



Attention-deficit/hyperactivity disorder (ADHD) is characterized by a persistent pattern of inattention, hyperactivity, and impulsivity across contexts that interferes with an individual’s development and functioning (American Psychiatric Association, 2013). It is one of the most common childhood disorders, with approximately 6.1 million children in the United States diagnosed with ADHD (Danielson et al., Reference Danielson, Bitsko, Ghandour, Holbrook, Kogan and Blumberg2018). Without appropriate assistance, children diagnosed with ADHD may be at elevated risk for experiencing academic and peer relationship challenges (Erskine et al., Reference Erskine, Norman, Ferrari, Chan, Copeland, Whiteford and Scott2016; Gardner & Gerdes, Reference Gardner and Gerdes2015). Moreover, the majority of children diagnosed with ADHD are 12–17 years old (Danielson et al., Reference Danielson, Bitsko, Ghandour, Holbrook, Kogan and Blumberg2018). By understanding the developmental origins of ADHD, children could be diagnosed earlier in their lives and be provided with appropriate interventions and assistance to foster good academic outcomes and positive peer relationships. Thus, it is important to examine the developmental origins of ADHD symptoms.
Most research discussing the etiology of ADHD focuses on genetic aspects of the disorder, suggesting that children with ADHD were born with a genetic predisposition to the disorder. However, epigenetic processes shape the development of ADHD (e.g., Faraone & Biederman, Reference Faraone and Biederman2000; Lifford et al., Reference Lifford, Harold and Thapar2009; Nigg et al., Reference Nigg, Sibley, Thapar and Karalunas2020); behavioral and environmental factors also may play a key role (Hamza et al., Reference Hamza, Halayem, Bourgou, Daoud, Charfi and Belhadj2019). Indeed, a number of longitudinal studies have identified qualities of early mother-child interactions that may lead to the development of ADHD symptoms, such as intrusiveness and overstimulating care (Carlson et al., Reference Carlson, Jacobvitz and Sroufe1995; Jacobvitz & Sroufe, Reference Jacobvitz and Sroufe1987; Keown, Reference Keown2012) and hostility (Lifford et al, Reference Lifford, Harold and Thapar2009). Little is known, however, about the underlying mechanisms through which parenting quality may influence the development of ADHD. Given that an inability to regulate emotions effectively has been associated with symptoms of ADHD, such as issues with attention, impulsivity, and hyperactivity (Bunford et al., Reference Bunford, Evans and Wymbs2015), one such mechanism may be through parental influences on the development of children’s emotion regulation.
Most studies examining caregiving antecedents of ADHD focus on maternal parenting, but consideration of fathers’ parenting is also critical given fathers’ unique role in their children’s development of regulatory skills (e.g., Jacobvitz et al., Reference Jacobvitz, Aviles, Aquino, Tian, Zhang and Hazen2022; Lamb, Reference Lamb2004). Thus, the goal of the current study is to address these gaps in the literature by: (1) examining the influence of fathers’ emotionally disengaged interactions with their infants on their children’s emotion regulation during toddlerhood and, subsequently, their ADHD symptoms at age 7; and (2) investigating relations among fathers’ minimizing responses to toddler distress, toddlers’ emotion regulation, and the later development of child ADHD symptoms.
The role of paternal parenting in the development of emotion regulation and ADHD
Emotion regulation is the ability to moderate, inhibit, enhance, or maintain emotional experiences and expressions (Calkins & Hill, Reference Calkins, Hill and Gross2007). A core symptom of ADHD is difficulty regulating emotions effectively in socially appropriate ways (Bunford et al., Reference Bunford, Evans and Wymbs2015). Specifically, ADHD is often characterized by underregulation: high emotional reactivity and the inability to inhibit the impulsive expression of emotions (Banaschewski et al., Reference Banaschewski, Jennen-Steinmetz, Brandeis, Buitelaar, Kuntsi, Poustka, Sergeant, Sonuga-Barke, Frazier-Wood, Albrecht, Chen, Uebel, Schlotz, van der Meere, Gill, Manor, Miranda, Mulas, Oades and Asherson2012; Martel, Reference Martel2009; Walcott & Landau, Reference Walcott and Landau2004). Further, children diagnosed with ADHD exhibit difficulties with emotion regulation that may result in more negative social, emotional, and academic outcomes (Wehmeier et al., Reference Wehmeier, Schacht and Barkley2010). Given the associations between emotional underregulation and negative adjustment outcomes in children with ADHD, it is important to examine early predictors of emotional dysregulation when analyzing antecedents of ADHD symptoms.
Parents play a pivotal role in their children’s development of emotion regulation. Infancy and early childhood are characterized by the rapid maturation of neural systems underlying emotional control, and the acquisition of strategies necessary for emotional and behavioral control build exponentially (Diamond, Reference Diamond, Levin, Eisenberg and Benton1991; Grossmann, Reference Grossmann2013), Thus, parenting behaviors during infancy and toddlerhood may have the greatest influence on the development of children’s emotion regulation skills. Parents serve as co-regulators of emotional distress during infancy, as children have not yet developed appropriate emotion regulation strategies. As such, sensitive parenting is imperative for the development of children’s emotion regulation skills, and insensitive parenting characteristics may lead to emotion regulation difficulties. For example, research has shown that, when compared to children of mothers who responded to their distress with sensitivity, those who received intrusive maternal care in infancy demonstrated later difficulties with emotion regulation (Halligan et al., Reference Halligan, Cooper, Fearon, Wheeler, Crosby and Murray2013) and were more likely to develop symptoms of ADHD (Jacobvitz & Sroufe, Reference Jacobvitz and Sroufe1987).
