



Introduction
Although historical perspectives can be traced back to philosophical and theological texts (Martin et al., Reference Martin2015), the notion of “successful aging” (SA) began to be used in the literature in the 1950s (see Baker, Reference Baker1959) and has been defined in a variety of ways by numerous researchers (Cosco et al., Reference Cosco, Prina, Perales, Stephan and Brayne2014; Depp and Jeste, Reference Depp and Jeste2006). One of the earliest definitions of SA was proposed by Havighurst (Reference Havighurst1961) as “a statement of the conditions of individual and social life under which the individual person gets a maximum of satisfaction and happiness and society maintains an appropriate balance among satisfactions for the various groups which make it up-old, middle-aged, and young, men and women, etc.” (p. 8), both a testable experience and an adaptable theory. Since then, the concept of SA has been widely adopted by the science of gerontology and extensively used in literature on aging (Lee et al., Reference Lee, Lan and Yen2011).
Many researchers have proposed their own models by making the conceptual and operational definition of SA the context of their research, and thus various perspectives on SA have developed. In a review conducted by Depp and Jeste (Reference Depp and Jeste2006), 29 different definitions of SA were identified that can be classified under four basic headings: physical functioning/disability, cognitive functioning, well-being/life satisfaction, and productive/social engagement. Cosco et al. (Reference Cosco, Prina, Perales, Stephan and Brayne2014), in a comprehensive analysis that included the findings of 84 studies, found 105 operational definitions of SA. In summary, SA is an interdisciplinary concept that, despite all the efforts so far, still lacks a generally accepted definition.
Rowe and Kahn’s model of successful aging
Models and theories of SA can be categorized under two main headings: biomedical and psychosocial (Bowling and Dieppe, Reference Bowling and Dieppe2005). One of the most influential and widely cited biomedical SA models in the literature has been proposed by Rowe and Kahn (Reference Rowe and Kahn1997). Based on the distinction between aging and disease, Rowe and Kahn (Reference Rowe and Kahn1997) defined three forms of aging: (a) pathological aging, which is identified by the presence of serious diseases that result in some form of impairment; (b) usual aging, which is characterized by the absence of serious illnesses but also by a heightened chance of developing them; and (c) successful aging, which is described by three primary characteristics: low risk of disease and disease-related impairment, high physical and cognitive functional capacity, and active engagement with life.
According to Rowe and Kahn’s (Reference Rowe and Kahn1997) conceptualization, an individual who is successfully aging has high physical and cognitive function, low risk of chronic disease and disability, and social engagement in older age. Despite its many strengths and contributions, Rowe and Kahn’s (Reference Rowe and Kahn1997) SA model has also sparked a lot of criticism and suggestions. For example, some researchers argue that Rowe and Kahn’s model is not sufficiently comprehensive and suggest that positive spirituality (Crowther et al., Reference Crowther, Parker, Achenbaum, Larimore and Koenig2002), financial security (Iwamasa and Iwasaki, Reference Iwamasa and Iwasaki2011), and leisure activities (Lee et al., Reference Lee, Lan and Yen2011) should also be considered components of SA.
Socioemotional selectivity theory
Socioemotional selectivity theory (SST), as one of the most basic theories in the literature on aging today (Dietz and Fasbender, Reference Dietz and Fasbender2022; Fung and Isaacowitz, Reference Fung and Isaacowitz2016), was developed by Carstensen et al. (Reference Carstensen, Isaacowitz and Charles1999), not as a successful aging model, but to explain the social and emotional development of the individual depending on the perception of time left in life. According to the basic tenet of the theory, the future time perspective (FTP) is one of the fundamental concepts of the theory, and it plays a fundamental and crucial role in motivation, emotion, social goals, and partner selection (Carstensen, Reference Carstensen2006). However, the FTP is conceptualized in different ways by different researchers. In one of the earliest definitions of FTP, Lewin (Reference Lewin1939) refers to it as: “the scope of time ahead which influences present behavior” (p. 879). According to Zimbardo and Boyd’s Time Perspective Theory (Reference Zimbardo and Boyd1999), the time perspective is defined as a personal and usually unconscious attitude toward time frames that aids in providing events a sense of order, coherence, and meaning. In contrast, for Brothers et al. (Reference Brothers, Gabrian, Wahl and Diehl2016), FTP has an adaptable, cognitive, motivational, and age-related structure that represents a two-pronged process within the framework of SST.
