



This study shows the importance of psychosocial early action in the face of a natural catastrophe. Policy actions could include the provision of this service in the most affected areas. Specifically, the present study identified people with mental health problems and under pharmacological treatment, those who lived in a region affected by the catastrophe, and women as vulnerable groups.
On 19th September 2021, the ”Tajogaite" volcano erupted on the island of La Palma in the Canary Islands, Spain. Although a volcanic risk alert had been issued by the competent authorities, the eruption surprised the residents of the island and they had to immediately evacuate their homes. The active eruption lasted until 13th December 2021 (Instituto Geográfico Nacional [National Geographic Institute], 2021), and the damage caused by the volcano was dramatic, ranging from material losses (1,218.87 hectares of land and more than 1,600 buildings were affected) (Cabildo Insular de La Palma, 2021) to economic (e.g., local business closing), and social impact (e.g., reallocation of people, or physical health consequences including exposure to toxic gases and the associated stress burden). Undoubtedly, the eruption was a great shock for residents and people close to La Palma (e.g., non-residents born in the island), whom had and will have to also face some psychological consequences.
Previous studies have evaluated the effects of volcanic eruptions on the mental health. For example, the most frequent symptomatology during the acute phase after different natural catastrophes in Japan (one of them a volcano) were anxiety, mood and physical symptoms, and sleep problems (Takagi et al., Reference Takagi, Takahashi, Fukuo, Arai and Tachikawa2021). In another study on the eruption of the Japanese Miyake Island in 2000, it was found that material losses and uncertainty were significantly associated with higher rates depression, being specially affected those participants who had lived longer on the island, had previous evacuation experiences, or had a lower socioeconomical status (Goto et al., Reference Goto, Wilson, Kahana and Slane2006). Also, in the Ambae Island in Vanuatu, the mental distress of displacement due to a volcano eruption was higher among women who had no support available (Zahlawi et al., Reference Zahlawi, Roome, Chan, Campbell, Tosiro, Malanga, Tagaro, Obed, Iaruel, Taleo, Tarivonda, Olszowy and Dancause2019). In addition, from the perspective of mental well-being, the long-term effect of other natural disasters on this variable has been studied, finding that physical factors such as the natural environment or safety, as well as meaningful or social activities, affected well-being in a consistent and cumulative manner (Ampuero et al., Reference Ampuero, Goldswosthy, Delgado and Miranda2015). Furthermore, psychological well-being can be affected after a volcanic eruption, even in those who have not been evacuated (Gissurardóttir, Reference Gissurardóttir2015).
There are also some studies looking at the long-term impact of natural disasters. Ohta et al. (Reference Ohta, Araki, Kawasaki, Nakane, Honda and Mine2003), found that the proportion of evacuees with anxiety decreased significantly from 66.1% to 45.6% from 6 months to 44 months after a Japanese volcanic eruption, while depression levels remained stable until 44 months after the disaster. Authors also found that recovery was more difficult for older people in general. Also, a study examining the impact of the Eyjafjallajökull volcano eruption in Iceland in 2010 showed that mental health effects, i.e., mental distress, post-traumatic stress disorder (PTSD) and perceived stress, were persistent between 6 and 9 months following the event, both in exposed and unexposed people (Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018). It was also found that, after 3 years of the experience, exposed people showed higher levels of insomnia than at the time of the event, while psychological distress and perceived stress remained similar, and PTSD symptoms decreased (Hlodversdottir et al., Reference Hlodversdottir, Petursdottir, Carlsen, Gislason and Hauksdottir2016). Given this longitudinal evidence, it was important to evaluate the psychological impact of the eruption of the Tajogaite volcano in La Palma to support and expand this knowledge.
Longitudinal research has also looked at the moderators of the impact when living a natural disaster. It has been found that mental health is more affected in people physically closest to the area of the disaster, highlighting the place attachment importance (Hidalgo & Hernández, Reference Hidalgo and Hernández2001). For example, Carlsen et al. (Reference Carlsen, Hauksdottir, Valdimarsdottir, Gíslason, Einarsdottir, Runolfsson, Briem, Finnbjornsdottir, Gudmundsson, Kolbeinsson, Thorsteinsson and Pétursdóttir2012), found greater psychological morbidity among residents close to the eruption zone, as well as among people who showed physical symptomatology 6–9 months after the disaster. Warsini et al. (Reference Warsini, Buettner, Mills, West and Usher2015) found that two years after a volcano eruption in Indonesia, survivors closest to the area and women who owned their own home had higher scores of concerns regarding the impact of the event. In Spain, Ruiz and Hernández (Reference Ruiz and Hernández2014) found that place attachment diminished in the residents nearest the volcanic process, with more active coping strategies. It was found that the proximity to the disaster was related to levels of fear, anger, loss, and active confrontation, being higher on towns nearer the volcano. In addition, although the eruption had almost no material or human damage, there was a significant psychological impact. It is important to know whether these results would replicate in a similar situation and context such as the eruption of the Tajogaite volcano in La Palma.