The role of father-infant interactions in children’s emotional development has been particularly understudied, despite recent findings indicating that t father-child interaction in the early years may play an important role in children’s early emotional development (Hazen et al., Reference Hazen, McFarland, Jacobvitz and Boyd-Soisson2010; Paquette, Reference Paquette2004). Fathers’ play with infants and young children is generally vigorous, spontaneous, and state-disrupting (Lamb, Reference Lamb2004; Volling et al., Reference Volling, Stevenson, Safyer, Gonzalez, Lee, Volling and Cabrera2019), thus constantly upregulating children’s emotional arousal. For young children, playing with a much stronger – but friendly and trustworthy – opponent brings wariness, while also being exhilarating (Sandseter, Reference Sandseter2010). Furthermore, the competitiveness and upregulated arousal that results from this type of play provide opportunities for children to learn to control their emotions, interpret others’ emotions, and manage their own impulses (Peterson & Flanders, Reference Peterson, Flanders, Tremblay, Hartup and Archer2005). During this period of varying degrees of emotional arousal, fathers’ engagement may play a major role in their children’s downregulation of arousal. That is, fathers who are emotionally engaged with their children during play will recognize when their children are overstimulated and effectively calm their infants when this occurs (Hazen et al., Reference Hazen, McFarland, Jacobvitz and Boyd-Soisson2010). Because fathers engage in more physical and emotionally stimulating play (e.g., rough-and-tumble) than mothers, they may provide unique opportunities for their children to practice their regulatory skills (Gregory et al., Reference Gregory, Kivisto, Perdue and Estell2019; Lamb, Reference Lamb2004; Volling et al., Reference Volling, Stevenson, Safyer, Gonzalez, Lee, Volling and Cabrera2019). However, when fathers are emotionally disengaged while caring for their infant, they cannot be perceptive or responsive to their infant’s need to be soothed; thus, they cannot provide the care necessary for the infant to develop emotional self-regulation, leading the child to exhibit difficulties with emotion regulation. In support of this view, fathers’ (but not mothers’) emotional withdrawal during interaction with their infants was found to be associated with their children’s greater externalizing symptoms (Ramchandani et al., Reference Ramchandani, Domoney, Sethna, Psychogiou, Vlachos and Murray2013).
During toddlerhood, when children begin to understand and use language, parents move beyond serving as emotional co-regulators and begin the process of emotional socialization, defined as “socialization of children’s understanding, experience, expression, and regulation of emotion” (Eisenberg et al., Reference Eisenberg, Cumberland and Spinrad1998, p. 231). For a child to gain an appropriate awareness of their negative emotions and learn how to manage them effectively, parents must be engaged and attuned to the context of the emotional expression, in order to help the child identify the emotion and its cause, support their child’s emotional expression, coach children through it, and model adaptive emotion regulation (Gottman et al., Reference Gottman, Katz and Hooven1997). For example, if a toddler starts to tantrum because he is not ready to go home from the playground yet, a supportive response might be, “I know you are angry that we need to go home now. Let’s take a deep breath and think of something fun we can do when we get home.” (Eisenberg et al., Reference Eisenberg, Cumberland and Spinrad1998; Gross, Reference Gross2013). Responding to children’s distress in a minimizing way could be particularly detrimental to children’s development of emotion regulation skills. When a parent responds to their toddlers’ emotional distress with minimizing responses, such as “That’s nothing to cry about, don't be a baby,” they teach their children that their emotions are inappropriate or not valid, and that they cannot count on the parent for comfort during times of distress. Parents who are emotionally disengaged and/or minimize their child’s distress also lose the opportunity to actively teach and model appropriate regulation strategies. In addition to not providing a model of adaptive emotion regulation or providing emotional support for handling negative emotions, this sort of emotional “gaslighting” is likely to be particularly frustrating, leading to even greater underregulation, while at the same time giving the child no tools for coping with such frustration. Subsequently, difficulties in regulating emotions in early childhood may be associated with greater ADHD symptoms by middle childhood and adolescence, a time during which most ADHD diagnoses occur. Indeed, parents’ minimizing reactions toward their children’s negative emotions have been associated with their children’s greater negative affectivity and poorer emotion regulation skills (Eisenberg & Fabes, Reference Eisenberg and Fabes1994).
By examining father-infant interaction in infancy and toddlerhood and assessing emotion regulation at 24 months, the current study can help to elucidate earlier developmental pathways that may be particularly informative for intervention and prevention efforts. Thus, whereas the majority of literature linking parenting to the early development of emotion regulation focuses on maternal parenting, the current study adds to existing work by examining fathers’ emotional disengagement during infancy and minimizing responses to children’s distress during toddlerhood in relation to children’s development of emotion regulation skills during toddlerhood and ADHD symptoms at age 7.
Current study
The current study will examine the following hypotheses: (1) Fathers’ emotional disengagement with their children at 8 months will be directly associated with children’s difficulties with emotion regulation at 24 months; (2) Fathers’ minimizing responses to their children’s distress at 24 months will be directly associated with children’s difficulties with emotion regulation at 24 months; (3) Children’s difficulties with emotion regulation at 24 months will be directly associated with ADHD symptoms at age 7; (4) There will be a significant indirect effect between fathers’ emotionally disengaged parenting at 8 months and children’s ADHD symptoms at age 7 through toddlers’ difficulties with emotion regulation, and (5) There will be a significant indirect effect between fathers’ minimizing responses to their children’s distress at 24 months and children’s ADHD symptoms at age 7 through toddlers’ difficulties with emotion regulation.