SST claims that chronological age provides an ideal basis for the evaluation of FTP as its strongest and most robust predictor. Specifically, as people age, they move from an “open-ended” time perspective to a “limited” time perspective (Lang and Carstensen, Reference Lang and Carstensen2002). Consistent with SST, there is a vast body of research covering young adulthood to old age revealing higher chronological age to be related to a more limited time, that is, older adults report a more limited FTP than their younger counterparts (Brothers et al., Reference Brothers, Gabrian, Wahl and Diehl2016; Lang and Carstensen, Reference Lang and Carstensen2002; Soylu and Ozekes, Reference Soylu and Ozekes2020).
According to SST, because FTP is perceived as more limited with increasing age, individuals tend to limit their social circles and interact with smaller social groups, being those who can best provide them with emotionally meaningful experiences (Carstensen, Reference Carstensen2006). In other words, peripheral relationships are more vulnerable to change depending on the FTP, whereas very close social relations, such as family relationships, are usually more enduring. The purpose of this selective narrowing of the social network is to maximize positive emotional experiences while minimizing emotional risks (Carstensen et al., Reference Carstensen, Isaacowitz and Charles1999). This assertion has been confirmed in many cultures among different age groups in studies using different research methods.
For example, in a cross-sectional study, Lang and Carstensen (Reference Lang and Carstensen1994) indicated that the number of very close ties between old and very old persons is the same, but the number of less close partners is reduced in the very old group among community-dwelling adults aging 70–104 years. In English and Carstensen’s (Reference English and Carstensen2014) longitudinal study, it was reported that social networks consistently decrease in size after reaching the age of 50, and this continues until the end of life. The decline in the size of one’s social network is generally at the expense of people from whom one feels relatively distant, whereas the number of very close contacts remains relatively constant over time. In a meta-analysis supporting this finding, involving a sample spanning adolescence to old age, the global social network was noted to increase up until young adulthood and then to enter a constant decline, while the family network remained constant from adolescence to old age (Wrzus et al., Reference Wrzus, Hänel, Wagner and Neyer2013).
Purpose of the present study
The main objective of the present study is to test the basic tenets of the SST regarding social network characteristics in a model where the outcome variable is SA in a non-Western semi-collectivist culture. Rowe and Kahn (Reference Rowe and Kahn2015), who developed one of the most widely accepted SA models, claim that SST is a life-course-oriented and psychology-based theory that emphasizes the “how” of SA, whereas our SA model emphasizes the “what” of SA, and we opted to treat Rowe and Kahn (Reference Rowe and Kahn2015) as an outcome variable.
In the studies conducted to date in which different approaches are adopted, several variables have been put forward as indicators of SA, such as psychological well-being (Matud et al., Reference Matud, Bethencourt, Ibáñez and Fortes2020), life satisfaction (Dumitrache et al., Reference Dumitrache, Rubio and Cordón-Pozo2019), and self-rated successful aging (Cassidy et al., Reference Cassidy2021). In contrast, there have been few studies combining a broad range of biomedical and psychosocial criteria in a single model. Addressing this shortfall, the present study proposes and tests a biopsychosocial SA model based on Rowe and Kahn’s (Reference Rowe and Kahn1987, Reference Rowe and Kahn1997) SA model and the suggestions of previous researchers (Cosco et al., Reference Cosco, Prina, Perales, Stephan and Brayne2014; Whitley et al., Reference Whitley, Benzeval and Popham2020). The present study builds on the body of available literature by combining different indicators from two main SA approaches (i.e. biomedical and psychosocial) that have to date been studied in largely separate studies and investigates the potential explanatory mechanisms behind SA.
On the basis of the predictions of the SST, we hypothesized (H1) that chronological age would be negatively correlated with (a) a “focus on opportunities” and (b) positively correlated with a “focus on limitations.” Next, we hypothesized (H2) that the FTP would be positively correlated with (a) an outer circle (i.e. the number of close or less close social partners), (b) biopsychosocial SA, and (c) social satisfaction, (d) but not correlated with an inner circle (i.e. the number of very close social partners). Next, the inner circle was expected (H3) to yield direct positive relations with (a) social satisfaction, but not (b) biopsychosocial SA. In turn, we hypothesized (H4) that social satisfaction will have a positive direct link with biopsychosocial SA. We further hypothesized (H5) that the outer circle was not significantly correlated with (a) social satisfaction and (b) biopsychosocial SA. Beyond these direct associations, we hypothesized (H6) that the FTP will have positive indirect effects on biopsychosocial SA via the mediating role of (a) social satisfaction but not (b) the inner circle and (c) the outer circle. Supplementary File 1 shows the direct, indirect, or mediating pathways from FTP to biopsychosocial SA.