Taking this evidence into account, the aim of the present study was to evaluate the psychological impact that the eruption of the Tajogaite volcano had on La Palma population and on people related to the island (i.e., people who are not currently living on the island, but are somehow connected to it) during the last moments of the eruption and subsequent months. Sociodemographic variables, the levels of depression, anxiety, perceived stress, and psychological well-being were evaluated. Descriptive analyses and regression models were carried out to identify the main predictors and protectors of the psychological impact of the natural disaster short and medium term (6 weeks, one month, and six months after the eruption).
The main hypothesis raised in this study was that levels of anxiety will decrease in time, while depression and perceived stress levels will remain stable, something in line with the information provided by previous studies on this topic (Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018).
Method
Procedure
An exploratory longitudinal study was designed with three self-administered online evaluations after the eruption of the volcano: From November 3rd 2021 (six and a half weeks after the start of the eruption) to December 9th 2021 (Wave 1); after 2 months, from January 26th 2022, to February 22nd 2022 (Wave 2); and after 7 months, from June 21st 2022, to July 11th 2022 (Wave 3). In a snowball sampling, participants were contacted via WhatsApp, email, Facebook and close friends asking for volunteers to complete a self-administered survey about the impact of the volcanic eruption.
Prior to completing the assessment, participants were informed about the study and signed the informed consent form. They were given the option to provide their email account to be contacted in the future. For data protection, a pseudo-randomization approach was used where two different files were created: One file contained the email account and an anonymous code and another file contained the anonymous code and the answers to the questionnaires. Only researchers in this study had access to these data. Moreover, the study was approved by the ethical board of the School of Psychology of the university (Internal Ref.: CE_20220317–02_SAL) and data was treated following the Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation).
Participants
Using the snowball sampling, 487 participants was recruited in the first wave (N W1 = 487). Sixteen participants were excluded for being younger than 18 years old, leaving a final sample size of 471 participants. Those who provided their email direction were contacted again after 2 months (Wave 2) (N W2 = 90, 19.1%) and after 7 months (Wave 3 N W3 = 47, 10%). Sample size was not calculated a priori, it was a convenient sample based on the following inclusion criteria: (a) Being a resident of La Palma or having close contact with the island (home, work, farms, relatives, friends and/or acquaintances), and (b) and being older than 18 years old. There were no other exclusion criteria. The real percentage of attrition cannot be calculated given that 122 participants were excluded from Wave 1, 53 from Wave 2, and 21 from Wave 3 because they lacked an identifier (did not provide their email to be contacted in the future).
Variables and Instruments
Sociodemographic Characteristics
Participants reported their age, gender (male, female, non-binary) whether they were studying or working and whether they lived alone or accompanied. Also, they reported their residential status, i.e., being resident of the island and present during the eruption, resident of the island but not present during the eruption, or non-resident but close contact with the island.
Ad hoc yes-no questions were used to ask participants if they had been evacuated and if they had suffered any type of loss, taking into account the characteristics of the island’s population (“Do you live in a region that has been directly affected by the volcano?”; “Have you been evacuated and also lost material objects (house, belongings…) because of the volcano?”; “Have you been evacuated and also lost farms or orchards because of the volcano?”; Have you been evacuated and also lost your job because of the volcano?”).
Finally, participants reported whether they had ever received a diagnosis of mental disorder and whether they had received psychopharmacological treatment in their life.
Psychological Impact
Depressive symptomatology was measured by the Patient Health Questionnaire–9 (PHQ–9; Spitzer et al., Reference Spitzer, Kroenke and Williams1999), which is a self-report questionnaire based on “Diagnostic and Statistical Manual of Mental Disorders, 4th Ed.” (DSM–IV) depression criteria (American Psychiatric Association, 1994). The scale is composed by 9 items evaluating the frequency of each symptom from 0 (Never) to 3 (Almost every day). Scores were calculated by adding up the values of each item and can be categorized in minimal (0–4), mild (5–9), moderate (10–14), moderate-severe (15–19), and severe (20–27) depressive symptomatology. The Spanish version of the questionnaire (Cassiani-Miranda et al., Reference Cassiani-Miranda, Vargas-Hernández, Pérez-Aníbal, Herazo-Bustos and Hernández-Carrillo2017) was used in this study and reliability was good, Cronbach’s alpha. 89.
Anxiety symptoms were evaluated with the Generalized Anxiety Disorder–7 (GAD–7; Spitzer et al., Reference Spitzer, Kroenke, Williams and Löwe2006), a 7-item self-report questionnaire to assess anxiety according to the DSM–IV diagnostic criteria. Each item was rated on a four-point scale from 0 (Not at all) to 3 (Nearly every day), with the final score being between 0–21 (calculated by adding up the values of each item). The total score can be categorized into four severity groups: Minimal (0–4), mild (5–9), moderate (10–14), and severe (14–20). The Spanish version of the questionnaire was used in this study (García-Campayo et al., Reference García-Campayo, Zamorano, Ruiz, Pardo, Pérez-Páramo, López-Gómez, Freire and Rejas2010) and test-retest reliability was excellent in the present sample, Cronbach’s alpha. 92.
