


Individuals of South Asian origin are at high risk of developing type 2 diabetes mellitus (T2DM) and the prevalence of T2DM is two to four times greater in South Asians than in their white European counterparts( Reference Gholap, Davies and Patel 1 ). Furthermore, diabetes occurs 5–10 years earlier in South Asian individuals compared with white European individuals( Reference Gholap, Davies and Patel 1 , Reference Forouhi, Sattar and Tillin 2 ). South Asians are the largest ethnic minority group in the UK; therefore determining modifiable risk factors that can be targeted in this population is key. Evidence suggests that migrant South Asian populations and those in urban areas of India are at greater risk of T2DM compared with those in rural areas, and lifestyle factors including dietary habits are likely to have greater impact on insulin resistance than genetic factors( Reference Misra, Khurana and Isharwal 3 ). However, studies investigating dietary profiles and the relationship between dietary intake and T2DM risk within the South Asian population are scarce( Reference Isharwal, Misra and Wasir 4 ).
The WHO has estimated that up to 2·7 million lives around the world could be saved with sufficient fruit and vegetable consumption( 5 ). Fruit and vegetables are accepted as beneficial for the prevention of cancer and CVD and evidence surrounding their role in the prevention of T2DM is growing( Reference Van't Veer, Jansen and Klerk 6 , Reference Carter, Gray and Troughton 7 ). We recently demonstrated a strong inverse association with glucose regulation and fruit and vegetable intake in a cross-sectional population at risk of diabetes( Reference Carter, Gray and Talbot 8 ). Furthermore, reported intake of fruit and vegetables is low in South Asian individuals living in India; the INTERHEART study demonstrated that daily consumption of fruit and vegetables by South Asians was lower than individuals from other countries, despite vegetarianism being common in the South Asian population examined( Reference Joshi, Islam and Pais 9 ). Within Europe fruit and vegetable intake has also been observed to be lower in migrant South Asian communities compared with white Europeans; however, these data are out of date( Reference Ness, Cappuccio and Atkinson 10 ).
Vitamin C consistently demonstrates a high correlation with fruit and vegetable intake( Reference Zino, Skeaff and Williams 11 , Reference Broekmans, Klopping-Ketelaars and Schuurman 12 ), with about 90 % of dietary vitamin C being obtained from fruit and vegetable consumption( Reference Michels, Welch and Luben 13 ). We aimed to determine if plasma vitamin C, a marker for fruit and vegetable intake, was different between South Asian and white European individuals screened for diabetes. Vitamin C is also an antioxidant and may potentially be depleted under conditions of oxidative stress; therefore we also aimed to determine if levels of oxidative stress as measured by urinary F2-isoprostanes were different between ethnic groups.
Methods
Participants
Participants were recruited as part of the screening phase of a large community intervention trial for the prevention of T2DM, Let's Prevent Diabetes, as described in detail elsewhere( Reference Gray, Khunti and Williams 14 ). The data reported in the present study are from a nested sub-study in which participants provided a plasma vitamin C sample( Reference Carter, Gray and Talbot 8 ). Individuals between 40 and 75 years if white European or 25 to 75 years if South Asian (originating from India, Pakistan and Bangladesh) were included. Individuals were excluded if they were unable to give informed consent, were pregnant or lactating, had established diabetes, had a terminal illness or required an interpreter for any language other than South Asian.
Anthropometric and biochemical measures
Standard operating procedures were used to measure height (m), weight (kg), waist circumference (cm), hip circumference (cm) and blood pressure (mmHg) and to collect current and previous medical history, medication, smoking status and family history. Social deprivation was determined using the Index of Multiple Deprivation using postcodes( 15 ). Self-completed questionnaires determined physical activity( Reference Craig, Marshall and Sjöström 16 ) and dietary intake( Reference Roe, Strong and Whiteside 17 , Reference Little, Barnett and Margetts 18 ).
Participants received a standard 75 g oral glucose tolerance test and were categorised according to WHO 1999 criteria( Reference World Health 19 ). Plasma glucose was determined using the hexokinase method with a CV of 1·61 % (Abbott Laboratories). HbA1c was quantified using HPLC on an automated DCCT aligned Biorad aligned system (Bio-Rad Laboratories), with a CV < 0·1 %. Serum lipids were measured by enzymic methods (Dade Behring Dimension Analyser). Plasma vitamin C was measured on a Cobas FARA centrifugal analyser with a fluorescent attachment (Roche Diagnostics) at Queen's University Belfast. Analysis of urinary F2-isoprostane and creatinine is as described elsewhere( Reference Carter, Gray and Talbot 8 ).
The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the East Midlands–Nottingham Research Ethics Committee. Written informed consent was obtained from all subjects/patients. The Let's Prevent Diabetes study is registered with ISRCTN (http://www.controlled-trials.com/); reference no. ISRCTN80605705.