Method
Participants
Data were collected in a large Southwestern city as part of the Parents and Partners longitudinal study that followed families over the transition to parenthood through middle childhood (N = 124). To meet inclusion criteria for participation, couples had to speak English, be cohabiting, and be in the third trimester of pregnancy with their first child. Couples were recruited through public service radio announcements, press releases in the newspaper, birthing classes, and flyers posted at birthing clinics. Almost all the couples in the sample (95.9%) were married. At the time of recruitment, mothers’ ages ranged from 16 to 42 (M = 29), and fathers’ ages ranged from 19 to 50 (M = 31). The majority of the participants identified as White (84%), with the remaining couples identifying as Hispanic/Latino (8%), Black (2%), or biracial or of another ethnicity (6%). The median family income of the sample was $30,000–$44,999 (24.3%), with 17% of the couples earning less than $30,000 and living below the poverty line for the year when the sample was collected, 27.1% earning $45,000–$60,000, and 31.4% earning over $60,000. Most participants were well-educated: 17% of the mothers and fathers had earned a graduate degree, 46% of the mothers and 38% of the fathers had a bachelor’s degree, 25% of the mothers and 35% of the fathers did not graduate from college but reported training beyond high school, and 9% of mothers and 8% of fathers had a high school degree. At 3–6 weeks postpartum, parents indicated the sex of their infant. The sample was composed of 73 males (58%) and 51 females (41%).
The data used for this longitudinal study were collected in three waves: at 8 months postpartum, at 24 months postpartum, and when the child was 7 years of age. Upon completion of each data collection wave, parents received a $50 savings bond, newsletters from the laboratory containing project updates, a copy of videotaped interactions with their child, t-shirts educational books for their child, and an audiotape of lullabies. At 24 months, 108 families remained in the sample. By 7 years, 85 families remained in the sample. Data from 71 children were included in the analyses at age 7 because only teachers who knew the children for at least 3 months were asked to complete a children’s behavior questionnaire. The couples who reported family incomes between $0 and $30,000 at the first data collection wave were more likely to drop out of the study by 7 years than families with higher household incomes (χ2 (4) = 12.22, p < .05). There were no significant differences in any other demographic variables between couples who remained in the study at 7 years and those who did not.
Procedure
When infants were 3–6 weeks old, mothers completed reports about children’s sex and temperament. When infants were 8 months old, mothers and fathers reported on father involvement, and fathers were videotaped during home visits as they engaged in interactions with their children. When children were 24 months old, parents and children attended the laboratory. Fathers engaged in free play, cleanup, and puzzle-type tasks with their children. Children also completed two challenging and frustrating tasks with a researcher. When children were 7 years old, teachers completed an assessment of childhood behavior problems.
Measures
Fathers’ emotionally disengaged interactions with infants
During home visits, when infants were 8 months old, fathers were individually videotaped with their infants during 30-min interactions in which fathers were instructed to change their infants’ clothes, feed their infants, and play with their infants as they ordinarily would. The Infant Caregiving Scales (ICS; Hazen, Reference Hazen1997) were used to assess father disengagement. The ICS is composed of 90 items that derive from examples of caregiving from Ainsworth’s global scales for assessing acceptance, cooperation, and sensitivity (Ainsworth et al., Reference Ainsworth, Blehar, Waters and Wall1978). A criterion sort method (Waters & Deane, Reference Waters and Deane1985) was utilized to develop several discrete caregiving scales, including emotional disengagement. Trained coders rated each item on the ICS scale according to the extent to which they were diagnostic of emotional disengagement. Items in which coders agreed were highly reflective of emotional disengagement or emotional attunement (reverse scored) were then averaged to develop the emotional disengagement subscale, which consists of eight items that measure the extent to which parents display flat and emotionally withdrawn affect during interactions with their infants. Each item was scored based on father-child interactions across all three contexts, and then scores on the 8 items were summed to create the final father disengagement score. This subscale does not measure the extent to which the parents were physically withdrawn or uninvolved with their infants. Example items include: “Parent and baby share joy in their interaction; they get obvious pleasure from being together.” (reverse scored) “Parent shows physical affection to baby (e.g., tender kisses, strokes baby’s hair) without interfering with the baby’s wishes.” (reverse scored). “Parent and baby’s interaction seems flat and disengaged.” Cronbach’s alpha for the scale was .72. All coders were blind to the hypotheses of the study and all other coded data from the study. 102 of the 118 tapes (86%) were double-coded for reliability. Seven tapes with low inter-rater reliability were also coded by a third coder. The ratings were averaged across all coders. Inter-rater reliability for emotional disengagement, assessed using intraclass correlations (ICC), was .64. Evidence for concurrent and criterion validity for the ICS has been obtained. Fathers’ attachment status predicts emotional disengagement at 8 months (McFarland-Piazza et al., Reference McFarland-Piazza, Hazen, Jacobvitz and Boyd-Soisson2012). Prenatal marital negativity also predicted parents' ICS emotional disengagement (Gallegos et al., Reference Gallegos, Murphy, Benner, Jacobvitz and Hazen2017). Further, there is continuity in paternal sensitivity from 8 to 24 months (Jacobvitz et al., Reference Jacobvitz, Aviles, Aquino, Tian, Zhang and Hazen2022).