Perceived stress was assessed using the Spanish version of the Perceived Stress Scale (PSS; Cohen et al., Reference Cohen, Kamarck and Mermelstein1983; Remor, Reference Remor2006). It consists of 14 self-report items that evaluate the level in which participants felt stress in relation to the events occurred during the last month (e.g., During the last month, how often did you feel unable to control the important things in your life?). Frequency was rated from 0 (Never) to 4 (Very often). Total scores were calculated by reversing the scores of inverse items (4, 5, 6, 7, 9, 10, and 13), so that higher scores reflect higher levels of perceived stress, and then adding up the values of each item. This questionnaire showed good test-retest reliability in the present sample, Cronbach’s alpha. 88.
Well-being was measured using the Pemberton Happiness Index (PHI; Hervás & Vázquez, Reference Hervás and Vázquez2013), which is a self-report measure to evaluate remembered well-being. It consists of 11 items measuring the level of agreement with sentences such as “I feel very satisfied with my life” from 0 (Totally disagree) to 10 (Totally agree). Total scores were calculated by reversing Item 10, adding up each item and dividing the score by 11, so that higher scores reflect higher levels of well-being. Test-retest reliability for the PHI in the present sample was good, Cronbach’s alpha. 88.
Data Analysis
Descriptive analyses were conducted to evaluate sociodemographic characteristics and symptomatology levels of the sample at the different time points. Then, correlation analyses were carried out to explore the relationships between depression, anxiety, perceived stress, and well-being, and sociodemographic variables in all three waves. Given that depression, well-being and age did not follow a normal distribution, Spearman correlations were calculated between quantitative variables. Moreover, the Kruskall Wallis test was computed between quantitative and polytomous variables and point biserial correlations were calculated between quantitative and dichotomous variables. Finally, multilevel lineal models were computed to evaluate the change of symptoms in time and potential predictors of that change. The hierarchical structure of the data was considered by grouping observations into time points (Wave 1, 2, and 3). Intraclass Correlation Coefficients (ICC) were computed to evaluate whether this aggrupation could explain a high proportion of variance (> 30%). Then, models with random intercepts and fixed slopes were compared to models with random intercepts and slopes to evaluate which one had a significantly higher fit. All the analyses were carried out in RStudio and multilevel lineal models were computed using library(nlme).
Results
Sociodemographic Characteristics
The sample included participants from 18 to 70 years old, being the man age approximately 37 years old in all waves. Also, most of the sample was composed by women, did not live alone, and had an occupation (study or work). Moreover, most participants were residents who were present in the island at the time of the eruption, but less than a half of the sample lived in a region that had been directly affected by the volcano. Regarding loss, around 15% of the sample had been evacuated and lost some material objects because of the eruption, around 10% had been evacuated and lost farms or orchards, and only around 4% had been evacuated and lost their job. Finally, around 25% of the sample had received a diagnosis of mental disorder or symptomatology in their life, and around 40% had received psychopharmacological treatment (anxiolytics, antidepressants, relaxants, etc.), but less than a half had been prescribed by a doctor or psychiatrist. Details of demographic information can be found in Table 1.
Table 1. Demographic Information and Mean Levels of Symptomatology of La Palma Population in Wave 1 (Six and a Half Weeks after the Volcanic Eruption), Wave 2 (2 Months Later) and Wave 3 (7 Months Later)

Note. N Wave 1 = number of participants with inclusion criteria; N Wave 2 = number of participants who could be identified as having completed Evaluations 1 and 2; N Wave 3 = number of participants who could be identified as having completed Evaluations 1, 2, and 3. PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalized Anxiety Disorder-7; PSS-14 = Perceived Stress Scale; PHI = Pemberton Happiness Index.
Correlation between Variables
Depressive symptoms was significantly correlated to anxious symptoms (ρ = .84, p < .001), perceived stress (ρ = .80, p < .001), and well-being (ρ = –.71, (p < .001). Also, depression levels were significantly correlated to residential situation (
 $ {\unicode{x03C7}}^2 $
= 8.27, p = .02), living alone (rpb = .21, p = .002), living in a region directly affected by the volcano (rpb = .30, p < 001), having been evacuated and also lost material objects, farms or orchards, or the job (rpb = .25, p < .001; rpb = .24, p < .001; rpb = .18, p = .008, respectively), having ever received a mental health diagnosis (rpb = .36, p < .001), and having ever taken psychotropic drugs (rpb = .43, p < .001). However, depressive symptoms was not significantly correlated with age (ρ = .07, p = .27), gender
$ {\unicode{x03C7}}^2 $
= 8.27, p = .02), living alone (rpb = .21, p = .002), living in a region directly affected by the volcano (rpb = .30, p < 001), having been evacuated and also lost material objects, farms or orchards, or the job (rpb = .25, p < .001; rpb = .24, p < .001; rpb = .18, p = .008, respectively), having ever received a mental health diagnosis (rpb = .36, p < .001), and having ever taken psychotropic drugs (rpb = .43, p < .001). However, depressive symptoms was not significantly correlated with age (ρ = .07, p = .27), gender
 $ \Big(\unicode{x03C7} $
2 = 5.99, p = .05), or occupation (rpb = –.06, p = .38).