Methods
Sampling and procedure
The inclusion criteria were as follows: (a) aged at least 50 years; (b) residing in a community as a local older adult resident, or resident of a nursing home for more than six months; (c) no severe cognitive impairment (after obtaining written and verbally informed consent, all adults were screened using the Mini-Mental State Examination [MMSE] test, and those scoring above the recommended cutoff [≥20] [M = 26.03, SD = 2.38] were included) and, (d) able to communicate.
For the identification of community-dwelling adults to take part in the study, the first researcher applied to the municipal centers with the study proposal for the collection of data. The municipal centers also provided the first author with schedules of the painting, sports, music, etc. programs run for the elderly, in which the first author subsequently joined. The attendees of the programs were invited to participate in the study, and those that agreed were interviewed in an available room in the municipal centers. Regarding nursing home residents, nursing home staff members were requested to compile a list of residents who they believed were capable and willing to participate in the study. The researcher then approached each individual on the list to provide details about the study protocol and to invite them to participate in the study. All study procedures were approved by the Ege university’s ethical committee (Approval number = 04/10, 204).
Measures
Indicators of SA
Chronic disease and disability
The participants were asked about the presence of chronic disease(s) (e.g. cancer). The Katz Index of Independence in Activities of Daily Living Scale (Katz ADL; Katz et al., Reference Katz, Ford, Moskowitz, Jackson and Jaffe1963) was used to determine the disability status of the participants, which measures ability in six self-care tasks, such as feeding, using a dichotomous rating (0 = dependent; 1 = independent). A score of six indicates full function or independent. The internal consistency in the present study was α = .77.
Physical and cognitive functioning
Physical functioning was assessed using the Lawton Instrumental Activities of Daily Living Scale (Lawton IADL; Lawton and Brody, Reference Lawton and Brody1969). Items are rated trichotomously (1 = unable, 2 = able with help, 3 = able without help). A score of 8–16 indicates dependence or semi-dependence, and scores of 17–24 indicate independence. α reliability estimate for the scale was .95 in the present study.
Cognitive impairment was measured using the MMSE test (Folstein et al., Reference Folstein, Folstein and McHugh1975), which consists of 11 items. There are five subsections in the MMSE and the maximum score is 30. The MMSE scale is used to classify cognitive impairment in older adults into the following categories: 24–30 indicates intact cognitive function; 20–23 indicates mild cognitive impairment; 10–19 indicates moderate cognitive impairment; and 0–9 indicates severe cognitive impairment (Güngen et al., Reference Güngen, Ertan, Eker, Yaşar and Engin2002).
Active engagement with life
Consistent with previous research (Brandt et al., Reference Brandt, Deindl and Hank2012), participants were defined as being actively engaged if they reported: (a) living with a partner; having “provided help to family, friends, or neighbors” or having “gone to a sport, social, or other kind of club” in the month preceding the interview; and (b) having done “any paid work” or “voluntary or charity work” in the month preceding the interview, or having provided any grandchild care during the past twelve months.
Psychological well-being
An 18-item version of the psychological well-being scale was used to assess well-being (PWB; Ryff and Keyes, Reference Ryff and Keyes1995). Responses were measured on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), such that higher scores indicated higher well-being. The internal consistency in this study was .95.
Life satisfaction
This was measured with a 5-item Life Satisfaction Scale (LS; Diener et al., Reference Diener, Emmons, Larsen and Griffin1985). Participants responded to the items using a Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). The measure produces a total score, with higher scores indicating better life satisfaction. The internal consistency in this study was .90.
Subjective SA
In line with Montross et al. (Reference Montross2006), participants were asked to rate themselves in terms of SA on a Likert-type single item which ranging from 1 (least successful) to 10 (most successful).
Measures used to test the SST
Future time perspective
We used a 10-item FTP Scale (Carstensen and Lang, Reference Carstensen and Lang1996) to assess time perspective. The FTP scale comprises two dimensions to examine the focus on opportunities (FTO) and focus on limitations (FTL). Responses are made on a 7-point Likert-type scale (1 = very untrue to 7 = very true). α reliability estimates for the scales were as follows: .94 for FTO and .85 for FTL in the present sample.