Fathers’ minimizing responses to toddler’s emotional distress
When the children were 24 months old, they visited the laboratory with their parents. At this visit, fathers were videotaped interacting with their child during 20 min of free play in a playroom followed by10 min of cleanup. Fathers were instructed to play with their child as they ordinarily would and during the cleanup portion, fathers were asked to get their child to help clean up as much as possible. The cleanup task was carried out to assess how parents and children responded to children’s negative emotions since children typically did not want to stop playing or clean up. Next, father-child dyads completed two problem-solving tasks requiring parental assistance. Fathers were instructed to first let the child work independently on the problem and then “give any help you think he/she needs.” The first task was typically easy for the child. It involved removing a lure from a space between two closely spaced tubes using a stick. The next task was more difficult, usually requiring parental assistance. Since mother-child interactions also were assessed during this visit, for the second task, half the children completed one of the following two tasks with mother and the other half completed one of the following tasks with fathers. One task involved the child putting bristle blocks end to end, and then pushing the assembled bristle blocks through a long clear plastic tube to remove the lure placed in the middle of the tube. The other task required the child to use a block to weigh down one end of a long wooden level to raise the other end of the level whereby a treat could be reached through a hole in the plexiglass box. Children’s strategies for managing potential frustration (including seeking help from the parent) was observed.
Two coders rated fathers’ minimizing responses to their children’s negative emotions using the Parents' Responses to Children’s Emotions Rating Scales (PRCERS; Boyd-Soisson, Reference Boyd-Soisson2002b), which is based on scales from the Parental Coping with Children’s Negative Emotions Questionnaire (Fabes et al., Reference Fabes, Eisenberg and Bernzweig1990). The minimizing scale, used in the present study, is a 7-point Likert observational rating that examined the degree to which parents dismissed or devalued negative emotions that children expressed. Examples of minimizing responses include sarcasm (e.g., saying, “Oh, it’s the end of the world!”), ignoring the child’s upset behavior, or telling the child that he or she is overreacting (e.g., “Oh, that doesn't hurt, do not be a baby!”). Lower scores reflect an absence of minimizing responses, and higher scores reflect more frequent and intense displays of minimizing responses. Three coders were trained and reliable to utilize the PRCERS, and blind to all other data. When ratings differed across two coders by more than one point, a third trained coder rated the interaction as well. To evaluate reliability, 70% of the videotapes were double-coded, in addition to eight tapes that were conference coded as part of training. The average scores of all raters were used in the analyses. Average ICC for the minimizing scale was high (.85.). Evidence for criterion validity for the PRCERS was obtained. For example, as expected, fathers’ attachment status assessed prior to the child’s birth has been shown to predict minimizing responses with their children at 24 months (Boyd-Soisson, Reference Boyd-Soisson2002b), and mothers’ use of minimizing responses at 24 months was found to predict children’s externalizing behaviors at school age (Murphy et al., Reference Murphy, Jacobvitz, Boyd-Soisson and Hazen2017).
Children’s emotion regulation
At this same laboratory visit, children spent 5–10 min completing two challenging and frustrating tasks in the presence of only the researcher to measure their emotion regulation without parental assistance. The first task consisted of effectively connecting tinker toys to successfully retrieve snacks trapped inside a tube. The second task consisted of retrieving toys from a large, locked plexiglass box. The activities were designed to measure children’s abilities to cope with frustration, as they were too difficult for most children to complete without assistance. The child would need to effectively manage their emotions to then solicit help from the researcher to retrieve the toys.
The tasks were later coded on three 7-point scales using the Children’s Emotion Regulation Scales (Boyd-Soisson, Reference Boyd-Soisson2002a), including children’s adaptive emotion regulation, overregulation, and underregulation. Only the emotional underregulation subscale was used in the present study, given that ADHD symptoms are characterized by emotional reactivity and the lack of ability to inhibit negative emotional expressions (Banaschewski et al., Reference Banaschewski, Jennen-Steinmetz, Brandeis, Buitelaar, Kuntsi, Poustka, Sergeant, Sonuga-Barke, Frazier-Wood, Albrecht, Chen, Uebel, Schlotz, van der Meere, Gill, Manor, Miranda, Mulas, Oades and Asherson2012; Martel, Reference Martel2009; Walcott & Landau, Reference Walcott and Landau2004), and not the overregulation or inhibition of negative emotions. The adaptive emotion regulation subscale also was not used because the low end of this scale included both over- and underregulation, and only underregulation was expected to be related to ADHD symptoms.
Emotional underregulation was characterized by frustration that resulted in crying, screaming, or tantrums, and whether the researcher was unable to calm or comfort the child. An example of emotional underregulation is the child experiencing such extreme distress after failing the task that they were unable to ask the researcher for assistance (verbally or nonverbally, through gestures). Higher scores on the scale indicated higher levels of children’s emotional underregulation. Two observers, who were blind to all other data of the study, were trained by an expert coder using 15% of videotapes. The two observers then rated 65% of the remaining videotapes for reliability and showed high reliability. The reliability scores for emotional underregulation were averaged (ICC = .96). Validation of the emotional underregulation assessment was obtained in two studies. Children’s emotional underregulation has been associated with maternal emotional dysregulation, that is, mothers’ elevated tendency to exhibit distress in response to children’s negative emotions (Aviles et al., Reference Aviles, Reisz, Jacobvitz and Hazen2022). Moreover, fathers’ frightening behaviors with their children at 8 months predicted children’s emotional underregulation at 24 months (Hazen et al., Reference Hazen, McFarland, Jacobvitz and Boyd-Soisson2010).