$ \Big(\unicode{x03C7} $
2 = 5.99, p = .05), or occupation (rpb = –.06, p = .38).
Regarding anxious symptoms, it was significantly correlated with perceived stress and well-being (ρ = .71, p < .001; ρ = –.49, p < .001, respectively). Also, anxiety levels were significantly correlated with gender (
 $ {\unicode{x03C7}}^2 $
= 10.91, p = .004), living alone (rpb = .16, p = .02), living in a region directly affected by the volcano (rpb = .36, p < .001), having been evacuated and also lost material objects, farms or orchards (rpb = 0.25, p < .001; rpb = .23, p < .001), having ever received a mental health diagnosis (rpb = .29, p < .001), and having ever taken psychotropic drugs (r
pb = .40, p < .001). However, anxious symptoms were not significantly correlated with age (ρ = .08, p = .22), residential situation (
$ {\unicode{x03C7}}^2 $
= 10.91, p = .004), living alone (rpb = .16, p = .02), living in a region directly affected by the volcano (rpb = .36, p < .001), having been evacuated and also lost material objects, farms or orchards (rpb = 0.25, p < .001; rpb = .23, p < .001), having ever received a mental health diagnosis (rpb = .29, p < .001), and having ever taken psychotropic drugs (r
pb = .40, p < .001). However, anxious symptoms were not significantly correlated with age (ρ = .08, p = .22), residential situation (
 $ {\unicode{x03C7}}^2 $
= 5.88, p = .05), occupation (rpb = –.03, p = .66), or having been evacuated and also lost the job (rpb = .09, p = .16).
$ {\unicode{x03C7}}^2 $
= 5.88, p = .05), occupation (rpb = –.03, p = .66), or having been evacuated and also lost the job (rpb = .09, p = .16).
Moreover, perceived stress was significantly correlated to well-being (ρ = –.67, p < .001), gender (
 $ {\unicode{x03C7}}^2 $
= 6.34, p = .04), living in a region directly affected by the volcano (r = .21, p = .002), having ever received a mental health diagnosis (rpb = .32, p < .001), and having ever taken psychotropic drugs (rpb = .28, p < .001). However, it was not significantly correlated with age (ρ = –.03, p = .67), residential situation (
$ {\unicode{x03C7}}^2 $
= 6.34, p = .04), living in a region directly affected by the volcano (r = .21, p = .002), having ever received a mental health diagnosis (rpb = .32, p < .001), and having ever taken psychotropic drugs (rpb = .28, p < .001). However, it was not significantly correlated with age (ρ = –.03, p = .67), residential situation (
 $ {\unicode{x03C7}}^2 $
= 4.33, p = .11), living alone (rpb = .09, p = .17), occupation (rpb = .05, p = .42), or having been evacuated and also lost material objects, farms or orchards, or the job (rpb = .12, p = .07; rpb = .13, p = .05; rpb = .09, p = .16).
$ {\unicode{x03C7}}^2 $
= 4.33, p = .11), living alone (rpb = .09, p = .17), occupation (rpb = .05, p = .42), or having been evacuated and also lost material objects, farms or orchards, or the job (rpb = .12, p = .07; rpb = .13, p = .05; rpb = .09, p = .16).
Finally, worse well-being levels were significantly correlated to gender (
 $ {\unicode{x03C7}}^2 $
= 6.57, p = .04), living alone (rpb = –.17, p = .01), having been evacuated and lost farms or orchards (rpb = –.21, p = .002), having ever received a mental health diagnosis (rpb = –.39, p < .001), and having ever taken psychotropic drugs (rpb = –.31, p < .001). However, well-being levels were not significantly correlated with age (ρ = .02, p = .78), residential situation (
$ {\unicode{x03C7}}^2 $
= 6.57, p = .04), living alone (rpb = –.17, p = .01), having been evacuated and lost farms or orchards (rpb = –.21, p = .002), having ever received a mental health diagnosis (rpb = –.39, p < .001), and having ever taken psychotropic drugs (rpb = –.31, p < .001). However, well-being levels were not significantly correlated with age (ρ = .02, p = .78), residential situation (
 $ {\unicode{x03C7}}^2 $
= 1.60, p = .45), occupation (rpb = .00, p = .98), living in a region directly affected by the volcano (r = –.08, p = .24), or having been evacuated and also lost material objects or the job (rpb = –.07, p = .33; rpb = –.13, p = 05).