Social networks characteristics
The social networks of participants were assessed with the circle-diagram method (Kahn and Antonucci, Reference Kahn, Antonucci, Baltes and Brim1980). Participants reported the names or numbers of network partners in three concentric circles with a smaller fourth circle in the center in which the word “you” was written. In the inner circle, participants were asked to list “people you feel very close to, so close that it would be hard to imagine life without them”; in the middle circle, they were asked to list “people you don't feel quite so close to as those in the inner circle but who are still very important to you”; in the outer circle, they were asked to list “people you feel less close to but who are still important to you.”
Social satisfaction
In line with Lang and Carstensen (Reference Lang and Carstensen2002), social satisfaction was assessed with two items: “How satisfied are you with your social partners in general?” and “How satisfied are you with your family and relatives” on a rating scale ranging from 1 (very dissatisfied) to 5 (very satisfied) where higher ratings reflected higher social satisfaction. The two measures were positively correlated (r = .63, p < .001).
Statistical Analyses
All variables were checked and screened for missing data, normality, and the presence of univariate and multivariate outliers (Tabachnick and Fidell, Reference Tabachnick and Fidell2013). Twelve extreme cases were detected as univariate outliers, and four cases were detected as multivariate outliers with the inspection of Mahalanobis distances, so were excluded from the data.
First, the biopsychosocial SA model was tested using exploratory factor analysis (EFA) and then confirmatory factor analysis (CFA). The basic tenets of the SST were investigated with preliminary analysis and pathways using structural equation models (Kline, Reference Kline2016). Benchmarks for acceptable fit were small and non-significant chi-squared values, for the comparative fit index (CFI) and Tucker-Lewis Index (TLI) >.90 acceptable (Byrne, Reference Byrne2012), >.95 good fit; standardized root-mean-square residual (SRMR) <.08; root-means-square of error of approximation (RMSEA) <.06 (Hu and Bentler, Reference Hu and Bentler1999). To test the significance of the hypothesized indirect relations in the model, we used bootstrap procedures to run the model with 10,000 bootstrap samples. If the 95% confidence interval (CI) does not contain zero, then the indirect effects are considered significant and indicate mediation (Mallinckrodt et al., Reference Mallinckrodt, Abraham, Wei and Russell2006). Descriptive statistics and preliminary analyses were conducted in SPSS (version 25) and in R (version 3.6.3; R Core Team, 2021) and structural equation model analyses were conducted in Mplus (version 8; Muthén and Muthén, Reference Muthén and Muthén1998–2017).
Results
Sample characteristics
A total of 561 people from Izmir on the western coast of Turkey were approached in July 2019 and February 2020 for the study. Izmir is Turkey’s third largest city and is known for the modern lifestyle and the generally more individualistic attitude of its residents when compared to the rest of Turkey (Sahin-Acar and Leichtman, Reference Sahin-Acar and Leichtman2018). Of the initial sample of 561 people, 25 (4.7%) living in a nursing home and 21 (3.9%) community-dwelling older adults scored ≤19 in the MMSE test and so were excluded from the study (total 46 [8.6%]). The remaining 515 eligible participants were given questionnaires to fill out. The forms with more than 10% missing responses were excluded from the sample (n = 21). Moreover, 16 of those who were recruited and tested did not provide valid data due to statistical assumptions. After removing these participants, the final sample consisted of 478 adults. The characteristics of participants included in the study are summarized in Table 1.
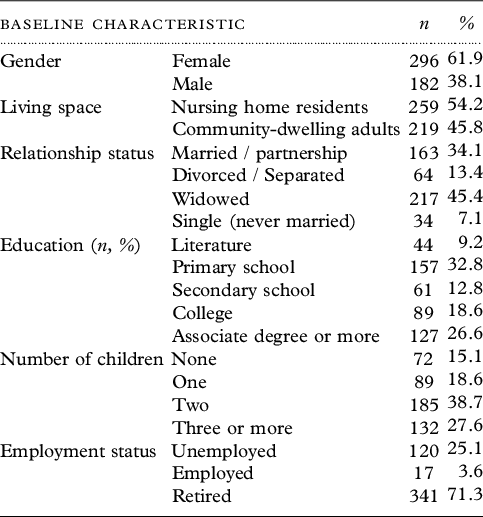
Table 1. Sample characteristics

Note. N = 478. The participants included in the analyses had a mean age of 72.11 years (SD = 10.43), with ages ranging from 50–98 years.