Attention-deficit/hyperactivity disorder symptoms
Teachers completed the Teacher Report Form (TRF; Achenbach, Reference Achenbach1991) to assess children’s symptoms of ADHD at age 7, using the DSM-IV-oriented ADHD scale. The TRF is composed of 120 items that measure emotional/behavioral problems and social competencies in the school setting for children from ages 4 to 18. The ADHD scale combines the 14 items assessing inattention and 12 items assessing hyperactivity-impulsivity for a total of 26 items with each item rated on a 3-point scale, with 0 indicating “not true,” 1 indicating “somewhat or sometimes true,” and 2 indicating “very true or often true.” Example items include: “Has trouble concentrating or paying attention.” “Can't sit still,” “Can't concentrate,” and “Impulsive or acts without thinking.” Cronbach’s alpha (used to test internal reliability) for the TRF was .95.
Control variables
Infant temperament
Mothers completed the Infant Behavior Questionnaire (IBQ; Rothbart, Reference Rothbart1981) at 3–6 weeks postpartum. The IBQ utilizes 94 items to assess infant behavior on the following six domains: smiling and laughter, fear, distress to limitations, soothability, duration of orienting, and activity level. The activity level subscale of the IBQ was used in the current study (α = .76). The subscale included 7 items that were rated on a 7-point scale, with greater scores indicating higher frequency or intensity of the behavior. Some example items of this subscale are: “During feeding, how often did the baby squirm or kick?” “When placed in an infant seat or car seat, how often did the baby wave arms and kick?”
Fathers’ involvement in infant caregiving
At 8 months postpartum, mothers and fathers were asked to report how much time they each individually spent caring for their infant during a typical week. On a chart for each week, they identified the number of hours, from 6 a.m. to 11 p.m., that they each spent caring for their child in the previous week. Fathers’ share of childcare was calculated by dividing the total number of hours per week that the child was awake and needing care, and then dividing that by the number of hours per week in which the father was solely responsible for the child’s care. In this sample, fathers reported between 0 and 43 hr a week alone caring for their child, with an average of 8.7 hr a week and a standard deviation of 8.9 hr.
Data analyses
A path analysis model was conducted using Mplus Version 8.6. The model examined whether fathers’ emotionally disengaged parenting at 8 months and fathers’ minimizing responses to children’s distress at 24 months would forecast children’s emotional underregulation at 24 months and, subsequently, children’s ADHD symptoms at age 7 (See Figure 1). Missing data were accounted for through the full information maximum likelihood estimation.
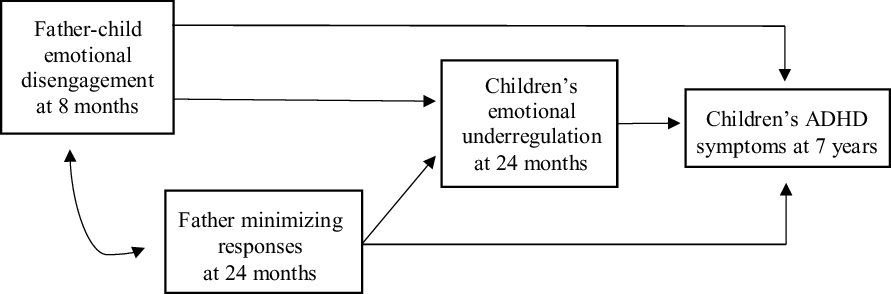
Figure 1. Conceptual model showing influence of father emotional disengagement and minimizing responses on children’s ADHD symptoms through children’s emotional underregulation. Note. Solid lines represent expected significant paths at p < .05. The indirect effect between father emotional disengagement on children’s ADHD symptoms through children’s emotion regulation will be examined. The indirect effect between father minimizing responses on children’s ADHD symptoms through children’s emotional underregulation will also be examined.
The model controlled for family income because it is related to the quality of care parents provide their children (Lombardi, Reference Lombardi2021) and because income differed among those who stayed in the study until 7 years. Child sex was entered as a covariate, given that parents interact with their children differently based on children’s sex (Mascaro et al., Reference Mascaro, Rentscher, Hackett, Mehl and Rilling2017), children may show differences in emotional expression based on their sex (e.g., girls showing more positive emotions; Chaplin & Aldao, Reference Chaplin and Aldao2013), and boys are more often than girls diagnosed with ADHD (Danielson et al., Reference Danielson, Bitsko, Ghandour, Holbrook, Kogan and Blumberg2018). Infant activity level has been associated with ADHD symptoms (Meeuwsen et al., Reference Meeuwsen, Perra, Van Goozen and Hay2019). Thus, infant temperament was entered as a covariate. Further, because children’s temperament influences their emotion regulation abilities (Calkins & Mackler, Reference Calkins, Mackler, Underwood and Rosen2011), temperament was included as a control variable. Lastly, because one-third of the fathers in this sample were uninvolved in caregiving during infancy, and father involvement is likely to influence the extent to which parenting practices are associated with children’s regulatory skills, father involvement was entered as a covariate.
Specifically, family income at 8 months was regressed on fathers’ emotionally disengaged parenting at 8 months, and family income at 24 months was regressed on fathers’ minimizing responses at 24 months. Fathers’ involvement at 8 months was regressed on fathers’ emotionally disengaged parenting at 8 months, fathers’ minimizing responses at 24 months, children’s emotional underregulation at 24 months, and children’s ADHD symptoms at 7 years. Infant sex was regressed on fathers’ emotionally disengaged parenting at 8 months, fathers’ minimizing responses at 24 months, and children’s ADHD symptoms at 7 years. Infant sex and infant activity level at 3–6 weeks postpartum were regressed on children’s emotional underregulation at 24 months and ADHD symptoms at 7 years.