Statistical analysis
All statistical analysis was carried out using SPSS version 18·0 (SPSS Inc.). Baseline characteristics were described using frequency and descriptive techniques for categorical and continuous variables. Differences between ethnic groups were tested using independent t tests for continuous variables and χ2 tests for categorical variables. The association between ethnic group (explanatory variable) and plasma vitamin C (outcome) was investigated using linear regression. Adjustment for several confounders was carried out: age, sex and BMI (model 1); model 1 plus the use of vitamins, smoking, deprivation (model 2); model 2 plus 2-h glucose, blood pressure, total cholesterol, HDL, TAG, activity and urinary F2-isoprostanes (model 3).
Results
Baseline characteristics
From a total of 2878 participants who provided plasma vitamin C, 1820 were white European and 253 South Asian, and thus included in this analysis; the remaining 805 participants (those of black, Chinese or other ethnic backgrounds) were excluded. Baseline characteristics are presented in Table 1. All measures of glycaemic control were significantly lower in white European compared with South Asian participants. No difference was observed in levels of oxidative stress (as measured by urinary F2-isoprostanes) between the two ethnic groups.
Table 1. Baseline characteristic of white European (WE) and South Asian (SA) participants
(Mean values and standard deviations or numbers and percentages)
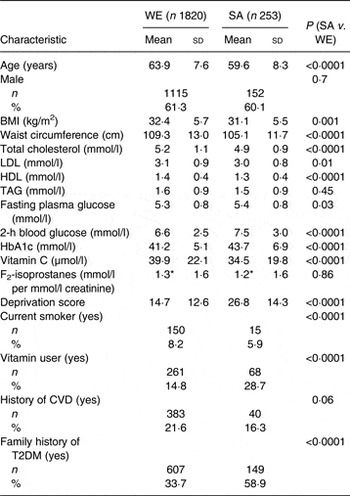
T2DM, type 2 diabetes mellitus.
*Geometric mean.
Plasma vitamin C and ethnicity
Mean plasma vitamin C was significantly lower in the South Asian participants compared with white Europeans (34·5 (sd 19·8) v. 39·9 (sd 22·1) µmol/l, respectively; P ≤ 0·0001). A greater percentage of South Asian individuals had plasma vitamin C deficiency, as demonstrated by plasma vitamin C concentration ≤ 11·4 µmol/l( Reference Schleicher, Carrol and Ford 20 ) (15·5 % (n 39) v. 11·4 % (n 207); P = 0·08). Furthermore, significantly fewer South Asian individuals consumed five portions of fruit and vegetables per d, as determined by a plasma vitamin C concentration of equal to or greater than 50 µmol/l (23·2 % (n 58) v. 31·4 % (n 558); P = 0·01).
For each 1 sd increase in plasma vitamin C (20 µmol/l) there was an associated 0.10 (95 % CI –0·11, –0·04) mmol/l (P ≤ 0·0001) and 0·05 (95 % CI –0·16, 0·07) mmol/l (P = 0·46) decrease in fasting blood glucose in white European and South Asian populations, respectively. For each 1 sd increase in plasma vitamin C (20 µmol/l) there was an associated 0·07 (95 % CI –0·30, –0·07) mmol/l (P ≤ 0·002) and 0·10 (95 % CI –0·7, 0·1) mmol/l (P = 0·14) decrease in 2-h blood glucose in white European and South Asian populations, respectively.
Table 2 presents results from linear regression conducted between ethnicity and plasma vitamin C. Unadjusted regression analyses demonstrated average plasma vitamin C to be 1·78 (95 % CI 0·83, 2·74) µmol/l (P < 0·001) lower in South Asians compared with white Europeans. The significant association between plasma vitamin C and ethnicity remained after adjustment for age, sex, BMI, vitamin use, smoking and deprivation score (P ≤ 0·0001). The association also remained significant after inclusion of 2-h glucose, blood pressure, lipids, activity levels and urinary F2-isoprostanes (P = 0·02).
Table 2. Association between ethnicity (white European v. South Asian) and plasma vitamin C
(Regression coefficients and 95 % confidence intervals)
*Regression coefficient showing the difference in plasma vitamin C between ethnic groups (white European being the reference group).
†Model 1: adjusted for age, sex and BMI.
‡Model 2: model 1 plus use of vitamins, smoking status and deprivation score.
§Model 3: model 2 plus 2-h glucose, blood pressure, total cholesterol, HDL, TAG, family history of type 2 diabetes mellitus, activity and urinary F2-isoprostanes.