Missing data
The results of Little’s Missing Completely at Random test were non-significant, χ2(856) = 837.353, p = .669, indicating the complete randomness of the missing data. The expectation-maximization algorithm was used to impute missing values.
EFA and CFA of biopsychosocial SA model
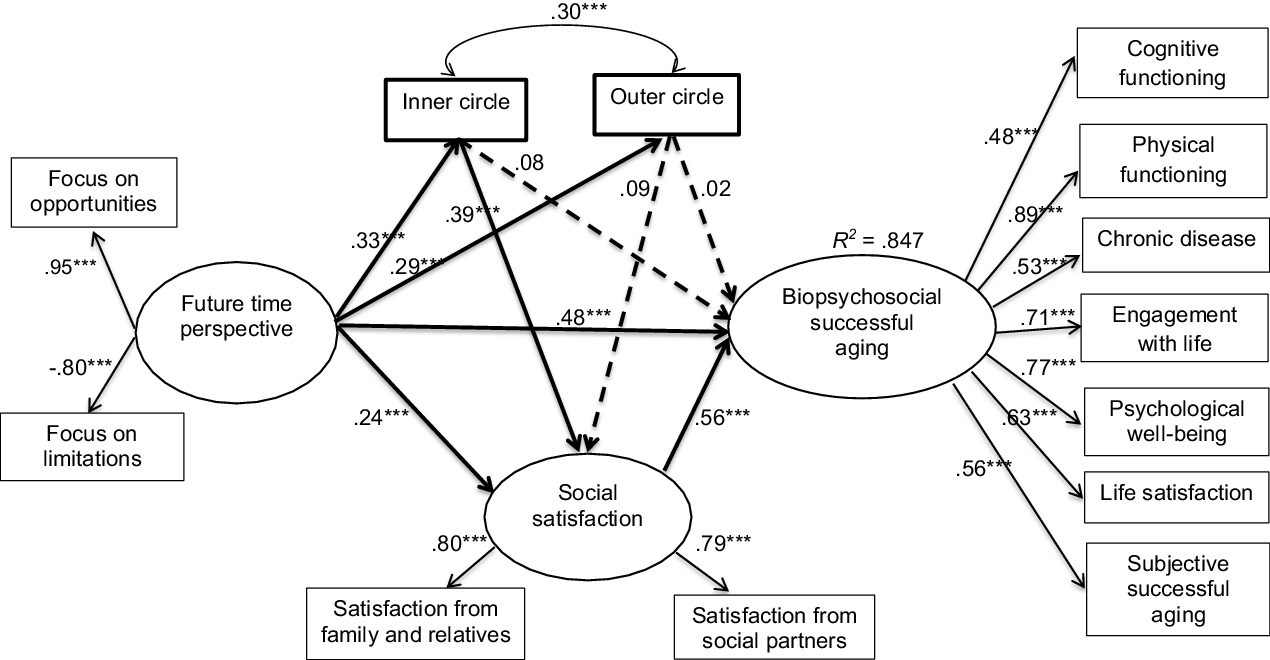
The findings within EFA and CFA showed a good fit to the data. The factor loadings of the observed variables were significant (all p’s < .001) and are presented in Figure 1. Detailed findings are presented in Supplementary File 2.

Figure 1. Factor model of the biopsychosocial successful aging model. Note. The illustration shows the standardized model parameters for the model estimated. Psychological well-being, life satisfaction, and subjective successful aging coded as continuous variables; cognitive functioning, physical functioning, chronic disease, and engagement with life coded as dichotomous variables.
Model testing
Measurement and structural model
The measurement model demonstrated an acceptable fit to the data: χ2 (41) = 107.148, p < .001, CFI = .932, TLI = .909, SRMR = .058, and RMSEA = .058 (%90 CI [.045–.072]). Factor loadings of the observed variables and correlations among the latent variables were significant (p < .001). The hypothesized structural model was not an acceptable fit to the data: χ2 (58) = 211.330, p < .001, CFI = .881, TLI = .840, SRMR = .064, and RMSEA = .074 (%90 CI [.064–.085]). In line with the modification indices, we decided to examine alternative models and the inner and outer circles were allowed to correlate in the structural models. The alternative structural model fit was acceptable χ2 (57) = 156.668, p < .001, CFI = .923, TLI = .894, SRMR = .058 and RMSEA = .060 (%90 CI [.049–.072]) and accounted for 84.7% of the variance in biopsychosocial SA. The fit of this model is significantly improved compared with the hypothesized structural model (χ2 Δ = 65.945, p < .001).