Results
Table 1 provides means, standard deviations, and ranges for the variables of interest. Table 2 provides bivariate correlations for all study variables. Father-child emotional disengagement was positively associated with child emotional underregulation and negatively associated with family income at 8 months. Father minimizing responses was positively associated with child emotional underregulation and ADHD symptoms. Child emotional underregulation was positively associated with children’s ADHD symptoms. ADHD symptoms was negatively associated with family income at 8 months. Father involvement was negatively associated with family income at 8 months and positively associated with family income at 24 months.
Table 1. Means, sample sizes, standard deviations, and range of variables of interest
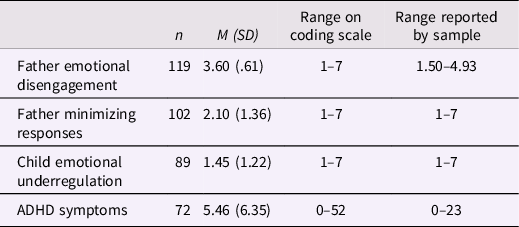
Note: Father emotional disengagement was assessed at 8 months. Father minimizing responses and children’s emotional underregulation were assessed at 24 months. ADHD symptoms were assessed at 7 years.
Table 2. Bivariate correlations of study variables
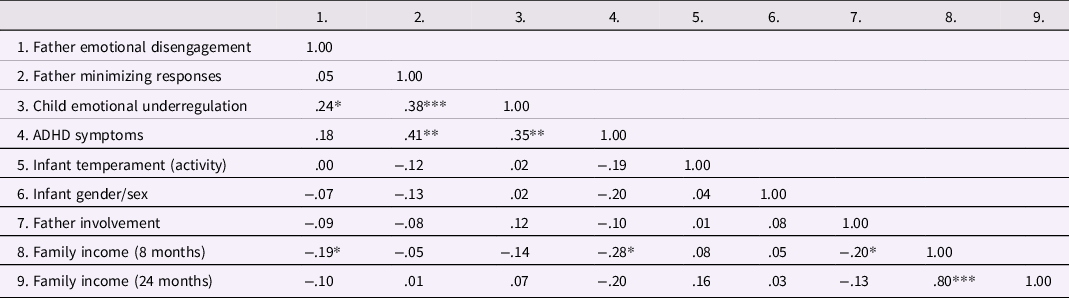
Note. Significance levels are: *p < .05, **p < .01, and ***p < .001. Father emotional disengagement was assessed at 8 months. Father minimizing responses and children’s emotional underregulation were assessed at 24 months. ADHD symptoms were assessed at 7 years. Infant temperament and gender/sex were assessed 3–6 weeks postpartum. Father involvement was assessed at 8 months. Family income was assessed at 8 and 24 months.
Figure 2 shows the results for the path analysis. The model fit the data well, χ2 (10) = 9.72, p = .47, root mean square error of approximation = .00 (90% CI = .00, .10), comparative fit index = 1.00, Tucker–Lewis index: 1.02, standardized root mean square residual = .05. The results indicated that fathers’ emotional disengagement at 8 months predicted children’s emotional underregulation at 24 months (β = .27, p < .01). That is, children of fathers who were disengaged when they were infants displayed more emotional underregulation at 24 months old. Moreover, fathers’ minimizing responses to children’s distress at 24 months were associated with children’s emotional underregulation at 24 months (β = .41, p < .001). That is, more displays of paternal minimizing responses were related to greater child emotional underregulation at 24 months. In turn, children’s emotional underregulation at 24 months predicted ADHD symptoms at age 7 (β = .35, p < .01). That is, children who displayed greater emotional underregulation at 24 months showed more ADHD symptoms at age 7. The indirect effect between fathers’ emotionally disengaged parenting and children’s later ADHD symptoms was significant (β = .10, p < .05). Similarly, the indirect effect between fathers’ minimizing responses to children’s distress and children’s later ADHD symptoms was significant (β = .14, p < .01).
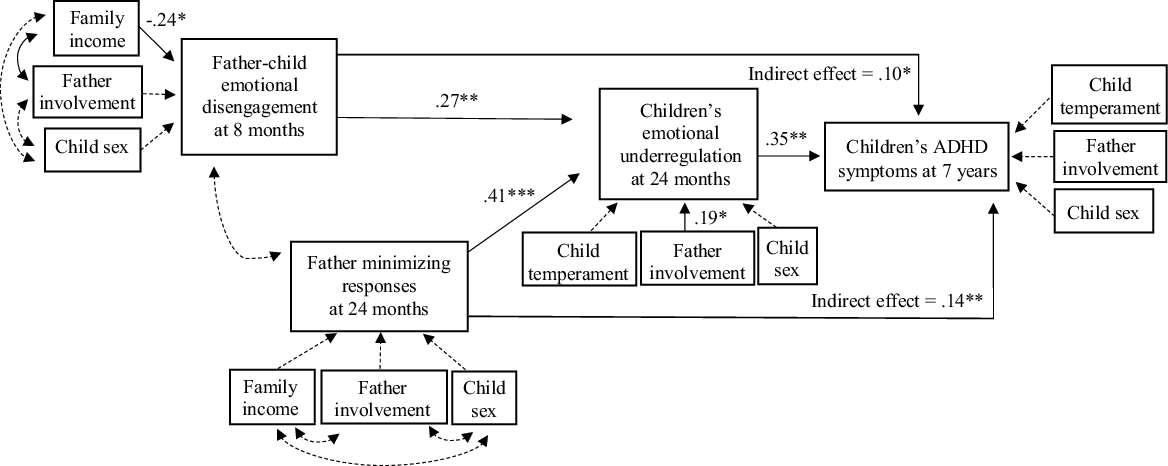
Figure 2. Model showing the influence of father emotional disengagement and minimizing responses on children’s ADHD symptoms through children’s emotional underregulation. Note. Solid lines represent significant paths at p < .05. Dashed lines represent nonsignificant paths. Significance levels are ***p < .001, **p < .01, and *p < .05. Both indirect effects between father emotional disengagement and minimizing responses on children’s ADHD symptoms through children’s emotional underregulation were significant.