$ {\unicode{x03C7}}^2 $
= 1.60, p = .45), occupation (rpb = .00, p = .98), living in a region directly affected by the volcano (r = –.08, p = .24), or having been evacuated and also lost material objects or the job (rpb = –.07, p = .33; rpb = –.13, p = 05).
Multilevel Regression Models
Multilevel lineal models were computed to evaluate the change of symptoms in time (see Figure 1 and Tables 2 and 3) and potential predictors of that change, i.e., those variables identified as significant in correlation analyses. In all cases, ICCs were above 30% showing that grouping observations into time points explained a high percentage of variance. Moreover, the use of random slopes did not show a significantly better fit than the use of fixed slopes in any case according to the Likelihood Ratio test (LRModel 1 = 1.91, p = .38; LRmodel 2 = 2.37, p = .31; LRModel 3 = 0.01, p = .99; LRModel 4 = 0.02, p = .99). Therefore, all models were computed with random intercepts and fixed slopes, i.e., assuming that individuals started with varying levels of symptomatology, but they had the same pattern of change at the following time points.

Figure 1. Change in Depression, Anxiety, Perceived Stress, and Well-being in Time (Waves 1, 2, and 3) after the Tajogaite Volcano Eruption in la Palma
Table 2. Correlations between Variables in All Waves
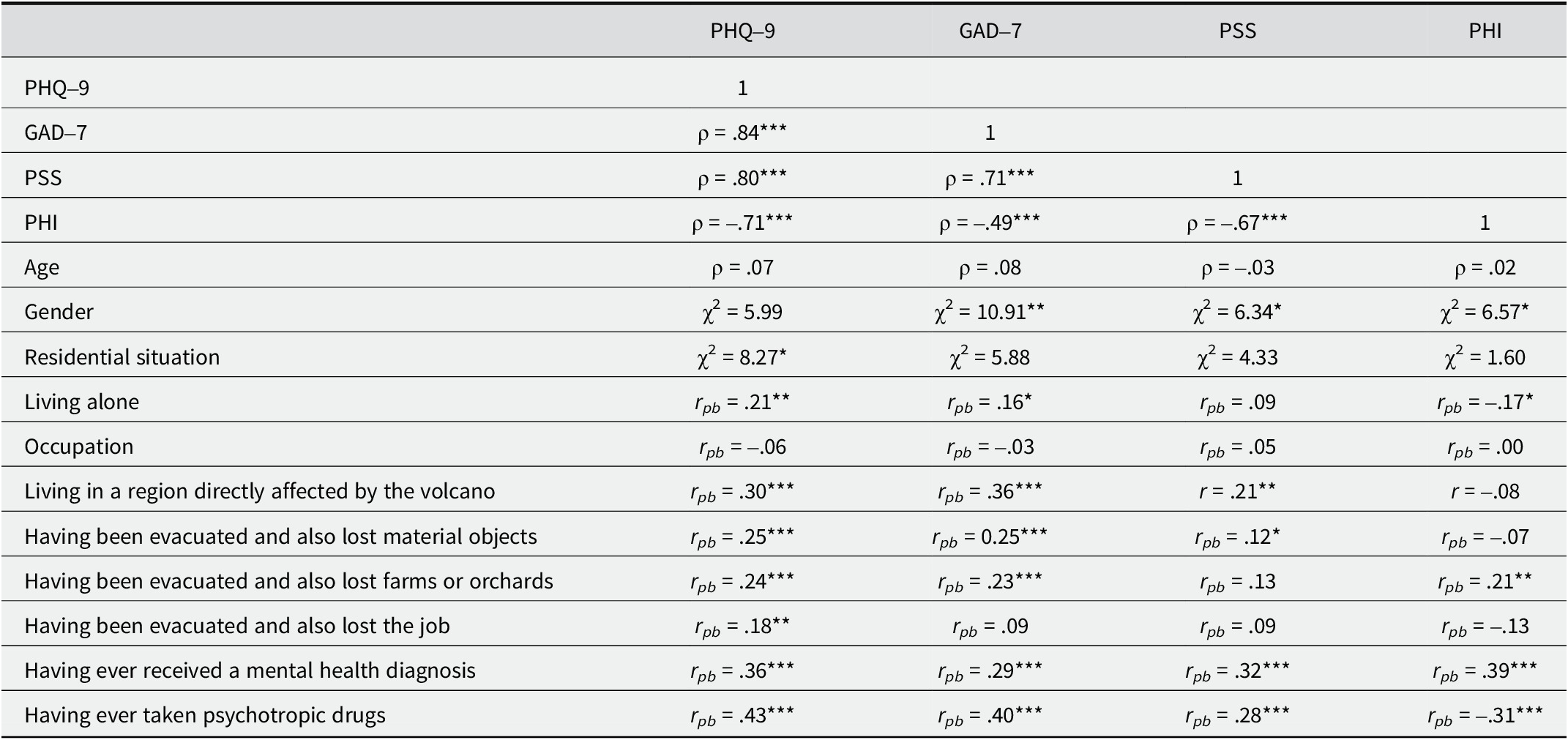
Note. Spearman correlations were calculated between quantitative variables, the Kruskall Wallis test was computed between quantitative and polytomous variables, and point biserial correlations were calculated between quantitative and dichotomous variables.