Test of direct relations
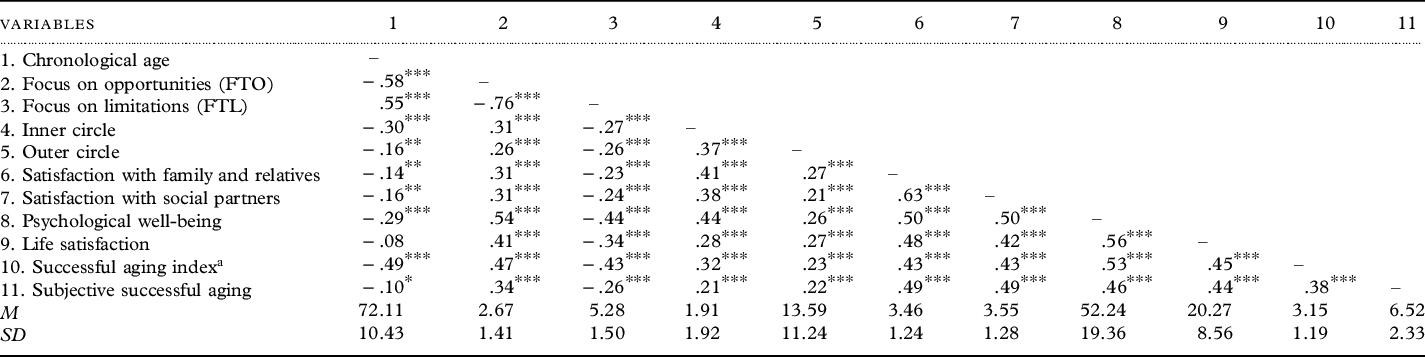
Correlations among variables are presented in Table 2. In line with first hypothesis, chronological age was negatively correlated with FTO scores (r = −.58, p < .001) (H1a); however, it was positively correlated with FTL scores (r = .55, p < .001) (H1b). Consistent with H2, the FTP significantly predicted the outer circle (β = .29, p < .001) (H2a), biopsychosocial SA (β = .48, p < .001) (H2b), and social satisfaction (β = .24, p < .001) (H2c). In contrast to our expectation, the FTP significantly predicted the inner circle (β = .33, p < .001) (H2d). The inner circle significantly predicted social satisfaction (β = .39, p < .001) (H3a); but did not significantly predict biopsychosocial SA (β = .08, p = .209) (H3b). Social satisfaction significantly predicted biopsychosocial SA (β = .56, p < .001) (H4). As expected, the outer circle did not significantly predict social satisfaction (β = .09, p = .053) (H5a) and biopsychosocial SA (β = .02, p = .634) (H5b). Standardized unique direct relations for the model are depicted in Figure 2.

Figure 2. Standardized direct effects and percentage of variance explained in the hypothesized structural model. Note. Statistics are standardized regression coefficients. Dotted lines indicate hypothesized non-significant relations; bold lines indicate hypothesized significant direct relationships. **p < .01. ***p < .001.
Table 2. Inter-correlations for study variables

Note. aSuccessful aging index was computed the number of five achieved indicators of SA (i.e. high physical functioning, high cognitive functioning, no chronic disease, without disability, and active engagement with life); *p-value < .05. **p-value < .01. ***p-value < .001.
Test of indirect relations
Results of the mediation analyses are seen in Table 3. As expected, the indirect effects of the FTP on biopsychosocial SA via social satisfaction were significant (β = .132, SE = .027, %95 CI [.080–.185]) (H6a). The indirect effects of the FTP on biopsychosocial SA via the inner circle (β = .027, SE = .023, %95 CI [−.010 to .078]) (H6b) and outer circle (β = .006, SE = .012, %95 CI [−.020 to .029]) (H6c) were not significant. However, we do not have such a hypothesis, there was one significant indirect sequential path from the FTP to biopsychosocial SA. The indirect effects of the FTP on biopsychosocial SA first, via the inner circle, and second, via social satisfaction, were significant (β = .071, SE = .014, %95 CI [.046–.100]). The other path first, via the outer circle, and second, via social satisfaction, was not significant (β = .014, SE = .008, %95 CI [.000–.030]). The significant total indirect relationships and findings from the comparison of the hypothesized partially mediated model, and the fully mediated model suggest that the mediator variables are partially mediated in the relationship between FTP and biopsychosocial SA. Detailed findings are presented in Supplementary File 3.