Discussion
The present study extended the research that has previously focused almost entirely on the contribution of early maternal care to ADHD symptoms by investigating the longitudinal associations between fathers’ parenting in infancy and toddlerhood and their children’s ADHD symptoms in middle childhood, through children’s emotion regulation in early childhood. Specifically, we examined two distinct paternal behaviors, emotional disengagement in infancy and minimizing responses to children’s distress in toddlerhood, in relation to their children’s emotion regulation in toddlerhood and ADHD symptoms in middle childhood. This specificity allows for greater identification of parenting behaviors that are important for the development of children’s early emotion regulation. This study is also one of the first to examine the unique role of paternal care in the development of ADHD symptoms in children.
Results demonstrated that fathers’ disengaged behavior with their infants at 8 months and minimizing responses to their children at 24 months predict their children’s poor emotion regulation at 24 months, which in turn predicts the development of ADHD symptoms at 7 years. Our investigation also revealed that fathers’ minimizing responses to their children’s distress at 24 months are associated with children’s poor emotion regulation at 24 months.
Our findings add to a growing body of literature, suggesting that fathers play an important role in their children’s development of emotion regulation, presumably because they tend to engage in stimulating and challenging play (Volling et al., Reference Volling, Stevenson, Safyer, Gonzalez, Lee, Volling and Cabrera2019). Fathers’ stimulating interactions with their infants may provide unique opportunities for infants to up-regulate and down-regulate their levels of arousal and develop self-regulatory skills. This up and down modulation may then shape children’s biological systems in developing adaptive responses to emotionally challenging situations (Porges & Furman, Reference Porges and Furman2011). Further, fathers can scaffold appropriate behavioral strategies for regulating arousal both when children are getting excited and when they are attempting to calm down. When fathers disengage with their children, they are unable to facilitate skills that may lead to more sophisticated regulatory strategies at both a behavioral and a biological level. Moreover, when fathers respond to their children’s negative emotions by minimizing them, they invalidate and devalue their children’s feelings and emotional experience, thus, teaching their children that expressing and feeling negative emotions is not appropriate. When children cannot turn to their parents for comfort during times of distress, they are not provided with opportunities to observe and practice adaptive emotion regulation skills. Therefore, when fathers withdraw or minimize, not acknowledging or valuing their children’s difficult emotions, children are forced to manage their emotions on their own, leading to inappropriate emotional underregulation (Eisenberg & Fabes, Reference Eisenberg and Fabes1994).
This study is one of the first to provide evidence for the role of paternal caregiving in the development of ADHD symptoms in children. Maternal insensitive caregiving behaviors that involve intrusiveness and interference have been associated with children’s difficulties with emotion regulation (e.g., Halligan et al., Reference Halligan, Cooper, Fearon, Wheeler, Crosby and Murray2013) and later ADHD symptoms (Carlson et al., Reference Carlson, Jacobvitz and Sroufe1995; Jacobvitz & Sroufe, Reference Jacobvitz and Sroufe1987). We expected that, because fathers typically engage in stimulating play that can provide infants with opportunities to regulate their behavior, fathers’ emotionally disengaged behavior during infancy and minimizing their child’s distress during toddlerhood would contribute to children’s difficulties with self-regulation and the development of ADHD symptoms in young children. Data in the present study provide evidence for this hypothesis. Fathers’ disengagement and minimizing behaviors may have long-term impacts on children’s emotion regulation and, subsequently, manifestations of ADHD symptomatology.
This work has important implications for understanding early developmental pathways that place children on trajectories that may lead to increased inattention and hyperactivity. Our findings also aid in intervention and prevention efforts given that early parenting behaviors can be addressed during infancy and toddlerhood to prevent negative emotional or behavioral outcomes in children, including poor impulse control and physical aggression (Sullivan et al., Reference Sullivan, Helms, Kliewer and Goodman2010), as well as poor academic outcomes due to the inability to focus on school work (Graziano et al., Reference Graziano, Reavis, Keane and Calkins2007). Early regulatory skills have also been tied to later higher-order cognitive abilities associated with executive functioning, including attention and inhibitory control (Colombo, Reference Colombo2001). Executive functioning capacities, including attention and inhibitory control, are supported in the prefrontal cortex, which undergoes major structural and functional changes during infancy (Diamond, Reference Diamond, Levin, Eisenberg and Benton1991). Thus, infancy is a critical period for the development of these early regulatory skills, and fathers’ parenting behaviors may play a key role in their development.