*** <.001. ** <.01. * <.05.
Table 3. Multilevel Models Evaluating the Prediction of Depressive Symptoms, Anxiety, Perceived Stress, and Well-being

Note: N observations = 223; N groups = 96; ICC = Intraclass Correlation Coefficient to compare null models with fixed and random intercepts. Model 1 evaluates the prediction of depressive symptoms; Model 2 evaluates the prediction of anxious symptoms; Model 3 evaluates the prediction of perceived stress; Model 4 evaluates the prediction of well-being.
Model 1
Model 1 included depressive symptoms as the dependent variable and time, anxious symptoms, perceived stress, well-being, residential situation, living alone, living in a region affected by the eruption, having been evacuated and lost materials, farms or orchards, or the job, having ever received a mental diagnosis, and having ever taken pharmacological treatment as predictors. It was found that time did not significantly explain depression scores. However, anxious symptoms, perceived stress, well-being, and having ever taken pharmacological treatment were significant predictors. Specifically, higher levels of anxiety and perceived stress, and having ever taken pharmacological treatment significantly predicted higher levels of depressive symptoms, while higher levels of well-being significantly predicted lower levels of depressive symptoms.
Model 2
Model 2 includes anxious symptoms as the dependent variable and time, depressive symptoms, perceived stress, well-being, gender, living alone, living in a region affected by the eruption, having been evacuated and lost materials, or farms or orchards, having ever received a mental diagnosis, and having ever taken pharmacological treatment as predictors. Anxiety levels were significantly predicted by time, perceived stress, gender, living in a region affected by the eruption, and having ever taken pharmacological treatment. Specifically, lower levels of anxiety were predicted from wave to wave, while significantly higher levels of anxiety were shown in women compared to men. Moreover, higher levels of perceived stress, living in a region affected by the eruption, and having ever taken pharmacological treatment predicted higher anxiety levels.
Model 3
Model 3 included perceived stress as the dependent variable and time, depressive symptoms, anxious symptoms, well-being, gender, residential situation, living in a region affected by the eruption, having ever received a mental diagnosis, and having ever taken pharmacological treatment as predictors. Specifically, lower levels of perceived stress were predicted from wave to wave, while significantly higher levels of perceived stress were shown in women compared to men. Also, higher levels of anxiety significantly predicted higher levels of perceived stress, while higher levels of well-being significantly predicted lower levels of perceived stress.
Model 4
Finally, Model 4 included well-being as the dependent variable and time, depressive symptoms, anxious symptoms, perceived stress, living alone, having been evacuated and farms or orchards, having ever received a mental diagnosis, and having ever taken pharmacological treatment as predictors. It was found that higher levels of depressive symptoms, higher levels of perceived stress, and living alone significantly predicted lower levels of well-being.
Discussion
The aim of this research was to investigate the impact of the eruption of the “Tajogaite” volcano on mental health of La Palma residents and people related to the island. Specifically, depression, anxiety, perceived stress, and well-being were assessed, as well as their evolution in time and their relationship with sociodemographic variables of interest.
Based on previous literature (Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018; Ohta et al., Reference Ohta, Araki, Kawasaki, Nakane, Honda and Mine2003), the main hypothesis was that levels of anxiety would decrease in time, while depression and perceived stress levels would remain stable. Our study found that time was a significant predictor of anxiety. Specifically, anxiety significantly decreased in time going from moderate (M = 11.43) 6 weeks after the start of the eruption (when it had not finished) to mild (M = 9.28) six months later. As expected, time did not significantly explain depression scores and levels remained at the moderate category in all waves (M W1 = 12.24, M W2 = 11.48, M W3 = 10.26). However, lower levels of perceived stress were predicted from wave to wave, being highest at the acute phase of the disaster (M W1 = 30.05, M W2 = 26.3, M W3 = 25.51). These results are consistent with previous research showing that anxiety, depression and mental distress are some of the most common symptoms in the first moments after a volcanic eruption (Goto et al., Reference Goto, Wilson, Kahana and Slane2006; Takagi et al., Reference Takagi, Takahashi, Fukuo, Arai and Tachikawa2021; Zahlawi et al., Reference Zahlawi, Roome, Chan, Campbell, Tosiro, Malanga, Tagaro, Obed, Iaruel, Taleo, Tarivonda, Olszowy and Dancause2019). Moreover, it has been previously reported that, after a period following the eruption, people tend to improve in anxiety and stress symptomatology, but recover more slowly in depression (Ohta et al., Reference Ohta, Araki, Kawasaki, Nakane, Honda and Mine2003).