Table 3. Direct, indirect, and total effects of FTP to successful aging via social satisfaction, inner, and outer circle

Note. FTP = Future Time Perspective; SA = Successful Aging. SS = Social Satisfaction; C. = Circle; CI = Confidence Interval; LL = Lower Limit; UL = Upper Limit.
Discussion
Carstensen (Reference Carstensen2006) argued that there is a transition from the FTO to the FTL with increasing age. Consistent with the SST, it was found that as chronological age increased, the perception of limitations increased, and a sense that time is open-ended decreased. This finding is consistent with many research findings conducted both in our country (i.e. Turkey) and in other countries and is one of the most well-known findings of the SST in the literature (Lang and Carstensen, Reference Lang and Carstensen2002; Mahlo and Windsor, Reference Mahlo and Windsor2021; Soylu and Ozekes, Reference Soylu and Ozekes2020).
In line with SST and previous studies reporting a positive relationship between FTO and the number of people in the social network (Lang and Carstensen, Reference Lang and Carstensen2002; Windsor et al., Reference Windsor, Fiori and Crisp2011), the results of the present study reveal that as time is perceived as open-ended, the number of individuals who feel less close increases significantly. On the basis of the SST, this finding suggests that when the remaining lifetime seems unlimited, individuals increase their social network size to achieve information-seeking goals (Carstensen, Reference Carstensen2006). However, contrary to the SST argument that suggests the number of people who an individual feels very close to does not differ depending on the FTP (Carstensen et al., Reference Carstensen, Isaacowitz and Charles1999), we found that the FTO positively predicted the number of very close social partners. Wrzus et al. (Reference Wrzus, Hänel, Wagner and Neyer2013) indicated that the social network is affected by many factors, including culture, and this finding may have resulted from cultural values. Specifically, in the Turkish culture, the values attributed to children and parents, being among those to whom people feel closest, have changed over time, with a sharp increase noted in psychological values and a consequent decrease in economic values (Kagitcibasi and Ataca, Reference Kagitcibasi and Ataca2005). Therefore, cross-cultural research is needed on how the components of the social network follow a pattern depending on the FTP.
McGinnis (Reference McGinnis2018), in a study of adults aged 45–58, found that FTO positively predicted life satisfaction, and individuals with FTO perceived their lives as more satisfying. More recently, Sakakibara and Ishii (Reference Sakakibara and Ishii2020) have shown that FTO leads to increased well-being through the mediation of emotion regulation. In line with these studies, it was found that the FTO directly and positively predicted biopsychosocial SA, which includes both the psychosocial and the biomedical indicators of SA in the present study. It should be noted, however, that while identifying the effect of emotion regulation strategies on SA falls outside the scope of this study, future studies may consider the role of emotion regulation strategies in SA.
Jang (Reference Jang2020) examined the factors associated with SA based on the ecological system model and stated that satisfaction with a spouse was related to SA. Similarly, Dumitrache et al. (Reference Dumitrache, Rubio and Cordón-Pozo2019) focused on psychosocial resources that predict SA and indicated that satisfaction with family was the main social resource influencing older adult’s SA. In the present study, consistent with these findings, it was found that social satisfaction positively predicted SA and was a partial mediator variable between the FTP and SA. In other words, perceiving time as open-ended increases the individual’s satisfaction from social relations, which in turn results in a higher SA. Considering that the prevalence of multimorbidity is increased substantially with age (Barnett et al., Reference Barnett, Mercer, Norbury, Watt, Wyke and Guthrie2012) and that adults need more social support when they experience health problems or functional impairments (Bruggencate et al., Reference Bruggencate, Luijkx and Sturm2018), it is obviously not surprising that the FTL with increasing age predicts social satisfaction and that those who are highly satisfied with their social relationships age more successfully. It is possible that adults who are well satisfied with their social relations have obtained more information and developed rich strategies that make it easier to cope with the problems in daily life that result from the aging process.