Drawing on the family systems theory, it might be important for future studies to examine how interconnections among relationships in the same family are related to children’s self-regulatory skills. Boundary disturbances during triadic (mother, father and toddler) interactions, which involved mothers forming an alliance with their child or parents putting children in the middle of their conflict, have been found to forecast ADHD in middle childhood (Jacobvitz et al, Reference Jacobvitz, Hazen, Curran and Hitchens2004). In these families, fathers were more likely to become disengaged. Fathers may also be more likely to disengage with their infants when mothers are more intrusive (and vice versa). These experiences with both parents may then make it significantly more difficult for children to regulate emotion, elevating the risk of developing inattentive, impulsive, and hyperactive symptoms of ADHD. Future work is needed to investigate this possibility. It is also possible that multiple types of fathering behaviors have an impact on children’s ADHD symptoms, with some fathers being emotionally disengaged and others interfering with their child’s ongoing moods and interests. It will be important for future studies to examine whether father intrusiveness is related to the development of ADHD symptoms and if so, whether these behaviors are uniquely predictive above and beyond minimizing and disengaging behavior.
It is important to consider the conclusions from the present study in light of its limitations. First, it is worth noting that the current sample size is small, due to our longitudinal design following families for 7 years, the use of qualitative interviews, and observations of parent-child interactions in different contexts. Moreover, although the sample from the study was generally socioeconomically diverse, with 17% of the sample living below the poverty line, the generalizability of these findings remains limited based on the racial and ethnic characteristics of the sample and may not be generalizable to racial and ethnic minority populations. In addition, given the restraints of our data, parents’ minimizing responses were measured at the same time point as children’s emotion regulation, making the direction of causality less clear. That is, it is possible that fathers might respond in a more minimizing way when their toddlers display more emotional outbursts. With this in mind, future longitudinal studies are needed to examine whether parents’ minimizing responses in their first year predict children’s emotion regulation in a larger sample. Similarly, it is important to examine the reciprocal relation between parent and child behavior, especially for the relation between fathers’ minimizing responses and children’s emotional regulation, as these were measured at the same time point. It may be the case that children with biological predispositions to be emotionally distressed (e.g., temperamentally reactive) may be more likely to provoke negative responses from some parents (e.g., minimizing behaviors), and parents' minimizing reactions could, as a result, further undermine children’s emotion regulation. Further, the current study utilized a sample of married, different-gender/sex couples. Thus, these findings cannot be generalized to the role of fathers in more diverse families (e.g., same-gender/sex couples, single parents). Future studies must also examine these relations with same-gender/sex couples and single fathers, as they continue to be underrepresented in parenting research. Lastly, a potential drawback of the current sample is that it is a community sample rather than a clinical sample with children diagnosed with ADHD, thus, restricting the maximum values for ADHD symptoms. The level of emotional disengagement observed in the current sample may be higher in samples with clinically diagnosed children. Therefore, it will be important to replicate this study using a clinical sample of children diagnosed with ADHD to determine whether similar or different mechanisms could play a role for these children.
Despite these limitations, this study also has several methodological strengths. Whereas most studies rely on self-report data when assessing parenting quality and parents’ reports of child outcomes, the current study used observational assessment of father-infant dyads interacting across multiple contexts (i.e., play, feeding, changing clothes) at home, a naturalistic environment, when infants were 8 months, and in a laboratory context with structured tasks at 24 months. Further, unlike most previous studies that obtain parent reports of childhood behavior problems in middle school, we obtain reports from teachers, thus eliminating potential parental bias and adding robustness to the findings. Another strength of the study is that we utilize parent-child observations and teacher reports, which reduce shared method bias. Additionally, by examining parenting behaviors in early childhood and ADHD symptoms in middle childhood, we addressed a gap in the literature that researchers urged must be examined. Specifically, Nigg et al. (Reference Nigg, Sibley, Thapar and Karalunas2020) emphasized that “Parent-child processes preceding clinical ADHD in the first 12–24 months of life are hardly studied – despite an established literature on the role of early parenting in the consolidation of self-regulation” and posed the question regarding whether sensitive parenting practices in early childhood could prevent ADHD in some cases.
Finally, most parenting programs continue to focus primarily on mother-child dyads (Panter-Brick et al., Reference Panter-Brick, Burgess, Eggerman, McAllister, Pruett and Leckman2014). Findings in this study highlight the importance of adapting the content and goals of specific interventions to more appropriately engage fathers and assist them based on the unique contribution that they have to their children’s emotional development. Specifically, because fathers are less emotionally expressive than mothers (Wong et al., Reference Wong, McElwain and Halberstadt2009) and mask their emotional experiences more than mothers (Dunsmore et al., Reference Dunsmore, Her, Halberstadt and Perez-Rivera2009), parenting interventions for fathers must address these issues that are unique to them. For instance, these interventions could focus on addressing the role of socialization of gender expectations on emotional expression (i.e., males expected to suppress their emotions), which may lead to fathers experiencing fewer difficulties with emotional expression as well as learn how to engage in conversations with their children about their emotions. The findings from the current study emphasize that fathers’ parenting behaviors play a unique role in the development of their infants and toddlers’ emotional development. Knowing that fathers’ emotional disengagement and minimizing responses hinder their children’s emotion regulation and, as a result, may lead to the development of ADHD symptoms, these results can be implemented in future research studies and parenting programs to foster positive father-child relationships and enhance children’s overall development.
Funding statement
This research was supported by the National Science Foundation (NH and DJ, grant number SBR-9212990) and the Hogg Foundation for Mental Health (NH and DJ, grant number 3332).
Conflicts of interest
None.





 Open access
Open access