educational attainment leads to improved learning capacity in children and qualifies them for further academic and vocational opportunities and can affect economic development. While school test scores are not particularly relevant to adult and elderly populations, improved physical activity, muscle strength, optimal mental functioning, protein quality, Fe deficiency, and vitamin B12 deficiency-related anaemia are important issues in adult and elderly populations. ASF supplementation also has the potential to improve the nutritional status and function of adult and elderly populations, particularly muscle strength, cognitive function and overall quality of life.
Acknowledgements
The authors pay special tribute to the late psychologist and child development expert Dr Marian Sigman (UCLA) for her extensive input into the cognitive and educational aspects of the CNP. The authors thank Minnie Kamore, the field supervising psychologist, for obtaining the test scores from the schools and supervising the cognitive assessments and Montague W. Demment for providing the vision to support the funding of the study through the Global Livestock Collaborative Research Support Program (GL-CRSP).
The present study was supported by the GL-CRSP, United States Agency for International Development (DAN-1328-G-00-0046-00), with partial funding from the James A. Coleman African Study Center (UCLA) and the National Cattleman's Beef Association (PCE-G-98-00 036-00). GL-CRSP, the James A. Coleman African Study Center and the National Cattleman's Beef Association had no role in the design and analysis of the study or in the writing of this article.
The authors' contributions were as follows: J. L. H. analysed data for her PhD dissertation and wrote the initial draft of the paper; R. E. W. designed and guided data analysis for the PhD dissertation and the present paper and edited the paper; N. O. B. oversaw the field research and served as the Kenyan Principal Investigator; O. M. G. guided the interpretation of the data; N. D. provided critical and relevant literature review and played a critical role in the drafting of the final paper and figures; C. G. N. designed, conducted and oversaw the research study, served as the Principal Investigator, wrote the paper, and had primary responsibility for the final content. All authors read and approved the final manuscript.
None of the authors has any conflicts of interest.