The stability and gravity of depressive symptoms, as suggested in previous literature, could be related to the interaction between the personal experience of the eruption and other factors such as previous vulnerabilities, lack of social support or lower economic resources (Cova & Rincón, Reference Cova and Rincón2010). Furthermore, it seems that depressive symptoms could be related to greater functional impairment than PTSD or anxiety symptoms, something that could explain why levels of depressive symptoms remain high for longer than other types of symptoms (Hussain et al., Reference Hussain, Weisaeth and Heir2011).
On the other hand, the reduction of anxiety symptoms over time has also been related in other studies to the reduction of uncertainty and feelings of insecurity. Both, uncertainty and insecurity would be reduced after evacuation and stabilization of the event (Afifi et al., Reference Afifi, Felix and Afifi2012).
However, mixed results are found regarding the development in time of perceived stress. Previous studies show that, long periods of time after the disaster (6 months to 3 years), the levels of perceived stress remain stable both in exposed and unexposed people (Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018; Hlodversdottir et al., Reference Hlodversdottir, Petursdottir, Carlsen, Gislason and Hauksdottir2016). This discrepancy shows the necessity to follow participants in time after a disaster given that, while in the medium term there may be an improvement in more acute symptomatology, it is possible that some other gets exacerbated and may need professional support.
Levels of well-being were explored both at the acute phase after the start of the eruption and one and six months after. Previous literature has shown that positive emotions can act as buffering of psychological distress in catastrophic events (Vázquez & Hervás, Reference Vázquez and Hervás2010). However, it is not a common measured variable during disasters. For example, Ruiz and Hernández (Reference Ruiz and Hernández2014) found that positive emotions (interest, mood, activation, enthusiasm, pride) were the strongest during the volcanic eruption in El Hierro in the Canary Islands, Spain. These results point to the importance to further research the protective role that well-being levels could play in these situations. Moreover, all symptoms were significantly correlated in the expected direction, i.e., levels of depression, anxiety, and perceived stress were positively correlated, while well-being was significantly and inversely correlated to all of them. This is important to take into account during these type of catastrophes given that comorbidity is highly common within mood disorders and should be addressed when given psychological support (e.g., Barlow et al., Reference Barlow, Farchione, Bullis, Gallagher, Latin, Sauer-Zavala, Thompson-Hollands, Conklin, Boswell, Ametaj, Carl, Boettcher and Cassiello-Robbins2017).
Regarding demographic variables, it was found that most of the sample in the first wave was present on the island during the volcano eruption (71.55%), with almost 44% living in areas that were directly affected by the volcano. Also, around 25% of participants had been evacuated and around 20% had had a mental health diagnosis or previous symptomatology, with almost 39% having received some type of pharmacological treatment. In the following assessments the percentages remained similar, although there was an increase in the percentage of people reporting being evacuated and suffering some type of material loss (%W1 = 9.98, %W2 = 15.56, %W3 = 14.89), being diagnosed with a mental disorder (%W1 = 19.53, %W2 = 25.56, %W3 = 29.79), and receive psychopharmacological treatment (%W1 = 38.64, %W2 = 47.78, %W3 = 40.43). In addition, having a previous diagnosis and having ever followed a pharmacological treatment was significantly associated with a greater psychological impact (higher symptoms of depression, anxiety, and perceived stress, and lower levels of well-being). Living in a region directly affected by the volcano also correlated with all variables except well-being and having been evacuated correlated with all variables except perceived stress. These results seem to point to groups of special vulnerability, such as those people who have been directly affected by the volcano, as consistently reported in prior research (Carlsen et al., Reference Carlsen, Hauksdottir, Valdimarsdottir, Gíslason, Einarsdottir, Runolfsson, Briem, Finnbjornsdottir, Gudmundsson, Kolbeinsson, Thorsteinsson and Pétursdóttir2012; Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018; Goto et al., Reference Goto, Wilson, Kahana and Slane2006; Warsini et al., Reference Warsini, Buettner, Mills, West and Usher2015), as well as people with previous mental health problems. Furthermore, the relationship found between depressive symptoms and proximity to the eruption could also be associated with greater attachment to the place and a greater number of losses, as has been found in other research (Goto et al., Reference Goto, Wilson, Kahana and Slane2006). On the other hand, a surprising finding is that age showed no relationship with any of the measures of psychological impact. Previous literature shows that older people may be more psychologically affected by this type of events (Goto et al., Reference Goto, Wilson, Kahana and Slane2006; Ohta et al., Reference Ohta, Araki, Kawasaki, Nakane, Honda and Mine2003). Future studies could investigate the moderators in the relationship between age and mental health impact after a natural disaster.
The results from the multilevel regression models help us identify potential predictors and protectors of the different symptom categories. On the one hand, significant predictors of depression were anxiety, perceived stress, and having undergone previous pharmacological treatment. Significant predictors of anxiety were perceived stress, living in a region affected by the volcano, being female and previous pharmacological treatment, while perceived stress was significantly predicted by anxiety and being female. These results are consistent with previous research showing higher levels of anxiety and distress in women during these events (Takagi et al., Reference Takagi, Takahashi, Fukuo, Arai and Tachikawa2021; Warsini et al., Reference Warsini, Buettner, Mills, West and Usher2015; Zahlawi et al., Reference Zahlawi, Roome, Chan, Campbell, Tosiro, Malanga, Tagaro, Obed, Iaruel, Taleo, Tarivonda, Olszowy and Dancause2019). Nevertheless, it is surprising that gender was not a significant predictor of depression given the higher prevalence of this disorder in women compared to men (World Health Organization, 2021).