There have been several studies conducted in different countries, including the United States (Montross et al., Reference Montross2006) and Spain and Costa Rica (Blanco-Molina et al., Reference Blanco-Molina, Pinazo-Hernandis, Montoro-Rodriguez and Tomas2021), reporting that the number of close friends and level of social functioning based on the size, closeness, and contact frequency of one’s social network is related significantly to SA. In contrast to these studies, Bruin et al. (Reference Bruin, Parker and Strough2020) indicated that well-being was more strongly related to social satisfaction than to the reported number of close friends and concluded that the sense of relationship quality, rather than relationship number, had a greater impact on well-being. In line with the findings of Bruin et al. (Reference Bruin, Parker and Strough2020), our hypothesis concerning the significant effect of social satisfaction on SA was confirmed. In other words, as expected, we found that social satisfaction, rather than the number of very close social partners, positively predicted a higher SA. Our findings reveal that the most important factor in social relationships is not quantity but quality, which is consistent with the findings of previous studies (Fratiglioni et al., Reference Fratiglioni, Wang, Ericsson, Maytan and Winblad2000; Uchino et al., Reference Uchino, Cacioppo and Kiecolt-Glaser1996).
Our results reveal the magnitude of the FTP for the number of people from whom one feels relatively distant (i.e. outer circle) and very close (i.e. inner circle) were small to medium, indicating that the inner and outer circles are similarly affected by the FTP, contrary to SST. Furthermore, the inner circle was found to have a greater effect size (i.e. medium) than the FTP (i.e. small) for social satisfaction. This finding is of particular interest, as it approves the tenets of SST by indicating that the FTP more strongly affects social satisfaction, though indirectly, via the inner circle. Lastly, our findings reveal that social satisfaction has a greater effect on SA than FTP in adults aged 50–98 years. Practically speaking, clinicians should be more interested in social satisfaction levels when seeking to enhance SA in future studies.
In summary, when the findings of the present study were evaluated as a whole, relatively expected results were obtained in the light of previous findings and the predictions of the SST. More specifically, in line with the SST, it was found that future time is perceived as more limited with increasing age, while the belief that time is limited was found to be associated with a smaller social network. Conversely, those who perceive future time as being open-ended tended to witness a greater increase in their social networks. According to our findings, the realization that time is a limited personal resource fundamentally changes the number of peoples’ close and not close social partners. Beyond testing the basic tenets of the theory, one of the most important findings of the present study is that the number of close social partners and social satisfaction are two sequential mediator variables between the FTP and SA. More specifically, our data suggest that individuals who perceive future time as open-ended increase the number of social partners to whom they feel very close, which has a positive impact on SA by increasing the satisfaction obtained from social relationships.
Consequently, this study expands on existing knowledge by providing novel evidence of a much more complex pattern of SST arguments that result in SA. It is worthy of note, however, that these findings were obtained from a study of a non-Western semi-collectivist culture, and that the characteristics of different social networks may be culture-specific. As such, future studies should include people from different cultures and explore the moderating role of culture in the relationship between these variables. All in all, as suggested by Rowe and Kahn (Reference Rowe and Kahn2015), it can be said that the tenets of Carstensen et al.’s (Reference Carstensen, Isaacowitz and Charles1999) SST are largely valid in adults aged 50–98 years, and the complex relationship pattern between the variables results in successful aging.
Limitations and future directions
The present study contributes to existing literature by considering the aging experiences of individuals and the social development process that allow SA. However, there are several limitations that must be considered. One of the limitations of the current study is that because the community-dwelling adults were recruited from centers attended by participants with good health, this may have caused the sample to be biased. As a further limitation, the living space of the respondents (i.e. community-dwelling adults and nursing home residents) was not considered a moderator variable in the present study, and so future studies should test the models for these two subgroups. Furthermore, aging is a dynamic process that can have a negative impact on the general well-being of the individual by impairing health and functional status. Previous studies carried out with the longitudinal method suggested that individuals who were initially classified as successful agers could not maintain this situation in the follow-ups, and their SA status changed (McLaughlin et al., Reference McLaughlin, Connell, Heeringa, Li and Roberts2010; Ulfa and Sartika, Reference Ulfa and Sartika2019). With this cross-sectional study, a snapshot was taken of the SA status of adults in different age groups and living in different contexts.
Conflict of interest
None.
Source of funding
This study is based in part on the primary author’s doctoral thesis, which was supported by the “Koç University Prof. Dr. Cigdem Kagitcibasi Human Development Research Award” in 2020.
Description of authors’ roles
C.S designed the study, collected the data, and wrote the paper. He was responsible for the statistical design of the study and for carrying out the statistical analysis. B.C.Ö. contributed to manuscript writing and supervised the data collection process.
Acknowledgements
The authors wish to acknowledge all those who participated in this study.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1041610222001090





 Open access
Open access