Discussion
These data provide much needed current information of the fruit and vegetable intake of South Asian individuals in the UK. South Asian participants had significantly lower mean plasma vitamin C compared with white Europeans. This is consistent with the observation that significantly fewer South Asians consumed the recommended five portions of fruit and vegetables per d, as determined by a plasma vitamin C of ≥ 50 µmol/l( Reference Khaw, Wareham and Bingham 21 ). The data support a study which was published over 10 years ago which also found South Asians to have lower vitamin C levels compared with white Europeans( Reference Ness, Cappuccio and Atkinson 10 ), suggesting that government campaigns have not yet successfully reached the South Asian population.
The South Asian participants in the present study had significantly higher HbA1c, and fasting and 2-h glucose than their white European counterparts as demonstrated in a number of other studies( Reference Mostafa, Davies and Webb 22 , Reference Lee, Brancati and Yeh 23 ). We have previously demonstrated an association between plasma vitamin C and glycaemic parameters in this cohort( Reference Carter, Gray and Talbot 8 ). However, separate analysis of the two ethnic groups found this relationship only remained significant in the white European population. We suggest that this is probably due to smaller numbers in the South Asian population reducing power to detect an association; this is supported in that the effect size is broadly similar in the two ethnic groups. Furthermore, the strong significant difference in vitamin C concentration between the two ethnic groups remains when adjusting for glucose control. Thus the suggestion that lower consumption of fruits and vegetables by South Asian individuals may contribute to an increased probability of developing T2DM exists.
Plasma vitamin C is an antioxidant as well as a biomarker for fruit and vegetable intake, and under high levels of oxidative stress antioxidant levels may become depleted( Reference Bullo, Casas-Agustench and Amigo-Correig 24 ). However, we found no difference in urinary F2-isoprostanes between ethnic groups; thus differences probably reflect intake not depletion.
The need for future investigation into failure of the current government initiatives that promote fruit and vegetable intake are required, with particular focus on South Asian communities; furthermore, investigations of how dietary practices can be successfully manipulated in the South Asian population are required.
Strengths and limitations
The study provides robust biomarker data on fruit and vegetable consumption from a large multi-ethnic cohort. Nutritional biomarkers remove the reliance of self-report and can be used across ethnic groups. The South Asian individuals included were from a homogeneous cohort, with the majority (96 %) originating from India. Furthermore, we invited participants from a large area of the English Midlands; however, intake levels may be different in populations from other areas of the UK.
The present study is cross-sectional by design; thus the direction of association cannot be defined. The possibility that South Asian individuals utilise vitamin C differently to white Europeans cannot be excluded. It is imperative that randomised studies are carried out which provide foods high in vitamin C to both white European and South Asian participants to allow concentrations of plasma vitamin C to be examined pre- and post-consumption. Furthermore, it cannot be excluded that different cooking methods across ethnic groups do not influence vitamin C intake. Vitamin C is water soluble and easily depleted from foods with prolonged cooking.
Dietary intake was additionally assessed using the Dietary Instrument for Nutritional Education( Reference Roe, Strong and Whiteside 17 , Reference Little, Barnett and Margetts 18 ); however, completion rates were extremely low and therefore the data have not been included in the analysis. The questionnaire was adapted for use in a South Asian community as part of the Health Survey for England; however, it has not been validated in this population( Reference Roe, Strong and Whiteside 17 ). Further research is required that includes ethnic-specific questionnaires.
Conclusion
Fewer South Asian individuals consumed five portions of fruit and vegetables per d compared with white Europeans as measured by plasma vitamin C. Furthermore, plasma vitamin C was significantly lower in South Asians compared with their white European counterparts. The effects of tailored advice to this high-risk group should be investigated.
Acknowledgements
We would like to thank both Dr Jayne Woodside and Dr Sarah Gilchrist from Queen's University Belfast for their analysis of plasma vitamin C. We would also like to give special thanks to Duncan Talbot from Unilever Discover, Colworth Science Park, UK, for the analysis of urinary F2-isoprostanes.
The present study presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (no. RP-PG-0606-1272). The views expressed in this publication are those of the author(s) and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health. The project was supported by the NIHR Collaboration for Leadership in Applied Health Research and Care – Leicestershire, Northamptonshire and Rutland and The NIHR Leicester–Loughborough Diet, Lifestyle and Physical Activity Biomedical Research Unit which is a partnership between University Hospitals of Leicester NHS Trust, Loughborough University and the University of Leicester.
All authors have contributed to the paper: P. C., M. J. D. and K. K. came up with the original idea for the study; P. C. conducted the research; L. J. G. and D. H. M. carried out the statistical analysis for the study; P. C. wrote the article and all other authors gave input to the final version of the manuscript. All authors have seen and approved the contents of the manuscript.
K. K. and M. J. D. have received grants from the NIHR for studies on the prevention of type 2 diabetes. P. C., L. J. G. and D. H. M. have no conflicts of interest to declare.



 Open access
Open access