The proximity to the disaster (e.g., living in a region affected by the volcano) is also a common variable found to be related to anxiety, which could be produced by changes in attachment to the island or feelings of loss (Carlsen et al., Reference Carlsen, Hauksdottir, Valdimarsdottir, Gíslason, Einarsdottir, Runolfsson, Briem, Finnbjornsdottir, Gudmundsson, Kolbeinsson, Thorsteinsson and Pétursdóttir2012; Gissurardóttir et al., Reference Gissurardóttir, Hlodversdóttir, Thordardóttir, Pétursdóttir and Hauksdóttir2018; Ruiz & Hernández, Reference Ruiz and Hernández2014). In fact, from the resource conservation theory (Hobfoll, Reference Hobfoll2001), losses are a fundamental variable in the stress process, which explains how a greater proximity to the affected area and more affectation in terms of the evaluation of materials or belongings are predictors of symptomatology. On the other hand, well-being was a significant protector of depression and perceived stress, but not anxiety. At the same time, lower levels of well-being were significantly predicted by depressive symptomatology, perceived stress, and living alone. This result shows importance of social support during these events. This is consistent with previous studies showing the relationship between lack of available support and greater psychological distress in displacements due to volcanic activity (Zahlawi et al., Reference Zahlawi, Roome, Chan, Campbell, Tosiro, Malanga, Tagaro, Obed, Iaruel, Taleo, Tarivonda, Olszowy and Dancause2019).
The psychological impact of the volcano is diverse, with the different symptomatology being related to each other. Thus, it is essential to act to reduce the suffering of people in natural disasters. Previous literature shows how psychosocial interventions have proved adequate to limit the chronicity of psychological problems and improve well-being (Thordardottir et al., Reference Thordardottir, Gudmundsdottir, Petursdottir, Valdimarsdottir and Hauksdottir2018), being highly relevant to address the socio-spatial connection with the region (Berroeta & de Carvalho, Reference Berroeta and de Carvalho2021). Previous catastrophes show that there are higher rates of medical than psychosocial care due stigma (Goto et al., Reference Goto, Wilson, Kahana and Slane2006). Psychological support should be promoted since the onset of the crisis and continue until its end with some type of follow-up (Makwana, Reference Makwana2019), and it should be accessible to those who need it to avoid further burden and distress.
Finally, there are several limitations in this research, and results should be interpreted with caution. First, the sampling method was not controlled and led to under-representation of certain groups, such as older people, and over-representation of others (e.g., women were the 79% of the sample). In addition, sample size was not calculated a priori and attrition was high along the waves and could have affected the results, as well as the sample size is not particularly large and the sample is self-referred, which may affect the generalizability of the results. Moreover, the assessment of some demographic variables was made with ad hoc questions, for example, the impact of events associated with the volcano (evacuation). However, the inclusion of standardized and validated tools was not possible given the specificity of the situation and cultural context. On the other hand, in the multilevel symptom prediction models, the presence of symptomatology in many cases is a predictor of another variable (e.g., anxiety is a predictor of depression). Although we considered carrying out these models excluding these variables, it was decided to include them because of their strong effect, which shows the importance of comorbidity in symptomatology. However, it would be advisable to carry out factor models or pathway analysis models to explain these effects in more detail in the future.
The present research shows the impact in mental health in La Palma population after the Tajogaite volcanic eruption. Results allowed us to identify particularly vulnerable groups such as people with mental health problems and under pharmacological treatment, those who lived in a region affected by the catastrophe, and women. Early actions from a psychosocial framework are encouraged to provide mental health care to those who need it.
Authorship credit
C. C. M.: Conceptualization, data curation, formal analisis, methodology, resources, validation, visualization, writing–original draft, writing–review & editing. I. N. R.: Conceptualization, data curation, formal analysis, methodology, software, validation, visualization, writing–original draft, writing–review & editing. C. G.-S.: Conceptualization, formal analysis, methodology, validation, visualization, writing–original draft, writing–review & editing. C. M. M.: Conceptualization, methodology, project andministration, supervision, validation, visualization, writing–original draft, writing–review & editing.
Data sharing
Data will be shared upon razonable request to the corresponding author.
Acknowledgement
The team in charge of this investigation would like to thank Enrique Hernández (responsible for the page ”Volcanoes and Science Today"), who gave greater visibility to this study and supported residents throughout the event. We would also like to thank Daniel Vázquez Estévez, who also participated in the data analysis of the research.
Conflicts of Interest
None.





 Open access
Open access